Evaluation of Salivary Indoxyl Sulfate with Proteinuria for Predicting Graft Deterioration in Kidney Transplant Recipients

 , and
, and
Abstract
:1. Introduction
2. Results
2.1. Baseline Patients’ Characteristics
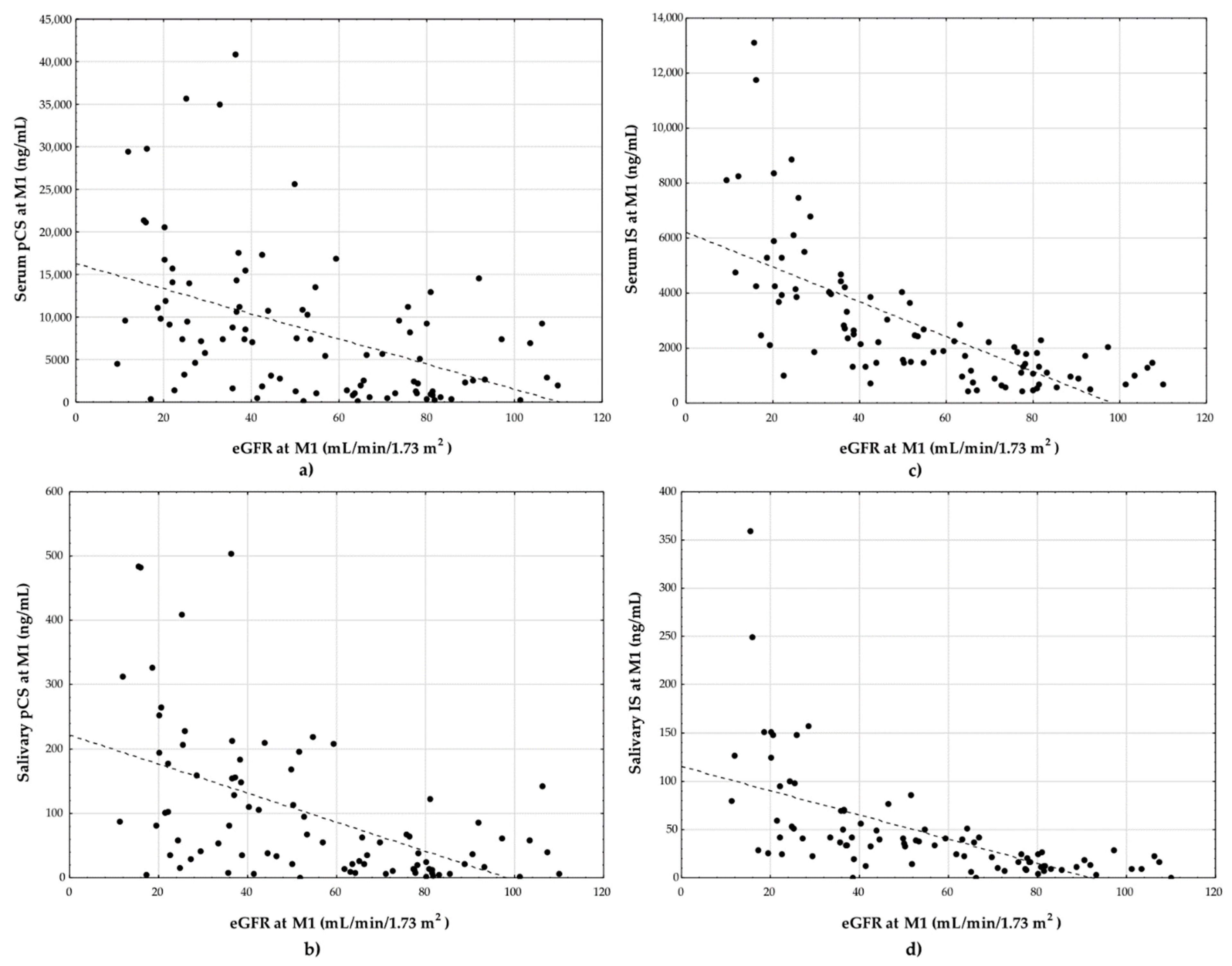
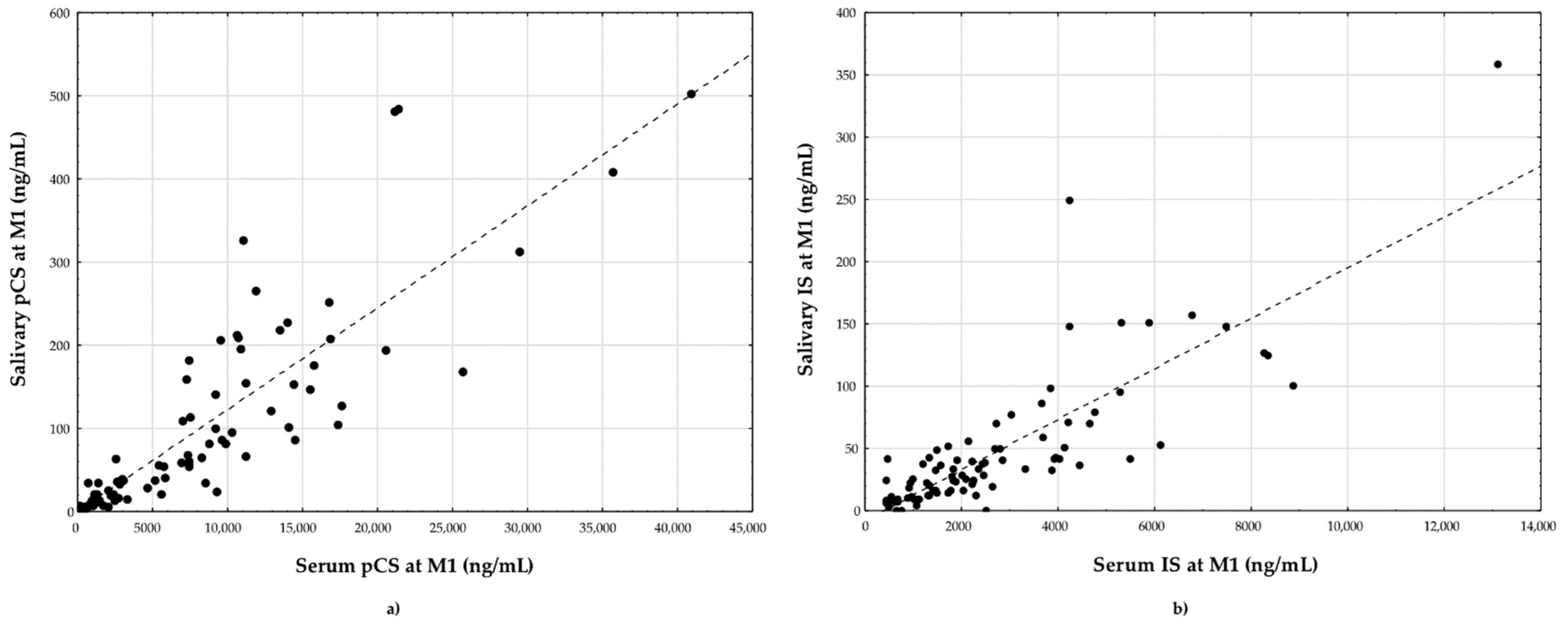
2.2. Evaluation of Graft Function—eGFR, Salivary and Serum pCS and IS
2.3. Analysis of Risk Factors for Graft Deterioration
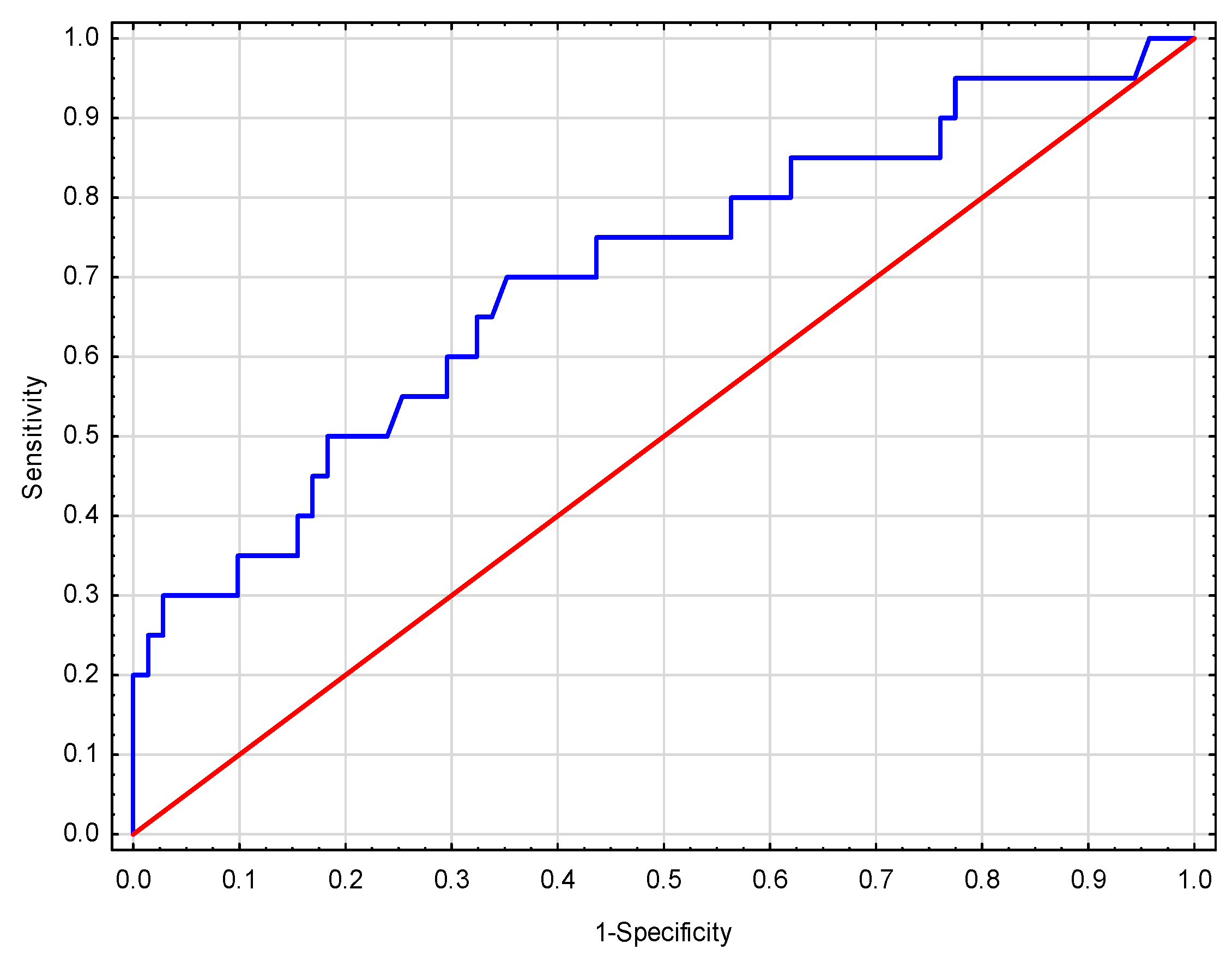
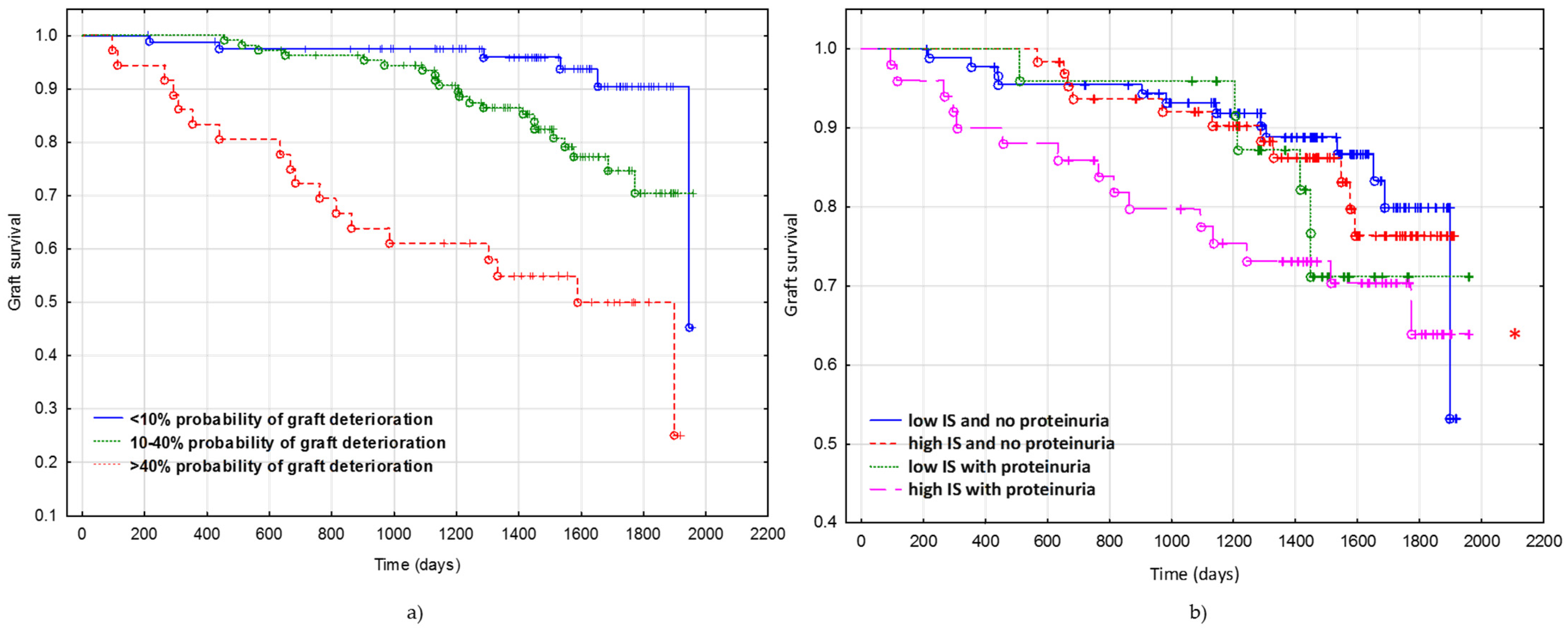
2.4. Predicted Probability of Deterioration of Graft Function
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Study Group and Sample Collection
5.2. Total Salivary and Serum pCS and IS Form Measurements
5.3. Biochemical Parameters Measurements
5.4. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nakamura, M.; Seki, G.; Iwadoh, K.; Nakajima, I.; Fuchinoue, S.; Fujita, T.; Teraoka, S. Acute kidney injury as defined by the RIFLE criteria is a risk factor for kidney transplant graft failure. Clin. Transplant. 2012, 26, 520–528. [Google Scholar] [CrossRef]
- Czyżewski, L.; Sańko-Resmer, J.; Wyzgał, J.; Kurowski, A. Assessment of health-related quality of life of patients after kidney transplantation in comparison with hemodialysis and peritoneal dialysis. Ann. Transplant. 2014, 19, 576–585. [Google Scholar] [CrossRef]
- Shiran, M.B.; Barzegar Marvasti, M.; Shakeri-Zadeh, A.; Shahidi, M.; Tabkhi, N.; Farkhondeh, F.; Kalantar, E.; Asadinejad, A. Enhancement of Toxic Substances Clearance from Blood Equvalent Solution and Human Whole Blood through High Flux Dialyzer by 1 MHz Ultrasound. J. Biomed. Phys. Eng. 2017, 7, 107–116. [Google Scholar]
- Kolonko, A.; Chudek, J.; Kujawa-Szewieczek, A.; Czerwieńska, B.; Wiecek, A. Serum copeptin level predicts a rapid decrease of overhydration after kidney transplantation. Clin. Chem. Lab. Med. 2014, 52, 1297–1303. [Google Scholar] [CrossRef]
- Caplin, B.; Kumar, S.; Davenport, A. Patients’ perspective of haemodialysis-associated symptoms. Nephrol. Dial. Transplant. 2011, 26, 2656–2663. [Google Scholar] [CrossRef]
- Kostro, J.Z.; Hellmann, A.; Kobiela, J.; Skóra, I.; Lichodziejewska-Niemierko, M.; Dębska-Ślizień, A.; Śledziński, Z. Quality of Life After Kidney Transplantation: A Prospective Study. Transplant. Proc. 2016, 48, 50–54. [Google Scholar] [CrossRef]
