NF1 Patients Receiving Breast Cancer Screening: Insights from The Ontario High Risk Breast Screening Program


Abstract
:1. Introduction
2. Results
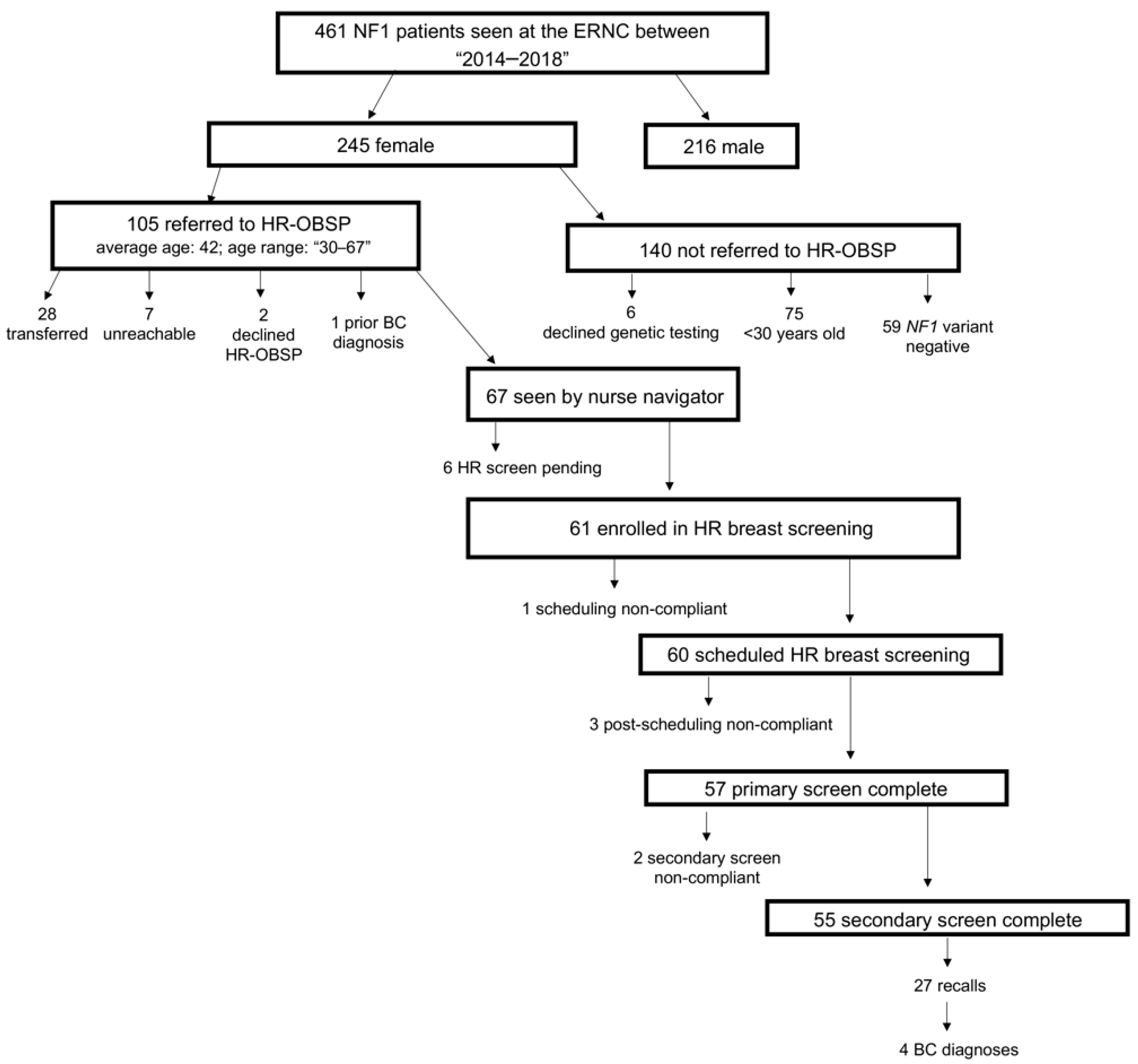
2.1. Patient Population
2.2. Imaging Findings
2.3. Patient Screening Uptake
2.4. Breast Cancer Incidence in NF1 Patients Receiving High-Risk Screening
2.5. Family History in NF1 Patients Enrolled in High-Risk Screening
2.6. HR-OBSP Screen Scheduling
3. Discussion
4. Materials and Methods
4.1. Patient Population
4.2. Data Collection and Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Uusitalo, E.; Leppävirta, J.; Koffert, A.; Suominen, S.; Vahtera, J.; Vahlberg, T.; Pöyhönen, M.; Peltonen, J.; Peltonen, S. Incidence and mortality of neurofibromatosis: A total population study in Finland. J. Invest. Dermatol. 2015, 135, 904–906. [Google Scholar] [CrossRef] [PubMed]
- Huson, S.M.; Compston, D.A.; Clark, P.; Harper, P.S. A genetic study of von Recklinghausen neurofibromatosis in south east Wales. I. Prevalence, fitness, mutation rate, and effect of parental transmission on severity. J. Med. Genet. 1989, 26, 704–711. [Google Scholar] [CrossRef] [PubMed]
- Ferner, R.E.; Huson, S.M.; Thomas, N.; Moss, C.; Willshaw, H.; Evans, D.G.; Upadhyaya, M.; Towers, R.; Gleeson, M.; Steiger, C.; et al. Guidelines for the diagnosis and management of individuals with neurofibromatosis 1. J. Med. Genet. 2006, 44, 81–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jett, K.; Friedman, J.M. Clinical and genetic aspects of neurofibromatosis 1. Genet. Med. 2010, 12, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Elefteriou, F.; Kolanczyk, M.; Schindeler, A.; Viskochil, D.H.; Hock, J.M.; Schorry, E.K.; Crawford, A.H.; Friedman, J.M.; Little, D.; Peltonen, J.; et al. Skeletal abnormalities in neurofibromatosis type 1: Approaches to therapeutic options. Am. J. Med. Genet. A 2009, 149, 2327–2338. [Google Scholar] [CrossRef] [PubMed]
- Szudek, J.; Birch, P.; Riccardi, V.M.; Evans, D.G.; Friedman, J.M. Associations of clinical features in neurofibromatosis 1 (NF1). Genet. Epidemiol. 2000, 19, 429–439. [Google Scholar] [CrossRef]
