Risk of Hematologic Malignant Neoplasms after Postoperative Treatment of Breast Cancer

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
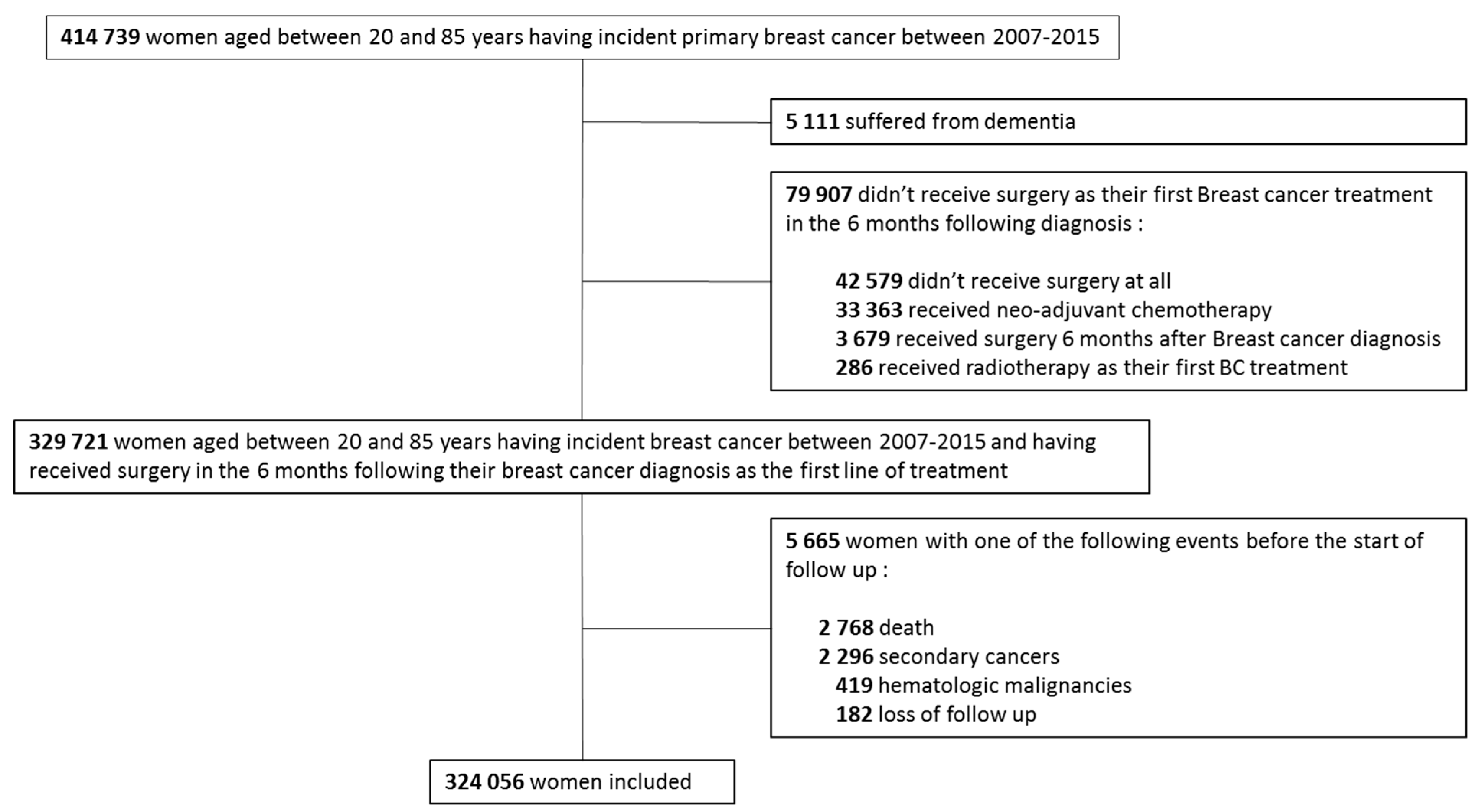
2.2. Study Population
2.3. Exposure Definition
2.4. Covariates
2.5. Outcomes
2.6. Statistical Analyses
3. Results
3.1. Patient’s Characteristics
3.2. Hematologic Malignancies’ Occurrence in the Whole Cohort and by Exposure Groups
3.3. Risk of HM According to BC Treatment Modalities
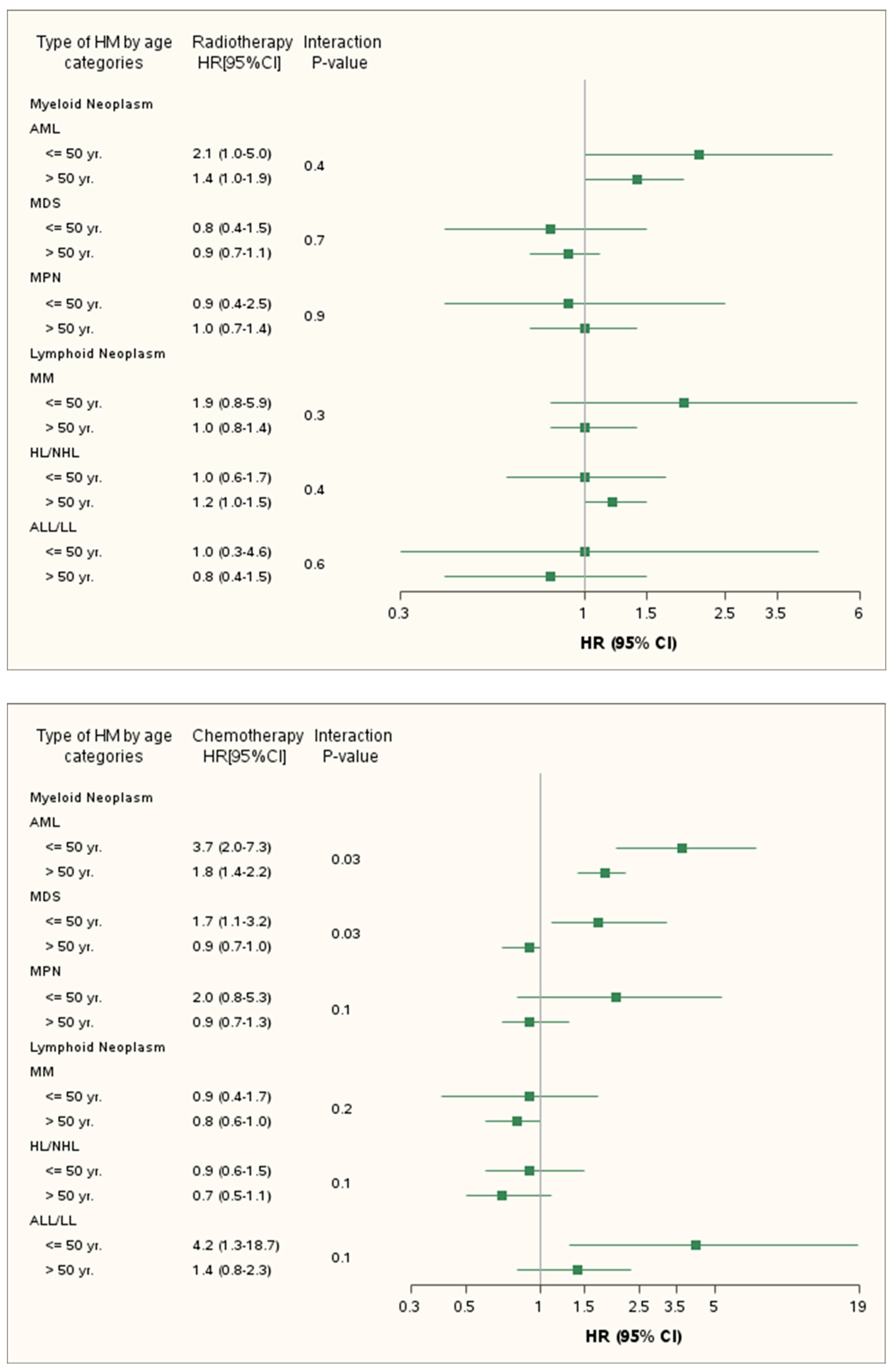
3.4. Risk of Hematologic Malignancies Stratified by Age
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Morton, L.M.; Dores, G.M.; Schonfeld, S.J.; Linet, M.S.; Sigel, B.S.; Lam, C.J.K.; Tucker, M.A.; Curtis, R.E. Association of Chemotherapy for Solid Tumors with Development of Therapy-Related Myelodysplastic Syndrome or Acute Myeloid Leukemia in the Modern Era. JAMA Oncol. 2019, 5, 318–325. [Google Scholar] [CrossRef] [PubMed]
- Wolff, A.C.; Blackford, A.L.; Visvanathan, K.; Rugo, H.S.; Moy, B.; Goldstein, L.J.; Stockerl-Goldstein, K.; Neumayer, L.; Langbaum, T.S.; Theriault, R.L.; et al. Risk of marrow neoplasms after adjuvant breast cancer therapy: The national comprehensive cancer network experience. J. Clin. Oncol. 2014, 33, 340–348. [Google Scholar] [CrossRef] [PubMed]
- Martin, M.G.; Welch, J.S.; Luo, J.; Ellis, M.J.; Graubert, T.A.; Walter, M.J. Therapy related acute myeloid leukemia in breast cancer survivors, a population-based study. Breast Cancer Res. Treat. 2009, 118, 593–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beadle, G.; Baade, P.; Fritschi, L. Acute myeloid leukemia after breast cancer: A population-based comparison with hematological malignancies and other cancers. Ann. Oncol. 2009, 20, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Curtis, R.E.; Boice, J.D.; Stovall, M.; Bernstein, L.; Greenberg, R.S.; Flannery, J.T.; Schwartz, A.G.; Weyer, P.; Moloney, W.C.; Hoover, R.N. Risk of leukemia after chemotherapy and radiation treatment for breast cancer. N. Engl. J. Med. 1992, 326, 1745–1751. [Google Scholar] [CrossRef] [PubMed]
- Morton, L.M.; Dores, G.M.; Tucker, M.A.; Kim, C.J.; Onel, K.; Gilbert, E.S.; Fraumeni, J.F., Jr.; Curtis, R.E. Evolving risk of therapy-related acute myeloid leukemia following cancer chemotherapy among adults in the United States, 1975–2008. Blood 2013, 121, 2996–3004. [Google Scholar] [CrossRef] [PubMed]