- Rangaswami, J.; Mathew, R.O.; Parasuraman, R.; Tantisattamo, E.; Lubetzky, M.; Rao, S.; Yaqub, M.S.; Birdwell, K.A.; Bennett, W.; Dalal, P.; et al. Cardiovascular disease in the kidney transplant recipient: Epidemiology, diagnosis and management strategies. Nephrol. Dial. Transplant. 2019, 34, 760–773. [Google Scholar] [CrossRef]
- Irish, W.D.; Ilsley, J.N.; Schnitzler, M.A.; Feng, S.; Brennan, D.C. A risk prediction model for delayed graft function in the current era of deceased donor renal transplantation. Am. J. Transplant. 2010, 10, 2279–2286. [Google Scholar] [CrossRef]
- Zaza, G.; Ferraro, P.M.; Tessari, G.; Sandrini, S.; Scolari, M.P.; Capelli, I.; Minetti, E.; Gesualdo, L.; Girolomoni, G.; Gambaro, G.; et al. Predictive model for delayed graft function based on easily available pre-renal transplant variables. Intern. Emerg. Med. 2015, 10, 135–141. [Google Scholar] [CrossRef]
- Hernández, D.; Sánchez-Fructuoso, A.; González-Posada, J.M.; Arias, M.; Campistol, J.M.; Rufino, M.; Morales, J.M.; Moreso, F.; Pérez, G.; Torres, A.; et al. A novel risk score for mortality in renal transplant recipients beyond the first posttransplant year. Transplantation 2009, 88, 803–809. [Google Scholar] [CrossRef]
- Foroutan, F.; Friesen, E.L.; Clark, K.E.; Motaghi, S.; Zyla, R.; Lee, Y.; Kamran, R.; Ali, E.; De Snoo, M.; Orchanian-Cheff, A.; et al. Risk Factors for 1-Year Graft Loss After Kidney Transplantation: Systematic Review and Meta-Analysis. Clin. J. Am. Soc. Nephrol. 2019, 14, 1642–1650. [Google Scholar] [CrossRef]
- Kaboré, R.; Haller, M.C.; Harambat, J.; Heinze, G.; Leffondré, K. Risk prediction models for graft failure in kidney transplantation: A systematic review. Nephrol. Dial. Transplant. 2017, 32, ii68–ii76. [Google Scholar] [CrossRef] [Green Version]
- Baskin-Bey, E.S.; Kremers, W.; Nyberg, S.L. A recipient risk score for deceased donor renal allocation. Am. J. Kidney Dis. 2007, 49, 284–293. [Google Scholar] [CrossRef]
- Kers, J.; Peters-Sengers, H.; Heemskerk, M.B.A.; Berger, S.P.; Betjes, M.G.H.; van Zuilen, A.D.; Hilbrands, L.B.; de Fijter, J.W.; Nurmohamed, A.S.; Christiaans, M.H.; et al. Predicition models for delayed graft function: External validation on The Dutch Prospective Renal Transplantation Registry. Nephrol. Dial. Transplant. 2018, 33, 1259–1268. [Google Scholar] [CrossRef] [Green Version]