- Uusitalo, E.; Rantanen, M.; Kallionpää, R.A.; Pöyhönen, M.; Leppävirta, J.; Ylä-Outinen, H.; Riccardi, V.M.; Pukkala, E.; Pitkäniemi, J.; Peltonen, S.; et al. Distinctive cancer associations in patients with neurofibromatosis type 1. J. Clin. Oncol. 2016, 34, 1978–1986. [Google Scholar] [CrossRef] [PubMed]
- Walker, L.; Thompson, D.; Easton, D.; Ponder, B.; Ponder, M.; Frayling, I.; Baralle, D. A prospective study of neurofibromatosis type 1 cancer incidence in the UK. Br. J. Cancer 2006, 95, 233–238. [Google Scholar] [CrossRef]
- Sharif, S.; Moran, A.; Huson, S.M.; Iddenden, R.; Shenton, A.; Howard, E.; Evans, D.G.R. Women with neurofibromatosis 1 are at a moderately increased risk of developing breast cancer and should be considered for early screening. J. Med. Genet. 2007, 44, 481–484. [Google Scholar] [CrossRef] [Green Version]
- Madanikia, S.A.; Bergner, A.; Ye, X.; Blakeley, J.O. Increased risk of breast cancer in women with NF1. Am. J. Med. Genet. A 2012, 158, 3056–3060. [Google Scholar] [CrossRef]
- Wang, X.; Levin, A.M.; Smolinski, S.E.; Vigneau, F.D.; Levin, N.K.; Tainsky, M.A. Breast cancer and other neoplasms in women with neurofibromatosis type 1: A retrospective review of cases in the Detroit metropolitan area. Am. J. Med. Genet. A 2012, 158, 3061–3064. [Google Scholar] [CrossRef] [PubMed]
- Seminog, O.O.; Goldacre, M.J. Age-specific risk of breast cancer in women with neurofibromatosis type 1. Br. J. Cancer 2015, 112, 1546–1548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howell, S.J.; Hockenhull, K.; Salih, Z.; Evans, D.G. Increased risk of breast cancer in neurofibromatosis type 1: Current insights. Breast Cancer (Dove Med. Press) 2017, 9, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Suarez-Kelly, L.P.; Yu, L.; Kline, D.; Schneider, E.B.; Agnese, D.M.; Carson, W.E. Increased breast cancer risk in women with neurofibromatosis type 1: A meta-analysis and systematic review of the literature. Hered. Cancer Clin. Pract. 2019, 17, 12. [Google Scholar] [CrossRef]
- Evans, D.G. Are we ready for targeted early breast cancer detection strategies in women with NF1 aged 30–49 years? Am. J. Med. Genet. A 2012, 158, 3054–3055. [Google Scholar] [CrossRef]
- Recently Updated NCCN Clinical Practice Guidelines in OncologyTM. Available online: https://www.nccn.org/professionals/physician_gls/recently_updated.aspx (accessed on 1 February 2019).
