The Brain Penetrating and Dual TORC1/TORC2 Inhibitor, RES529, Elicits Anti-Glioma Activity and Enhances the Therapeutic Effects of Anti-Angiogenetic Compounds in Preclinical Murine Models

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Reagents and Drugs Preparation
2.2. Cell Lines and Cell Cultures
2.3. Cell Viability, Cell Cycle, and Apoptosis Analyses
2.4. Cell Lysates and Enzymatic Analysis
2.5. Glioblastoma Xenograft Model
2.6. Immunohistochemical Analyses
2.7. Orthotopic Intra-Cranial Model
2.8. Matrigel Plug Assay
2.9. Statistics
3. Results
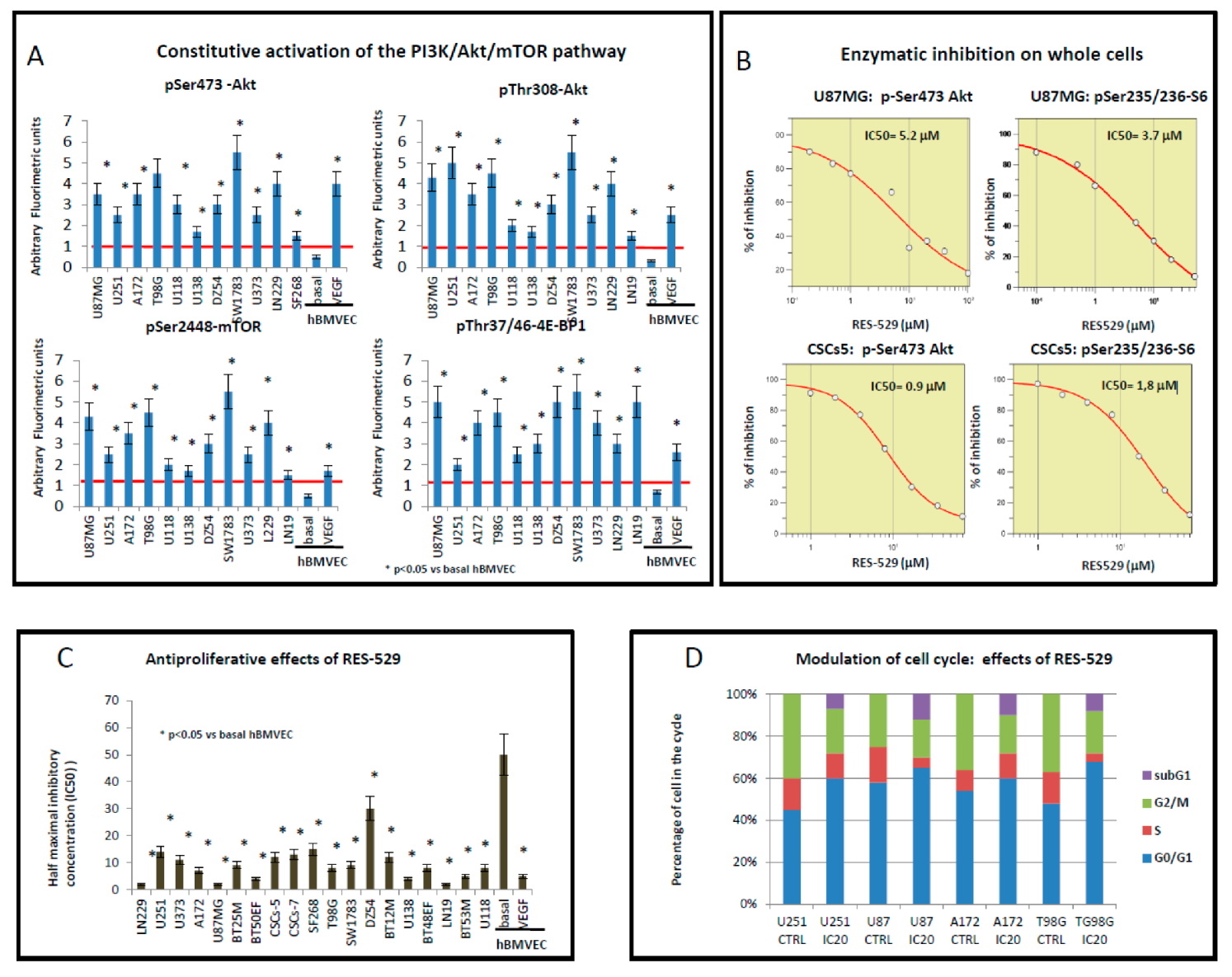
3.1. Antiproliferative Effects of RES529
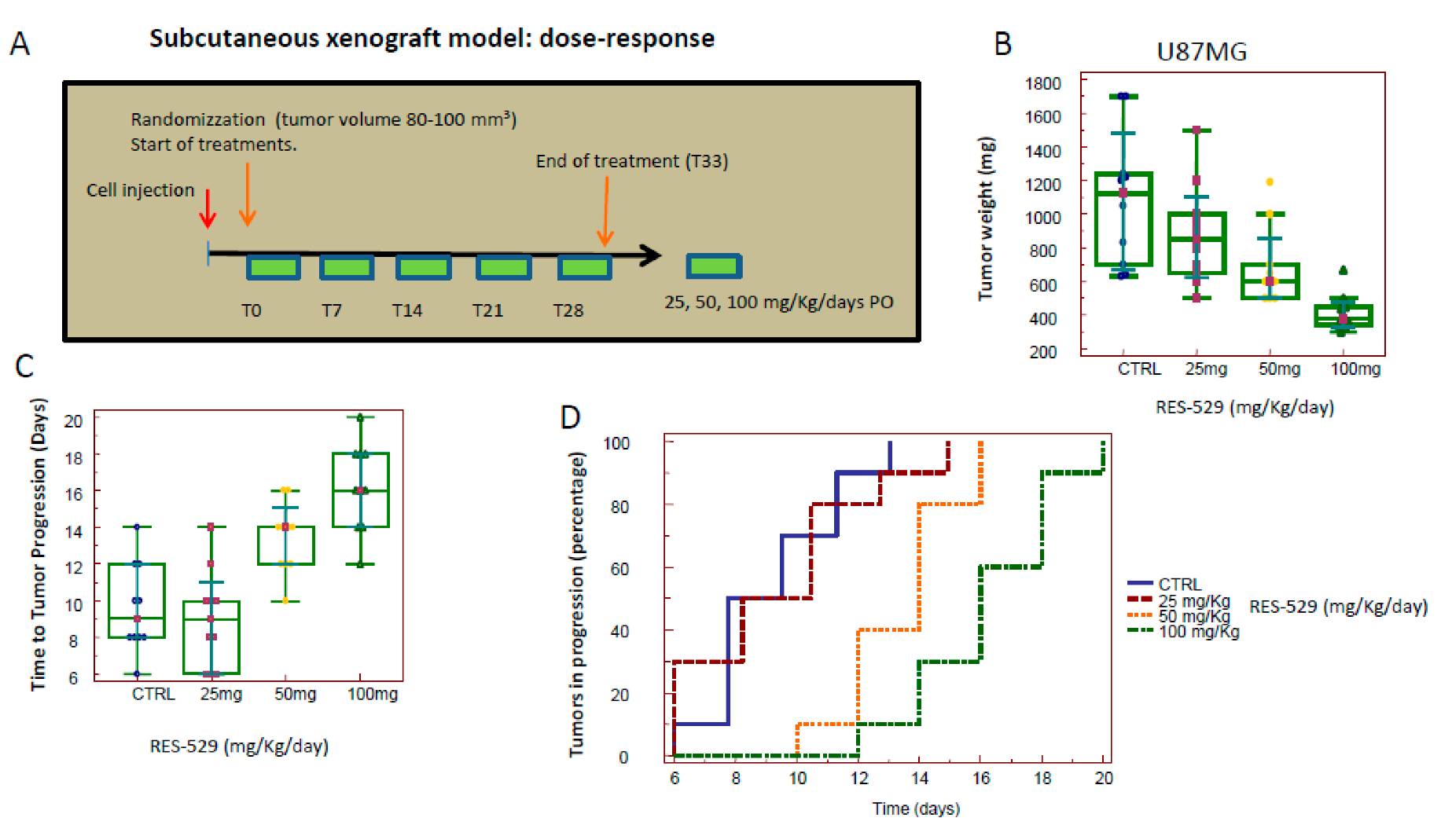
3.2. RES529 In Vivo Monotherapy
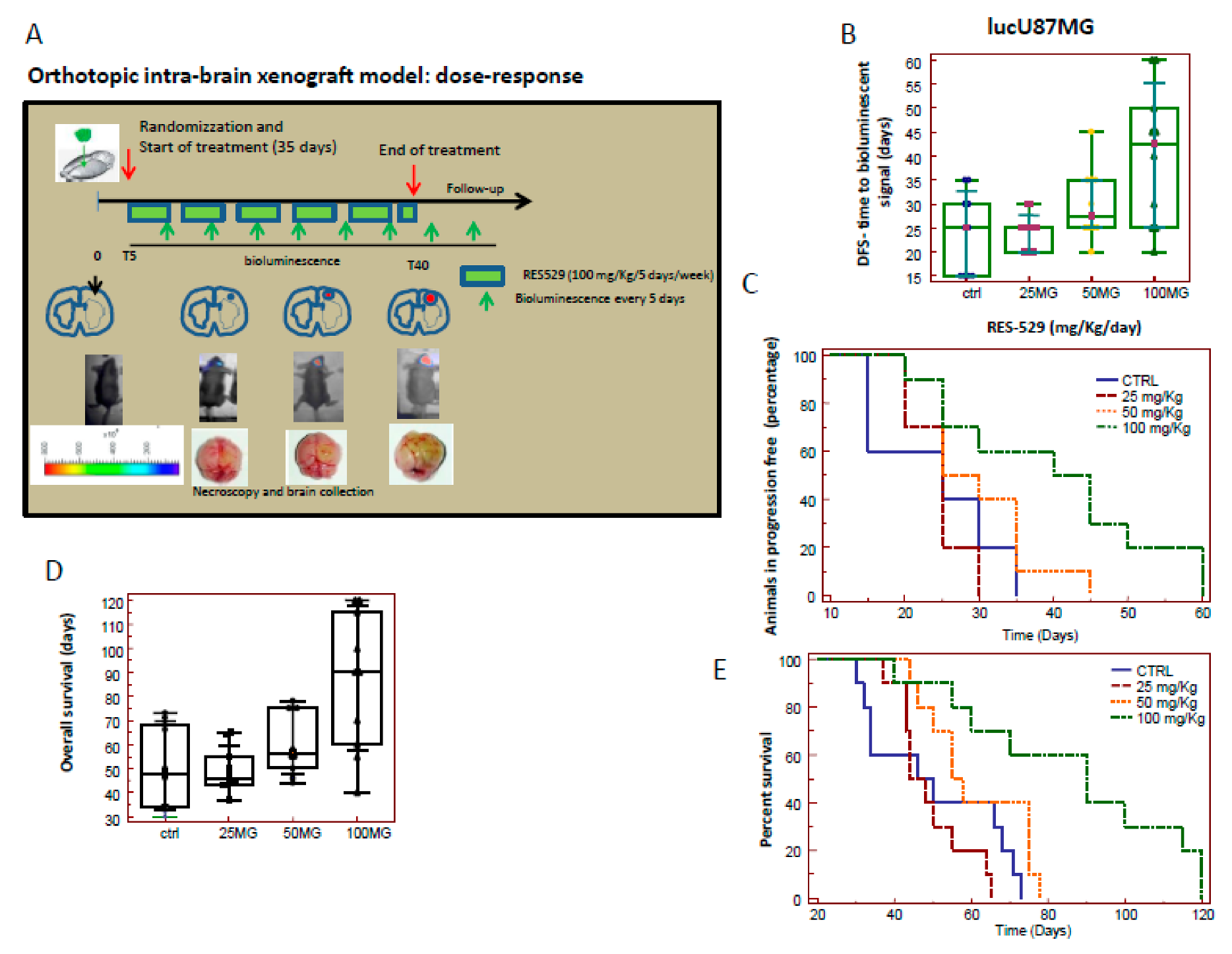
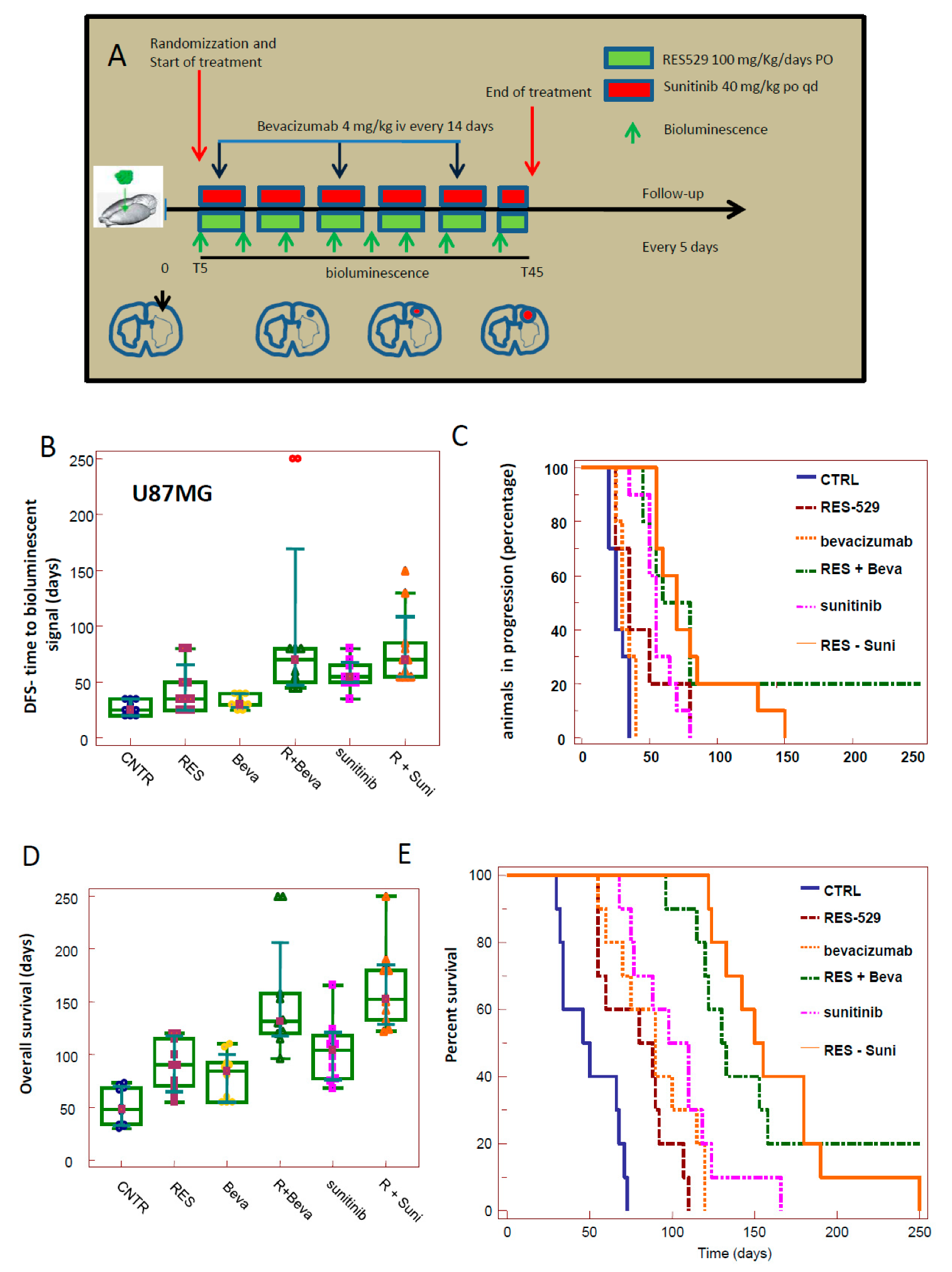
3.3. RES529 Increased Disease-Free and Overall Survival in Orthotopic Intra-Brain Tumours
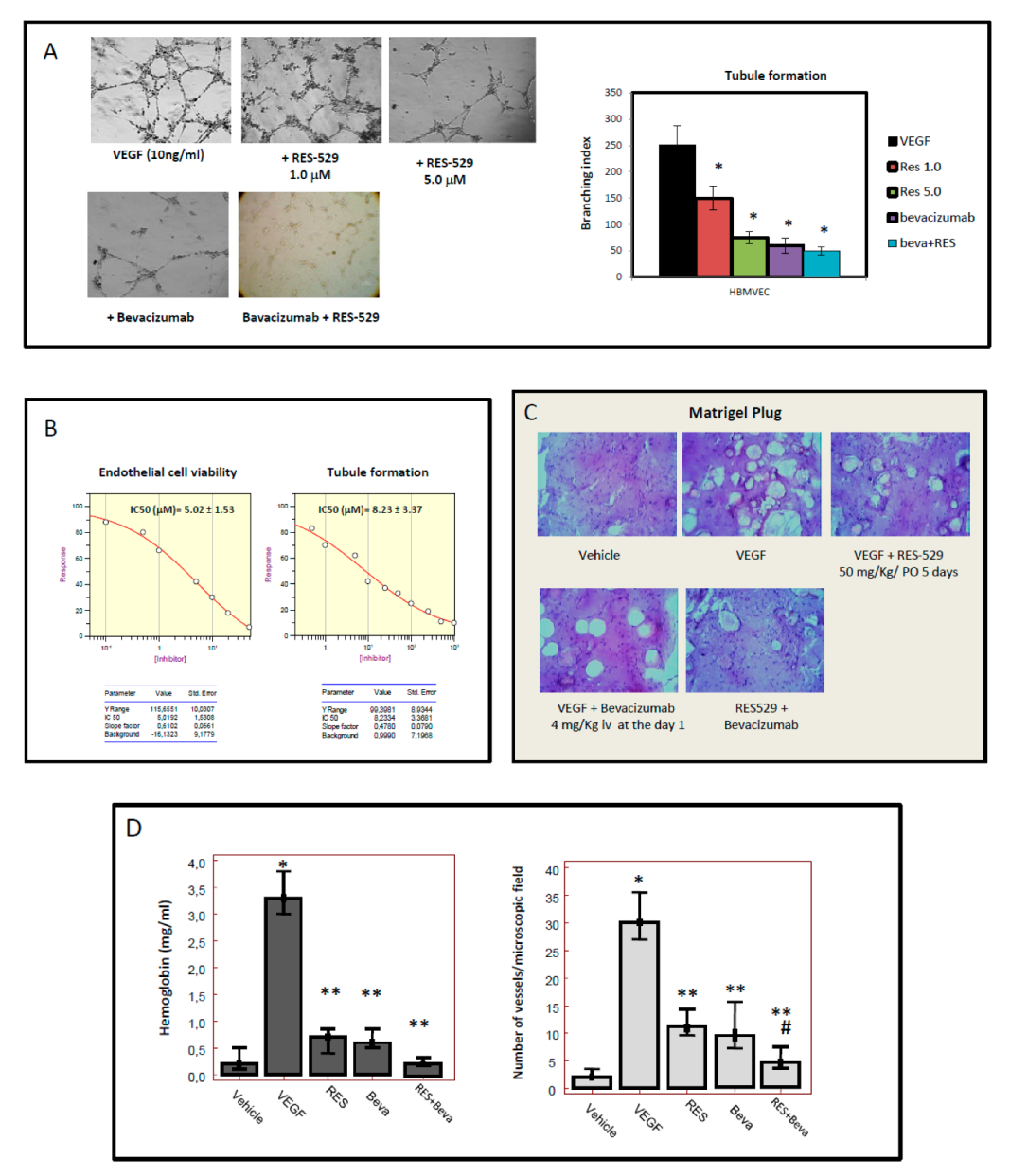
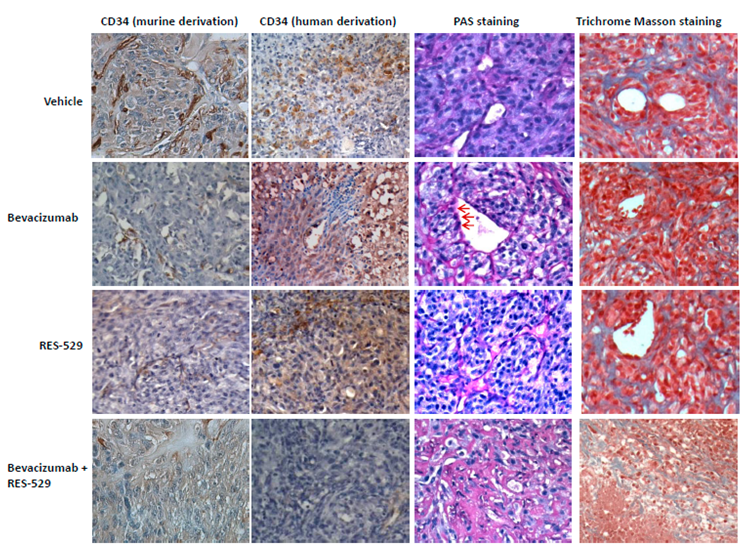
3.4. RES529 Blocks Angiogenesis and Vasculomimicry
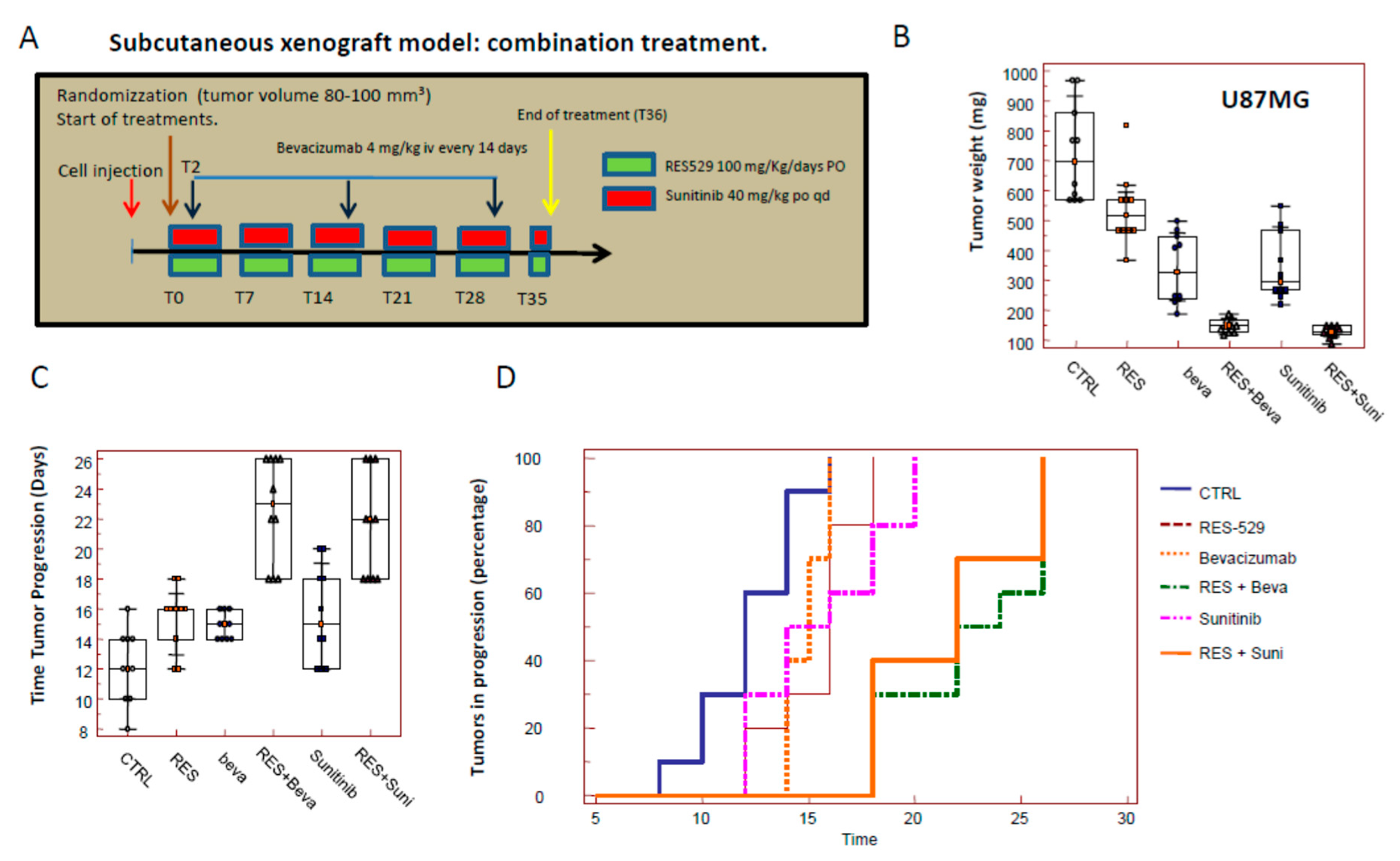
3.5. RES529 Shows Additive Effects with Anti-Angiogenetic Therapy In Vivo: (Subcutaneous Xenograft Model)
3.6. Histological Analyses
3.7. Orthotopic Intracranial Model with Luciferase U87MG Cells
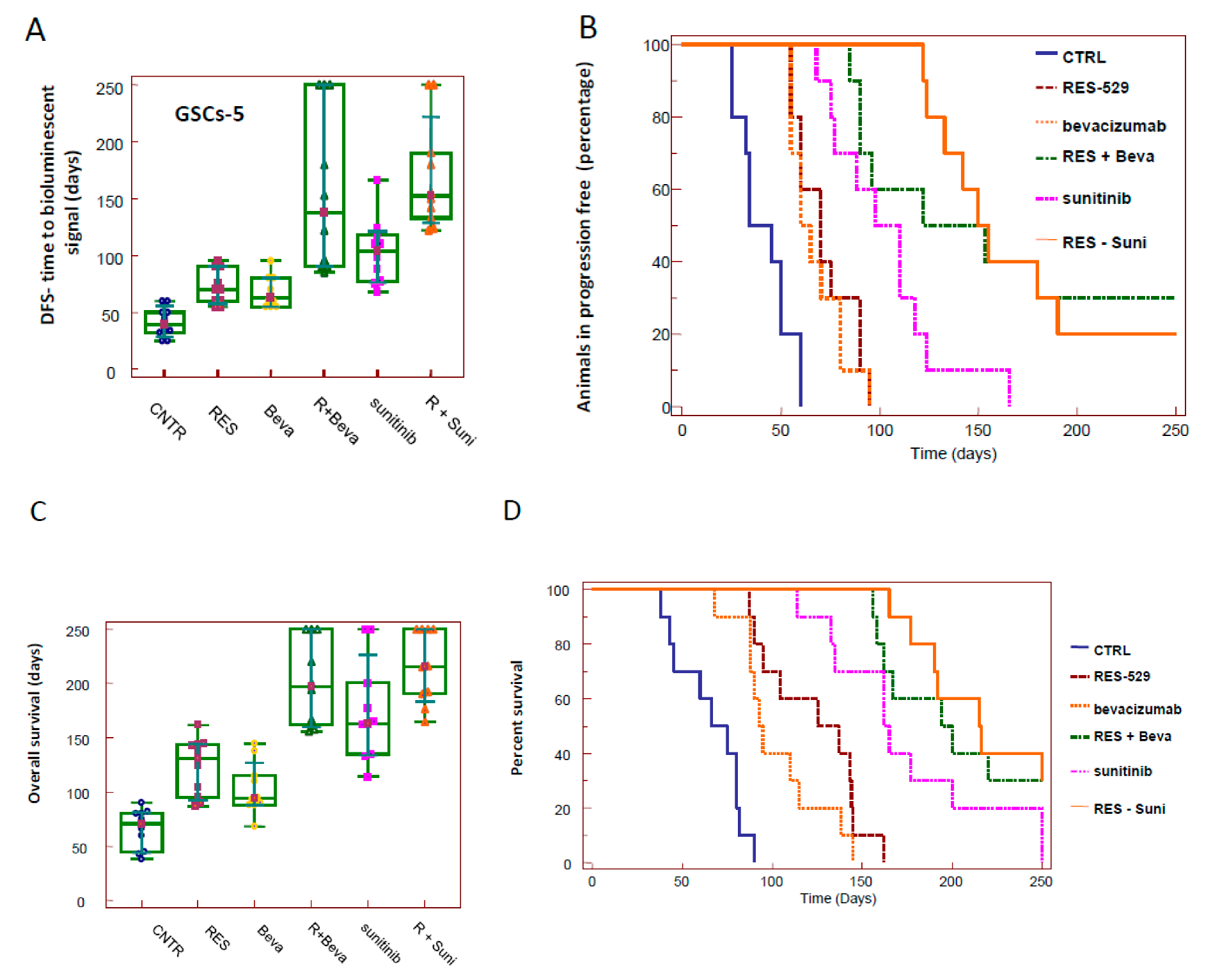
3.8. Orthotopic Intracranial Model with Tumor Propagating Cells
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ostrom, Q.T.; Gittleman, H.; Truitt, G.; Boscia, A.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2011–2015. Neuro Oncol. 2018, 20, iv1–iv86. [Google Scholar] [CrossRef] [PubMed]
- Lukas, R.V.; Wainwright, D.A.; Ladomersky, E.; Sachdev, S.; Sonabend, A.M.; Stupp, R. Newly Diagnosed Glioblastoma: A Review on Clinical Management. Oncology 2019, 33, 91–100. [Google Scholar] [PubMed]
- Scully, S.; Francescone, R.; Faibish, M.; Bentley, B.; Taylor, S.L.; Oh, D.; Schapiro, R.; Moral, L.; Yan, W.; Shao, R. Transdifferentiation of glioblastoma stem-like cells into mural cells drives vasculogenic mimicry in glioblastomas. J. Neurosci. 2012, 32, 12950–12960. [Google Scholar] [CrossRef] [PubMed]
- Hardee, M.E.; Zagzag, D. Mechanisms of glioma-associated neovascularization. Am. J. Pathol. 2012, 181, 1126–1141. [Google Scholar] [CrossRef] [PubMed]
- Sobol-Milejska, G.; Mizia-Malarz, A.; Musiol, K.; Chudek, J.; Bożentowicz-Wikarek, M.; Wos, H.; Mandera, M. Serum levels of vascular endothelial growth factor and basic fibroblast growth factor in children with brain tumors. Adv. Clin. Exp. Med. 2017, 26, 571–575. [Google Scholar] [CrossRef] [PubMed]
- De Gramont, A.; Van Cutsem, E. Investigating the potential of bevacizumab in other indications: Metastatic renal cell, non-small cell lung, pancreatic and breast cancer. Oncology 2005, 69, 46–56. [Google Scholar] [CrossRef]