- Noble, J.; Jouve, T.; Malvezzi, P.; Süsal, C.; Rostaing, L. Transplantation of Marginal Organs: Immunological Aspects and Therapeutic Perspectives in Kidney Transplantation. Front. Immunol. 2019, 10, 3142. [Google Scholar] [CrossRef] [Green Version]
- Temilola, D.O.; Bezuidenhout, K.; Erasmus, R.T.; Stephen, L.; Davids, M.R.; Holmes, H. Salivary creatinine as a diagnostic tool for evaluating patients with chronic kidney disease. BMC Nephrol. 2019, 20, 387. [Google Scholar] [CrossRef] [Green Version]
- Korytowska, N.; Sankowski, B.; Wyczałkowska-Tomasik, A.; Pączek, L.; Wroczyński, P.; Giebułtowicz, J. The utility of saliva testing in the estimation of uremic toxin levels in serum. Clin. Chem. Lab. Med. 2018, 57, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Eknoyan, G.; Lameire, N.; Eckardt, K.; Kasiske, B.; Wheeler, D.; Levin, A.; Levey, A.S. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar]
- Hosmer, D.W.; Hosmer, T.; Le Cessie, S.; Lemeshow, S. A comparison of goodness-of-fit tests for the logistic regression model. Stat. Med. 1997, 16, 965–980. [Google Scholar] [CrossRef]
- Mottola, C.; Girerd, N.; Duarte, K.; Aarnink, A.; Giral, M.; Dantal, J.; Garrigue, V.; Mourad, G.; Buron, F.; Morelon, E.; et al. Prognostic value for long-term graft survival of estimated glomerular filtration rate and proteinuria quantified at 3 months after kidney transplantation. Clin. Kidney J. 2020, 13, 791–802. [Google Scholar] [CrossRef] [PubMed]
- Molcho, M.; Rozen-Zvi, B.; Shteinmats, T.; Ben Dor, N.; Vahav, I.; Nesher, E.; Rahamimov, R. Temporal changes of proteinuria after kidney transplantation: Association with cardiovascular morbidity and mortality. J. Nephrol. 2020, 33, 1059–1066. [Google Scholar] [CrossRef]
- Ponticelli, C.; Glassock, R.J. Posttransplant recurrence of primary glomerulonephritis. Clin. J. Am. Soc. Nephrol. 2010, 5, 2363–2372. [Google Scholar] [CrossRef] [Green Version]
- Infante, B.; Rossini, M.; Leo, S.; Troise, D.; Netti, G.S.; Ranieri, E.; Gesualdo, L.; Castellano, G.; Stallone, G. Recurrent Glomerulonephritis after Renal Transplantation: The Clinical Problem. Int. J. Mol. Sci. 2020, 21, 5954. [Google Scholar] [CrossRef]
