Circulating p-Cresyl Sulfate, Non-Hepatic Alkaline Phosphatase and Risk of Bone Fracture Events in Chronic Kidney Disease-Mineral Bone Disease

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Results
2.1. Age, Prevalence of DM, HD Vintage, Kt/V Urea, PCS, NHALP, Normalized Protein Catabolic Rate, Albumin, Phosphate, iPTH, Hemoglobin and Hematocrit Levels Were Significantly Different Between BF Event and Event-Free Groups
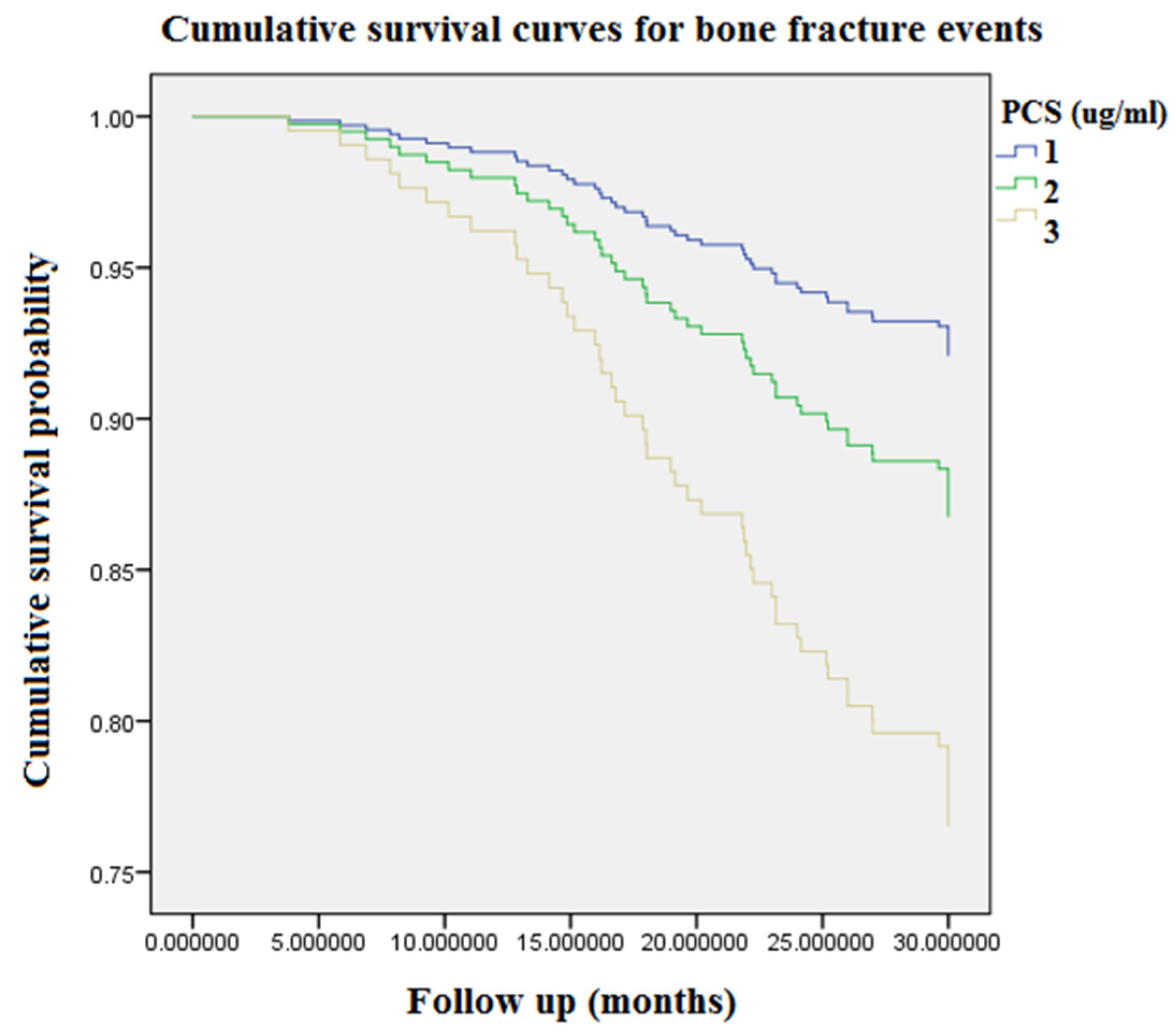
2.2. BF Event Rates, Kt/V Urea, NHALP, Albumin, Blood Urea Nitrogen, Calcium and iPTH Levels Were Significantly Different among PCS Tertile Groups
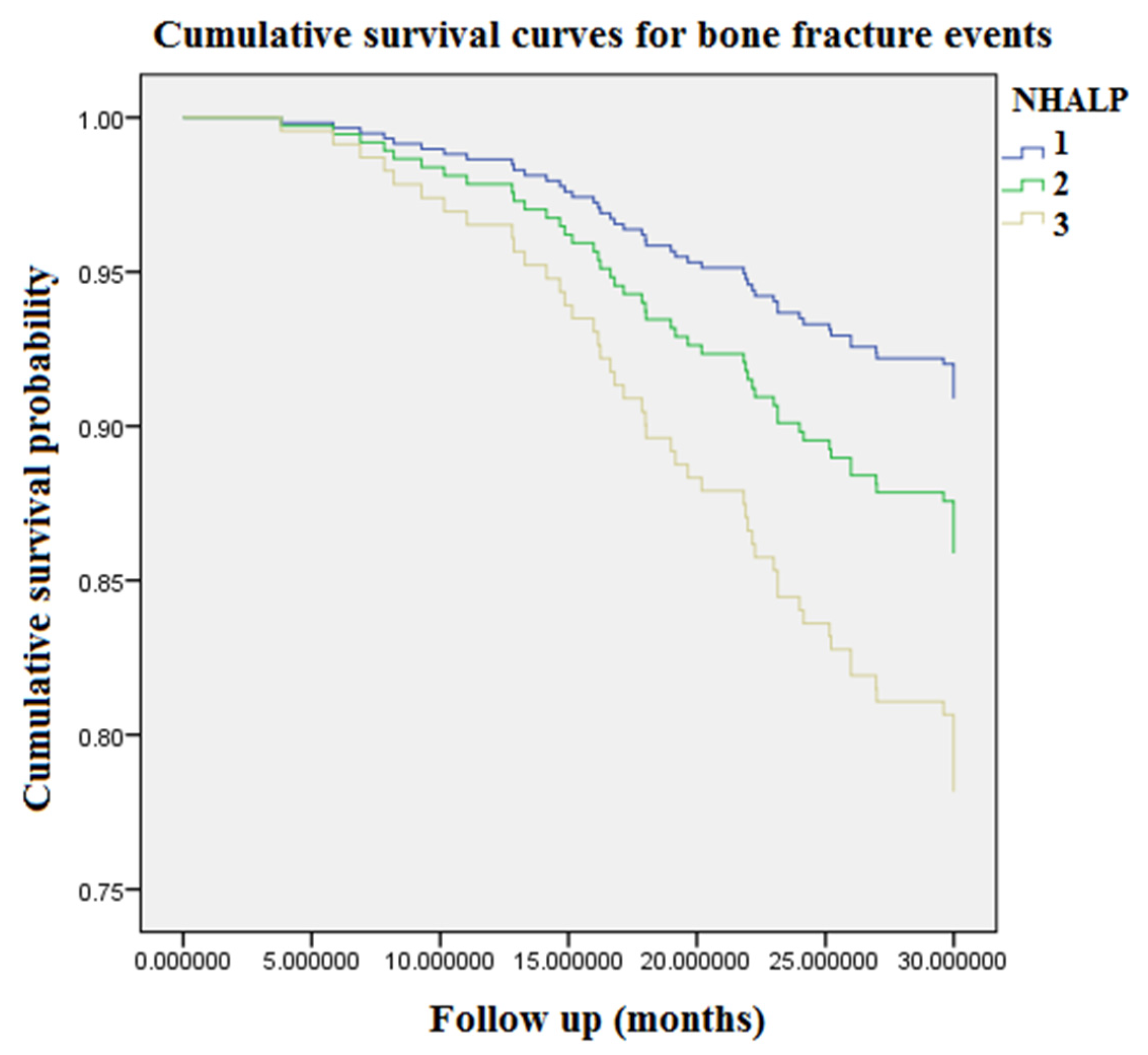
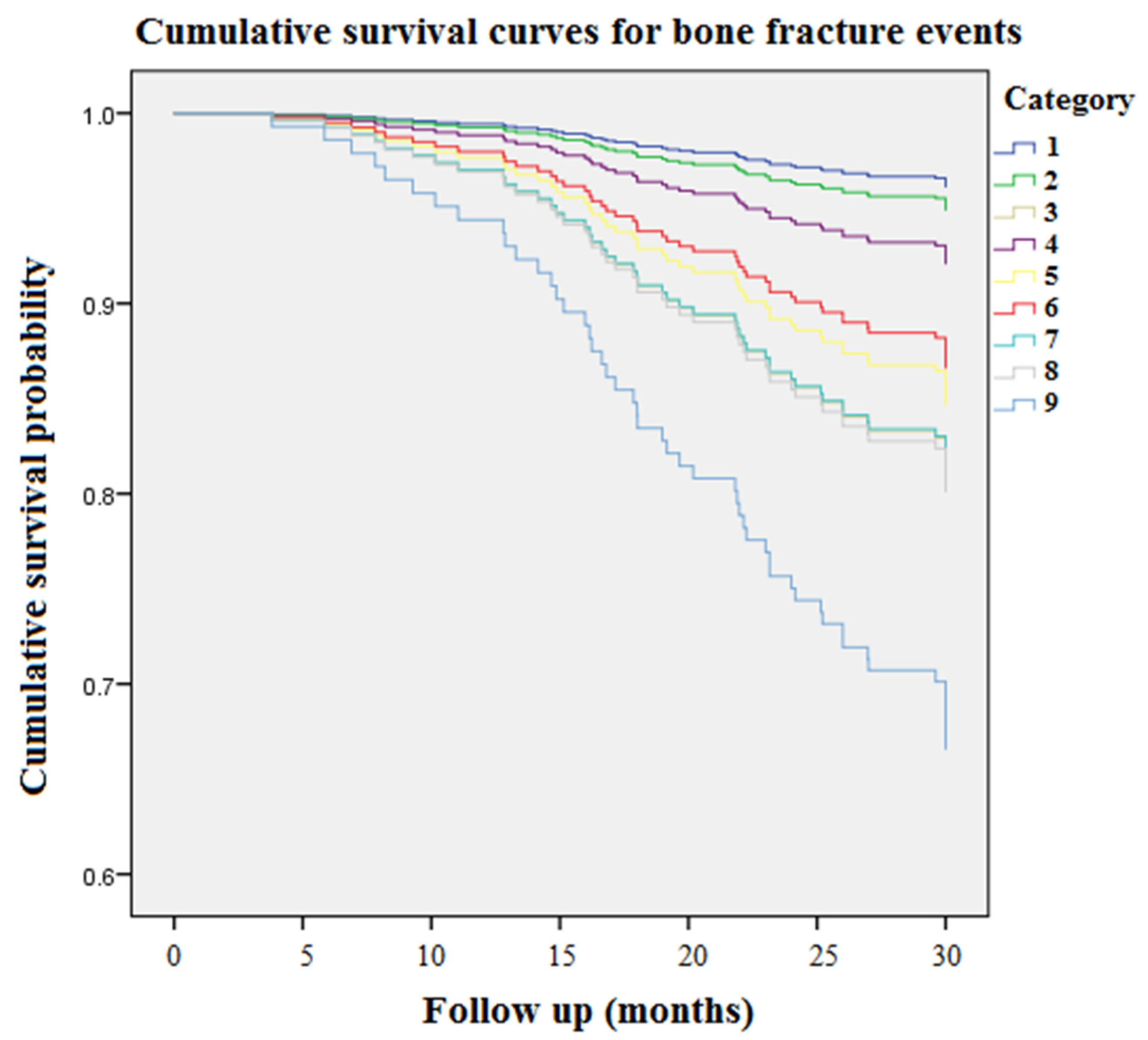
2.3. The Highest Concentration Tertiles of PCS and NHALP Are Related to an Incremental Risk of BFs
2.4. In Multivariate Cox Regression Analysis, the Associations between the Highest PCS Tertile and Risk of BF Events Remain Robust
3. Discussion
4. Methods
4.1. Participants in the Cohort
4.2. Assessment of Outcomes
4.3. Measurement of Circulating PCS Levels
4.4. Assessment of Covariates
4.5. Statistics
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Isakova, T.; Nickolas, T.L.; Denburg, M.; Yarlagadda, S.; Weiner, D.E.; Gutiérrez, O.M.; Bansal, V.; Rosas, S.E.; Nigwekar, S.; Yee, J.; et al. KDOQI US Commentary on the 2017 KDIGO Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Am. J. Kidney Dis. 2017, 70, 737–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hung, K.C.; Chang, J.F.; Hsu, Y.H.; Hsieh, C.Y.; Wu, M.S.; Wu, M.Y.; Chiu, I.J.; Syu, R.S.; Wang, T.M.; Wu, C.C.; et al. Therapeutic Effect of Calcimimetics on Osteoclast-Osteoblast Crosslink in Chronic Kidney Disease and Mineral Bone Disease. Int. J. Mol. Sci. 2020, 21, 8712. [Google Scholar] [CrossRef]