- Webb, T. Vascular normalization: Study examines how antiangiogenesis therapies work. J. Natl. Cancer Inst. 2005, 97, 336–337. [Google Scholar] [CrossRef]
- Cohen, M.H.; Shen, Y.L.; Keegan, P.; Pazdur, R. FDA drug approval summary: Bevacizumab (Avastin) as treatment of rGBM. BMC Cancer 2009, 14, 1131–1138. [Google Scholar]
- Gutin, P.H.; Iwamoto, F.M.; Beal, K.; Mohile, N.A.; Karimi, S.; Hou, B.L.; Lymberis, S.; Yamada, Y.; Chang, J.; Abrey, L.E. Safety and efficacy of bevacizumab with hypofractionated stereotactic irradiation for recurrent malignant gliomas. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 156–163. [Google Scholar] [CrossRef]
- Chamberlain, M.C.; Johnston, S.K. Salvage therapy with single agent bevacizumab for recurrent glioblastoma. J. Neuro-Oncol. 2010, 96, 259–269. [Google Scholar] [CrossRef]
- Higa, G.M.; Abraham, J. Biological mechanisms of bevacizumab-associated adverse events. Expert Rev. Anticancer Ther. 2009, 9, 999–1007. [Google Scholar] [CrossRef] [PubMed]
- Cachia, D.; Elshafeey, N.A.; Kamiya-Matsuoka, C.; Hatami, M.; Alfaro-Munoz, K.D.; Mandel, J.J.; Colen, R.; DeGroot, J.F. Radiographic patterns of progression with associated outcomes after bevacizumab therapy in glioblastoma patients. J. Neuro-Oncol. 2017, 135, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Urup, T.; Staunstrup, L.M.; Michaelsen, S.R.; Vitting-Seerup, K.; Bennedbæk, M.; Toft, A.; Olsen, L.R.; Jønson, L.; Issazadeh-Navikas, S.; Broholm, H.; et al. Transcriptional changes induced by bevacizumab combination therapy in responding and non-responding recurrent glioblastoma patients. BMC Cancer 2017, 17, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Mu, L.; Yang, C.; Gao, Q.; Long, Y.; Ge, H.; DeLeon, G.; Jin, L.; Chang, Y.E.; Sayour, E.J.; Ji, J.; et al. CD4+ and Perivascular Foxp3+ T Cells in Glioma Correlate with Angiogenesis and Tumor Progression. Front. Immunol. 2017, 8, 1451. [Google Scholar] [CrossRef] [PubMed]
- Tamura, R.; Tanaka, T.; Ohara, K.; Miyake, K.; Morimoto, Y.; Yamamoto, Y.; Kanai, R.; Akasaki, Y.; Murayama, Y.; Tamiya, T.; et al. Persistent restoration to the immunosupportive tumor microenvironment in glioblastoma by bevacizumab. Cancer Sci. 2019, 110, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Gravina, G.L.; Mancini, A.; Marampon, F.; Colapietro, A.; Delle Monache, S.; Sferra, R.; Vitale, F.; Richardson, P.J.; Patient, L.; Burbidge, S.; et al. The brain-penetrating CXCR4 antagonist, PRX177561, increases the antitumor effects of bevacizumab and sunitinib in preclinical models of human glioblastoma. J. Hematol. Oncol. 2017, 10, 5–21. [Google Scholar] [CrossRef] [PubMed]
