Efficacy and Safety of Botulinum Toxin Type A on Persistent Myofascial Pain: A Randomized Clinical Trial

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Results
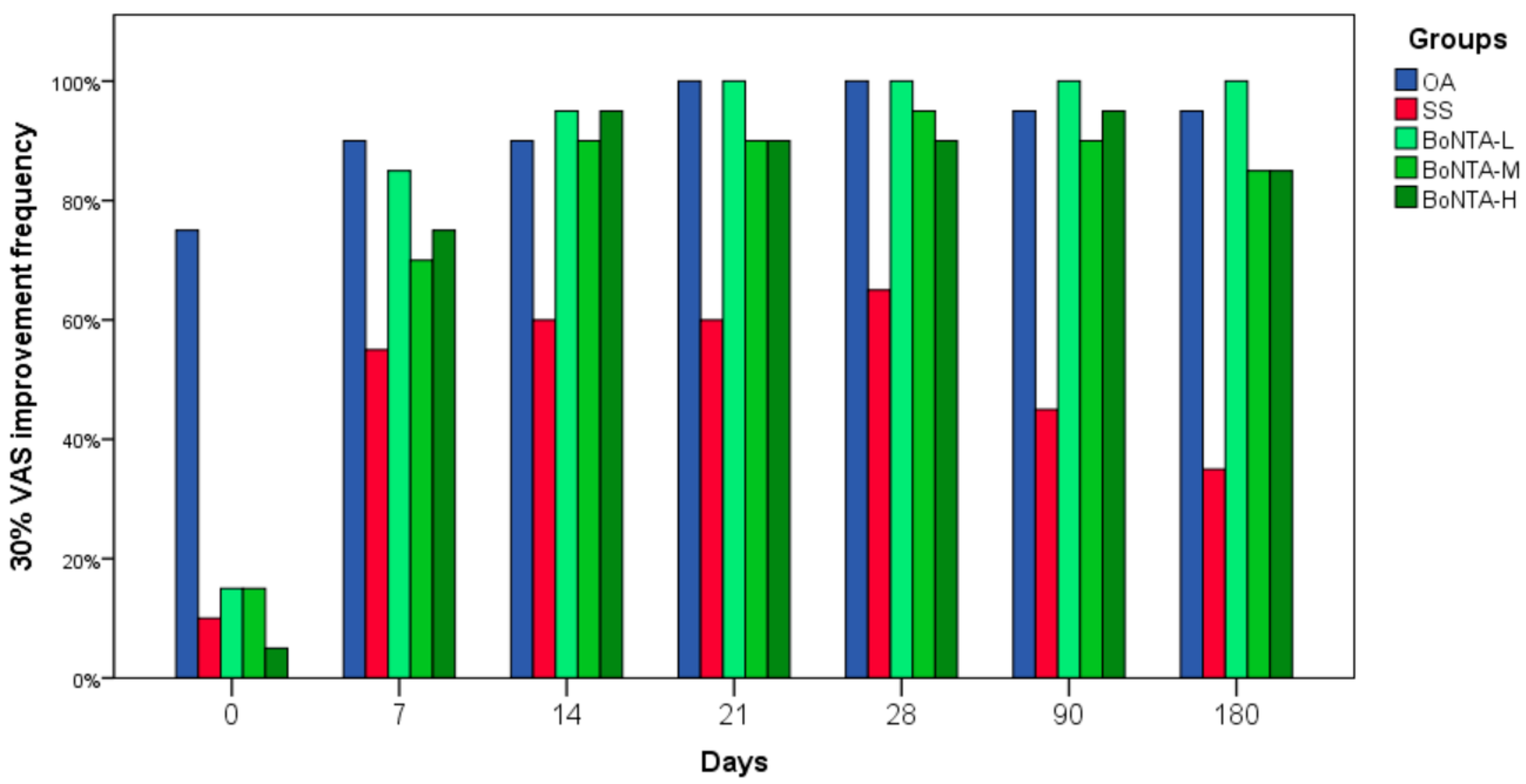
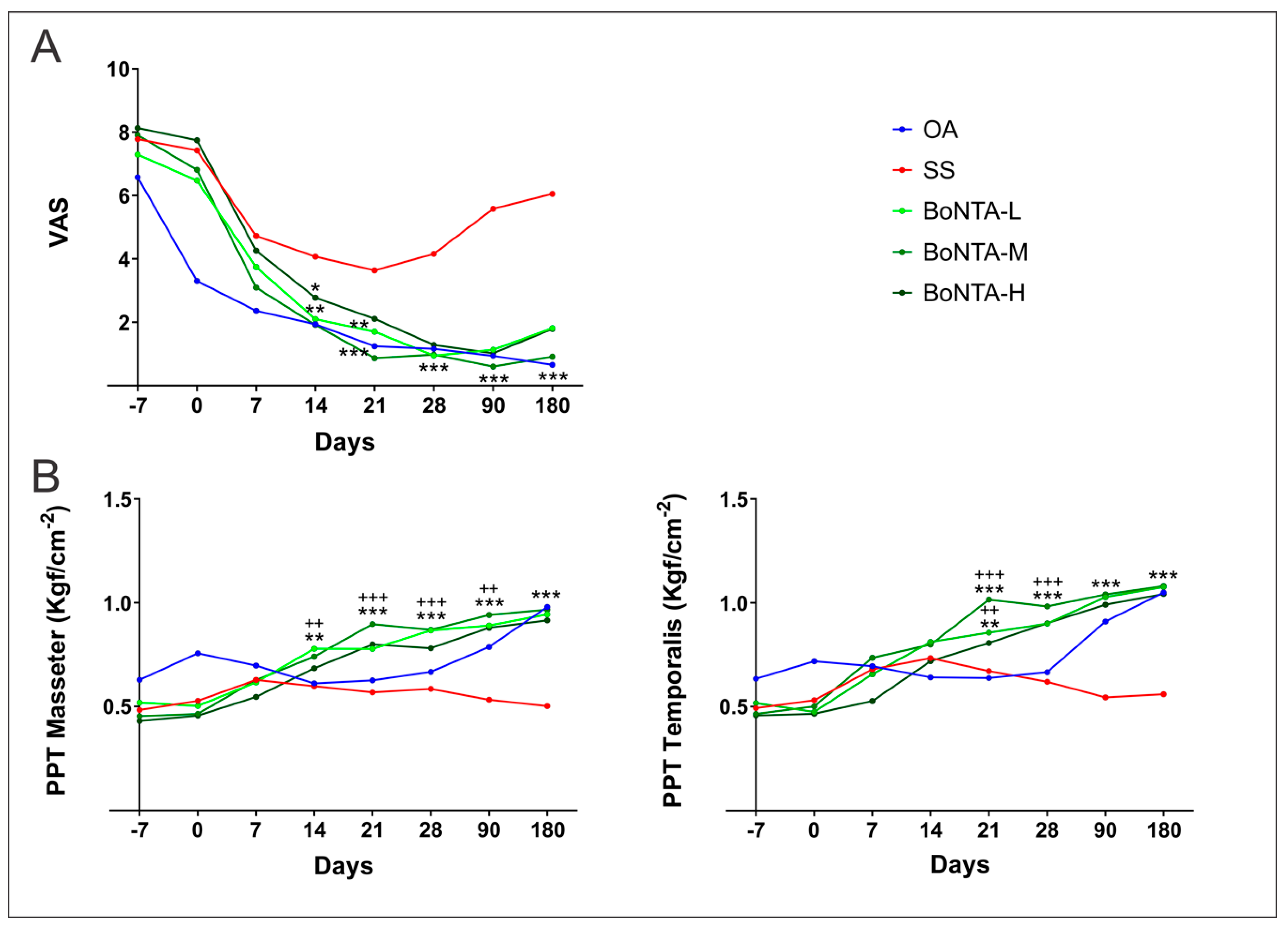
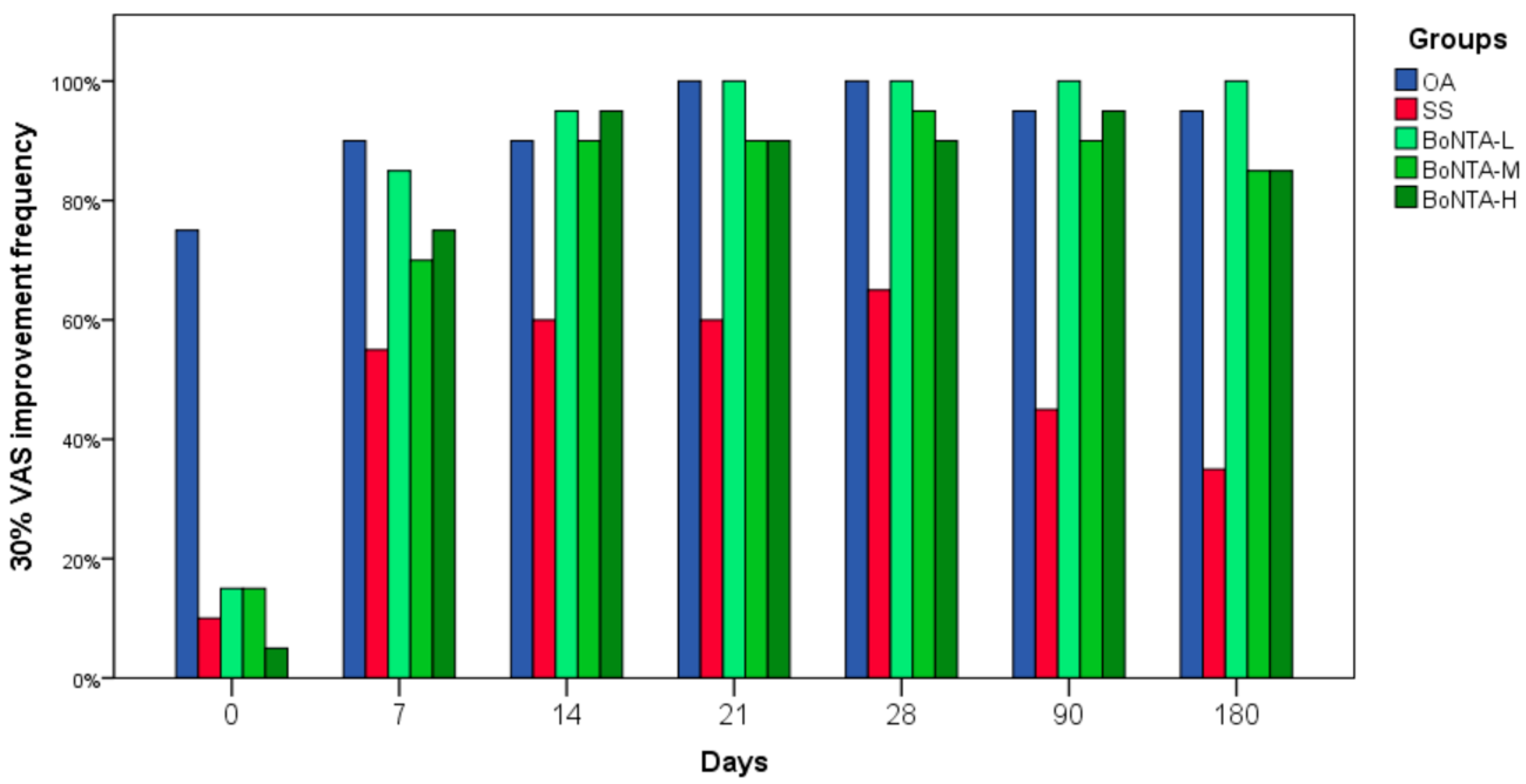
2.1. Subjective Pain (VAS)
2.2. Pressure Pain Threshold (PPT)
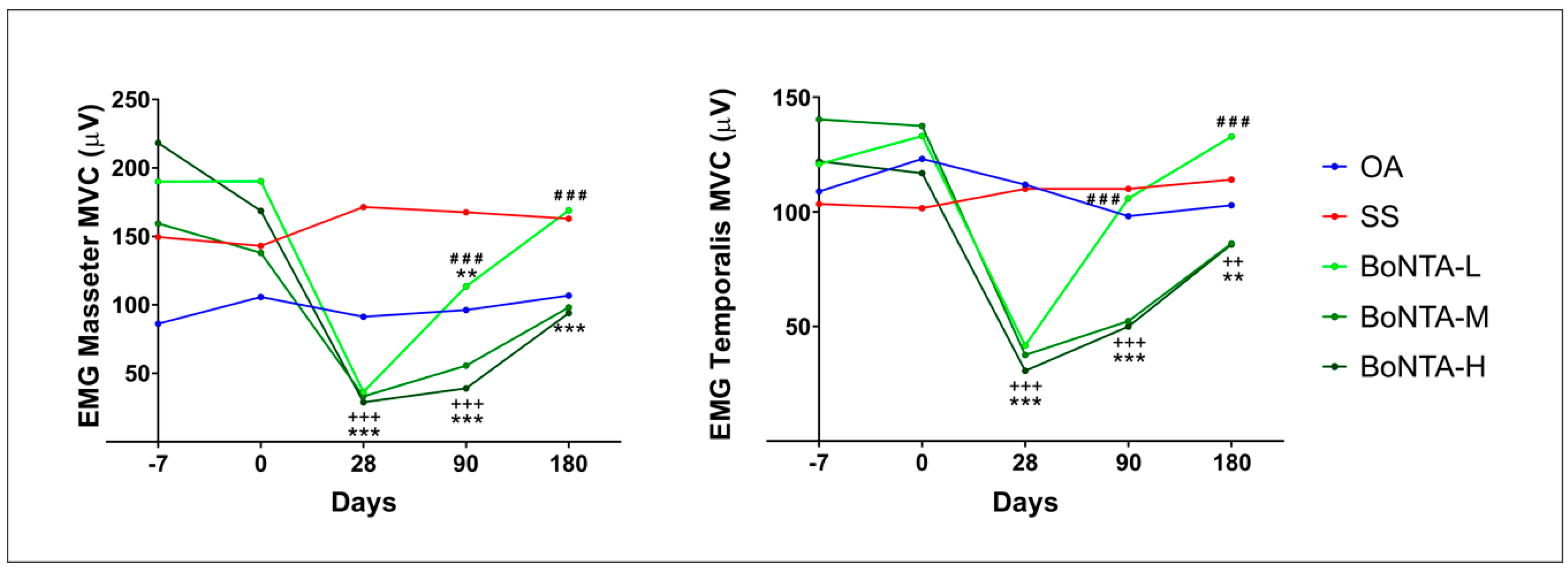
2.3. Electromyographic Activity
2.4. Masticatory Performance
2.5. Ultrasound Imaging
2.6. Cone Beam Computed Tomography
3. Discussion
4. Conclusions
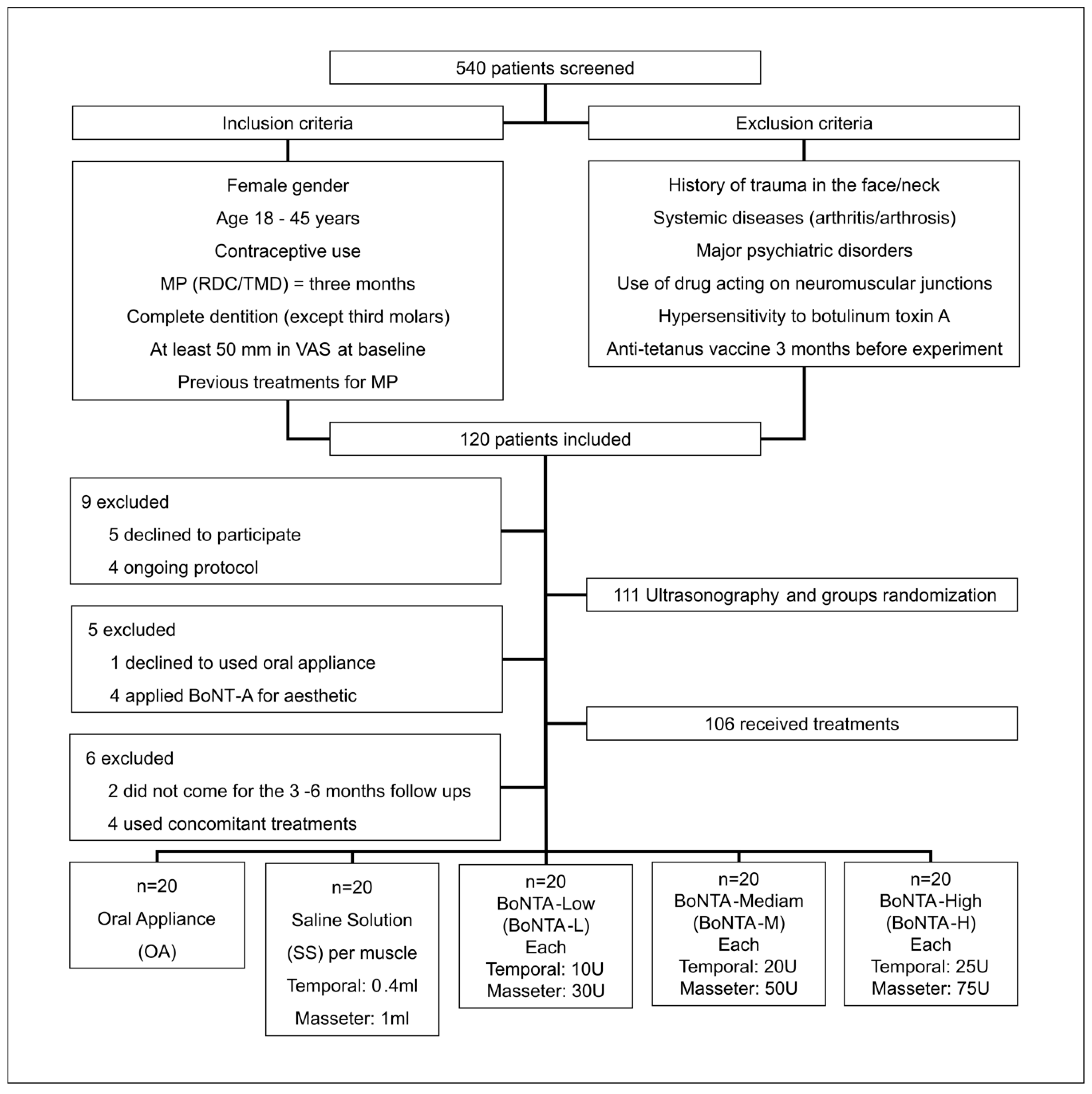
5. Methods
5.1. Subjects
5.2. Randomization
5.3. Treatments
5.3.1. Counseling (CLS)
5.3.2. Oral Appliance (OA)
5.3.3. BoNT-A and SS
5.4. Outcomes
5.4.1. Primary Outcomes
Subjective Pain: Visual Analog Scale (VAS)
Pressure Pain Threshold (PPT)
5.4.2. Secondary Outcomes
Electromyography (EMG)
Masticatory Performance (MP)
Ultrasound Imaging (UI)
Cone Beam Computed Tomography (CBCT)
5.5. Statistical Analysis
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Manfredini, D.; Ahlberg, J.; Winocur, E.; Guarda-Nardini, L.; Lobbezoo, F. Correlation of RDC/TMD axis I diagnoses and axis II pain-related disability. A multicenter study. Clin. Oral Investig. 2011, 15, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Ohrbach, R.; Dworkin, S.F. The Evolution of TMD Diagnosis: Past, Present, Future. J. Dent. Res. 2016, 95, 1093–1101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guarda-Nardini, L.; Manfredini, D.; Salamone, M.; Salmaso, S.; Tonello, S.; Ferronato, G. Efficacy of botulinum toxin in treating myofascial pain in bruxers: A controlled placebo pilot study. Cranio J. Craniomandib. Pract. 2008, 26, 126–135. [Google Scholar] [CrossRef]
