Potential Prognostic Role of 18F-FDG PET/CT in Invasive Epithelial Ovarian Cancer Relapse. A Preliminary Study

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
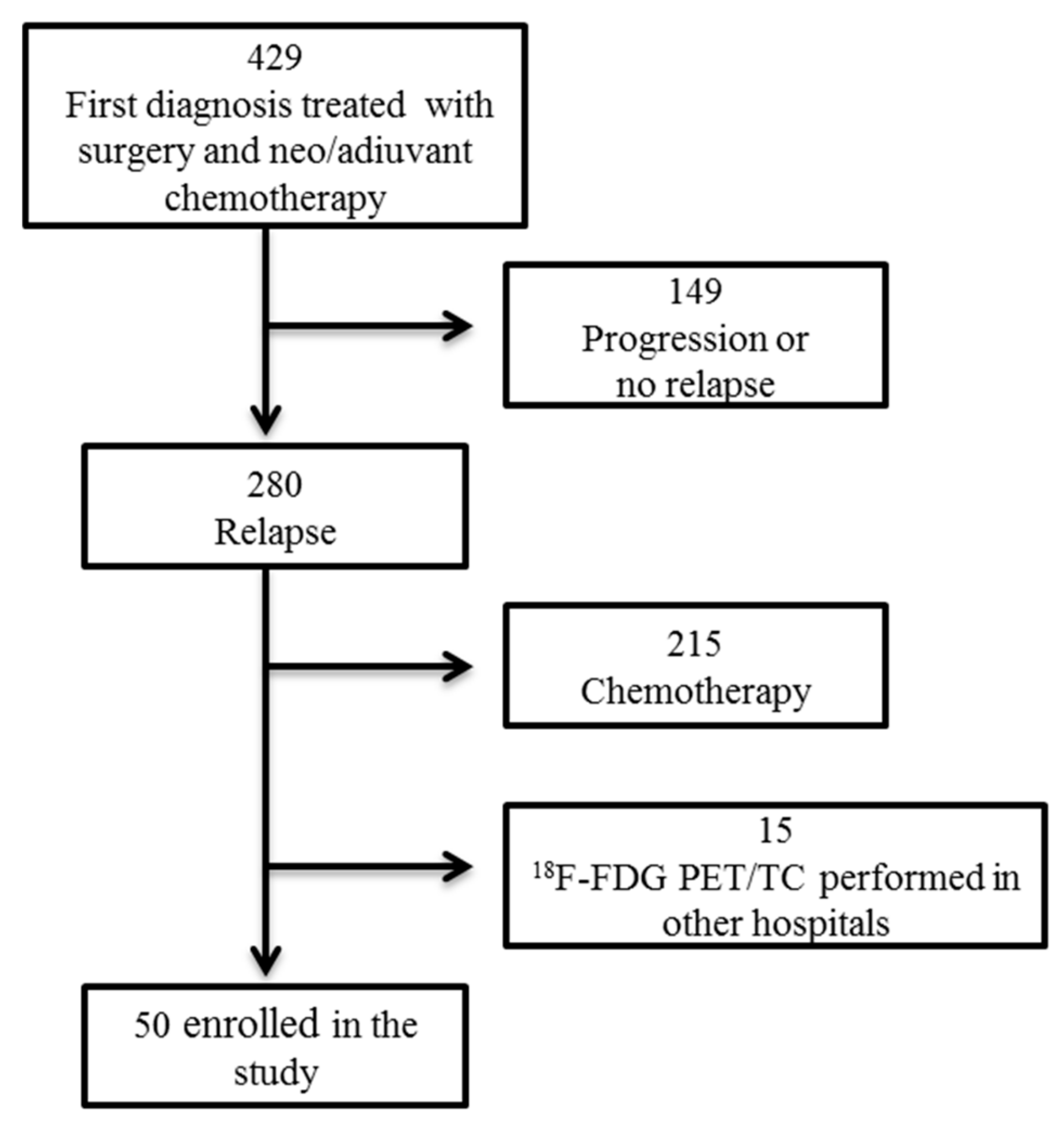