- Six, I.; Flissi, N.; Lenglet, G.; Louvet, L.; Kamel, S.; Gallet, M.; Massy, Z.A.; Liabeuf, S. Uremic Toxins and Vascular Dysfunction. Toxins 2020, 12, 404. [Google Scholar] [CrossRef] [PubMed]
- Vervloet, M. Modifying Phosphate Toxicity in Chronic Kidney Disease. Toxins 2019, 11, 522. [Google Scholar] [CrossRef] [Green Version]
- Gryp, T.; Vanholder, R.; Vaneechoutte, M.; Glorieux, G. p-Cresyl Sulfate. Toxins 2017, 9, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, J.F.; Hsieh, C.Y.; Liou, J.C.; Liu, S.H.; Hung, C.F.; Lu, K.C.; Lin, C.C.; Wu, C.C.; Ka, S.M.; Wen, L.L.; et al. Scavenging Intracellular ROS Attenuates p-Cresyl Sulfate-Triggered Osteogenesis through MAPK Signaling Pathway and NF-κB Activation in Human Arterial Smooth Muscle Cells. Toxins 2020, 12, 472. [Google Scholar] [CrossRef]
- Hénaut, L.; Mary, A.; Chillon, J.M.; Kamel, S.; Massy, Z.A. The Impact of Uremic Toxins on Vascular Smooth Muscle Cell Function. Toxins 2018, 10, 218. [Google Scholar] [CrossRef] [Green Version]
- Lim, Y.J.; Sidor, N.A.; Tonial, N.C.; Che, A.; Urquhart, B.L. Uremic Toxins in the Progression of Chronic Kidney Disease and Cardiovascular Disease: Mechanisms and Therapeutic Targets. Toxins 2021, 13, 142. [Google Scholar] [CrossRef]
- Kazama, J.J.; Iwasaki, Y.; Fukagawa, M. Uremic osteoporosis. Kidney Int. Suppl. 2013, 3, 446–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwasaki, Y.; Kazama, J.J.; Yamato, H.; Matsugaki, A.; Nakano, T.; Fukagawa, M. Altered material properties are responsible for bone fragility in rats with chronic kidney injury. Bone 2015, 81, 247–254. [Google Scholar] [CrossRef]