- Kwiatkowski, S.C.; Guerrero, P.A.; Hirota, S.; Chen, Z.; Morales, J.E.; Aghi, M.; McCarty, J.H. Neuropilin-1 modulates TGFβ signaling to drive glioblastoma growth and recurrence after anti-angiogenic therapy. PLoS ONE 2017, 12, e0185065. [Google Scholar] [CrossRef]
- Festuccia, C.; Gravina, G.L.; Giorgio, C.; Mancini, A.; Pellegrini, C.; Colapietro, A.; Delle Monache, S.; Maturo, M.G.; Sferra, R.; Chiodelli, P.; et al. UniPR1331, a small molecule targeting Eph/ephrin interaction, prolongs survival in glioblastoma and potentiates the effect of antiangiogenic therapy in mice. Oncotarget 2018, 9, 24347–24363. [Google Scholar] [CrossRef]
- Gabrusiewicz, K.; Liu, D.; Cortes-Santiago, N.; Hossain, M.B.; Conrad, C.A.; Aldape, K.D.; Fuller, G.N.; Marini, F.C.; Alonso, M.M.; Idoate, M.A.; et al. Anti-vascular endothelial growth factor therapy-induced glioma invasion is associated with accumulation of Tie2-expressing monocytes. Oncotarget 2014, 5, 2208–2220. [Google Scholar] [CrossRef] [Green Version]
- Goyal, P.; Tenenbaum, M.; Gupta, S.; Kochar, P.S.; Bhatt, A.A.; Mangla, M.; Kumar, Y.; Mangla, R. Survival prediction based on qualitative MRI diffusion signature in patients with recurrent high grade glioma treated with bevacizumab. Quant. Imaging Med. Surg. 2018, 8, 268–279. [Google Scholar] [CrossRef] [Green Version]
- Shimizu, T.; Ishida, J.; Kurozumi, K.; Ichikawa, T.; Otani, Y.; Oka, T.; Tomita, Y.; Hattori, Y.; Uneda, A.; Matsumoto, Y.; et al. δ-catenin promotes bevacizumab-induced glioma invasion. Mol. Cancer Ther. 2019, 18, 812–822. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Zhang, C.; Cui, M.; Niu, J.; Ding, W. Inhibition of Bevacizumab-induced Epithelial-Mesenchymal Transition by BATF2 Overexpression Involves the Suppression of Wnt/β-Catenin Signaling in Glioblastoma Cells. Anticancer Res. 2017, 37, 4285–4294. [Google Scholar] [PubMed]
- De Boüard, S.; Herlin, P.; Christensen, J.G.; Lemoisson, E.; Gauduchon, P.; Raymond, E.; Guillamo, J.S. Antiangiogenic and anti-invasive effects of sunitinib on experimental human glioblastoma. Neuro-Oncol. 2007, 9, 412–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatipoglu, G.; Hock, S.W.; Weiss, R.; Fan, Z.; Sehm, T.; Ghoochani, A.; Buchfelder, M.; Savaskan, N.E.; Eyüpoglu, I.Y. Sunitinib impedes brain tumor progression and reduces tumor-induced neurodegeneration in the microenvironment. Cancer Sci. 2015, 106, 160–170. [Google Scholar] [CrossRef]
- D’Amico, R.; Lei, L.; Kennedy, B.C.; Sisti, J.; Ebiana, V.; Crisman, C.; Christensen, J.G.; Gil, O.; Rosenfeld, S.S.; Canoll, P.; et al. The addition of Sunitinib to radiation delays tumor growth in a murine model of glioblastoma. Neurol. Res. 2012, 34, 252–261. [Google Scholar] [CrossRef] [Green Version]