2.1. Population and Protocol
2.2. Radiopharmaceuticals, Imaging Protocol and Images Analysis
2.3. Statistical Analysis
3. Results
3.1. Population and Clinical Data
3.2. Surgical Data
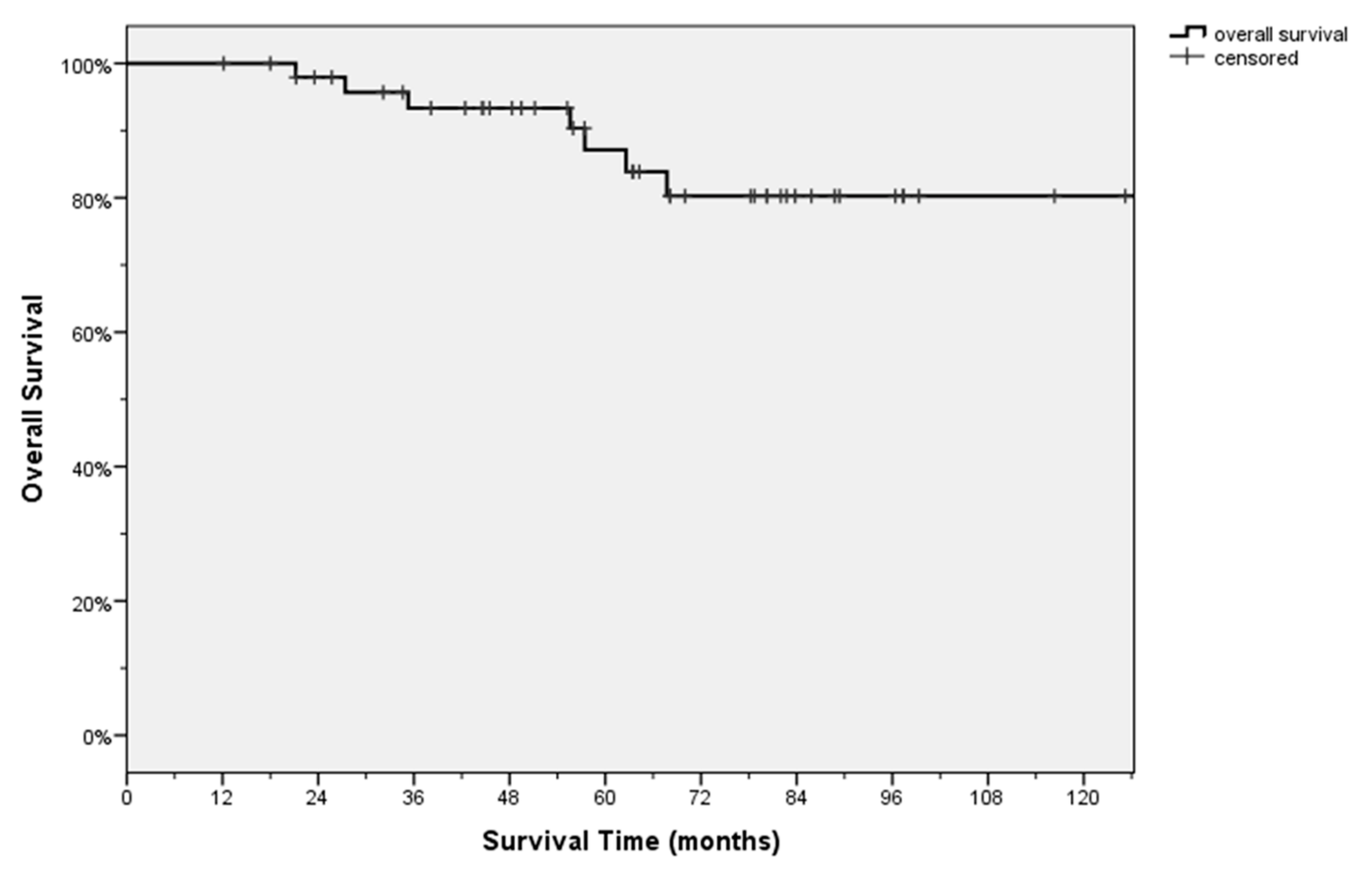
