A Multidisciplinary Team Guided Approach to the Management of cT3 Laryngeal Cancer: A Retrospective Analysis of 104 Cases

 , , ,
, , ,
Abstract
:1. Introduction
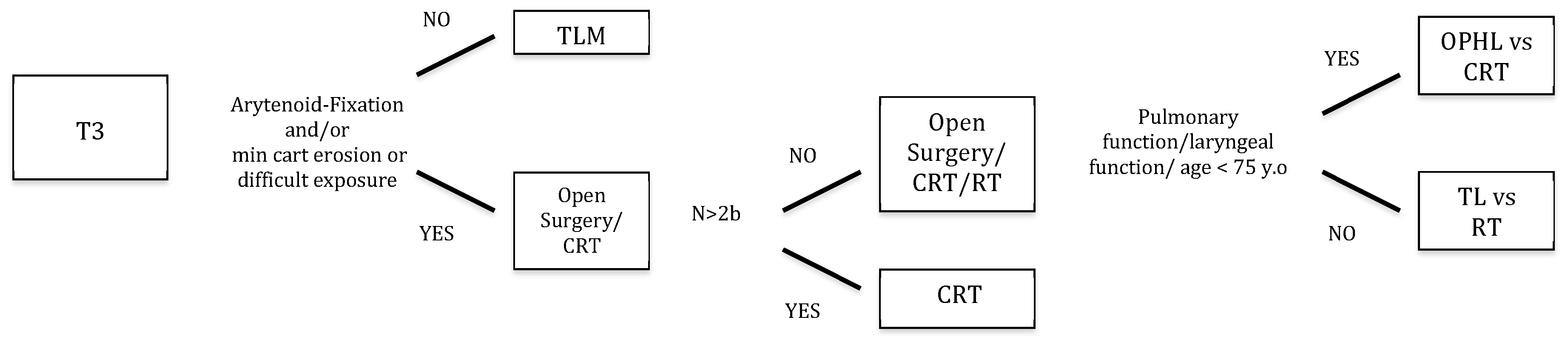
2. Materials and Methods
3. Statistical Analysis
4. Results
4.1. Treatment Characteristics
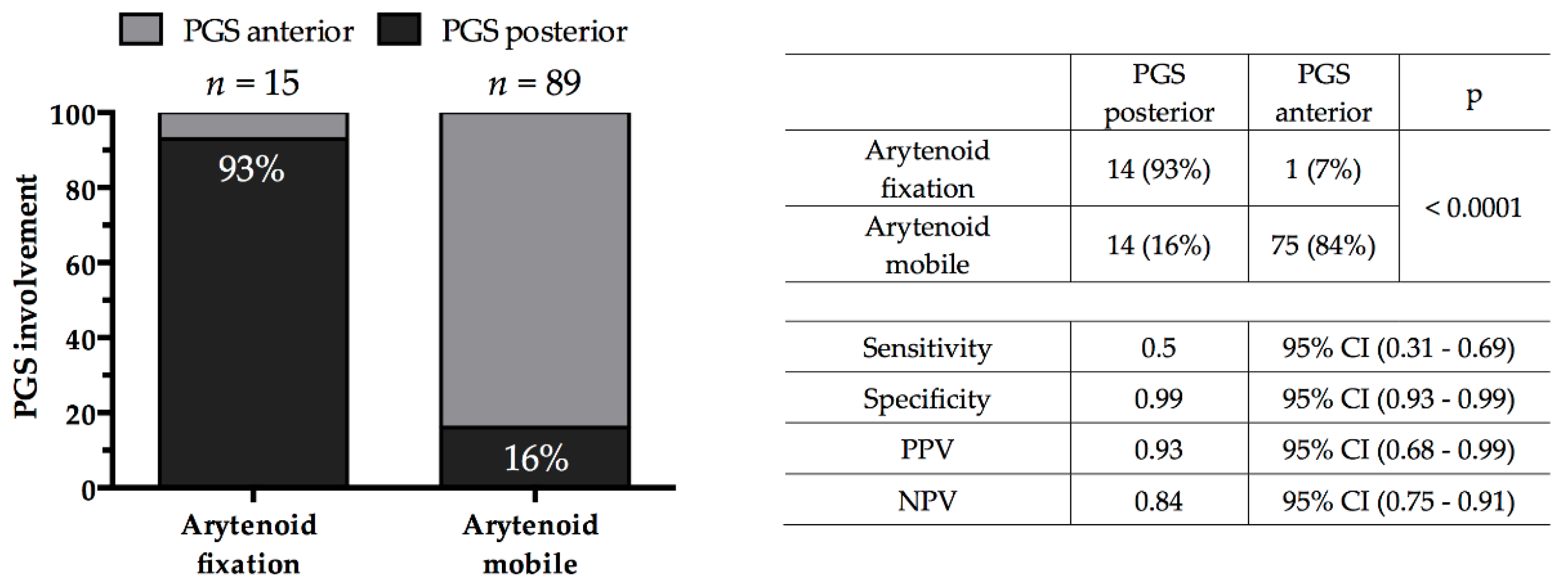
4.2. Association of Clinical and Radiological Findings
4.3. Groups Comparison Analysis
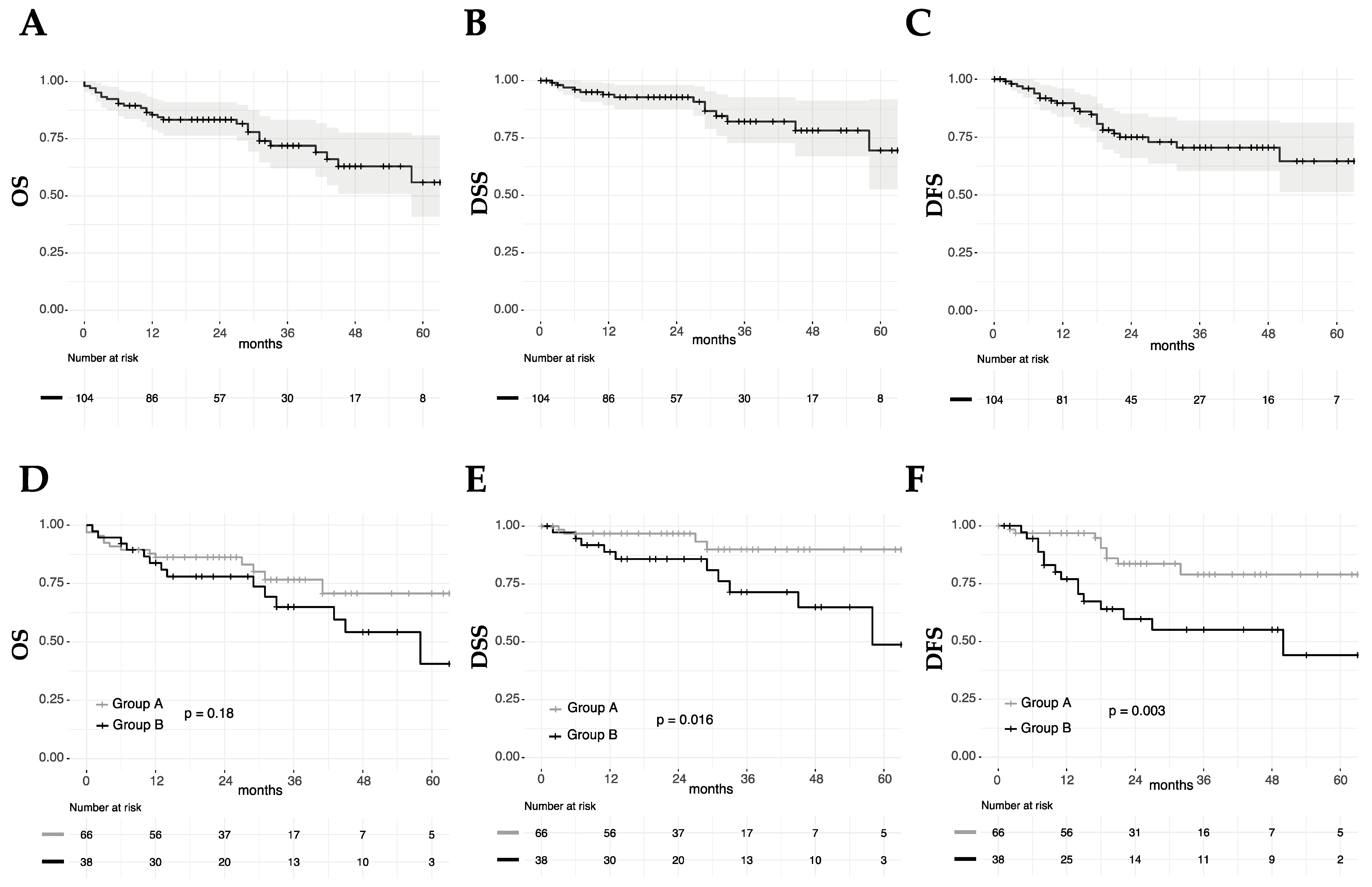
4.4. Survival Analysis
4.5. Univariate Survival Analysis
4.6. Multivariate Survival Analysis
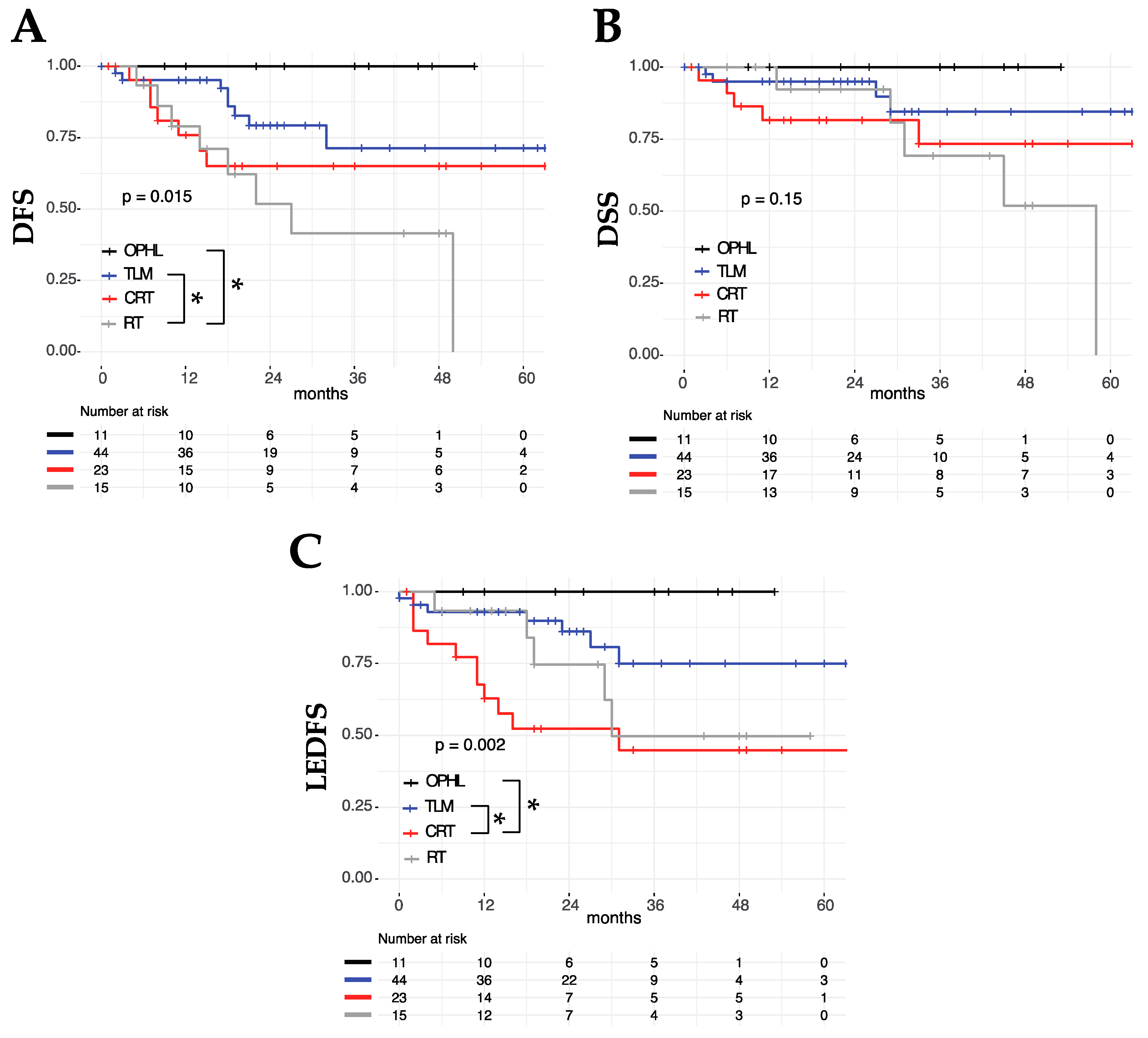
4.7. OP Approaches and LEDFS
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hoffman, H.T.; Porter, K.; Karnell, L.H.; Cooper, J.S.; Weber, R.S.; Langer, C.J.; Ang, K.; Gay, G.; Stewart, A.; Robinson, R.A. Laryngeal Cancer in the United States: Changes in Demographics, Patterns of Care, and Survival. Laryngoscope 2006, 116, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, A.Y.; Halpern, M. Factors Predictive of Survival in Advanced Laryngeal Cancer. Arch. Otolaryngol. Head Neck Surg. 2007, 133, 1270–1276. [Google Scholar] [CrossRef] [Green Version]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours, 8th ed.; John Wiley and Sons: Chichester, UK, 2017; p. 272. ISBN 9781119263579. [Google Scholar]
- Vilaseca, I.; Bernal-sprekelsen, M. Transoral Laser Microsurgery for Locally Advanced Laryngeal Cancer. Acta. Otorrinolaringol. 2012, 64, 140–149. [Google Scholar] [CrossRef]
- Succo, G.; Crosetti, E.; Bertolin, A.; Piazza, C.; Molteni, G.; Cirillo, S.; Petracchini, M.; Tascone, M.; Sprio, A.E.; Berta, G.N.; et al. Treatment for T3 to T4a laryngeal cancer by open partial horizontal laryngectomies: Prognostic impact of different pathologic tumor subcategories. Head Neck 2018, 40, 1897–1908. [Google Scholar] [CrossRef] [PubMed]
- Ravanelli, M.; Paderno, A.; Del Bon, F.; Montalto, N.; Pessina, C.; Battocchio, S.; Farina, D.; Nicolai, P.; Maroldi, R.; Piazza, C. Prediction of Posterior Paraglottic Space and Cricoarytenoid Unit Involvement in Endoscopically T3 Glottic Cancer with Arytenoid Fixation by Magnetic Resonance with Surface Coils. Cancers (Basel). 2019, 11, 67. [Google Scholar] [CrossRef]
- Del Bon, F.; Piazza, C.; Lancini, D.; Paderno, A.; Bosio, P.; Taboni, S.; Morello, R.; Montalto, N.; Missale, F.; Incandela, F.; et al. Open Partial Horizontal Laryngectomies for T3–T4 Laryngeal Cancer: Prognostic Impact of Anterior vs Posterior Laryngeal Compartmentalization. Cancers (Basel). 2019, 11, 289. [Google Scholar] [CrossRef] [PubMed]
- Forastiere, A.A.; Goepfert, H.; Maor, M.; Pajak, T.F.; Weber, R.; Morrison, W.H.; Glisson, B.; Trotti, A.; Ridge, J.A.; Chao, C.; et al. Concurrent Chemotherapy and Radiotherapy for Organ Preservation in Advanced Laryngeal Cancer. N. Engl. J. Med. 2003, 349, 2091–2098. [Google Scholar] [CrossRef]