- Fianchi, L.; Pagano, L.; Piciocchi, A.; Candoni, A.; Gaidano, G.; Breccia, M.; Criscuolo, M.; Specchia, G.; Maria Pogliani, E.; Maurillo, L.; et al. Characteristics and outcome of therapy-related myeloid neoplasms: Report from the Italian network on secondary leukemias. Am. J. Hematol. 2015, 90, E80–E85. [Google Scholar] [CrossRef]
- Chen, W.; Wang, E.; Lu, Y.; Gaal, K.K.; Huang, Q. Therapy-Related Acute Lymphoblastic Leukemia Without 11q23 Abnormality: Report of Six Cases and a Literature Review. Am. J. Clin. Pathol. 2010, 133, 75–82. [Google Scholar] [CrossRef]
- Krishnan, B.; Morgan, G.J. Non-Hodgkin lymphoma secondary to cancer chemotherapy. Cancer Epidemiol. Biomark. Prev. 2007, 16, 377–380. [Google Scholar] [CrossRef]
- Aldoss, I.; Stiller, T.; Tsai, N.C.; Song, J.Y.; Cao, T.; Bandara, N.A.; Salhotra, A.; Khaled, S.; Aribi, A.; Al Malki, M.M.; et al. Therapy-related acute lymphoblastic leukemia has distinct clinical and cytogenetic features compared to de novo acute lymphoblastic leukemia, but outcomes are comparable in transplanted patients. Haematologica 2018, 103, 1662–1668. [Google Scholar] [CrossRef]
- Aldoss l Dagis, A.; Palmer, J.; Forman, S.; Pullarkat, V. Therapy-related ALL: Cytogenetic features and hematopoietic cell transplantation outcome. Bone Marrow Transplant. 2015, 50, 746–748. [Google Scholar] [CrossRef] [PubMed]
- Abdulwahab, A.; Sykes, J.; Kamel-Reid, S.; Chang, H.; Brandwein, J.M. Therapy-related acute lymphoblastic leukemia is more frequent than previously recognized and has a poor prognosis. Cancer 2012, 118, 3962–3967. [Google Scholar] [CrossRef] [PubMed]
- Jabagi, M.J.; Vey, N.; Goncalves, A.; Le Tri, T.; Zureik, M.; Dray-Spira, R. Evaluation of the Incidence of Hematologic Malignant Neoplasms Among Breast Cancer Survivors in France. JAMA Netw. Open. 2019, 2, e187147. [Google Scholar] [CrossRef] [PubMed]
- Lemaitre, M.; Kirchgesner, J.; Rudnichi, A.; Carrat, F.; Zureik, M.; Carbonnel, F.; Dray-Spira, R. Association Between Use of Thiopurines or Tumor Necrosis Factor Antagonists Alone or in Combination and Risk of Lymphoma in Patients with Inflammatory Bowel Disease. JAMA 2017, 318, 1679–1686. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, K.; Bertrand, M.; Bader, G.; Lucot, J.P.; Dray-Spira, R.; Zureik, M. Association of Hysteroscopic vs Laparoscopic Sterilization with Procedural, Gynecological, and Medical Outcomes. JAMA 2018, 319, 375–387. [Google Scholar] [CrossRef]
- Waks, A.G.; Winer, E.P. Breast Cancer Treatment: A Review. JAMA 2019, 321, 288–300. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, J.; Massarut, S.; Vaidya, H.; Alexander, E.; Richards, T.; Caris, J.; Sirohi, B.; Tobias, J.S. Rethinking neoadjuvant chemotherapy for breast cancer. BMJ 2018, 360, j5913. [Google Scholar] [CrossRef]