3.3. Follow Up Data
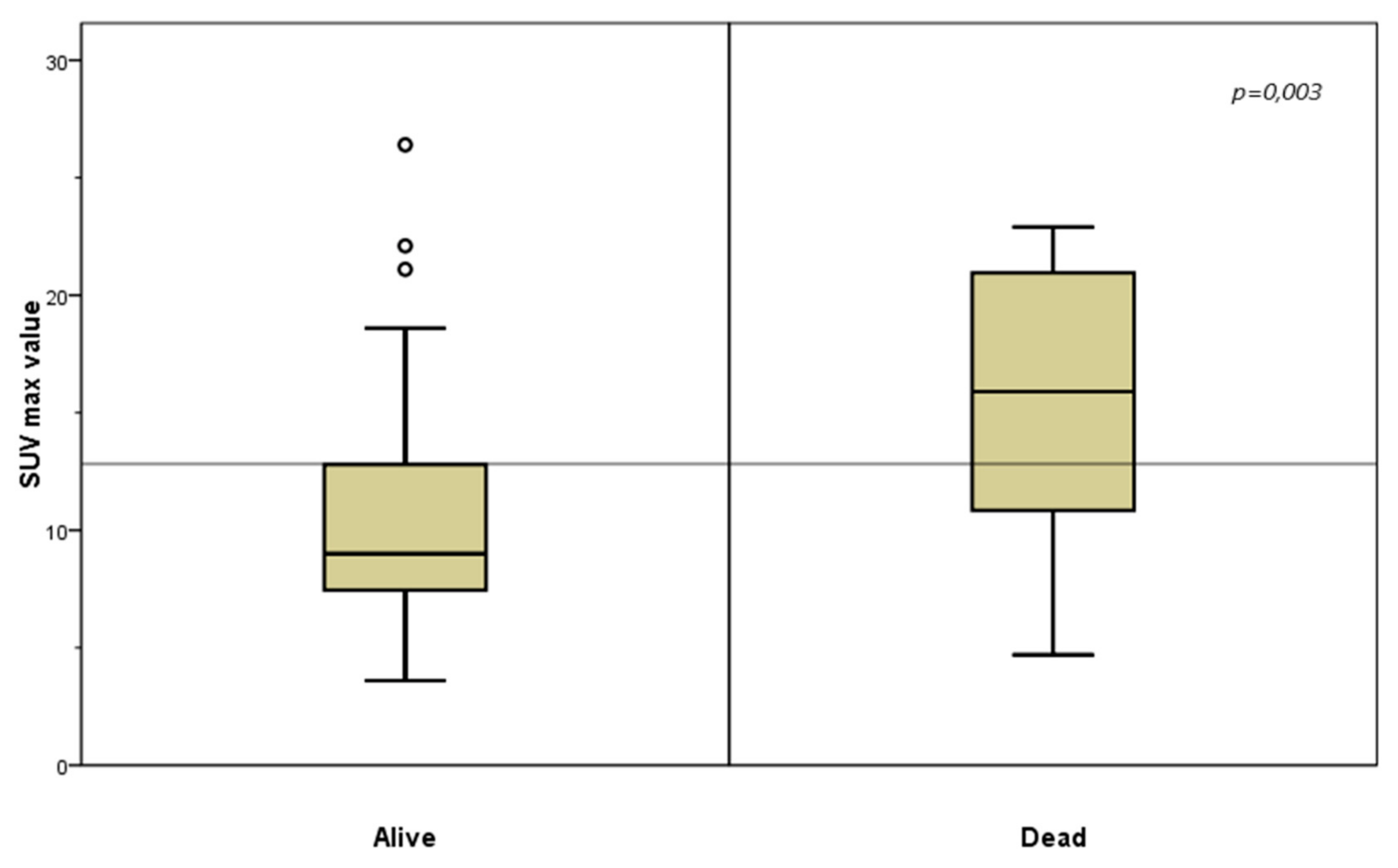
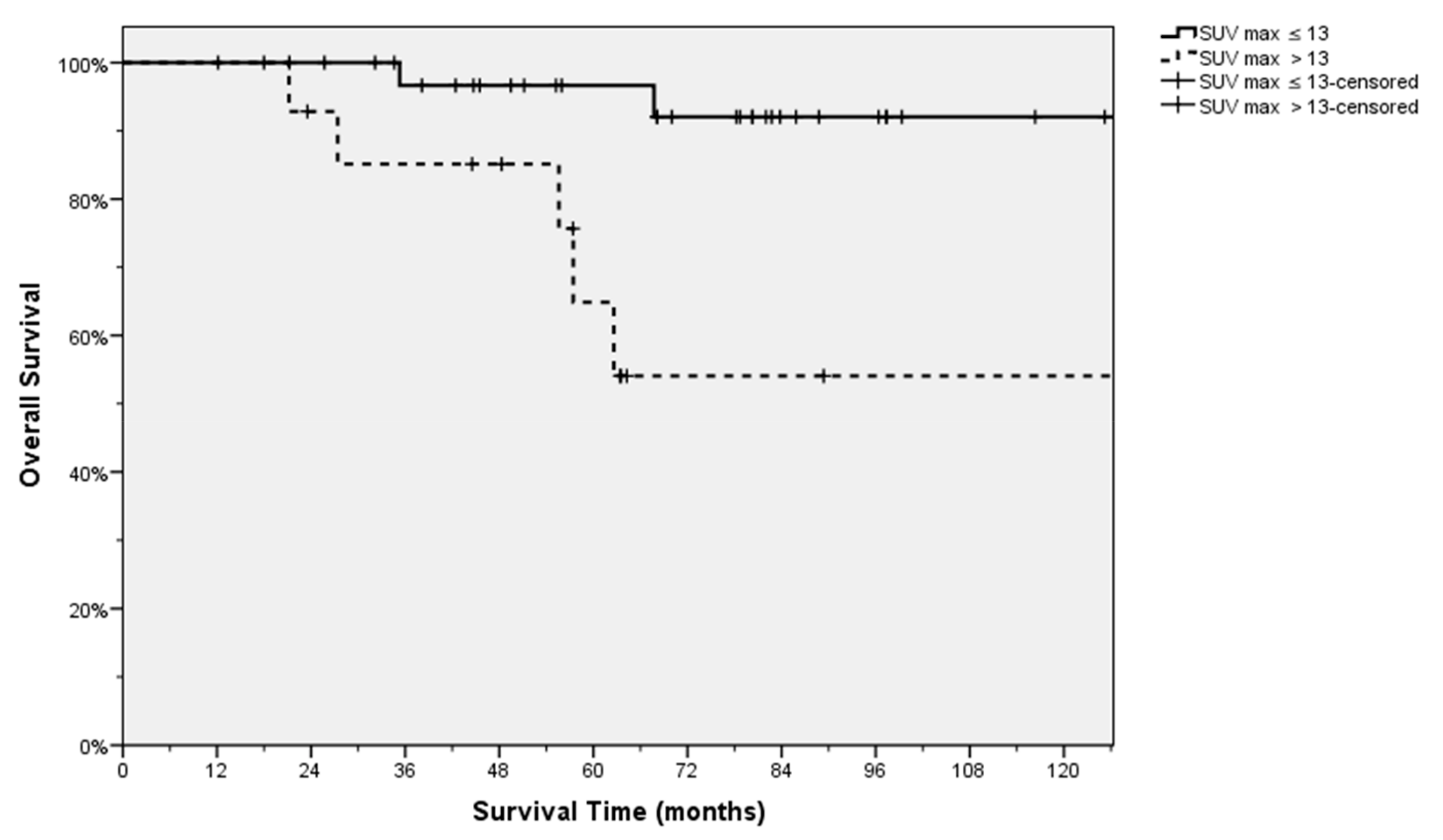
3.4. PET’s Data Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Howlader, N.; Noone, A.M.; Krapcho, M.; Neyman, N.; Aminou, R.; Waldron, W. SEER Cancer Statistics Review, 1975–2008, National Cancer Institute. Available online: http://seer.cancer.gov/csr/1975_2008 (accessed on 20 October 2011).