- Greene, C.S. The etiology of temporomandibular disorders: Implications for treatment. J. Orofac. Pain 2001, 15, 93–105, discussion 106–16. [Google Scholar] [PubMed]
- De Laat, A.; Stappaerts, K.; Papy, S. Counseling and Physical Therapy as Treatment for Myofascial Pain of the Masticatory System. J. Orofac. Pain 2003, 17, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Dym, H.; Bowler, D.; Zeidan, J. Pharmacologic Treatment for Temporomandibular Disorders. Dent. Clin. N. Am. 2016, 60, 367–379. [Google Scholar] [CrossRef]
- Conti, P.C.R.; De Alencar, E.N.; Da Mota Corrêa, A.S.; Lauris, J.R.P.; Porporatti, A.L.; Costa, Y.M. Behavioural changes and occlusal splints are effective in the management of masticatory myofascial pain: A short-term evaluation. J. Oral Rehabil. 2012, 39, 754–760. [Google Scholar] [CrossRef]
- Matak, I.; Lackovic, Z. Botulinum toxin A, brain and pain. Prog. Neurobiol. 2014, 119–120, 39–59. [Google Scholar] [CrossRef] [Green Version]
- Muñoz-Lora, V.R.M.; Clemente-Napimoga, J.T.; Ballassini, H.; Gomes-Macedo, C.; De la Torre Canales, G.; Rizzatti- Barbosa, C.M. Botulinum toxin type A reduces inflammatory hypernociception induced by arthritis in the temporomadibular joint of rats. Toxicon 2017, 129, 52–57. [Google Scholar] [CrossRef]
- Matak, I.; Bölcskei, K.; Bach-rojecky, L.; Helyes, Z. Mechanisms of Botulinum Toxin Type A Action on Pain. Toxins 2019, 11, 459. [Google Scholar] [CrossRef] [Green Version]
- Ernberg, M.; Hedenberg-Magnusson, B.; List, T.; Svensson, P. Efficacy of botulinum toxin type A for treatment of persistent myofascial TMD pain: A randomized, controlled, double-blind multicenter study. Pain 2011, 152, 1988–1996. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.A.; Lerner, M.Z.; Blitzer, A. IncobotulinumtoxinA Injection for Temporomandibular Joint Disorder: A Randomized Controlled Pilot Study. Ann. Otol. Rhinol. Laryngol. 2017, 126, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Kurtoglu, C.; Gur, O.H.; Kurkcu, M.; Sertdemir, Y.; Guler-Uysal, F.; Uysal, H. Effect of Botulinum Toxin-A in Myofascial Pain Patients With or Without Functional Disc Displacement. J. Oral Maxillofac. Surg. 2008, 66, 1644–1651. [Google Scholar] [CrossRef] [PubMed]
- Guarda-Nardini, L.; Stecco, A.; Stecco, C.; Masiero, S.; Manfredini, D. Myofascial pain of the jaw muscles: Comparison of short-term effectiveness of botulinum toxin injections and Fascial Manipulation technique. Cranio J. Craniomandib. Pract. 2012, 30, 95–102. [Google Scholar] [CrossRef]
- Muñoz Lora, V.R.M.; Del Bel Cury, A.A.; Jabbari, B.; Lacković, Z. Botulinum Toxin Type A in Dental Medicine. J. Dent. Res. 2019, 98, 1450–1457. [Google Scholar] [CrossRef]
- Raphael, K.G.; Tadinada, A.; Bradshaw, J.M.; Janal, M.N.; Sirois, D.A.; Chan, K.C.; Lurie, A.G. Osteopenic consequences of botulinum toxin injections in the masticatory muscles: A pilot study. J. Oral Rehabil. 2014, 41, 555–563. [Google Scholar] [CrossRef]
- Lee, H.-J.; Kim, S.-J.; Lee, K.-J.; Yu, H.-S.; Baik, H.-S. Repeated injections of botulinum toxin into the masseter muscle induce bony changes in human adults: A longitudinal study. Korean J. Orthod. 2017, 47, 222–228. [Google Scholar] [CrossRef] [Green Version]
- Matthys, T.; Ho Dang, H.A.; Rafferty, K.L.; Herring, S.W. Bone and cartilage changes in rabbit mandibular condyles after 1 injection of botulinum toxin. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 999–1009. [Google Scholar] [CrossRef] [Green Version]