- Daly, M.B.; Klein, C.; Reiser, G. NCCN guidelines index table of contents discussion. Risk Assess. 2017, 110. [Google Scholar]
- Hasson, D.M.; Khera, S.Y.; Meade, T.L.; Dupont, E.L.; Greenberg, H.M.; Diaz, N.M.; Romilly, A.P.; Cox, C.E. Problems with the use of breast conservation therapy for breast cancer in a patient with neurofibromatosis type 1: A case report. Breast J. 2008, 14, 188–192. [Google Scholar] [CrossRef]
- Da Silva, A.V.; Rodrigues, F.R.; Pureza, M.; Lopes, V.G.S.; Cunha, K.S. Breast cancer and neurofibromatosis type 1: A diagnostic challenge in patients with a high number of neurofibromas. BMC Cancer 2015, 15, 183. [Google Scholar] [CrossRef]
- Wang, D.L.; Smith, K.B.; Esparza, S.; Leigh, F.A.; Muzikansky, A.; Park, E.R.; Plotkin, S.R. Emotional functioning of patients with neurofibromatosis tumor suppressor syndrome. Genet. Med. 2012, 14, 977–982. [Google Scholar] [CrossRef] [Green Version]
- Pride, N.A.; Crawford, H.; Payne, J.M.; North, K.N. Social functioning in adults with neurofibromatosis type 1. Res. Dev. Disabil. 2013, 34, 3393–3399. [Google Scholar] [CrossRef]
- Cohen, J.S.; Levy, H.P.; Sloan, J.; Dariotis, J.; Biesecker, B.B. Depression among adults with neurofibromatosis type 1: Prevalence and impact on quality of life. Clin. Genet. 2015, 88, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Frayling, I.M.; Mautner, V.-F.; van Minkelen, R.; Kallionpaa, R.A.; Aktaş, S.; Baralle, D.; Ben-Shachar, S.; Callaway, A.; Cox, H.; Eccles, D.M.; et al. Breast cancer risk in neurofibromatosis type 1 is a function of the type of NF1 gene mutation: A new genotype-phenotype correlation. J. Med. Genet. 2018, 209–219. [Google Scholar] [CrossRef]
- Stewart, D.R.; Korf, B.R.; Nathanson, K.L.; Stevenson, D.A.; Yohay, K. Care of adults with neurofibromatosis type 1: A clinical practice resource of the American College of Medical Genetics and Genomics (ACMG). Genet. Med. 2018, 20, 671–682. [Google Scholar] [CrossRef] [PubMed]
- Cancer Care Ontario (CCO). Information for Healthcare Providers on the Ontario Breast Screening Program (OBSP). Available online: https://archive.cancercare.on.ca/pcs/screening/breastscreening/OBSP/ (accessed on 15 January 2019).