- Weinstein, G.; Myers, E.; Shapshay, S.; Weber, R. Nonsurgical Treatment of Laryngeal Cancer. N. Engl. J. Med. 2004, 350, 1049–1053. [Google Scholar]
- Timme, D.W.; Jonnalagadda, S.; Patel, R.; Rao, K.; Robbins, K.T. Treatment Selection for T3 / T4a Laryngeal Cancer: Chemoradiation Versus Primary Surgery. Ann. Otol. Rhinol. Laryngol. 2015, 124, 845–851. [Google Scholar] [CrossRef]
- Lefebvre, J.; Ang, K.K. Larynx preservation clinical trial design: Key issues and recommendations-a consensus panel summary. Int. J. Radiat. Oncol. Biol. Phys. 2009, 73, 1293–1303. [Google Scholar] [CrossRef] [PubMed]
- Pfister, D.G.; Laurie, S.A.; Weinstein, G.S.; Mendenhall, W.M.; Adelstein, D.J.; Ang, K.K.; Clayman, G.L.; Fisher, S.G.; Forastiere, A.A.; Harrison, L.B.; et al. American Society of Clinical Oncology Clinical Practice Guideline for the Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer. J. Clin. Oncol. 2006, 24, 3693–3704. [Google Scholar] [CrossRef]
- Piazza, C.; Cocco, D.; Del Bon, F.; Mangili, S.; Nicolai, P.; Peretti, G. Narrow band imaging and high definition television in the endoscopic evaluation of upper aero-digestive tract cancer. Acta. Otorhinolaryngol. Ital. 2011, 31, 70–75. [Google Scholar]
- Maroldi, R.; Ravanelli, M.; Farina, D. Magnetic resonance for laryngeal cancer. Curr. Opin. Otolaryngol. Head Neck Surg. 2014, 22, 131–139. [Google Scholar] [CrossRef]
- Sherman, E.J.; Fisher, S.G.; Kraus, D.H.; Zelefsky, M.J.; Seshan, V.E.; Singh, B.; Shaha, A.R.; Shah, J.P.; Wolf, G.T.; Pfister, D.G. TALK Score: Development and Validation of a Prognostic Model for Predicting Larynx Preservation Outcome. Laryngoscope 2012, 122, 1043–1050. [Google Scholar] [CrossRef] [PubMed]
- Remacle, M.; Eckel, H.E.; Antonelli, A.; Brasnu, D.; Chevalier, D.; Friedrich, G.; Olofsson, J.; Rudert, H.H.; Thumfart, W.; De Vincentiis, M.; et al. Endoscopic cordectomy: A proposal for a classification by the Working Committee, European Laryngological Society. Eur. Arch. Otorhinolaryngol. 2000, 257, 227–231. [Google Scholar] [CrossRef]
- Remacle, M.; Van Haverbeke, C.; Eckel, H.; Bradley, P.; Chevalier, D.; Djukic, V.; De Vicentiis, M.; Friedrich, G.; Olofsson, J.; Peretti, G.; et al. Proposal for revision of the European Laryngological Society classification of endoscopic cordectomies. Eur. Arch. Otorhinolaryngol. 2007, 264, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Remacle, M.; Hantzakos, A.; Evrard, A.-S.; Eckel, H.; Bradley, P.J.; Chevalier, D.; Djukic, V.; De Vincentiis, M.; Friedrich, G.; Olofsson, J.; et al. Endoscopic supraglottic laryngectomy: A proposal for a classification by the working committee on nomenclature, European Laryngological Society. Eur. Arch. Otorhinolaryngol. 2009, 266, 993–998. [Google Scholar] [CrossRef] [PubMed]