- Rafferty, K.L.; Liu, Z.J.; Ye, W.; Navarrete, A.L.; Nguyen, T.T.; Salamati, A.; Herring, S.W. Botulinum toxin in masticatory muscles: Short- and long-term effects on muscle, bone, and craniofacial function in adult rabbits. Bone 2012, 50, 651–662. [Google Scholar] [CrossRef] [Green Version]
- Pellett, S.; Yaksh, T.L.; Ramachandran, R. Current status and future directions of botulinum neurotoxins for targeting pain processing. Toxins 2015, 7, 4519–4563. [Google Scholar] [CrossRef]
- Purkiss, J.; Welch, M.; Doward, S.; Foster, K. Capsaicin-stimulated release of substance P from cultured dorsal root ganglion neurons: Involvement of two distinct mechanisms. Biochem. Pharmacol. 2000, 59, 1403–1406. [Google Scholar] [CrossRef]
- Bach-Rojecky, L.; Lacković, Z. Central origin of the antinociceptive action of botulinum toxin type A. Pharmacol. Biochem. Behav. 2009, 94, 234–238. [Google Scholar] [CrossRef] [Green Version]
- Matak, I.; Bach-Rojecky, L.; Filipović, B.; Lacković, Z. Behavioral and immunohistochemical evidence for central antinociceptive activity of botulinum toxin A. Neuroscience 2011, 186, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuna, S.H.; Celik, O.E.; Ozturk, O.; Golpinar, M.; Aktas, A.; Balcioglu, H.A.; Keyf, F.; Sahin, B. The effects of stabilization splint treatment on the volume of masseter muscle in sleep bruxism patients. Cranio 2018, 36, 286–293. [Google Scholar] [CrossRef]
- Dressler, D.; Saberi, F.A.; Barbosa, E.R. Botulinum toxin: Mechanisms of action. Arq. Neuropsiquiatr. 2005, 63, 180–185. [Google Scholar] [CrossRef] [Green Version]
- Park, H.U.; Kim, B.I.; Kang, S.M.; Kim, S.T.; Choi, J.H.; Ahn, H.J. Changes in masticatory function after injection of botulinum toxin type A to masticatory muscles. J. Oral Rehabil. 2013, 40, 916–922. [Google Scholar] [CrossRef]