- Black, A.P.; Cardozo, L.F.; Mafra, D. Effects of Uremic Toxins from the Gut Microbiota on Bone: A Brief Look at Chronic Kidney Disease. Ther. Apher. Dial. 2015, 19, 436–440. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, S.; Fukagawa, M. Uremic Toxicity and Bone in CKD. J. Nephrol. 2017, 30, 623–627. [Google Scholar] [CrossRef] [PubMed]
- Yeh, J.C.; Wu, C.C.; Choy, C.S.; Chang, S.W.; Liou, J.C.; Chen, K.S.; Tung, T.H.; Lin, W.N.; Hsieh, C.Y.; Ho, C.T.; et al. Non-Hepatic Alkaline Phosphatase, hs-CRP and Progression of Vertebral Fracture in Patients with Rheumatoid Arthritis: A Population-Based Longitudinal Study. J. Clin. Med. 2018, 7, 439. [Google Scholar] [CrossRef] [Green Version]
- Haarhaus, M.; Brandenburg, V.; Kalantar-Zadeh, K.; Stenvinkel, P.; Magnusson, P. Alkaline phosphatase: A novel treatment target for cardiovascular disease in CKD. Nat. Rev. Nephrol. 2017, 13, 429–442. [Google Scholar] [CrossRef] [PubMed]
- Pimentel, A.; Ureña-Torres, P.; Zillikens, M.C.; Bover, J.; Cohen-Solal, M. Fractures in patients with CKD-diagnosis, treatment, and prevention: A review by members of the European Calcified Tissue Society and the European Renal Association of Nephrology Dialysis and Transplantation. Kidney In.t 2017, 92, 1343–1355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pimentel, A.; Ureña-Torres, P.; Bover, J.; Luis Fernandez-Martín, J.; Cohen-Solal, M. Bone Fragility Fractures in CKD Patients. Calcif. Tissue Int. 2021, 108, 539–550. [Google Scholar] [CrossRef]
- Pimentel, A.; Bover, J.; Elder, G.; Cohen-Solal, M.; Ureña-Torres, P.A. The Use of Imaging Techniques in Chronic Kidney Disease-Mineral and Bone Disorders (CKD-MBD)-A Systematic Review. Diagnostics 2021, 11, 772. [Google Scholar] [CrossRef] [PubMed]