- Tai, H.C.; Lai, M.K.; Wang, S.M.; Chueh, S.C.; Yu, H.J. High incidence of urinary tract malignancy among patients with haematuria following kidney transplantation in Taiwan. Transpl. Int. 2009, 22, 403–407. [Google Scholar] [CrossRef]
- Kim, D.Y.; Abouljoud, M.; Parasuraman, R. The role of microscopic hematuria in the evaluation of urologic malignancy in renal transplant recipients. Transplant. Proc. 2010, 42, 1641–1642. [Google Scholar] [CrossRef] [PubMed]
- Orlandi, P.F.; Fujii, N.; Roy, J.; Chen, H.Y.; Lee Hamm, L.; Sondheimer, J.H.; He, J.; Fischer, M.J.; Rincon-Choles, H.; Krishnan, G.; et al. Hematuria as a risk factor for progression of chronic kidney disease and death: Findings from the Chronic Renal Insufficiency Cohort (CRIC) Study. BMC Nephrol. 2018, 19, 150. [Google Scholar] [CrossRef]
- Vivante, A.; Afek, A.; Frenkel-Nir, Y.; Tzur, D.; Farfel, A.; Golan, E.; Chaiter, Y.; Shohat, T.; Skorecki, K.; Calderon-Margalit, R. Persistent asymptomatic isolated microscopic hematuria in Israeli adolescents and young adults and risk for end-stage renal disease. JAMA 2011, 306, 729–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poesen, R.; Viaene, L.; Verbeke, K.; Augustijns, P.; Bammens, B.; Claes, K.; Kuypers, D.; Evenepoel, P.; Meijers, B. Cardiovascular disease relates to intestinal uptake of p-cresol in patients with chronic kidney disease. BMC Nephrol. 2014, 15, 87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.-J.; Wu, C.-J.; Pan, C.-F.; Chen, Y.-C.; Sun, F.-J.; Chen, H.-H. Serum Concentration of p-Cresol and Indoxyl Sulfate in Elderly Hemodialysis Patients. Int. J. Gerontol. 2011, 5, 80–83. [Google Scholar] [CrossRef] [Green Version]
- Brown, T.S.; Elster, E.A.; Stevens, K.; Graybill, J.C.; Gillern, S.; Phinney, S.; Salifu, M.O.; Jindal, R.M. Bayesian modeling of pretransplant variables accurately predicts kidney graft survival. Am. J. Nephrol. 2012, 36, 561–569. [Google Scholar] [CrossRef]
- Tang, H.; Poynton, M.R.; Hurdle, J.F.; Baird, B.C.; Koford, J.K.; Goldfarb-Rumyantzev, A.S. Predicting three-year kidney graft survival in recipients with systemic lupus erythematosus. ASAIO J. 2011, 57, 300–309. [Google Scholar] [CrossRef]
- Udomkarnjananun, S.; Townamchai, N.; Kerr, S.J.; Tasanarong, A.; Noppakun, K.; Lumpaopong, A.; Prommool, S.; Supaporn, T.; Avihingsanon, Y.; Praditpornsilpa, K.; et al. The First Asian Kidney Transplantation Prediction Models for Long-term Patient and Allograft Survival. Transplantation 2020, 104, 1048–1057. [Google Scholar] [CrossRef]