- Perrone, A.M.; Girolimetti, G.; Procaccini, M.; Marchio, L.; Livi, A.; Borghese, G.; Porcelli, A.M.; De Iaco, P.; Gasparre, G. Potential for mitochondrial DNA sequencing in the differential diagnosis of gynaecological malignancies. Int. J. Mol. Sci. 2018, 19, 48. [Google Scholar] [CrossRef]
- Girolimetti, G.; Perrone, A.M.; Santini, D.; Barbieri, E.; Guerra, F.; Ferrari, S.; Zamagni, C.; De Iaco, P.; Gasparre, G.; Turchetti, D. BRCA-Associated ovarian cancer: From molecular genetics to risk management. Biomed. Res. Int. 2014. [CrossRef] [PubMed]
- Bristow, R.E.; Tomacruz, R.S.; Armstrong, D.K.; Trimble, E.L.; Montz, F.J. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era: A meta-analysis. J. Clin. Oncol. 2002, 20, 1248–1259. [Google Scholar] [CrossRef]
- Ozols, R.F.; Bundy, B.N.; Greer, B.E.; Fowler, J.M.; Clarke-Pearson, D.; Burger, R.A.; Mannel, R.S.; DeGeest, K.; Hartenbach, E.M.; Baergen, R. Phase III trial of carboplatin and paclitaxel compared with cisplatin and paclitaxel in patients with optimally resected stage III ovarian cancer: A Gynecologic Oncology Group study. J. Clin. Oncol. 2003, 21, 3194–3200. [Google Scholar] [CrossRef] [PubMed]
- Girolimetti, G.; Guerra, F.; Iommarini, L.; Kurelac, I.; Vergara, D.; Maffia, M.; Vidone, M.; Amato, L.B.; Leone, G.; Dusi, S.; et al. Platinum-induced mitochondrial DNA mutations confer lower sensitivity to paclitaxel by impairing tubulin cytoskeletal organization. Hum. Mol. Genet. 2017, 26, 2961–2974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du Bois, A.; Luck, H.J.; Meier, W.; Adams, H.P.; Mobus, V.; Costa, S.; Bauknecth, T.; Richter, B.; Warm, M.; Schroder, W.; et al. A randomized clinical trial of cisplatin/paclitaxel versus carboplatin/paclitaxel as first-line treatment of ovarian cancer. J. Natl. Cancer Inst. 2003, 95, 1320–1329. [Google Scholar] [CrossRef]
- Du Bois, A.; Reuss, A.; Pujade-Lauraine, E.; Harter, P.; Ray-Coquard, I.; Pfisterer, J. Role of surgical outcome as prognostic factor in advanced epithelial ovarian cancer: A combined exploratory analysis of 3 prospectively randomized phase 3 multicenter trials: By the Arbeitsgemeinschaft Gynaekologische Onkologie Studiengruppe Ovarialkarzinom (AGO-OVAR) and the Groupe. Cancer 2009, 115, 1234–1244. [Google Scholar] [CrossRef] [PubMed]
- Krell, D.; Said Battistino, F.; Benafif, S.; Ganegoda, L.; Hall, M.; Rustin, G.J.S. Audit of CA125 follow-up after first-line therapy for ovarian cancer. Int. J. Gynecol. Cancer 2017, 27, 1118–1122. [Google Scholar] [CrossRef] [PubMed]
- Harter, P.; Sehouli, J.; Reuss, A.; Hasenburg, A.; Scambia, G.; Cibula, D.; Mahner, S.; Vergote, I.; Reinthaller, A.; Burges, A.; et al. Prospective validation study of a predictive score for operability of recurrent ovarian cancer: The Multicenter Intergroup Study DESKTOP II. A project of the AGO Kommission OVAR, AGO Study Group, NOGGO, AGO-Austria, and MITO. Int. J. Gynecol. Cancer 2011, 21, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Harter, P.; Du Bois, A.; Hahmann, M.; Hasenburg, A.; Burges, A.; Loibl, S.; Gropp, M.; Huober, J.; Fink, D.; Schröder, W.; et al. Surgery in recurrent ovarian cancer: The Arbeitsgemeinschaft Gynaekologische Onkologie (AGO) DESKTOP OVAR trial. Ann. Surg. Oncol. 2006, 13, 1702–1710. [Google Scholar] [CrossRef]
- Guerra, F.; Paiano, A.; Migoni, D.; Girolimetti, G.; Perrone, A.M.; De Iaco, P.; Fanizzi, F.P.; Gasparre, G.; Bucci, C. Modulation of RAB7A Protein expression determines resistance to cisplatin through late endocytic pathway impairment and extracellular vesicular secretion. Cancers 2019, 11, 52. [Google Scholar] [CrossRef] [PubMed]