- Tentori, F.; McCullough, K.; Kilpatrick, R.D.; Bradbury, B.D.; Robinson, B.M.; Kerr, P.G.; Pisoni, R.L. High rates of death and hospitalization follow bone fracture among hemodialysis patients. Kidney Int. 2014, 85, 166–173. [Google Scholar] [CrossRef] [Green Version]
- Naylor, K.L.; Garg, A.X.; Zou, G.; Langsetmo, L.; Leslie, W.D.; Fraser, L.A.; Adachi, J.D.; Morin, S.; Goltzman, D.; Lentle, B.; et al. Comparison of fracture risk prediction among individuals with reduced and normal kidney function. Clin. J. Am. Soc. Nephrol. 2015, 10, 646–653. [Google Scholar] [CrossRef] [Green Version]
- Nii-Kono, T.; Iwasaki, Y.; Uchida, M.; Fujieda, A.; Hosokawa, A.; Motojima, M.; Yamato, H.; Kurokawa, K.; Fukagawa, M. Indoxyl sulfate induces skeletal resistance to parathyroid hormone in cultured osteoblastic cells. Kidney Int. 2007, 71, 738–743. [Google Scholar] [CrossRef] [Green Version]
- Liu, W.C.; Wu, C.C.; Lim, P.S.; Chien, S.W.; Hou, Y.C.; Zheng, C.M.; Shyu, J.F.; Lin, Y.F.; Lu, K.C. Effect of uremic toxin-indoxyl sulfate on the skeletal system. Clin. Chim. Acta 2018, 484, 197–206. [Google Scholar] [CrossRef]
- Bezerra de Carvalho, K.S.; Vasco, R.F.V.; Custodio, M.R.; Jorgetti, V.; Moysés, R.M.A.; Elias, R.M. Chronic kidney disease is associated with low BMD at the hip but not at the spine. Osteoporos. Int. 2019, 30, 1015–1023. [Google Scholar] [CrossRef]
- Hsu, C.Y.; Chen, L.R.; Chen, K.H. Osteoporosis in Patients with Chronic Kidney Diseases: A Systemic Review. Int. J. Mol. Sci. 2020, 21, 6846. [Google Scholar] [CrossRef]