- Wuthrick, E.J.; Curran WJJr Camphausen, K.; Lin, A.; Glass, J.; Evans, J.; Andrews, D.W.; Axelrod, R.; Shi, W.; Werner-Wasik, M.; Haacke, E.M.; et al. A pilot study of hypofractionated stereotactic radiation therapy and sunitinib in previously irradiated patients with recurrent high-grade glioma. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 369–375. [Google Scholar] [CrossRef]
- Brennan, C.W.; Verhaak, R.G.; McKenna, A.; Campos, B.; Noushmehr, H.; Salama, S.R.; Zheng, S.; Chakravarty, D.; Sanborn, J.Z.; Berman, S.H.; et al. The somatic genomic landscape of glioblastoma. Cell 2013, 155, 462–477. [Google Scholar] [CrossRef]
- Gallia, G.L.; Rand, V.; Siu, I.M.; Eberhart, C.G.; James, C.D.; Marie, S.K.; Oba-Shinjo, S.M.; Carlotti, C.G.; Caballero, O.L.; Simpson, A.J. PIK3CA gene mutations in pediatric and adult glioblastoma multiforme. Mol. Cancer Res. 2006, 4, 709–714. [Google Scholar] [CrossRef]
- Stichel, D.; Ebrahimi, A.; Reuss, D.; Schrimpf, D.; Ono, T.; Shirahata, M.; Reifenberger, G.; Weller, M.; Hänggi, D.; Wick, W.; et al. Distribution of EGFR amplification, combined chromosome 7 gain and chromosome 10 loss, and TERT promoter mutation in brain tumors and their potential for the reclassification of IDHwt astrocytoma to glioblastoma. Acta Neuropathol. 2018, 136, 793–803. [Google Scholar] [CrossRef] [Green Version]
- McNeill, R.S.; Stroobant, E.E.; Smithberger, E.; Canoutas, D.A.; Butler, M.K.; Shelton, A.K.; Patel, S.D.; Limas, J.C.; Skinner, K.R.; Bash, R.E.; et al. PIK3CA missense mutations promote glioblastoma pathogenesis, but do not enhance targeted PI3K inhibition. PLoS ONE 2018, 13, e0200014. [Google Scholar] [CrossRef]
- Sonoda, Y.; Ozawa, T.; Aldape, K.D.; Deen, D.F.; Berger, M.S.; Pieper, R.O. Akt pathway activation converts anaplastic astrocytoma to glioblastoma multiforme in a human astrocyte model of glioma. Cancer Res. 2001, 61, 6674–6678. [Google Scholar] [PubMed]
- Chakravarti, A.; Zhai, G.; Suzuki, Y.; Sarkesh, S.; Black, P.M.; Muzikansky, A.; Loeffler, J.S. The prognostic significance of phosphatidylinositol 3-kinase pathway activation in human gliomas. J. Clin. Oncol. 2004, 22, 1926–1933. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Shoemaker, A.R.; Liu, X.; Woods, K.W.; Thomas, S.A.; de Jong, R.; Han, E.K.; Li, T.; Stoll, V.S.; Powlas, J.A.; et al. Potent and selective inhibitors of Akt kinases slow the progress of tumors in vivo. Mol. Cancer Ther. 2005, 4, 977–986. [Google Scholar] [CrossRef] [PubMed]
- Fan, Q.W.; Nicolaides, T.P.; Weiss, W.A. Inhibiting 4EBP1 in Glioblastoma. Clin. Cancer Res. 2018, 24, 14–21. [Google Scholar] [CrossRef]