- Succo, G.; Peretti, G.; Piazza, C.; Remacle, M.; Eckel, H.E.; Chevalier, D.; Simo, R.; Hantzakos, A.; Rizzotto, G.; Lucioni, M.; et al. Open partial horizontal laryngectomies: A proposal for classification by the working committee on nomenclature of the European Laryngological Society. Eur. Arch. Otorhinolaryngol. 2014, 271, 2489–2496. [Google Scholar] [CrossRef] [PubMed]
- Piazza, C.; Mangili, S.; Del Bon, F.; Paderno, A.; Grazioli, P.; Barbieri, D.; Perotti, P.; Garofolo, S.; Nicolai, P.; Peretti, G. Preoperative Clinical Predictors of Difficult Laryngeal Exposure for Microlaryngoscopy: The Laryngoscore. Laryngoscope 2014, 124, 2561–2567. [Google Scholar] [CrossRef]
- Garofolo, S.; Piazza, C.; Del Bon, F.; Mangili, S.; Guastini, L.; Mora, F.; Nicolai, P.; Peretti, G. Intraoperative Narrow Band Imaging Better Delineates Superficial Resection Margins During Transoral Laser Microsurgery for Early Glottic Cancer. Ann. Otol. Rhinol. Laryngol. 2015, 124, 294–298. [Google Scholar] [CrossRef]
- Fiz, I.; Mazzola, F.; Fiz, F.; Marchi, F.; Filauro, M.; Paderno, A.; Parrinello, G.; Piazza, C.; Peretti, G. Impact of close and positive margins in transoral laser microsurgery for TIS-T2 glottic cancer. Front. Oncol. 2017, 7, 245. [Google Scholar] [CrossRef] [PubMed]
- Colevas, A.D.; Yom, S.S.; Pfister, D.G.; Spencer, S.; Adelstein, D.; Adkins, D.; Brizel, D.M.; Burtness, B.; Busse, P.M.; Caudell, J.J.; et al. NCCN Guidelines ® Insights Head and Neck Cancers Featured Updates to the NCCN Guidelines. J. Natl. Compr. Canc. Netw. 2018, 16, 479–490. [Google Scholar] [CrossRef]
- Simo, R.; Bradley, P.; Chevalier, D.; Dikkers, F.; Eckel, H.; Matar, N.; Peretti, G.; Piazza, C.; Remacle, M.; Quer, M. European Laryngological Society: ELS recommendations for the follow-up of patients treated for laryngeal cancer. Eur Arch. Otorhinolaryngol. 2014, 271, 2469–2479. [Google Scholar] [CrossRef]
- Marchi, F.; Piazza, C.; Ravanelli, M.; Gaggero, G.; Parrinello, G.; Paderno, A.; Perotti, P.; Filauro, M.; Maroldi, R.; Peretti, G. Role of imaging in the follow-up of T2–T3 glottic cancer treated by transoral laser microsurgery. Eur. Arch. Otorhinolaryngol. 2017, 274, 3679–3686. [Google Scholar] [CrossRef] [PubMed]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Forastiere, A.; Lewin, J.S.; Nathan, C.A.; Adelstein, D.J.; Eisbruch, A.; Fass, G.; Fisher, S.G.; Laurie, S.A.; Le, Q.; Malley, B.O.; et al. Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer: American Society of Clinical Oncology Clinical Practice Guideline Update. J. Clin. Oncol. 2018, 36, 1143–1169. [Google Scholar] [CrossRef] [PubMed]