- Foucher, Y.; Daguin, P.; Akl, A.; Kessler, M.; Ladrière, M.; Legendre, C.; Kreis, H.; Rostaing, L.; Kamar, N.; Mourad, G.; et al. A clinical scoring system highly predictive of long-term kidney graft survival. Kidney Int. 2010, 78, 1288–1294. [Google Scholar] [CrossRef]
- Akl, A.; Ismail, A.M.; Ghoneim, M. Prediction of graft survival of living-donor kidney transplantation: Nomograms or artificial neural networks? Transplantation 2008, 86, 1401–1406. [Google Scholar] [CrossRef] [PubMed]
- Bang, K.; Lee, H.K.; Huh, W.; Lee, Y.J.; Woon, B.S.; Ro, H.; Hwang, Y.H.; Ha, J.; Park, M.H.; Kim, S.J.; et al. Assessment of deceased donor kidneys using a donor scoring system. Yonsei Med. J. 2010, 51, 870–876. [Google Scholar] [CrossRef]
- Shabir, S.; Halimi, J.M.; Cherukuri, A.; Ball, S.; Ferro, C.; Lipkin, G.; Benavente, D.; Gatault, P.; Baker, R.; Kiberd, B.; et al. Predicting 5-year risk of kidney transplant failure: A prediction instrument using data available at 1 year posttransplantation. Am. J. Kidney Dis. 2014, 63, 643–651. [Google Scholar] [CrossRef]
- Ho, J.; Wiebe, C.; Rush, D.N.; Rigatto, C.; Storsley, L.; Karpinski, M.; Gao, A.; Gibson, I.W.; Nickerson, P.W. Increased urinary CCL2: Cr ratio at 6 months is associated with late renal allograft loss. Transplantation 2013, 95, 595–602. [Google Scholar] [CrossRef]
- Guy, M.; Newall, R.; Borzomato, J.; Kalra, P.A.; Price, C. Use of a first-line urine protein-to-creatinine ratio strip test on random urines to rule out proteinuria in patients with chronic kidney disease. Nephrol. Dial. Transplant. 2009, 24, 1189–1193. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.N.; Wu, I.W.; Huang, Y.F.; Peng, S.Y.; Huang, Y.C.; Ning, H.C. Measuring serum total and free indoxyl sulfate and p-cresyl sulfate in chronic kidney disease using UPLC-MS/MS. J. Food Drug Anal. 2019, 27, 502–509. [Google Scholar] [CrossRef] [Green Version]
- Barreto, F.C.; Barreto, D.V.; Liabeuf, S.; Meert, N.; Glorieux, G.; Temmar, M.; Choukroun, G.; Vanholder, R.; Massy, Z.A.; on behalf of the European Uremic Toxin Work Group (EUTox). Serum indoxyl sulfate is associated with vascular disease and mortality in chronic kidney disease patients. Clin. J. Am. Soc. Nephrol. 2009, 4, 1551–1558. [Google Scholar] [CrossRef] [Green Version]