- Becker, C.M.; Oberoi, R.K.; McFarren, S.J.; Muldoon, D.M.; Pafundi, D.H.; Pokorny, J.L.; Brinkmann, D.H.; Ohlfest, J.R.; Sarkaria, J.N.; Largaespada, D.A.; et al. Decreased affinity for efflux transporters increases brain penetrance and molecular targeting of a PI3K/mTOR inhibitor in a mouse model of glioblastoma. Neuro Oncol. 2015, 17, 1210–1219. [Google Scholar] [CrossRef] [Green Version]
- Tian, T.; Li, X.; Zhang, J. mTOR signaling in cancer and mTOR inhibitors in solid tumor targeting therapy. Int. J. Mol. Sci. 2019, 20, 755. [Google Scholar] [CrossRef]
- Zhao, H.F.; Wang, J.; Shao, W.; Wu, C.P.; Chen, Z.P.; To, S.T.; Li, W.P. Recent advances in the use of PI3K inhibitors for glioblastoma multiforme: Current preclinical and clinical development. Mol. Cancer 2017, 16, 100. [Google Scholar] [CrossRef]
- Martelli, A.M.; Buontempo, F.; McCubrey, J.A. Drug discovery targeting the mTOR pathway. Clin. Sci. 2018, 132, 543–568. [Google Scholar] [CrossRef]
- El Shamieh, S.; Saleh, F.; Moussa, S.; Kattan, J.; Farhat, F. RICTOR gene amplification is correlated with metastasis and therapeutic resistance in triple-negative breast cancer. Pharmacogenomics 2018, 19, 757–760. [Google Scholar] [CrossRef]
- Masui, K.; Cavenee, W.K.; Mischel, P.S. mTORC2 and metabolic reprogramming in GBM: At the interface of genetics and environment. Brain Pathol. 2015, 25, 755–759. [Google Scholar] [CrossRef]
- Xue, Q.; Hopkins, B.; Perruzzi, C.; Udayakumar, D.; Sherris, D.; Benjamin, L.E. Palomid 529, a novel small-molecule drug, is a TORC1/TORC2 inhibitor that reduces tumor growth, tumor angiogenesis, and vascular permeability. Cancer Res. 2008, 68, 9551–9557. [Google Scholar] [CrossRef] [PubMed]
- Gravina, G.L.; Marampon, F.; Sherris, D.; Vittorini, F.; Di Cesare, E.; Tombolini, V.; Lenzi, A.; Jannini, E.A.; Festuccia, C. Torc1/Torc2 inhibitor, Palomid 529, enhances radiation response modulating CRM1-mediated survivin function and delaying DNA repair in prostate cancer models. Prostate 2014, 74, 852–868. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, M.A. RES-529: A PI3K/AKT/mTOR pathway inhibitor that dissociates the mTORC1 and mTORC2 complexes. Anticancer Drugs 2016, 27, 475–487. [Google Scholar] [CrossRef] [PubMed]
- Lin, F.; Buil, L.; Sherris, D.; Beijnen, J.H.; van Tellingen, O. Dual mTORC1 and mTORC2 inhibitor Palomid 529 penetrates the blood-brain barrier without restriction by ABCB1 and ABCG2. Int. J. Cancer 2013, 133, 1222–1233. [Google Scholar] [CrossRef]
- De Vries, N.A.; Beijnen, J.H.; Boogerd, W.; van Tellingen, O. Blood-brain barrier and chemotherapeutic treatment of brain tumors. Expert Rev. Neurother. 2006, 6, 1199–1209. [Google Scholar] [CrossRef]
- Oberoi, R.K.; Parrish, K.E.; Sio, T.T.; Mittapalli, R.K.; Elmquist, W.F.; Sarkaria, J.N. Strategies to improve delivery of anticancer drugs across the blood-brain barrier to treat glioblastoma. Neuro Oncol. 2016, 18, 27–36. [Google Scholar] [CrossRef]