- McCullagh, P.; Nelder, J.A. Generalized Linear Models, 2nd ed.; CRC Press: Boca Raton, FL, USA, 1989. [Google Scholar]
- Fine, J.P.; Gray, R.J. A Proportional Hazards Model for the Subdistribution of a Competing Risk. J. Am. Stat. Assoc. 1999, 94, 496–509. [Google Scholar] [CrossRef]
- Fisher, B.; Anderson, S.; Bryant, J.; Margolese, R.G.; Deutsch, M.; Fisher, E.R.; Jeong, J.H.; Wolmark, N. Twenty-Year Follow-up of a Randomized Trial Comparing Total Mastectomy, Lumpectomy, and Lumpectomy plus Irradiation for the Treatment of Invasive Breast Cancer. N. Engl. J. Med. 2002, 347, 1233–1241. [Google Scholar] [CrossRef] [Green Version]
- Suter, M.B.; Pagani, O. Should age impact breast cancer management in young women? Fine tuning of treatment guidelines. Ther. Adv. Med. Oncol. 2018, 10. [Google Scholar] [CrossRef]
- Hammond, M.E.; Hayes, D.F.; Dowsett, M.; Allred, D.C.; Hagerty, K.L.; Badve, S.; Fitzgibbons, P.L.; Francis, G.; Goldstein, N.S.; Hayes, M.; et al. American Society of Clinical Oncology/College of American Pathologists Guideline Recommendations for Immunohistochemical Testing of Estrogen and Progesterone Receptors in Breast Cancer. Arch. Pathol. Lab. Med. 2010, 134, e48–e72. [Google Scholar] [CrossRef] [PubMed]
- Foulkes, W.; Smith, I.; Reis-Filho, J. Triple-negative breast cancer. N. Engl. J. Med. 2010, 363, 1938–1948. [Google Scholar] [CrossRef] [PubMed]
- McNerney, M.E.; Godley, L.A.; Le Beau, M.M. Therapy-related myeloid neoplasms: When genetics and environment collide. Nat. Rev. Cancer 2017, 17, 513–527. [Google Scholar] [CrossRef]
- Allan, J.M.; Travis, L.B. Mechanisms of therapy-related carcinogenesis. Nat. Rev. Cancer 2005, 5, 943–955. [Google Scholar] [CrossRef]
- Godley, L.A.; Larson, R.A. Therapy-related myeloid leukemia. Semin. Oncol. 2008, 35, 418–429. [Google Scholar] [CrossRef] [PubMed]
- Sevcikova, K.; Zhuang, Z.; Garcia-Manero, G.; Alvarez, R.H.; Kantarjian, H.M.; Mego, M.; Albarracin, C.; Tang, G.; Strom, S.S.; Medeiros, L.J.; et al. Comprehensive analysis of factors impacting risks and outcomes of therapy-related myeloid neoplasms following breast cancer treatment. Leukemia 2016, 30, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Leone, G.; Fianchi, L.; Voso, M.T. Therapy-related myeloid neoplasms. Curr. Opin. Oncol. 2011, 23, 672–680. [Google Scholar] [CrossRef]