- Du Bois, A.; Vergote, I.; Ferron, G.; Reuss, A.; Meier, W.; Greggi, S.; Jensen, P.T.; Selle, F.; Guyon, F.; Pomel, C.; et al. A randomized controlled phase III study evaluating the impact of secondary cytoreductive surgery in recur- rent ovarian cancer: AGO DESKTOP III/ENGOT ov20. J. Clin. Oncol. 2017, 35, 5501. [Google Scholar] [CrossRef]
- Rubello, D.; Marzola, M.C.; Colletti, P.M. The prognostic value of 18F-FDG PET/CT in monitoring chemotherapy in ovarian cancer both at initial diagnosis and at recurrent disease. Clin. Nucl. Med. 2018, 43, 735–738. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Zhang, J.; Cheng, W.; Zhu, C.; Chen, L.; Xia, F.; Wang, M.; Yang, F.; Ma, X. Prognostic value of maximum standard uptake value, metabolic tumor volume, and total lesion glycolysis of positron emission tomography/computed tomography in patients with nasopharyngeal carcinoma: A systematic review and meta-analysis. Medicine (Baltimore) 2017, 96, 8084. [Google Scholar] [CrossRef]
- Lima, G.M.; Matti, A.; Vara, G.; Dondi, G.; Naselli, N.; De Crescenzo, E.M.; Morganti, A.G.; Perrone, A.M.; De Iaco, P.; Nanni, C.; et al. Prognostic value of posttreatment 18F-FDG PET/CT and predictors of metabolic response to therapy in patients with locally advanced cervical cancer treated with concomitant chemoradiation therapy: An analysis of intensity- and volume-based PET parameters. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 2139–2146. [Google Scholar] [CrossRef]
- Wahl, R.L.; Jacene, H.; Kasamon, Y.; Lodge, M.A. From RECIST to PERCIST: Evolving considerations for PET response criteria in solid tumors. J. Nucl. Med. 2009, 50, 122S–150S. [Google Scholar] [CrossRef]
- Vallius, T.; Hynninen, J.; Kemppainen, J.; Alves, V.; Auranen, K.; Matomäki, J.; Oksa, S.; Virtanen, J.; Grénman, S.; Auranen, A.; et al. 18F-FDG-PET/CT based total metabolic tumor volume change during neoadjuvant chemotherapy predicts outcome in advanced epithelial ovarian cancer. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 1224–1232. [Google Scholar] [CrossRef]
- Kim, C.Y.; Jeong, S.Y.; Chong, G.O.; Son, S.H.; Jung, J.H.; Kim, D.H.; Lee, S.W.; Ahn, B.C.; Lee, J. Quantitative metabolic parameters measured on F-18 FDG PET/CT predict survival after relapse in patients with relapsed epithelial ovarian cancer. Gynecol. Oncol. 2015, 136, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Kurman, R.J.; Carcangiu, M.L.; Herrington, C.S.; Young, R.H. WHO Classification of Tumours of Female Reproductive Organs, 4th ed.; IARC: Lyon, France, 2014. [Google Scholar]
- Shih, I.M.; Kurman, R.J. Ovarian tumorigenesis: A proposed model based on morphological and molecular genetic analysis. Am. J. Pathol. 2004, 164, 1511–1518. [Google Scholar] [CrossRef]
- Zeppernick, F.; Meinhold-Heerlein, I. The new FIGO staging system for ovarian, fallopian tube, and primary peritoneal cancer. Arch. Gynecol. Obstet. 2014, 290, 839–842. [Google Scholar] [CrossRef] [PubMed]
- Aletti, G.D.; Santillan, A.; Eisenhauer, E.L.; Hu, J.; Aletti, G.; Podratz, K.C.; Bristow, R.E.; Chi, D.S.; Cliby, W.A. A new frontier for quality of care in gynecologic oncology surgery: Multi-institutional assessment of short-term outcomes for ovarian cancer using a risk-adjusted model. Gynecol. Oncol. 2007, 107, 99–106. [Google Scholar] [CrossRef]
- Jacquet, P.; Sugarbaker, P.H. Clinical research methodologies in diagnosis and staging of patients with peritoneal carcinomatosis. Cancer. Treat. Res. 1996, 82, 359–374. [Google Scholar]