- Luchman, H.A.; Stechishin, O.D.; Dang, N.H.; Blough, M.D.; Chesnelong, C.; Kelly, J.J.; Nguyen, S.A.; Chan, J.A.; Weljie, A.M.; Cairncross, J.G.; et al. An in vivo patient-derived model of endogenous IDH1-mutant glioma. Neuro Oncol. 2012, 14, 184–191. [Google Scholar] [CrossRef]
- Mendiburu-Eliçabe, M.; Gil-Ranedo, J.; Izquierdo, M. Efficacy of rapamycin against glioblastoma cancer stem cells. Clin. Transl. Oncol. 2014, 16, 495–502. [Google Scholar] [CrossRef]
- Gravina, G.L.; Mancini, A.; Colapietro, A.; Delle Monache, S.; Sferra, R.; Vitale, F.; Cristiano, L.; Martellucci, S.; Marampon, F.; Mattei, V.; et al. The Small Molecule Ephrin Receptor Inhibitor, GLPG1790, Reduces Renewal Capabilities of Cancer Stem Cells, Showing Anti-Tumour Efficacy on Preclinical Glioblastoma Models. Cancers 2019, 11, 359. [Google Scholar] [CrossRef]
- Gravina, G.L.; Mancini, A.; Mattei, C.; Vitale, F.; Marampon, F.; Colapietro, A.; Rossi, G.; Ventura, L.; Vetuschi, A.; Di Cesare, E.; et al. Enhancement of radiosensitivity by the novel anticancer quinolone derivative vosaroxin in preclinical glioblastoma models. Oncotarget 2017, 8, 29865–29886. [Google Scholar] [CrossRef] [Green Version]
- Baumann, B.C.; Dorsey, J.F.; Benci, J.L.; Joh, D.Y.; Kao, G.D. Stereotactic intracranial implantation and in vivo bioluminescent imaging of tumor xenografts in a mouse model system of glioblastoma multiforme. J. Vis. Exp. 2012, 67, 4089. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Song, Q.; Wei, C.; Qu, J. LRIG1 inhibits hypoxia-induced vasculogenic mimicry formation via suppression of the EGFR/PI3K/AKT pathway and epithelial-to-mesenchymal transition in human glioma SHG-44 cells. Cell Stress Chaperones. 2015, 20, 631–641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jhanwar-Uniyal, M.; Jeevan, D.; Neil, J.; Shannon, C.; Albert, L.; Murali, R. Deconstructing mTOR complexes in regulation of Glioblastoma Multiforme and its stem cells. Adv. Biol. Regul. 2013, 53, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Luchman, H.A.; Stechishin, O.D.; Nguyen, S.A.; Lun, X.Q.; Cairncross, J.G.; Weiss, S. Dual mTORC1/2 blockade inhibits glioblastoma brain tumor initiating cells in vitro and in vivo and synergizes with temozolomide to increase orthotopic xenograft survival. Clin. Cancer Res. 2014, 20, 5756–5767. [Google Scholar] [CrossRef] [PubMed]
- Jhanwar-Uniyal, M.; Amin, A.G.; Cooper, J.B.; Das, K.; Schmidt, M.H.; Murali, R. Discrete signaling mechanisms of mTORC1 and mTORC2: Connected yet apart in cellular and molecular aspects. Adv. Biol. Regul. 2017, 64, 39–48. [Google Scholar] [CrossRef]
- Ramezani, S.; Vousooghi, N.; Kapourchali, F.R.; Hadjighasem, M.; Hayat, P.; Amini, N.; Joghataei, M.T. Rolipram potentiates bevacizumab-induced cell death in human glioblastoma stem-like cells. Life Sci. 2017, 73, 11–19. [Google Scholar] [CrossRef]