- Peretti, G.; Piazza, C.; Penco, S.; Santori, G.; Del Bon, F.; Garofolo, S.; Paderno, A.; Guastini, L.; Nicolai, P. Transoral laser microsurgery as primary treatment for selected T3 glottic and supraglottic cancers. Head Neck 2016, 38, 1107–1112. [Google Scholar] [CrossRef] [PubMed]
- Peretti, G.; Piazza, C.; Mora, F.; Garofolo, S.; Guastini, L. Reasonable limits for transoral laser microsurgery in laryngeal cancer. Curr. Opin. Otolaryngol. Head Neck Surg. 2016, 24, 135–139. [Google Scholar] [CrossRef] [Green Version]
- Sjögren, E. V Transoral Laser Microsurgery in Early Glottic Lesions. Curr. Otorhinolaryngol. Rep. 2017, 5, 56–68. [Google Scholar] [CrossRef]
- Blanch, J.-L.; Vilaseca, I.; Caballero, M.; Moragas, M.; Berenguer, J.; Bernal-sprekelsen, M. Outcome of transoral laser microsurgery for T2-T3 tumors growing in the laryngeal anterior commissure. Head Neck 2011, 10, 1252–1259. [Google Scholar] [CrossRef]
- Ansarin, M.; Cattaneo, A.; Santoro, L.; Massaro, M.A.; Zorzi, S.F.; Grosso, E.; Preda, L.; Alterio, D.; Surgery, N. Laser surgery of early glottic cancer in elderly Il trattamento del carcinoma glottico in stadio iniziale nel paziente anziano. Acta. Otorhinolaryngol. Ital. 2010, 135, 385–390. [Google Scholar]
- Mandelbaum, R.S.; Abemayor, E.; Mendelsohn, A.H. Laryngeal Preservation in Glottic Cancer: A Comparison of Hospital Charges and Morbidity among Treatment Options. Otolaryngol. Neck Surg. 2016, 155, 265–273. [Google Scholar] [CrossRef]
- Rodrigo, J.P.; Garcia-Velasco, F.; Ambrosch, P.; Vander Poorten, V.; Suárez, C.; Coca-pelaz, A.; Strojan, P.; Hutcheson, K.; Folz, B.J.; Bernal-sprekelsen, M.; et al. Transoral laser microsurgery for glottic cancer in the elderly: Efficacy and safety. Head Neck 2019, 1–8. [Google Scholar] [CrossRef]
- Piazza, C.; Filauro, M.; Paderno, A.; Marchi, F.; Perotti, P.; Morello, R.; Taboni, S.; Parrinello, G.; Incandela, F.; Iandelli, A.; et al. Three-dimensional map of isoprognostic zones in glottic cancer treated by transoral laser microsurgery as a unimodal treatment strategy. Front. Oncol. 2018, 8. [Google Scholar] [CrossRef] [PubMed]
- Zeitels, S.M. Infrapetiole Exploration of the Supraglottis for Exposure of the Anterior Glottal Commissure. J. Voic. 1998, 12, 117–122. [Google Scholar] [CrossRef]
- Peretti, G.; Piazza, C.; Del Bon, F. Function preservation using transoral laser surgery for T2–T3 glottic cancer: Oncologic, vocal, and swallowing outcomes. Eur. Arch. Otorhinolaryngol. 2013, 270, 2275–2281. [Google Scholar] [CrossRef]
- Succo, G.; Crosetti, E.; Bertolin, A.; Lucioni, M.; Arrigoni, G.; Panetta, V.; Sprio, A.E.; Berta, G.N.; Rizzotto, G. Benefits and drawbacks of open partial horizontal laryngectomies, part B: Intermediate and selected advanced stage laryngeal carcinoma. Head Neck 2015, 33, 649–657. [Google Scholar] [CrossRef]