- Kaplan, H.G.; Malmgren, J.A.; Atwood, M.K. Increased incidence of myelodysplastic syndrome and acute myeloid leukemia following breast cancer treatment with radiation alone or combined with chemotherapy: A registry cohort analysis 1990–2005. BMC Cancer 2011, 11, 260. [Google Scholar] [CrossRef]
- Kelleher, N.; Gallardo, D.; González-Campos, J.; Hernández-Rivas, J.M.; Montesinos, P.; Sarrá, J.; Gil, C.; Barba, P.; Guàrdia, R.; Brunet, S.; et al. Incidence, clinical and biological characteristics and outcome of secondary acute lymphoblastic leukemia after solid organ or hematologic malignancy. Leuk. Lymphoma 2016, 57, 86–91. [Google Scholar] [CrossRef]
- Mauch, P.M.; Kalish, L.A.; Marcus, K.C.; Coleman, C.N.; Shulman, L.N.; Krill, E.; Come, S.; Silver, B.; Canellos, G.P.; Tarbell, N.J. Second malignancies after treatment for laparotomy staged IA-IIIB Hodgkin’s disease: Long-term analysis of risk factors and outcome. Blood 1996, 87, 3625–3632. [Google Scholar]
- Kim, C.J.; Freedman, D.M.; Curtis, R.E.; Berrington de Gonzalez, A.; Morton, L.M. Risk of non-Hodgkin lymphoma after radiotherapy for solid cancers. Leuk. Lymphoma 2013, 54, 1691–1697. [Google Scholar] [CrossRef] [PubMed]
- Granfeldt Østgård, L.S.; Medeiros, B.C.; Sengeløv, H.; Nørgaard, M.; Andersen, M.K.; Dufva, I.H.; Friis, L.S.; Kjeldsen, E.; Marcher, C.W.; Preiss, B.; et al. Epidemiology and Clinical Significance of Secondary and Therapy-Related Acute Myeloid Leukemia: A National Population-Based Cohort Study. J. Clin. Oncol. 2015, 33, 3641–3649. [Google Scholar] [CrossRef] [PubMed]
- Wakeford, R. The cancer epidemiology of radiation. Oncogene 2004, 23, 6404–6428. [Google Scholar] [CrossRef] [Green Version]
- Shuryak, I.; Sachs, R.K.; Brenner, D.J. Cancer risks after radiation exposure in middle age. J. Natl. Cancer Inst. 2010, 102, 1628–1636. [Google Scholar] [CrossRef] [PubMed]
- Renella, R.; Verkooijen, H.M.; Fioretta, G.; Vlastos, G.; Kurtz, J.; Sappino, A.P.; Schäfer, P.; Neyroud-Caspar, I.; Bouchardy, C. Increased risk of acute myeloid leukaemia after treatment for breast cancer. Breast 2006, 15, 614–619. [Google Scholar] [CrossRef]
- Ornstein, M.C.; Mukherjee, S.; Mohan, S.; Elson, P.; Tiu, R.V.; Saunthararajah, Y.; Kendeigh, C.; Advani, A.; Kalaycio, M.; Maciejewski, J.P.; et al. Predictive factors for latency period and a prognostic model for survival in patients with therapy-related acute myeloid leukemia. Am. J. Hematol. 2014, 89, 168–173. [Google Scholar] [CrossRef]