- Akhavan, D.; Cloughesy, T.F.; Mischel, P.S. mTOR signaling in glioblastoma: Lessons learned from bench to bedside. Neuro Oncol. 2010, 12, 882–889. [Google Scholar] [CrossRef]
- Burger, M.C.; Breuer, S.; Cieplik, H.C.; Harter, P.N.; Franz, K.; Bähr, O.; Steinbach, J.P. Bevacizumab for Patients with Recurrent Multifocal Glioblastomas. Int. J. Mol. Sci. 2017, 18, 2469. [Google Scholar] [CrossRef]
- Zhang, W.; Qiu, X.G.; Chen, B.S.; Li, S.W.; Cui, Y.; Ren, H.; Jiang, T. Antiangiogenic therapy with bevacizumab in recurrent malignant gliomas: Analysis of the response and core pathway aberrations. Chin. Med. J. 2009, 122, 1250–1254. [Google Scholar]
- Mendiburu-Elicabe, M.; Yin, D.; Hadaczek, P.; Zhai, Y.; Forsayeth, J.; Bankiewicz, K.S. Systemic rapamycin alone may not be a treatment option for malignant glioma: Evidence from an in vivo study. J. Neurooncol. 2012, 108, 53–58. [Google Scholar] [CrossRef]
- McCarty, J.H. Glioblastoma resistance to anti-VEGF therapy: Has the challenge been MET? Clin. Cancer Res. 2013, 19, 1631–1633. [Google Scholar] [CrossRef]
- Piao, Y.; Park, S.Y.; Henry, V.; Smith, B.D.; Tiao, N.; Flynn, D.L.; de Groot, J.F. Novel MET/TIE2/VEGFR2 inhibitor altiratinib inhibits tumor growth and invasiveness in bevacizumab-resistant glioblastoma mouse models. Neuro Oncol. 2016, 18, 1230–1241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mimeault, M.; Hauke, R.; Mehta, P.P.; Batra, S.K. Recent advances in cancer stem/progenitor cell research: Therapeutic implications for overcoming resistance to the most aggressive cancers. J. Cell. Mol. Med. 2007, 11, 981–1011. [Google Scholar] [CrossRef] [PubMed]
- Gravina, G.L.; Marampon, F.; Petini, F.; Biordi, L.; Sherris, D.; Jannini, E.A.; Tombolini, V.; Festuccia, C. The TORC1/TORC2 inhibitor, Palomid 529, reduces tumor growth and sensitizes to docetaxel and cisplatin in aggressive and hormone-refractory prostate cancer cells. Endocr. Relat. Cancer 2011, 18, 385–400. [Google Scholar] [CrossRef]
- Lassen, U.; Sorensen, M.; Gaziel, T.B.; Hasselbalch, B.; Poulsen, H.S. Phase II study of bevacizumab and temsirolimus combination therapy for recurrent glioblastoma multiforme. Anticancer Res. 2013, 33, 1657–1660. [Google Scholar] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Experiment # | Experimental Model | Injected Cells | Treatments and Groups | Mice for Group | Experimental Measures and Endpoints |
|---|---|---|---|---|---|
| 01 | Subcutaneous xenograft | U87MG 1 × 106/tumor | RES529 group (25 mg/kg/day) RES529 group (50 mg/kg/day) RES529 group (100 mg/kg/day) | 5 animals/group (2 tumors/animal) |
|