- Ketteler, M.; Block, G.A.; Evenepoel, P.; Fukagawa, M.; Herzog, C.A.; McCann, L.; Moe, S.M.; Shroff, R.; Tonelli, M.A.; Toussaint, N.D.; et al. Executive summary of the 2017 KDIGO Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD) Guideline Update: What’s changed and why it matters. Kidney Int. 2017, 92, 26–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nam, M.; Huh, J.E.; Kim, M.S.; Ryu, D.H.; Park, J.; Kim, H.S.; Lee, S.Y.; Hwang, G.S. Metabolic alterations in the bone tissues of aged osteoporotic mice. Sci. Rep. 2018, 8, 8127. [Google Scholar] [CrossRef] [PubMed]
- Vanholder, R.; Pletinck, A.; Schepers, E.; Glorieux, G. Biochemical and Clinical Impact of Organic Uremic Retention Solutes: A Comprehensive Update. Toxins 2018, 10, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujii, H.; Goto, S.; Fukagawa, M. Role of Uremic Toxins for Kidney, Cardiovascular, and Bone Dysfunction. Toxins 2018, 10, 202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamza, E.; Metzinger, L.; Metzinger-Le Meuth, V. Uremic Toxins Affect Erythropoiesis during the Course of Chronic Kidney Disease: A Review. Cells 2020, 9, 2039. [Google Scholar] [CrossRef]
- Chang, J.F.; Chen, P.C.; Hsieh, C.Y.; Liou, J.C. A Growth Differentiation Factor 15-Based Risk Score Model to Predict Mortality in Hemodialysis Patients. Diagnostics 2021, 11, 286. [Google Scholar] [CrossRef]
- Chang, J.F.; Chou, Y.S.; Wu, C.C.; Chen, P.C.; Ko, W.C.; Liou, J.C.; Hsieh, C.Y.; Lin, W.N.; Wen, L.L.; Chang, S.W.; et al. A Joint Evaluation of Neurohormone Vasopressin-Neurophysin II-Copeptin and Aortic Arch Calcification on Mortality Risks in Hemodialysis Patients. Front. Med. 2020, 7, 102. [Google Scholar] [CrossRef] [Green Version]
- Chang, J.F.; Liu, S.H.; Lu, K.C.; Ka, S.M.; Hsieh, C.Y.; Ho, C.T.; Lin, W.N.; Wen, L.L.; Liou, J.C.; Chang, S.W.; et al. Uremic Vascular Calcification Is Correlated With Oxidative Elastic Lamina Injury, Contractile Smooth Muscle Cell Loss, Osteogenesis, and Apoptosis: The Human Pathobiological Evidence. Front. Med. 2020, 7, 78. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Overall Population (n = 352) | BF Events (n = 51) | Event-Free Survivors (n = 301) | |