- Tsai, C.Y.; Lin, Y.C.; Su, B.; Yang, L.Y.; Chiu, W.C. Masseter muscle fibre changes following reduction of masticatory function. Int. J. Oral Maxillofac. Surg. 2012, 41, 394–399. [Google Scholar] [CrossRef] [PubMed]
- Balanta-Melo, J.; Toro-Ibacache, V.; Torres-Quintana, M.A.; Kupczik, K.; Vega, C.; Morales, C.; Hernández-Moya, N.; Arias-Calderón, M.; Beato, C.; Buvinic, S. Early molecular response and microanatomical changes in the masseter muscle and mandibular head after botulinum toxin intervention in adult mice. Ann. Anat. 2018, 216, 112–119. [Google Scholar] [CrossRef]
- De la Torre Canales, G.; Poluha, R.L.; Lora, V.M.; Araújo Oliveira Ferreira, D.M.; Stuginski-Barbosa, J.; Bonjardim, L.R.; Cury, A.A.D.B.; Conti, P.C.R. Botulinum toxin type A applications for masticatory myofascial pain and trigeminal neuralgia: What is the evidence regarding adverse effects? Clin. Oral Investig. 2019, 23, 3411–3421. [Google Scholar] [CrossRef]
- Balanta-Melo, J.; Toro-Ibacache, V.; Kupczik, K.; Buvinic, S. Mandibular Bone Loss after Masticatory Muscles Intervention with Botulinum Toxin: An Approach from Basic Research to Clinical Findings. Toxins 2019, 11, 84. [Google Scholar] [CrossRef] [Green Version]
- Dworkin, S.F.; LeResche, L. Research diagnostic criteria for temporomandibular disorders: Review, criteria, examinations and specifications, critique. J. Craniomandib. Disord. 1992, 6, 301–355. [Google Scholar] [PubMed]
- Ferreira-Valente, M.A.; Pais-Ribeiro, J.L.; Jensen, M.P. Validity of four pain intensity rating scales. Pain 2011, 152, 2399–2404. [Google Scholar] [CrossRef]
- Isselée, H.; De Laat, A.; Bogaerts, K.; Lysens, R. Short-term reproducibility of pressure pain thresholds in masticatory muscles measured with a new algometer. J. Orofac. Pain 1998, 12, 203–209. [Google Scholar]