- Petrillo, M.; De Iaco, P.; Cianci, S.; Perrone, M.; Costantini, B.; Ronsini, C.; Scambia, G.; Fagotti, A. Long-term survival for platinum-sensitive recurrent ovarian cancer patients treated with secondary cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy (HIPEC). Ann. Surg. Oncol. 2016, 23, 1660–1665. [Google Scholar] [CrossRef]
- Friedlander, M.; Trimble, E.; Tinker, A.; Alberts, D.; Avall-Lundqvist, E.; Brady, M.; Harter, P.; Pignata, S.; Pujade-Lauraine, E.; Sehouli, J.; et al. Clinical trials in recurrent ovarian cancer. Int. J. Gynecol. Cancer 2011, 21, 771–775. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.A. Segmentation of positron emission tomography images: Some recommendations for target delineation in radiation oncology. Radiother. Oncol. 2010, 96, 302–307. [Google Scholar] [CrossRef]
- Heitz, F.; Du Bois, A.; Kurzeder, C.; Pfisterer, J.; Barinoff, J.; Grabowski, J.; Hilpert, F.; Mahner, S.; Harter, P. Surgery for recurrent ovarian cancer. Womens Health (Lond.) 2011, 7, 529–535. [Google Scholar] [CrossRef]
- De Gaetano, A.M.; Calcagni, M.L.; Rufini, V.; Valenza, V.; Giordano, A.; Bonomo, L. Imaging of peritoneal carcinomatosis with FDG PET-CT: Diagnostic patterns, case examples and pitfalls. Abdom. Imaging 2009, 34, 391–402. [Google Scholar] [CrossRef] [PubMed]
- Kroeger, P.T., Jr.; Drapkin, R. Pathogenesis and heterogeneity of ovarian cancer. Curr. Opin. Obstet. Gynecol. 2017, 29, 26–34. [Google Scholar] [CrossRef]
- Giudice, M.T.; D’Indinosante, M.; Cappuccio, S.; Gallotta, V.; Fagotti, A.; Scambia, G.; Petrillo, M. Secondary cytoreduction in ovarian cancer: Who really benefits? Arch. Gynecol. Obstet. 2018, 298, 873–879. [Google Scholar] [CrossRef]
- Chong, G.O.; Jeong, S.Y.; Lee, Y.H.; Lee, H.J.; Lee, S.W.; Han, H.S.; Hong, D.G.; Lee, Y.S. The ability of whole-body SUVmax in F-18 FDG PET/CT to predict suboptimal cytoreduction during primary debulking surgery for advanced ovarian cancer. J. Ovarian Res. 2019, 12, 12. [Google Scholar] [CrossRef]
- Griffin, L.R.; Thamm, D.H.; Selmic, L.E.; Ehrhart, E.J.; Randall, E. Pilot study utilizing Fluorine-18 fluorodeoxyglucose-positron emission tomography/computed tomography for glycolytic phenotyping of canine mast cell tumors. Vet. Radiol. Ultrasound 2018, 59, 461–468. [Google Scholar] [CrossRef]
- Paesmans, M.; Berghmans, T.; Dusart, M.; Garcia, C.; Hossein-Foucher, C.; Lafitte, J.J.; Mascaux, C.; Meert, A.P.; Roelandts, M.; Scherpereel, A.; et al. Primary tumor standardized uptake value measured on fluorodeoxyglucose positron emission tomography is of prognostic value for survival in non-small cell lung cancer: Update of a systematic review and meta-analysis by the European Lung Cancer Working Party for the International Association for the Study of Lung Cancer Staging Project. J. Thorac. Oncol. 2010, 5, 612. [Google Scholar] [CrossRef] [PubMed]
- Paesmans, M.; Garcia, C.; Wong, C.Y.O.; Patz, E.F., Jr.; Komaki, R.; Eschmann, S.; Govindan, R.; Vansteenkiste, J.; Meert, A.P.; De Jong, W.K.; et al. Primary tumour standardised uptake value is prognostic in nonsmall cell lung cancer: A multivariate pooled analysis of individual data. Eur. Respir. J. 2015, 46, 1751–1761. [Google Scholar] [CrossRef]
- Nair, V.S.; Krupitskaya, Y.; Gould, M.K. Positron emission tomography 18F-fluorodeoxyglucose uptake and prognosis in patients with surgically treated, stage I non-small cell lung cancer: A systematic review. J. Thorac. Oncol. 2009, 4, 1473. [Google Scholar] [CrossRef]