- Chiesta Estomba, C.; Betances Reinoso, F.; Lorenzo, A.; Farina Conde, J. Functional outcomes of supraglottic squamous cell carcinoma treated by transoral laser microsurgery compared with horizontal supraglottic laryngectomy in patients younger and older than 65 years. Acta. Otorhinolaryngol. Ital. 2016, 36, 450–458. [Google Scholar]
- Wang, Y.; Li, X.; Pan, Z. Analyses of functional and oncologic outcomes following supracricoid partial laryngectomy. Eur. Arch. Otorhinolaryngol. 2014, 272, 3463–3468. [Google Scholar] [CrossRef]
- Fuller, C.; Mohamed, A.S.R.; Garden, A.S.G.; Gunn, B.; Mulcahy, C.F.; Zafereo, M.; Phan, J.; Lai, S.Y.; Lewin, J.S.; Hutcheson, K.A.; et al. Long-Term Outcomes Following Multi-Disciplinary Management of T3 Larynx Squamous Cell Carcinomas: Modern Therapeutic Approaches Improve Functional Outcomes and Survival. Head Neck 2016, 38, 1739–1751. [Google Scholar] [CrossRef]
- Alba, J.R.; Basterra, J.; Ferrer, J.C.; Santonja, F.; Zapater, E. Hypothyroidism in patients treated with radiotherapy for head and neck carcinoma: Standardised long-term follow-up study. J. Laryngol. Otol. 2016, 130, 478–481. [Google Scholar] [CrossRef]
- Shariat, M.; Alias, N.A.A.; Biswal, B.M. Radiation effects on the intima—media thickness of the common carotid artery in post-radiotherapy patients with head and neck malignancy. Postgr. Med. J. 2008, 84, 609–612. [Google Scholar] [CrossRef]
- Riga, M.; Chelis, L.; Danielides, V.; Vogiatzaki, T.; Pantazis, T.; Pantazis, D. Systematic review on T3 laryngeal squamous cell carcinoma; still far from a consensus on the optimal organ preserving treatment. Eur. J. Surg. Oncol. 2016, 43, 20–31. [Google Scholar] [CrossRef]
- Dziegielewski, P.T.; O’Connell, D.A.O.; Klein, M.; Fung, C.; Singh, P.; Mlynarek, A.; Fung, D.; Harris, J.R.; Seikaly, H. Primary Total Laryngectomy versus Organ Preservation for T3 / T4a Laryngeal Cancer: A Population-Based Analysis of Survival Primary. J. Otolaryngol. Neck Surg. 2012, 41, S56–S64. [Google Scholar]
- Megwalu, U.C.; Sikora, A.G. Survival Outcomes in Advanced Laryngeal Cancer. JAMA Otolaryngol. Head Neck Surg. 2014, 140, 855–860. [Google Scholar] [CrossRef] [Green Version]
- Puxeddu, R.; Piazza, C.; Mensi, M.C.; Ledda, G.P.; Argiolas, F.; Peretti, G. Carbon dioxide laser salvage surgery after radiotherapy failure in T1 and T2 glottic carcinoma. Otolaryngol. Head Neck Surg. 2004, 130, 84–88. [Google Scholar] [CrossRef]
- Piazza, C.; Peretti, G.; Cattenao, A. Salvage Surgery After Radiotherapy for Laryngeal Cancer: From Endoscopic Resections to Open-Neck Partial and Total Laryngectomies. Arch. Otolaryngol. Head Neck Surg. 2007, 133, 1037–1043. [Google Scholar] [CrossRef]