- Wu, I.W.; Hsu, K.H.; Hsu, H.J.; Lee, C.C.; Sun, C.Y.; Tsai, C.J.; Wu, M.S. Serum free p-cresyl sulfate levels predict cardiovascular and all-cause mortality in elderly hemodialysis patients—A prospective cohort study. Nephrol. Dial. Transplant. 2012, 27, 1169–1175. [Google Scholar] [CrossRef] [Green Version]
- Krieter, D.H.; Hackl, A.; Rodriguez, A.; Chenine, L.; Moragues, H.L.; Lemke, H.D.; Wanner, C.; Canaud, B. Protein-bound uraemic toxin removal in haemodialysis and post-dilution haemodiafiltration. Nephrol. Dial. Transplant. 2010, 25, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Giebułtowicz, J.; Korytowska, N.; Sankowski, B.; Wroczyński, P. Development and validation of a LC-MS/MS method for quantitative analysis of uraemic toxins p-cresol sulphate and indoxyl sulphate in saliva. Talanta 2016, 150, 593–598. [Google Scholar] [CrossRef]
- Huang, S.T.; Shu, K.H.; Cheng, C.H.; Wu, M.J.; Yu, T.M.; Chuang, Y.W.; Chen, C.H. Serum total p-cresol and indoxyl sulfate correlated with stage of chronic kidney disease in renal transplant recipients. Transplant. Proc. 2012, 44, 621–624. [Google Scholar] [CrossRef]
- Ligabue, G.; Damiano, F.; Cuoghi, A.; De Biasi, S.; Bellei, E.; Granito, M.; Aldo, T.; Cossarizza, A.; Cappelli, G. p-Cresol and Cardiovascular Risk in Kidney Transplant Recipients. Transplant. Proc. 2015, 47, 2121–2125. [Google Scholar] [CrossRef]
- Liabeuf, S.; Desjardins, L.; Massy, Z.A.; Brazier, F.; Westeel, P.F.; Mazouz, H.; Titeca-Beauport, D.; Diouf, M.; Glorieux, G.; Vanholder, R.; et al. Levels of Indoxyl Sulfate in Kidney Transplant Patients, and the Relationship with Hard Outcomes. Circ. J. 2016, 80, 722–730. [Google Scholar] [CrossRef] [Green Version]
- Poesen, R.; Evenepoel, P.; de Loor, H.; Bammens, B.; Claes, K.; Sprangers, B.; Naesens, M.; Kuypers, D.; Augustijns, P.; Meijers, B. The influence of renal transplantation on retained microbial-human co-metabolites. Nephrol. Dial. Transplant. 2016, 31, 1721–1729. [Google Scholar] [CrossRef] [Green Version]
- Fricke, W.F.; Maddox, C.; Song, Y.; Bromberg, J.S. Human microbiota characterization in the course of renal transplantation. Am. J. Transplant. 2014, 14, 416–427. [Google Scholar] [CrossRef]