- Pope, G.D. Introduction to Surface Electromyography. Physiotherapy 1998, 84, 405. [Google Scholar] [CrossRef]
- De Felício, C.M.; Ferreira, C.L.P.; Medeiros, A.P.M.; Rodrigues Da Silva, M.A.M.; Tartaglia, G.M.; Sforza, C. Electromyographic indices, orofacial myofunctional status and temporomandibular disorders severity: A correlation study. J. Electromyogr. Kinesiol. 2012, 22, 266–272. [Google Scholar] [CrossRef]
- Sánchez-Ayala, A.; Vilanova, L.S.R.; Costa, M.A.; Farias-Neto, A. Reproducibility of a silicone-based test food to masticatory performance evaluation by different sieve methods. Braz. Oral Res. 2014, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castelo, P.M.; Gavião, M.B.D.; Pereira, L.J.; Bonjardim, L.R. Evaluation of changes in muscle thickness, bite force and facial asymmetry during early treatment of functional posterior crossbite. J. Clin. Pediatr. Dent. 2010, 34, 369–374. [Google Scholar] [CrossRef]
- Nejaim, Y.; Farias Gomes, A.; Valadares, C.V.; Costa, E.D.; Peroni, L.V.; Groppo, F.C.; Haiter-Neto, F. Evaluation of volume of the sphenoid sinus according to sex, facial type, skeletal class, and presence of a septum: A cone-beam computed tomographic study. Br. J. Oral Maxillofac. Surg. 2019, 57, 336–340. [Google Scholar] [CrossRef]
- Noguchi, K.; Gel, Y.R.; Brunner, E.; Konietschke, F. nparLD: An R Software Package for the Nonparametric Analysis of Longitudinal Data in Factorial Experiments. J. Stat. Softw. 2012, 50. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n |
|---|---|
| Mean age | 36.8 ± 5.6 |
| Gender: Female | 100 |
| Education | |
| Elementary school | 12 |
| High school | 39 |
| University | 49 |