- Giri, S.; Chi, M.; Johnson, B.; McCormick, D.; Jamy, O.; Bhatt, V.R.; Martin, M.G. Secondary acute lymphoblastic leukemia is an independent predictor of poor prognosis. Leuk. Res. 2015, 39, 1342–1346. [Google Scholar] [CrossRef]
- Rosenberg, A.S.; Brunson, A.; Paulus, J.K.; Tuscano, J.; Wun, T.; Keegan, T.H.M.; Jonas, B.A. Secondary acute lymphoblastic leukemia is a distinct clinical entity with prognostic significance. Blood Cancer J. 2017, 7, e605. [Google Scholar] [CrossRef]
- Kayser, S.; Döhner, K.; Krauter, J.; Köhne, C.H.; Horst, H.A.; Held, G.; von Lilienfeld-Toal, M.; Wilhelm, S.; Kündgen, A.; Götze, K.; et al. The impact of therapy-related acute myeloid leukemia (AML) on outcome in 2853 adult patients with newly diagnosed AML. Blood 2011, 117, 2137–2145. [Google Scholar] [CrossRef] [Green Version]
- Christiansen, D.H.; Andersen, M.K.; Pedersen-Bjergaard, J. Mutations with Loss of Heterozygosity of p53 Are Common in Therapy-Related Myelodysplasia and Acute Myeloid Leukemia After Exposure to Alkylating Agents and Significantly Associated with Deletion or Loss of 5q, a Complex Karyotype, and a Poor Prognosis. J. Clin. Oncol. 2001, 19, 1405–1413. [Google Scholar] [CrossRef]
- Cardoso, F.; van’t Veer, L.J.; Bogaerts, J.; Slaets, L.; Viale, G.; Delaloge, S.; Pierga, Je.; Brain, E.; Causeret, S.; DeLorenzi, M.; et al. 70-Gene Signature as an Aid to Treatment Decisions in Early-Stage Breast Cancer. N. Engl. J. Med. 2016, 375, 717–729. [Google Scholar] [CrossRef] [PubMed]
- Sparano, J.A.; Gray, R.J.; Makower, D.F.; Pritchard, K.I.; Albain, K.S.; Hayes, D.F.; Geyer, C.E., Jr.; Dees, E.C.; Goetz, M.P.; Olson, J.A. Jr.; et al. Adjuvant Chemotherapy Guided by a 21-Gene Expression Assay in Breast Cancer. N. Engl. J. Med. 2018, 379, 111–121. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Overall | Surgery Only | Surgery and Radiotherapy | Surgery and Chemotherapy | All 3 Modalities |
|---|---|---|---|---|---|
| 324 056 (100) | 50 323 (15.5) | 151 360 (46.7) | 13 937 (4.3) | 108 436 (33.5) | |
| Age at cohort entry | |||||
| Median age (IQR) | 59 (50–68) | 60 (50–70) | 63 (53–71) | 56 (47–64) | 55 (47–64) |
| Year of inclusion | |||||
| 2007–2009 | 105 560 (32.6) | 20 768 (41.3) | 44 251 (29.2) | 7 057 (50.6) | 33 484 (30.9) |
| 2010–2012 | 109 120 (33.7) | 14 862 (29.5) | 52 284 (34.5) | 3 784 (27.1) | 38 190 (35.2) |
| 2013–2015 | 109 376 (33.7) | 14 693 (29.2) | 54 825 (36.2) | 3 096 (22.2) | 36 762 (33.9) |
| Affiliation to Complementary Universal Health Insurance a | 14 257 (4.4) | 2 211 (4.4) | 4 862 (3.2) | 861 (6.2) | 6 323 (5.8) |