|---|---|---|---|
| Age (years) | 64.6 ± 9.3 | 69.9 ± 7.7 | 63.7 ± 9.3 |
| Male, n (%) | 181 (51.4) | 25 (49.0) | 156 (51.8) |
| Diabetes mellitus, n (%) | 160 (45.5) | 34 (66.7) | 126 (41.9) |
| Hypertension, n (%) | 180 (51.1) | 22 (43.1) | 158 (52.5) |
| Hemodialysis vintage (months) | 42 (18.9–80.9) | 75.8 (58.7–129.2) | 34.2 (17.1–76.0) |
| Kt/V urea | 1.5 ± 0.3 | 1.4 ± 0.3 | 1.5 ± 0.3 |
| PCS (μg/mL) | 20.9 ± 15.0 | 33.4 ± 21.0 | 18.8 ± 12.7 |
| NHALP (IU/L) | 86.3 ± 54.9 | 117.6 ± 86.8 | 81.0 ± 45.6 |
| nPCR | 1.1 ± 0.2 | 1.0 ± 0.2 | 1.1 ± 0.2 |
| Aspartate aminotransferase (IU/L) | 16.0 ± 6.7 | 15.6 ± 5.8 | 16.1 ± 6.9 |
| Alanine aminotransferase (IU/L) | 13.0 ± 9.9 | 15.0 ± 14.3 | 12.7 ± 8.9 |
| Total cholesterol (mg/dL) | 193.4 ± 48.0 | 202.8 ± 45.2 | 191.8 ± 48.3 |
| Triglyceride (mg/dL) | 206.5 ± 180.5 | 239.3 ± 181.3 | 200.9 ± 180.1 |
| Low-density lipoprotein | 106.1 ± 38.1 | 112.3 ± 40.2 | 105.0 ± 37.7 |
| Blood glucose (mg/dL) | 125.8 ± 60.1 | 134.3 ± 69.8 | 124.3 ± 58.3 |
| Blood urea nitrogen (mg/dL) | 59.7 ± 17.4 | 61.3 ± 19.2 | 59.4 ± 17.1 |
| Creatinine (mg/dL) | 10.2 ± 1.8 | 9.9 ± 1.6 | 10.3 ± 1.9 |
| Uric acid (mg/dL) | 7.4 ± 1.3 | 7.2 ± 0.9 | 7.5 ± 1.4 |
| Potassium (mmol L−1) | 4.5 ± 0.9 | 4.4 ± 0.7 | 4.6 ± 0.9 |
| Phosphate (mg/dL) | 5.2 ± 1.5 | 6.0 ± 1.5 | 5.0 ± 1.4 |
| Albumin (g/dL) | 3.9 ± 0.4 | 3.8 ± 0.5 | 3.9 ± 0.4 |
| Calcium (mg/dL) | 9.2 ± 0.7 | 9.2 ± 0.8 | 9.2 ± 0.7 |
| iPTH (pg/mL) | 236.5 (118.0–409.0) | 745.0 (628.0–925.0) | 201 (105.0–319.5) |
| Hemoglobin (g/dL) | 10.7 ± 1.4 | 10.2 ± 1.2 | 10.8 ± 1.5 |