- Pellini, R.; Pichi, B.; Ruscito, P.; Ceroni, A.R.; Caliceti, U.; Rizzotto, G.; Pazzaia, A.; Laudadio, P.; Piazza, C.; Peretti, G.; et al. Supracricoid partial laryngectomies after radiation failure: A multi-institutional series. Head Neck 2008, 30, 372–379. [Google Scholar] [CrossRef]
- Del Bon, F.; Piazza, C.; Mangili, S.; Redaelli De Zinis, L.O.; Nicolai, P.; Peretti, G. Transoral laser surgery for recurrent glottic cancer after radiotherapy: Oncologic and functional outcomes. Acta. Otorhinolaryngol. Ital. 2012, 32, 229–237. [Google Scholar]
- Meulemans, J.; Bijnens, J.; Delaere, P.; Vanden Poorten, V. Up-Front and salvage Transoral laser Microsurgery for early glottic squamous cell carcinoma: A single centre retrospective case series. Front. Oncol. 2018, 8, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Emerick, K.S.; Tomycz, L.; Bradford, C.R.; Lyden, T.H.; Chepeha, D.B.; Wolf, G.T.; Teknos, T.N. Primary versus secondary tracheoesophageal puncture in salvage total laryngectomy following chemoradiation. Otolaryngol. Neck Surg. 2009, 140, 386–390. [Google Scholar] [CrossRef]
- Alvarez-morujo, R.G.; Pascual, P.M.; Tucciarone, M.; Fernandez, M.F.; Encabo, R.S.; Guirado, T.M. Salvage total laryngectomy: Is a flap necessary? Braz. J. Otorhinolaryngol. 2018, 730. [Google Scholar]
- Okamoto, I.; Tsukahara, K.; Shimizu, A.; Sato, H. Post-operative complications of salvage total laryngectomy forpost-radiotherapy recurrent laryngeal cancer using pectoralis major myocutaneous flaps. Acta. Otolaryngol. 2019, 139, 167–171. [Google Scholar] [CrossRef]
- Kapila, M.; Deore, N.; Palav, R.; Kazi, R.; Shah, R.; Jagade, M. A brief review of voice restoration following total laryngectomy. Indian J. Cancer 2011, 48, 99–104. [Google Scholar]
- Moukarbel, R.V.; Doyle, P.C.; Yoo, J.H.; Franklin, J.H.; Day, A.M.B.; Fung, K. Voice-related quality of life (V-RQOL) outcomes in laryngectomees. Head Neck 2011, 33, 31–36. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients Characteristics | All Patients | Group A (Surgical) | Group B (Non-Surgical) | p | |
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | |||
| Mean age yr (range yr) | 70 (47–96) | 69 (47–91) | 72 (53–96) | 0.08 | |
| Gender | Female | 13 (12) | 9 (14) | 4 (11) | 0.76 |
| Male | 91 (88) | 57 (86) | 34 (89) | ||
| N category | N0 | 83 (80) | 59 (89) | 24 (63) | 0.006 |
| N1-N2b | 12 (11) | 4 (6) | 8 (21) | ||
| ≥N2c | 9 (9) | 3 (5) | 6 (16) | ||
| Site | Glottic | 47 (45) | 39 (59) | 8 (21) | 0.002 |
| Supraglottic | 32 (31) | 16 (24) | 16 (42) | ||
| Subglottic | 5 (5) | 3 (5) | 2 (5) | ||
| Transglottic | 20 (19) | 8 (12) | 12 (32) | ||
| Arytenoid fixation | No | 88 (85) | 61 (92) | 27 (71) | 0.009 |
| Yes | 16 (15) | 5 (8) | 11 (29) | ||
| TALK score | 0 | 17 (16) | 13 (20) | 4 (10) | 0.003 |
| 1 | 31 (30) | 23 (35) | 8 (21) | ||