- Vanholder, R.; Glorieux, G.; Massy, Z.A. Intestinal metabolites, chronic kidney disease and renal transplantation: Enigma Variations? Nephrol. Dial. Transplant. 2016, 31, 1547–1551. [Google Scholar] [CrossRef] [Green Version]
- Zou, K.H.; O’Malley, A.J.; Mauri, L. Receiver-operating characteristic analysis for evaluating diagnostic tests and predictive models. Circulation 2007, 115, 654–657. [Google Scholar] [CrossRef] [Green Version]
- Kalil, A.C.; Mattei, J.; Florescu, D.F.; Sun, J.; Kalil, R.S. Recommendations for the assessment and reporting of multivariable logistic regression in transplantation literature. Am. J. Transplant. 2010, 10, 1686–1694. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| M1 (n = 92) | M6 (n = 77) | M12 (n = 73) | p-Value | |||||
|---|---|---|---|---|---|---|---|---|
| Frequency (%)/Median (IQR) | M1 vs. M6 | M1 vs. M12 | M6 vs. M12 | |||||
| gender, female/male | 37/55 (40/60) | - | ||||||
| age, years | 53 (19) | 55 (18) | 56 (20) | - | ||||
| time post KTx, days | 1125 (844) | 1262 (889) | 1476 (761) | - | ||||
| the drug, CyA/Tac/Eve | 18/74/0 (20/80/-) | 16/61/0 (21/79/-) | 16/56/1 (22/77/1) | - | ||||
| smoking | current | 13 (14) | - | |||||
| ex-smoker | 32 (35) | - | ||||||
| never | 47 (51) | - | ||||||
| passive | 16 (17) | - | ||||||
| history of diabetes | 18 (20) | - | ||||||
| history of hypertension | 55 (60) | - | ||||||
| BMI, kg/m2 | 25.9 (4.4) 1 | 26.3 (4.6) 1 | 26.5 (4.6) 1 | 0.12347 | 0.00572 | 0.44694 | ||
| serum creatinine, mg/dL | 1.46 (1.03) | 1.41 (0.85) | 1.46 (0.88) | 0.18631 | 0.76843 | 0.00807 | ||
| eGFR, mL/min/1.73 m2 | 51 (48) | 51 (49) | 48 (45) | 0.18631 | 0.76843 | 0.00807 | ||
| CKD stage 2 | 1 | 9 (10) | 9 (12) | 6 (8) | - | |||
| 2 | 29 (31) | 22 (29) | 24 (33) | - | ||||
| 3 | 30 (33) | 27 (35) | 25 (34) | - | ||||
| 4 | 21 (23) | 15 (19) | 13 (18) | - | ||||
| 5 | 3 (3) | 4 (5) | 5 (7) | - | ||||
| salivary IS, ng/mL | 33 (37) 3 | 21 (39) 4 | 27 (39) | 0.19572 | 0.79488 | 1.00000 | ||
| serum IS, ng/mL | 2075 (2788) | 1715 (2489) | 1870 (2497) | 0.43288 | 1.00000 | 1.00000 | ||
| salivary pCS, ng/mL | 57 (139) 3 | 46 (86) 4 | 48 (78) | 0.17769 | 1.00000 | 0.14575 | ||
| serum pCS, ng/mL | 7103 (9651) | 4697 (6875) | 4755 (6636) | 0.36987 | 1.00000 | 0.50379 | ||
| hemoglobin, g/L | 136 (20) 1 | 136 (18) 1,5 | 134 (17) 1,5 | 0.89890 | 0.34903 | 0.16106 | ||