| Occupation | |
| Student | 24 |
| Employed | 62 |
| Unemployed | 14 |
| Pain duration | |
| 6 months | 41 |
| 1–2 years | 37 |
| 3 or more | 22 |
| RDC/TMD diagnoses | |
| Myofascial pain | 53 |
| Myofascial pain/Arthralgia | 12 |
| Myofascial pain/Disc displacement with reduction | 27 |
| Myofascial pain/Disc displacement without reduction | 8 |
| Groups | Periods of Evaluation | ||||||
|---|---|---|---|---|---|---|---|
| 0 D | 7 D | 14 D | 21 D | 28 D | 90 D | 180 D | |
| SS | 6.17 ± 0.66 Ba | 5.84 ± 0.74 Ca | 5.76 ± 0.78 Ba | 5.67 ± 0.87 Ca | 5.69 ± 0.86 Ba | 5.09 ± 1.07 Cb | 4.97 ± 1.10 Bb |
| BoNTA-L | 5.50 ± 0.89 Aab | 6.14 ± 0.71 CBc | 6.09 ± 0.64 Bc | 6.13 ± 0.76 CBc | 6.20 ± 0.44 Ac | 5.53 ± 0.70 BCb | 5.07 ± 0.80 Ba |
| BoNTA-M | 5.93 ± 0.88 ABa | 6.84 ± 0.50 Abc | 6.94 ± 0.59 Ac | 6.77 ± 0.70 Abc | 6.65 ± 0.61Ac | 6.28 ± 0.79 BCb | 6.19 ± 0.74 Aa |
| BoNTA-H | 5.94 ± 0.83 ABa | 6.42 ± 0.63 ABbc | 6.62 ± 0.49 Ab | 6.65 ± 0.58 ABb | 6.43 ± 0.66 Ab | 6.07 ± 0.72 ABac | 5.85 ± 0.88 Aa |
| Muscle/Groups | Periods of Evaluation | ||
|---|---|---|---|
| 0 D | 30 D | 90 D | |
| Temporalis in MVC | |||
| Saline solution | 2.45 ± 1.05 Aa | 2.45 ± 1.27 Aa | 2.57 ± 1.51 Aa |
| BoNTA-Low | 2.32 ± 0.71 Aa | 1.70 ± 0.65 ABb | 1.70 ± 0.59 ABb |
| BoNTA-Medium | 2.13 ± 0.88 Aa | 1.40 ± 0.55 Bb | 1.47 ± 0.62 Bb |
| BoNTA-High | 1.99 ± 0.82 Aa | 1.54 ± 0.71 Ba | 1.41 ± 0.43 Ba |
| Masseter in MVC | |||
| Saline solution | 11.70 ± 1.88 Aa | 12.04 ± 2.11 Aa | 12.09 ± 1.79 Aa |
| BoNTA-Low | 12.37 ± 1.75 Aa | 11.75 ± 1.47 ABb | 11.6 ± 1.70 ABb |
| BoNTA-Medium | 11.90 ± 1.55 Aa | 9.88 ± 1.83 Bb | 10.49 ± 1.72 Bb |
| BoNTA-High | 12.34 ± 1.68 Aa | 10.44 ± 1.26 Bb | 11.38 ± 1.67 Bb |
| Mandible Structures/Groups | Periods of Evaluation | |