- Lo, G.; Scaranelo, A.M.; Aboras, H.; Ghai, S.; Kulkarni, S.; Fleming, R.; Bukhanov, K.; Crystal, P. Evaluation of the utility of screening mammography for high-risk women undergoing screening breast MR imaging. Radiology 2017, 285, 36–43. [Google Scholar] [CrossRef]
- Chiarelli, A.M.; Prummel, M.V.; Muradali, D.; Majpruz, V.; Horgan, M.; Carroll, J.C.; Eisen, A.; Meschino, W.S.; Shumak, R.S.; Warner, E.; et al. Effectiveness of screening with annual magnetic resonance imaging and mammography: Results of the initial screen from the ontario high risk breast screening program. J. Clin. Oncol. 2014, 32, 2224–2230. [Google Scholar] [CrossRef]
- Easton, D.F.; Ford, D.; Bishop, D.T. Breast and ovarian cancer incidence in BRCA1-mutation carriers. Breast Cancer Linkage Consortium. Am. J. Hum. Genet. 1995, 56, 265–271. [Google Scholar]
- Antoniou, A.; Pharoah, P.D.P.; Narod, S.; Risch, H.A.; Eyfjord, J.E.; Hopper, J.L.; Loman, N.; Olsson, H.; Johannsson, O.; Borg, A.; et al. Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case series unselected for family history: A combined analysis of 22 studies. Am. J. Hum. Genet. 2003, 72, 1117–1130. [Google Scholar] [CrossRef]
- Warner, E.; Plewes, D.B.; Hill, K.A.; Causer, P.A.; Zubovits, J.T.; Jong, R.A.; Cutrara, M.R.; DeBoer, G.; Yaffe, M.J.; Messner, S.J.; et al. Surveillance of BRCA1 and BRCA2 mutation carriers with magnetic resonance imaging, ultrasound, mammography, and clinical breast examination. JAMA 2004, 292, 1317–1325. [Google Scholar] [CrossRef]
- Kriege, M.; Brekelmans, C.T.M.; Boetes, C.; Besnard, P.E.; Zonderland, H.M.; Obdeijn, I.M.; Manoliu, R.A.; Kok, T.; Peterse, H.; Tilanus-Linthorst, M.M.A.; et al. Efficacy of MRI and mammography for breast-cancer screening in women with a familial or genetic predisposition. N. Engl. J. Med. 2004, 351, 427–437. [Google Scholar] [CrossRef]
- Kuhl, C.K.; Schrading, S.; Bieling, H.B.; Wardelmann, E.; Leutner, C.C.; Koenig, R.; Kuhn, W.; Schild, H.H. MRI for diagnosis of pure ductal carcinoma in situ: A prospective observational study. Lancet Lond. Engl. 2007, 370, 485–492. [Google Scholar] [CrossRef]
- Gokalp, G.; Hakyemez, B.; Kizilkaya, E.; Haholu, A. Myxoid neurofibromas of the breast: Mammographical, sonographical and MRI appearances. Br. J. Radiol. 2007, 80, e234–e237. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, D.; Kaur, N.; Gami, A.; Hura, K.S.; Garg, G.; Mohanty, S.K. Neurofibromatosis and breast cancer: Do we need to revise the mammographic screening schedule in patients of neurofibromatosis? J. Cancer Res. Ther. 2017, 13, 583–585. [Google Scholar]
- Vetter, L.; Keller, M.; Bruckner, T.; Golatta, M.; Eismann, S.; Evers, C.; Dikow, N.; Sohn, C.; Heil, J.; Schott, S. Adherence to the breast cancer surveillance program for women at risk for familial breast and ovarian cancer versus overscreening: A monocenter study in Germany. Breast Cancer Res. Treat. 2016, 156, 289–299. [Google Scholar] [CrossRef]
- Lerman, C.; Daly, M.; Sands, C.; Balshem, A.; Lustbader, E.; Heggan, T.; Goldstein, L.; James, J.; Engstrom, P. Mammography adherence and psychological distress among women at risk for breast cancer. JNCI J. Natl. Cancer Inst. 1993, 85, 1074–1080. [Google Scholar] [CrossRef] [PubMed]
- Tinley, S.T.; Houfek, J.; Watson, P.; Wenzel, L.; Clark, M.B.; Coughlin, S.; Lynch, H.T. Screening adherence in BRCA1/2 families is associated with primary physicians’ behavior. Am. J. Med. Genet. A 2004, 125, 5–11. [Google Scholar] [CrossRef]
- Botkin, J.R.; Smith, K.R.; Croyle, R.T.; Baty, B.J.; Wylie, J.E.; Dutson, D.; Chan, A.; Hamann, H.A.; Lerman, C.; McDonald, J.; et al. Genetic testing for a BRCA1 mutation: Prophylactic surgery and screening behavior in women 2 years post testing. Am. J. Med. Genet. A 2003, 118, 201–209. [Google Scholar] [CrossRef]
- ACR BI-RADS Atlas® 5th edition. Available online: https://www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/Bi-Rads (accessed on 22 February 2019).