| Type of structure b | |||||
| Public hospitals | 110 282 (34.0) | 18 462 (36.7) | 49 294 (32.6) | 5 095 (36.6) | 37 431 (34.5) |
| Private hospitals | 142 515 (44.0) | 20 372 (40.5) | 69 677 (46.0) | 5 524 (39.6) | 46 942 (43.3) |
| Cancer Centers | 71 259 (22.0) | 11 489 (22.8) | 32 389 (21.4) | 3 318 (23.8) | 24 063 (22.2) |
| Comorbidities c | |||||
| Severe alcoholism | 4 902 (1.5) | 790 (1.6) | 2 300 (1.5) | 212 (1.5) | 1 600 (1.5) |
| Heavy smokers | 19 178 (5.9) | 3 184 (6.3) | 8 838 (5.8) | 782 (5.6) | 6 374 (5.9) |
| Morbid obesity | 40 548 (12.5) | 6 178 (12.3) | 20 047 (13.2) | 1 547 (11.1) | 12 776 (11.8) |
| Hypertension | 114 488 (35.3) | 18 072 (35.9) | 60 469 (40.0) | 4 062 (29.1) | 31 885 (29.4) |
| Diabetes | 32 277 (10.0) | 4 996 (9.9) | 16 059 (10.6) | 1 315 (9.4) | 9 907 (9.1) |
| Hyperlipidemia | 69 146 (21.3) | 10 530 (20.9) | 37 937 (25.1) | 2 331 (16.7) | 18 348 (16.9) |
| Heart disease | 37 814 (11.7) | 7 019 (13.9) | 20 895 (13.8) | 1 309 (9.4) | 8 591 (7.9) |
| HIV | 436 (0.1) | 87 (0.2) | 168 (0.1) | 26 (0.2) | 155 (0.1) |
| Hepatitis B & C | 1 536 (0.5) | 263 (0.5) | 764 (0.5) | 59 (0.4) | 450 (0.4) |
| Comedications c | |||||
| Immunosuppressant | 2 059 (0.6) | 303 (0.6) | 974 (0.6) | 84 (0.6) | 698 (0.6) |
| Antidepressants | 47 725 (14.7) | 7 769 (15.4) | 23 099 (15.3) | 1 897 (13.6) | 14 960 (13.8) |
| Benzodiazepine | 99 618 (30.7) | 16 513 (32.8) | 49 068 (32.4) | 4 035 (29.0) | 30 002 (27.7) |
| Contraception | 36 566 (11.3) | 5 005 (9.9) | 12 783 (8.4) | 1 610 (11.6) | 17 168 (15.8) |
| Hormone replacement therapy | 40 592 (12.5) | 6 343 (12.6) | 22 490 (14.9) | 1 323 (9.5) | 10 436 (9.6) |
| Breast cancer treatment* | |||||
| Type of surgery | |||||
| Partial mastectomy and lumpectomy | 264 972 (81.8) | 33 042 (65.6) | 141 165 (93.3) | 2 677 (19.2) | 57 006 (76.3) |
| Radical mastectomy | 59 084 (18.2) | 17 287 (34.4) | 10 195 (6.7) | 11 260 (80.8) | 25 715 (23.7) |
| Hormonal therapy d | 225 227 (69.5) | 21 614 (43.0) | 113 025 (74.7) | 9 145 (65.6) | 81 443 (75.1) |
| Aromatase Inhibitors | 156 655 (48.3) | 16 064 (31.9) | 85 984 (56.8) | 5 641 (40.5) | 48 966 (45.2) |
| SERM | 76 110 (23.5) | 6 489 (12.9) | 31 980 (21.1) | 3 715 (26.7) | 33 926 (31.3) |
| LHRH / GnRH agonist | 2 769 (0.9) | 220 (0.4) | 938 (0.6) | 204 (1.5) | 1 407 (1.3) |