| 2 | 35 (34) | 24 (36) | 11 (29) | ||
| 3 | 21 (20) | 6 (9) | 15 (40) | ||
| Treatment | TLM | 44 (42) | 44(66) | - | - |
| OPHL | 11 (11) | 11(17) | - | ||
| TL | 11 (11) | 11 (17) | - | ||
| RT | 15 (14) | - | 15 (39) | ||
| CRT | 23 (22) | - | 23 (61) | ||
| Variables | n (%) | OS | DFS | DSS | LEDFS * | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2-y (%, 95% CI) | 5-y (%, 95% CI) | p | 2-y (%, 95% CI) | 5-y (%, 95% CI) | p | 2-y (%, 95% CI) | 5-y (%, 95% CI) | p | 2-y (%, 95% CI) | 5-y (%, 95% CI) | p | ||
| All | 104 (100) | 83 (75–89) | 56 (37–71) | - | 75 (64–83) | 65 (48–77) | - | 93 (85–96) | 70 (46–84) | - | 78 (66–85) | 66 (52–77) | - |
| Age | |||||||||||||
| ≥70 | 54 (52) | 83 (69–91) | 44 (20–66) | 0.39 | 73 (56–84) | 52 (24–74) | 0.49 | 96 (84–99) | 59 (25–82) | 0.88 | 77 (60–88) | 61 (40–76) | 0.92 |
| <70 | 50 (48) | 84 (71–92) | 75 (56–87) | 76 (60–87) | 76 (60–87) | 89 (76–95) | 85 (67–93) | 77 (60–87) | 72 (53–84) | ||||
| Gender | |||||||||||||
| F | 13 (13) | 92 (57–99) | - | 0.35 | 63 (29–85) | - | 0.71 | 92 (57–99) | - | 0.91 | 80 (39–95) | - | 0.95 |
| M | 91 (88) | 82 (72–89) | 54 (35–70) | 77 (66–85) | 65 (47–79) | 93 (84–97) | 70 (45–85) | 77 (65–86) | 66 (52–78) | ||||
| N category | |||||||||||||
| N0 | 83 (80) | 90 (81–95) | 56 (0–0) | 0.005 | 79 (67–87) | 64 (41–80) | 0.02 | 96 (88–99) | 69 (34–88) | 0.02 | 82 (70–90) | 76 (61–86) | 0.004 |
| N1-N2b | 12 (11) | 61 (25–83) | - | 36 (6–69) | - | 81 (42–95) | - | 64 (23–87) | - | ||||
| ≥N2c | 9 (9) | 56 (20–80) | 56 (20–80) | 71 (26–92) | 71 (26–92) | 75 (31–93) | 75 (31–93) | 50 (15–77) | 33 (6–66) | ||||
| Site | |||||||||||||
| Glottic | 47 (45) | 85 (71–92) | 57 (32–76) | 0.30 | 75 (58–86) | 75 (58–86) | 0.98 | 96 (83–99) | 75 (43–91) | 0.66 | 76 (58–86) | 71 (51–84) | 0.96 |
| Supraglottic | 32 (31) | 73 (53–86) | 51 (25–72) | 73 (49–87) | 66 (41–83) | 89 (68–96) | 74 (47–89) | 80 (58–91) | 56 (28–77) | ||||
| Glottic-Subglottic | 5 (5) | 100% | - | 80 (20–97) | - | 100% | - | 75 (13–96) | - | ||||
| Transglottic | 20 (19) | 90 (65–97) | 52 (9–84) | 77 (48–91) | 58 (18–84) | 90 (65–97) | 52 (9–84) | 78 (46–92) | 67 (32–87) | ||||
| Arytenoid fixation | |||||||||||||
| No | 88 (85) | 85 (76–91) | 57 (35–74) | 0.36 | 77 (65–85) | 64 (44–78) | 0.33 | 94 (86–97) | 69 (42–85) | 0.54 | 80 (67–87) | 68 (52–79) | 0.17 |
| Yes | 16 (15) | 73 (44–89) | 52 (22–76) | 65 (35–84) | 65 (35–84) | 87 (56–96) | 74 (37–92) | 61 (27–84) | - | ||||
| Group | |||||||||||||
| A | 66 (63) | 86 (75–92) | 71 (51–84) | 0.18 | 84 (70–92) | 79 (62–89) | 0.003 | 97 (88–99) | 90 (74–96) | 0.016 | 89 (75–95) | 80 (61–91) | 0.002 |
| B | 38 (37) | 78 (61–88) | 41 (15–65) | 60 (40–75) | 44 (20–66) | 86 (69–94) | 49 (17–75) | 61 (42–76) | 47 (28–64) | ||||
| Type of OP treatment * | |||||||||||||