| 02 | Subcutaneous xenograft | A172 1 × 106/tumor | RES529 group (25 mg/kg/day) RES529 group (50 mg/kg/day) RES529 group (100 mg/kg/day) | 5 animals/group 2 tumors/animal |
|
| 03 | Subcutaneous xenograft | T98G 1 × 106/tumor | RES529 group (25 mg/kg/day) RES529 group (50 mg/kg/day) RES529 group (100 mg/kg/day) | 5 animals/group 2 tumors/animal |
|
| 04 | Orthotopic Intracranial xenograft | U87MG 1 × 103 | RES529 group (25 mg/kg/day) RES529 group (50 mg/kg/day) RES529 group (100 mg/kg/day) | 10 animals/group |
|
| 05 | Subcutaneous xenograft | U87MG 1 × 106/tumor | RES529 (50 mg/kg every day); Bevacizumab (4 mg/kg iv every 14 days) Sunitinib (40 mg/kg po qd) RES529 + Bevacizumab RES529 + Sunitinib | 5 animals/group 2 tumors/animal |
|
| 06 | Subcutaneous xenograft | A172 1 × 106/tumor | RES529 (50 mg/kg every day); Bevacizumab (4 mg/kg iv every 14 days) Sunitinib (40 mg/kg po qd) RES529 + Bevacizumab RES529 + Sunitinib | 5 animals/group 2 tumors/animal |
|
| 07 | Orthotopic Intracranial xenograft | U87MG 1 × 103 | RES529 (100 mg/kg every day); Bevacizumab (4 mg/kg iv every 14 days) Sunitinib (40 mg/kg po qd) RES529 + Bevacizumab RES529 + Sunitinib | 10 animals/group |
|
| 08 | Orthotopic Intracranial xenograft | GSCs-5 1 × 103 | RES529 (100 mg/kg every day); Bevacizumab (4 mg/kg iv every 14 days) Sunitinib (40 mg/kg po qd) RES529 + Bevacizumab RES529 + Sunitinib | 10 animals/group |
|
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gravina, G.L.; Mancini, A.; Colapietro, A.; Delle Monache, S.; Sferra, R.; Pompili, S.; Vitale, F.; Martellucci, S.; Marampon, F.; Mattei, V.; et al. The Brain Penetrating and Dual TORC1/TORC2 Inhibitor, RES529, Elicits Anti-Glioma Activity and Enhances the Therapeutic Effects of Anti-Angiogenetic Compounds in Preclinical Murine Models. Cancers 2019, 11, 1604. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11101604
Gravina GL, Mancini A, Colapietro A, Delle Monache S, Sferra R, Pompili S, Vitale F, Martellucci S, Marampon F, Mattei V, et al. The Brain Penetrating and Dual TORC1/TORC2 Inhibitor, RES529, Elicits Anti-Glioma Activity and Enhances the Therapeutic Effects of Anti-Angiogenetic Compounds in Preclinical Murine Models. Cancers. 2019; 11(10):1604. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11101604
Chicago/Turabian StyleGravina, Giovanni Luca, Andrea Mancini, Alessandro Colapietro, Simona Delle Monache, Roberta Sferra, Simona Pompili, Flora Vitale, Stefano Martellucci, Francesco Marampon, Vincenzo Mattei, and et al. 2019. "The Brain Penetrating and Dual TORC1/TORC2 Inhibitor, RES529, Elicits Anti-Glioma Activity and Enhances the Therapeutic Effects of Anti-Angiogenetic Compounds in Preclinical Murine Models" Cancers 11, no. 10: 1604. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11101604