| Hematologic Malignancy Type (n = 2 236) | Overall (1,647,704 PY) | Surgery Only (282,957 PY) | Surgery and Radiotherapy (746,236 PY) | Surgery and Chemotherapy (78,592 PY) | All 3 Modalities (540,311 PY) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. | IR per 100 000 PY (95%CI) | Median Time from BC to HM (IQR) | No. | IR per 100 000 PY (95%CI) | Median Time from BC to HM (IQR) | No. | IR per 100 000 PY (95%CI) | Median Time from BC to HM (IQR) | No. | IR per 100 000 PY (95%CI) | Median Time from BC to HM (IQR) | No. | IR per 100 000 PY (95%CI) | Median Time from BC to HM (IQR) | |
| Myeloid Neoplasm | |||||||||||||||
| Acute myeloid leukemia | 436 | 26.5 (24.0–29.0) | 3.2 (2.1–5.0) | 40 | 14.1 (10.1–19.2) | 5.5 (2.8–7.5) | 167 | 22.4 (19.1–26.0) | 3.5 (2.3–5.1) | 20 | 25.5 (15.5–39.3) | 2.8 (2.4–3.6) | 209 | 38.7 (33.6–44.3) | 2.7 (1.8–4.2) |
| Myelodysplastic syndrome | 552 | 33.5 (30.8–36.4) | 4.0 (2.6–5.9) | 98 | 34.6 (28.1–42.2) | 4.2 (3.0–6.3) | 272 | 36.5 (32.3–41.1) | 3.9 (2.5–5.7) | 29 | 36.9 (24.7–53.0) | 4.1 (2.7–6.5) | 153 | 28.3 (24.0–33.2) | 3.9 (2.5–6.0) |
| Myeloproliferative Neoplasms | 194 | 11.8 (10.2–13.5) | 4.1 (2.6–6.8) | 40 | 14.1 (10.1–19.3) | 4.6 (2.1–6.9) | 87 | 11.7 (9.3–14.4) | 3.7 (2.7–6.0) | 7 | 8.9 (3.6–18.3) | 6.9 (3.5–7.6) | 60 | 11.1 (8.5–14.3) | 4.3 (2.8–7.0) |
| Lymphoid Neoplasm | |||||||||||||||
| Multiple Myeloma | 310 | 18.8 (16.8–21.0) | 4.4 (2.9–6.5) | 53 | 18.7 (14.0–24.5) | 4.8 (3.4–6.7) | 165 | 22.1 (18.9–25.8) | 4.7 (3.2–6.5) | 15 | 19.1 (10.7–31.5) | 4.6 (2.8–7.6) | 77 | 14.3 (11.2–17.8) | 3.5 (2.5–5.6) |
| Hodgkin’s/Non-Hodgkin’s Lymphoma | 668 | 40.6 (37.5–43.8) | 4.7 (3.0–6.5) | 111 | 39.3 (32.3–47.3) | 4.5 (2.8–6.7) | 382 | 51.2 (46.2–56.6) | 4.6 (2.8–6.4) | 26 | 33.1 (21.6–48.5) | 6.4 (4.0–8.1) | 149 | 27.6 (23.3–32.4) | 4.8 (3.2–6.3) |
| Acute lymphoblastic leukemia/lymphocytic lymphoma | 76 | 4.6 (3.6–5.8) | 3.5 (2.2–5.7) | 12 | 4.4 (2.3–7.7) | 4.3 (2.5–6.2) | 28 | 3.7 (2.5–5.4) | 3.6 (2.3–5.1) | 5 | 7.1 (2.3–16.5) | 3.7 (1.8–5.6) | 31 | 5.7 (3.8–8.0) | 3.4 (2.0–6.1) |
| Hematologic Malignancy Type (n = 2236) | Surgery (n = 50 321) | Surgery and Radiotherapy (n = 151 362) | Surgery and Chemotherapy (n = 13933) | All 3 Modalities (n = 108 440) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Age-aHR1 (95%) | aHR2 (95%) | p-value | Age-aHR1 (95%) | aHR2 (95%) | p-value | Age-aHR1 (95%) | aHR2 (95%) | p-value | ||
| Myeloid Neoplasm | ||||||||||
| Acute myeloid leukemia | ref. | 1.4 (1.0–2.0) | 1.5 (1.0–2.1) | 0.04 | 2.2 (1.3–3.8) | 2.1 (1.2–3.6) | 0.007 | 3.4 (2.4–4.8) | 3.3 (2.3–4.7) | <0.0001 |
| Myelodysplastic syndrome | ref. | 1.0 (0.8–1.2) | 1.0 (0.8–1.2) | 0.8 | 1.7 (1.1–2.6) | 1.7 (1.1–2.5) | 0.02 | 1.4 (1.1–1.8) | 1.4 (1.1–1.8) | 0.01 |