| Hematocrit (%) | 33.1 ± 4.0 | 31.4 ± 4.1 | 31.5 ± 3.8 |
| Tertile 1 <16 μg/mL | Tertile 2 16–26.8 μg/mL | Tertile 3 >26.8 pg/mL | |
|---|---|---|---|
| Patients, n (%) | 126 (35.8) | 114 (32.4) | 112 (31.8) |
| BF events, n (%) | 10 (7.9) | 15 (13.2) | 26 (23.2) |
| Annual BF rates (%) | 3.4 | 5.6 | 9.8 |
| Age (years) | 64.1 ± 8.9 | 64.2 ± 9.0 | 65.6 ± 10.0 |
| Diabetes mellitus, n (%) | 58 (46.0) | 48 (42.1) | 54 (48.2) |
| Hypertension, n (%) | 60 (47.6) | 56 (49.1) | 64 (57.1) |
| Hemodialysis vintage (months) | 41.8 (20.2–71.4) | 51.7 (16.6–93.3) | 37.3 (20.2–89.5) |
| PCS (μg/mL) | 5.6 ± 4.4 | 22.1 ± 2.4 | 37.0 ± 12.5 |
| Kt/V urea | 1.5 ± 0.3 | 1.5 ± 0.3 | 1.4 ± 0.3 |
| NHALP | 65.6 ± 37.7 | 86.5 ± 27.6 | 109.4 ± 78.4 |
| nPCR (g/kg/day) | 1.1 ± 0.2 | 1.0 ± 0.3 | 1.1 ± 0.2 |
| Potassium (mmol L−1) | 4.6 ± 0.8 | 4.5 ± 0.9 | 4.5 ± 0.8 |
| Blood urea nitrogen (mg/dL) | 57.2 ± 15.2 | 59.5 ± 20.5 | 62.8 ± 16.0 |
| Creatinine (mg/dL) | 10.2 ± 1.8 | 10.5 ± 1.9 | 10.3 ± 1.6 |
| Blood glucose (mg/dL) | 130.0 ± 62.1 | 135.8 ± 79.8 | 135.6 ± 68.4 |
| Uric acid (mg/dL) | 7.6 ± 1.4 | 7.2 ± 1.0 | 7.5 ± 1.4 |
| Calcium (mg/dL) | 9.3 ± 0.9 | 9.2 ± 0.6 | 9.0 ± 0.6 |
| Phosphate (mg/dL) | 5.0 ± 1.5 | 5.1 ± 1.4 | 5.4 ± 1.4 |
| Albumin (g/dL) | 3.8 ± 0.4 | 4.0 ± 0.4 | 4.0 ± 0.4 |
| Intact parathyroid hormone (pg/mL) | 96.0 (53.2–139.0) | 224.0 (175.0–293.0) | 413.5 (341.0–552.0) |
| Hemoglobin (g/dL) | 10.8 ± 1.8 | 10.8 ± 1.2 | 10.4 ± 1.0 |
| Hematocrit (%) | 33.5 ± 5.7 | 33.5 ± 3.8 | 32.3 ± 3.2 |
| Model 1 | Model 2 | |
|---|---|---|
| HR (95% CI) p Value | HR (95% CI) p Value | |
| PCS Tertiles Tertile 3 vs. Tertile 1 | 3.25 (1.57–6.73) < 0.01 | 2.87 (1.02–8.09) < 0.05 |