|---|---|---|
| 0 D | 90 D | |
| Mandible head | ||
| Saline solution | 1249.91 ± 377.28 Aa | 1257.23 ± 396.93 Aa |
| BoNTA-Low | 1495,79 ± 491,02 Aa | 1508,54 ± 478,23 Aa |
| BoNTA-Medium | 1573,31 ± 418,47 Aa | 1580,88 ± 407,53 Aa |
| BoNTA-High | 1516,46 ± 429,90 Aa | 1483,69 ± 405,61 Bb |
| Coronoid Process | ||
| Saline solution | 217.2 ± 77.28 Aa | 210.9 ± 50.6 Aa |
| BoNTA-Low | 213.6 ± 122.3 Aa | 203.1 ± 213.8 Aa |
| BoNTA-Medium | 195.6 ± 118.1 Aa | 164.3 ± 135.9 Bb |
| BoNTA-High | 207.9 ± 108.7 Aa | 189.2 ± 93.8 Bb |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De la Torre Canales, G.; Alvarez-Pinzon, N.; Muñoz-Lora, V.R.M.; Vieira Peroni, L.; Farias Gomes, A.; Sánchez-Ayala, A.; Haiter-Neto, F.; Manfredini, D.; Rizzatti-Barbosa, C.M. Efficacy and Safety of Botulinum Toxin Type A on Persistent Myofascial Pain: A Randomized Clinical Trial. Toxins 2020, 12, 395. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12060395
De la Torre Canales G, Alvarez-Pinzon N, Muñoz-Lora VRM, Vieira Peroni L, Farias Gomes A, Sánchez-Ayala A, Haiter-Neto F, Manfredini D, Rizzatti-Barbosa CM. Efficacy and Safety of Botulinum Toxin Type A on Persistent Myofascial Pain: A Randomized Clinical Trial. Toxins. 2020; 12(6):395. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12060395
Chicago/Turabian StyleDe la Torre Canales, Giancarlo, Natalia Alvarez-Pinzon, Victor Ricardo Manuel Muñoz-Lora, Leonardo Vieira Peroni, Amanda Farias Gomes, Alfonso Sánchez-Ayala, Francisco Haiter-Neto, Daniele Manfredini, and Célia Marisa Rizzatti-Barbosa. 2020. "Efficacy and Safety of Botulinum Toxin Type A on Persistent Myofascial Pain: A Randomized Clinical Trial" Toxins 12, no. 6: 395. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12060395