| Myeloproliferative Neoplasms | ref. | 0.8 (0.5–1.1) | 0.9 (0.6–1.3) | 0.5 | 0.8 (0.4–1.8) | 0.8 (0.4–1.9) | 0.7 | 1.1 (0.7–1.7) | 1.2 (0.8–1.8) | 0.4 |
| Lymphoid Neoplasm | ||||||||||
| Multiple Myeloma | ref. | 1.1 (0.8–1.5) | 1.2 (0.9–1.6) | 0.3 | 1.3 (0.8–2.4) | 1.3 (0.7–2.4) | 0.3 | 1.1 (0.8–1.5) | 1.1 (0.8–1.6) | 0.5 |
| Hodgkin’s/Non-Hodgkin’s Lymphoma | ref. | 1.3 (1.0–1.6) | 1.3 (1.0–1.6) | 0.02 | 1.1 (0.7–1.7) | 1.1 (0.7–1.8) | 0.5 | 1.0 (0.8–1.3) | 1.0 (0.8–1.3) | 0.8 |
| Acute lymphoblastic leukemia/lymphocytic lymphoma | ref. | 0.8 (0.4–1.6) | 0.8 (0.4–1.7) | 0.6 | 1.7 (0.6–4.8) | 1.8 (0.6–5.3) | 0.3 | 1.4 (0.7–2.7) | 1.4 (0.7–2.8) | 0.4 |
| Hematologic Malignancy Type (n = 2236) | Chemotherapy (vs. no) | Radiotherapy (vs. no) | ||||
|---|---|---|---|---|---|---|
| Age-aHR (95%) | aHRa (95%) | p-value | Age-aHR (95%) | aHRa (95%) | p-value | |
| Myeloid Neoplasm | ||||||
| Acute myeloid leukemia | 2.4 (2.0–2.9) | 2.3 (1.8–2.8) | <0.0001 | 1.7 (1.3–2.3) | 1.5 (1.1–2.0) | 0.005 |
| Myelodysplastic syndrome | 1.5 (1.2–1.8) | 1.5 (1.2–1.8) | <0.0001 | 1.0 (0.8–1.2) | 0.9 (0.8–1.2) | 0.6 |
| Myeloproliferative Neoplasms | 1.3 (0.9–1.7) | 1.3 (0.9–1.7) | 0.1 | 0.9 (0.7–1.3) | 1.0 (0.7–1.4) | 0.8 |
| Lymphoid Neoplasm | ||||||
| Multiple Myeloma | 1.0 (0.8–1.3) | 1.0 (0.8–1.3) | 0.9 | 1.1 (0.8–1.4) | 1.1 (0.8–1.4) | 0.5 |
| Hodgkin’s/Non-Hodgkin’s Lymphoma | 0.9 (0.7–1.0) | 0.8 (0.7–1.1) | 0.06 | 1.2 (1.0–1.4) | 1.2 (1.0–1.5) | 0.05 |
| Acute lymphoblastic leukemia/lymphocytic lymphoma | 1.6 (1.0–2.6) | 1.7 (1.0–2.7) | 0.03 | 0.9 (0.5–1.6) | 0.8 (0.5–1.4) | 0.5 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jabagi, M.J.; Goncalves, A.; Vey, N.; Le Tri, T.; Zureik, M.; Dray-Spira, R. Risk of Hematologic Malignant Neoplasms after Postoperative Treatment of Breast Cancer. Cancers 2019, 11, 1463. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11101463
Jabagi MJ, Goncalves A, Vey N, Le Tri T, Zureik M, Dray-Spira R. Risk of Hematologic Malignant Neoplasms after Postoperative Treatment of Breast Cancer. Cancers. 2019; 11(10):1463. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11101463
Chicago/Turabian StyleJabagi, Marie Joelle, Anthony Goncalves, Norbert Vey, Thien Le Tri, Mahmoud Zureik, and Rosemary Dray-Spira. 2019. "Risk of Hematologic Malignant Neoplasms after Postoperative Treatment of Breast Cancer" Cancers 11, no. 10: 1463. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11101463