| proteinuria ≥10 mg/dL 12 | 32 (35) 5 | 29 (32) 6 | 22 (24) 7 | - | - | - | ||
| glucosuria ≥50 mg/dL | 7 (7.7) 5 | 4 (5.3) 6 | 3 (3.3) 7 | - | - | - | ||
| hematuria ≥0.03 mg/dL | UTI | 25 (27) 5 | 17 (23) 6 | 17 (24) 7 | - | - | - | |
| glomeruar | 2 (2.2) 5 | 3 (4.0) 6 | 1 (1.4) 7 | |||||
| BKV | 3 (19) 8 | 1 (13) 9 | 1 (10) 10 | - | - | - | ||
| CMV | 1 (4) 11 | 0 (0) 9 | 0 (0) 10 | - | - | - | ||
| rs (p) | eGFR | ||
|---|---|---|---|
| All Subjects (n = 92) | DoGF-Free Group (n = 72) | DoGF Group (n = 20) | |
| serum pCS | −0.50 (p = 0.00001) | −0.56 (p < 0.00001) | −0.52 (p = 0.01909) |
| salivary pCS | −0.55 (p < 0.00001) 1 | −0.61 (p < 0.00001) 2 | −0.47 (p = 0.06582) 3 |
| serum IS | −0.78 (p < 0.00001) | −0.76 (p < 0.00001) | −0.71 (p = 0.00042) |
| salivary IS | −0.76 (p < 0.00001) 1 | −0.75 (p < 0.00001) 2 | −0.62 (p = 0.01024) 3 |
| Univariate | Multivariate | |||||||
|---|---|---|---|---|---|---|---|---|
| Variable at M1 | β | OR | 95% CI | p-Value | β | OR | 95% CI | p-Value |
| salivary IS (per 10 ng/mL) | 0.183 | 1.20 | 1.05–1.37 | 0.00682 | 0.170 | 1.19 | 1.04–1.35 | 0.01269 |
| salivary pCS (per 10 ng/mL) | 0.014 | 1.02 | 0.99–1.04 | 0.32124 | – | |||
| hematuria 1 | 0.936 | 2.55 | 0.92–7.06 | 0.07142 | – | |||
| proteinuria 2 | 1.485 | 4.42 | 1.56–12.52 | 0.00522 | 1.305 | 3.69 | 1.22–11.12 | 0.02048 |
| glucosuria 3 | 1.806 | 6.09 | 0.94–39.36 | 0.05781 | – | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korytowska, N.; Wyczałkowska-Tomasik, A.; Pączek, L.; Giebułtowicz, J. Evaluation of Salivary Indoxyl Sulfate with Proteinuria for Predicting Graft Deterioration in Kidney Transplant Recipients. Toxins 2021, 13, 571. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13080571
Korytowska N, Wyczałkowska-Tomasik A, Pączek L, Giebułtowicz J. Evaluation of Salivary Indoxyl Sulfate with Proteinuria for Predicting Graft Deterioration in Kidney Transplant Recipients. Toxins. 2021; 13(8):571. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13080571
Chicago/Turabian StyleKorytowska, Natalia, Aleksandra Wyczałkowska-Tomasik, Leszek Pączek, and Joanna Giebułtowicz. 2021. "Evaluation of Salivary Indoxyl Sulfate with Proteinuria for Predicting Graft Deterioration in Kidney Transplant Recipients" Toxins 13, no. 8: 571. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13080571