| Diabetes mellitus (yes vs. no) | 2.61 (1.46–2.68) < 0.01 | 1.49 (0.76–2.95) 0.25 |
| NHALP (per 10 unit increase) | 1.09 (1.05–1.12) < 0.01 | 1.06 (1.01–1.11) < 0.01 |
| Age (per year increase) | 1.05 (1.00–1.10) < 0.05 | 1.06 (1.02–1.11) < 0.05 |
| Albumin (per unit increase) | 0.53 (0.30–0.95) < 0.05 | 0.81 (0.35–1.87) 0.62 |
| HD vintage (per month increase) | 1.02 (1.01–1.03) < 0.01 | 1.01 (1.00–1.02) < 0.05 |
| Phosphate (per unit increase) | 1.40 (1.19–1.64) < 0.01 | 1.48 (1.26–1.92) < 0.05 |
| iPTH (per 10 unit increase) | 1.02 (1.02–1.03) < 0.01 | 1.03 (1.02–1.03) < 0.01 |
| Hemoglobin (per unit increase) | 0.77 (0.63–0.93) < 0.01 | 0.82 (0.62–1.10) 0.18 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, J.-F.; Hsieh, C.-Y.; Liou, J.-C.; Lu, K.-C.; Zheng, C.-M.; Wu, M.-S.; Chang, S.-W.; Wang, T.-M.; Wu, C.-C. Circulating p-Cresyl Sulfate, Non-Hepatic Alkaline Phosphatase and Risk of Bone Fracture Events in Chronic Kidney Disease-Mineral Bone Disease. Toxins 2021, 13, 479. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13070479
Chang J-F, Hsieh C-Y, Liou J-C, Lu K-C, Zheng C-M, Wu M-S, Chang S-W, Wang T-M, Wu C-C. Circulating p-Cresyl Sulfate, Non-Hepatic Alkaline Phosphatase and Risk of Bone Fracture Events in Chronic Kidney Disease-Mineral Bone Disease. Toxins. 2021; 13(7):479. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13070479
Chicago/Turabian StyleChang, Jia-Feng, Chih-Yu Hsieh, Jian-Chiun Liou, Kuo-Cheng Lu, Cai-Mei Zheng, Mai-Szu Wu, Shu-Wei Chang, Ting-Ming Wang, and Chang-Chin Wu. 2021. "Circulating p-Cresyl Sulfate, Non-Hepatic Alkaline Phosphatase and Risk of Bone Fracture Events in Chronic Kidney Disease-Mineral Bone Disease" Toxins 13, no. 7: 479. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13070479