- Pan, L.; Gu, P.; Huang, G. Prognostic significance of SUV on PET/CT in patients with esophageal cancer: A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2009, 21, 1008. [Google Scholar] [CrossRef]
- Rizk, N.P.; Tang, L.; Adusumilli, P.S.; Bains, M.S.; Akhurst, T.J.; Ilson, D.; Goodman, K.; Rusch, V.W. Predictive value of initial PET-SUVmax in patients with locally advanced esophageal and gastroesophageal junction adenocarcinoma. J. Thorac. Oncol. 2009, 4, 875. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Diagnosis | Relapse | p | |
|---|---|---|---|
| Age | |||
| (Mean ± SD) | 53.0 ± 9.2 | 55.7 ± 9.5 | ns |
| Body mass Index (BMI) | |||
| (Mean ± SD) | 24.2 ± 6.7 | 25 ± 5.6 | ns |
| Histological parameters | |||
| Type 1 | 9 (18%) | ||
| Type 2 | 41 (82%) | ||
| Serous | 35 (70%) | ||
| Mucinous | 1 (2%) | ||
| Endometrioid | 11 (22%) | ||
| Clear cell | 3 (6%) | ||
| Tumor Grading | |||
| G1 | 2 (4%) | ||
| G2 | 6 (12%) | ||
| G3 | 42 (84%) | ||
| FIGO stage | |||
| I | 5 (10%) | ||
| II | 5 (10%) | ||
| III | 37 (74%) | ||
| IV | 3 (6%) | ||
| Genetic mutations | |||
| BRCA 1 | 4 (8%) | ||
| BRCA 2 | 2 (4%) | ||
| Missmatch repair (MMR) | 1 (2%) | ||
| No mutations | 43 (86%) | ||
| Bevacizumab | |||
| Yes | 6 (12%) | ||
| No | 44 (88%) | ||
| SUVmax | |||
| (Mean ± SD) | 11 ± 5.6 | ||
| TLG | |||
| (Mean ± SD) | 250.9 ± 946 | ||
| MTV | |||
| (Mean ± SD) | 34 ± 105.63 | ||
| CA 125 (U/mL) | |||
| 0–34 | 3 (6%) | 20 (40%) | |
| 35–499 | 18 (36%) | 25 (50%) | |
| 500–999 | 9 (18%) | 1 (2%) | |
| ≥1000 | 14 (28%) | 2 (4%) | |
| not available | 6 (12%) | 2 (4%) | 0.001 |
| ALETTI SCORE | |||
| Low complexity | 13 (26%) | 27 (54%) | |
| Mediun complexity | 26 (52%) | 19 (38%) | |
| High complexity | 11 (22%) | 4 (8%) | 0.001 |
| RESIDUAL DISEASE | |||
| CC0 | 45 (90%) | 44 (88%) | |
| CC1 | 4 (8%) | 0 (0%) | |
| CC2 | 1 (2%) | 2 (4%) | |
| CC3 | 0 (0%) | 4 (8%) | ns |
| Time between first relapse and death | |||
| (Mean ± SD) | 27.8 ±14.3 |
| PET Parameters | p-value | Odds Ratio | 95% CI | |
|---|---|---|---|---|
| Step 1 | Standardized Uptake Values (SUVmax) | 0.257 | 1.103 | 0.931–1.306 |
| Metabolic Tumor Volume MTV | 0.273 | 0.928 | 0.812–1.060 | |
| Total Lesion Glycolysis (TLG) | 0.180 | 1.010 | 0.996–1.024 | |
| Step 2 | Standardized Uptake Values (SUVmax) | 0.201 | 1.125 | 0.939–1.347 |
| Total Lesion Glycolysis (TLG) | 0.446 | 1.002 | 0.997–1.006 | |
| Step 3 | Standardized Uptake Values (SUVmax) | 0.024 | 1.177 | 1.021–1.356 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perrone, A.M.; Dondi, G.; Lima, G.M.; Castellucci, P.; Tesei, M.; Coluccelli, S.; Gasparre, G.; Porcelli, A.M.; Nanni, C.; Fanti, S.; et al. Potential Prognostic Role of 18F-FDG PET/CT in Invasive Epithelial Ovarian Cancer Relapse. A Preliminary Study. Cancers 2019, 11, 713. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11050713
Perrone AM, Dondi G, Lima GM, Castellucci P, Tesei M, Coluccelli S, Gasparre G, Porcelli AM, Nanni C, Fanti S, et al. Potential Prognostic Role of 18F-FDG PET/CT in Invasive Epithelial Ovarian Cancer Relapse. A Preliminary Study. Cancers. 2019; 11(5):713. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11050713
Chicago/Turabian StylePerrone, Anna Myriam, Giulia Dondi, Giacomo Maria Lima, Paolo Castellucci, Marco Tesei, Sara Coluccelli, Giuseppe Gasparre, Anna Maria Porcelli, Cristina Nanni, Stefano Fanti, and et al. 2019. "Potential Prognostic Role of 18F-FDG PET/CT in Invasive Epithelial Ovarian Cancer Relapse. A Preliminary Study" Cancers 11, no. 5: 713. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11050713