{kind=link}
| ACR BI-RADS Descriptor | Screening Mammography (n = 112) | Screening Breast Ultrasound (n = 3) | Screening Breast MRI (n = 108) | X-ray Guided Biopsy (n = 2) | US-Guided Biopsy (n = 10) | MRI-Guided Biopsy (n = 3) |
|---|---|---|---|---|---|---|
| Mass lesion | 1 (10%) | - | 8 (30%) | - | 8 (80%) | 1 (33%) |
| Focus of enhancement | - | - | 2 (7%) | - | - | 1 (33%) |
| Non-mass enhancement | - | - | 8 (30%) | - | 1 (10%) | 1 (33%) |
| Calcification | 4 (40%) | - | - | 2 (100%) | - | - |
| Distortion | 1 (10%) | - | - | - | 1 (10%) | - |
| Asymmetry | 3 (30%) | - | - | - | - | - |
| Other | 1 (10%) | 9 (33%) | ||||
| TOTAL | 10 (100%) | - | 27 (100%) | 2 (100%) | 10 (100%) | 3 (100%) |
| Total n (%) | |
|---|---|
| NF1 OBSP Referrals seen by nurse navigator | 67 |
| Average age at referral | 40 |
| Median | 40 |
| Range | 30–67 |
| Scheduled in HR breast screening | 60 (89) |
| Primary Screen Compliant | 57 (95) |
| Secondary Screen Compliant † | 55 (97) |
| Recalls | 27 (49) |
| Recall Compliant * | 27 (100) |
| Breast Cancer Diagnoses ** | 4 (7) |
| NF1 Variant | Age at Referral | BC FamilyHx | Abnormal Diagnostic Screen | Breast Pathology | Surgery | Medical Oncology | Radiation |
|---|---|---|---|---|---|---|---|
| NF1 exon 12–13 del | 44 | ≥SDR: 1 | Baseline 1st HR MRI OBSP screen | IDC GR III, and DCIS GR II, ER+/PR+/HER2− | Left breast Mx. and right breast prophylactic Mx. | Referred | N/A |
| NF1 c.4110 + 1G>T | 61 | FDR: 1; ≥SDR: 2 | Baseline 1st HR MRI OBSP screen | Microinvasive LCIS; apocrine DCIS ER+/PR− | BilLx | Declined TAM | RT |
| NF1 c.4973_4978delTCTATA | 45 | ≥SDR: 1 | Baseline 1st HR MRI OBSP screen | IDC GR III, ER−/PR−/HER2− | Lx and SNB | Adjuvant CT | Adjuvant RT |
| NF1 c.6792insA | 45 | None | Baseline 1st HR OBSP MRI and Mammogram screens | IDC GR II, ER+/PR+/HER2− | Left breast Lx and SNB | TAM | RT |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maani, N.; Westergard, S.; Yang, J.; Scaranelo, A.M.; Telesca, S.; Thain, E.; Schachter, N.F.; McCuaig, J.M.; Kim, R.H. NF1 Patients Receiving Breast Cancer Screening: Insights from The Ontario High Risk Breast Screening Program. Cancers 2019, 11, 707. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11050707
Maani N, Westergard S, Yang J, Scaranelo AM, Telesca S, Thain E, Schachter NF, McCuaig JM, Kim RH. NF1 Patients Receiving Breast Cancer Screening: Insights from The Ontario High Risk Breast Screening Program. Cancers. 2019; 11(5):707. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11050707
Chicago/Turabian StyleMaani, Nika, Shelley Westergard, Joanna Yang, Anabel M. Scaranelo, Stephanie Telesca, Emily Thain, Nathan F. Schachter, Jeanna M. McCuaig, and Raymond H. Kim. 2019. "NF1 Patients Receiving Breast Cancer Screening: Insights from The Ontario High Risk Breast Screening Program" Cancers 11, no. 5: 707. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11050707