| OPHL | 11 (11) | 90 (47–98) | - | 0.41 | 100% | 100% | 0.015 | 100% | 100% | 0.15 | 100% | - | 0.002 |
| TLM | 42 (40) | 86 (71–93) | 62 (36–80) | 79 (61–90) | 71 (47–86) | 95 (82–99) | 85 (62–94) | 88 (71–95) | 77 (53–89) | ||||
| RT-CHT | 23 (22) | 73 (50–87) | 66 (40–83) | 65 (40–82) | 65 (40–82) | 82 (58–93) | 73 (46–89) | 52 (29–71) | 45 (22–65) | ||||
| RT | 15 (14) | 86 (54–96) | 0% | 51 (22–75) | 0% | 92 (57–99) | 0% | 74 (39–91) | - | ||||
| OS | B | P | HR | 95% CI HR | |
| Inf | Sup | ||||
| Group B | 0.40 | 0.37 | 1.50 | 0.62 | 3.62 |
| N category | 0.02 | ||||
| N1-2b | 1.82 | 0.01 | 6.19 | 1.68 | 22.81 |
| ≥N2c | 0.67 | 0.32 | 1.95 | 0.53 | 7.20 |
| Presence of arytenoid fixation | −0.16 | 0.80 | 0.86 | 0.25 | 2.90 |
| Site | 0.47 | ||||
| Supraglottic | −0.46 | 0.40 | 0.63 | 0.21 | 1.86 |
| Glottic-subglottic | −13.76 | 0.98 | 0.00 | 0.00 | . |
| Transglottic | −1.05 | 0.11 | 0.35 | 0.10 | 1.29 |
| DSS | B | P | HR | 95% CI HR | |
| Inf | Sup | ||||
| Group B | 1.29 | 0.052 | 3.65 | 0.99 | 13.47 |
| N category | 0.09 | ||||
| N1-2b | 2.10 | 0.03 | 8.16 | 1.21 | 54.85 |
| ≥N2c | 0.99 | 0.33 | 2.69 | 0.36 | 19.85 |
| Presence of arytenoid fixation | −1.01 | 0.29 | 0.37 | 0.06 | 2.38 |
| Site | 0.80 | ||||
| Supraglottic | −0.88 | 0.32 | 0.41 | 0.07 | 2.36 |
| Glottic-subglottic | −13.85 | 0.98 | 0.00 | 0.00 | . |
| Transglottic | −0.32 | 0.68 | 0.73 | 0.16 | 3.30 |
| DFS | B | P | HR | 95% CIHR | |
| Inf | Sup | ||||
| Group B | 1.41 | 0.006 | 4.10 | 1.50 | 11.20 |
| N category | 0.14 | ||||
| N1-2b | 1.50 | 0.05 | 4.48 | 0.98 | 20.53 |
| ≥N2c | 0.23 | 0.78 | 1.26 | 0.24 | 6.67 |
| Presence of arytenoid fixation | −0.69 | 0.36 | 0.50 | 0.12 | 2.18 |
| Site | 0.53 | ||||
| Supraglottic | −0.77 | 0.20 | 0.47 | 0.14 | 1.51 |
| Glottic-subglottic | −0.74 | 0.42 | 0.48 | 0.08 | 2.90 |
| Transglottic | −0.79 | 0.21 | 0.45 | 0.13 | 1.57 |
| LEDFS | B | P | HR | 95% CI HR | |
| Inf | Sup | ||||
| Group B | 1.65 | 0.002 | 5.22 | 1.80 | 15.16 |
| N category | 0.04 | ||||
| N1-2b | 1.70 | 0.04 | 5.46 | 1.11 | 26.83 |
| ≥N2c | 1.80 | 0.02 | 6.02 | 1.40 | 25.90 |
| Presence of arytenoid fixation | −1.22 | 0.12 | 0.30 | 0.06 | 1.39 |
| Site | 0.30 | ||||
| Supraglottic | −1.16 | 0.09 | 0.32 | 0.08 | 1.22 |
| Glottic-subglottic | −1.05 | 0.35 | 0.35 | 0.04 | 3.19 |
| Transglottic | −0.89 | 0.18 | 0.41 | 0.11 | 1.49 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marchi, F.; Filauro, M.; Missale, F.; Parrinello, G.; Incandela, F.; Bacigalupo, A.; Vecchio, S.; Piazza, C.; Peretti, G. A Multidisciplinary Team Guided Approach to the Management of cT3 Laryngeal Cancer: A Retrospective Analysis of 104 Cases. Cancers 2019, 11, 717. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11050717
Marchi F, Filauro M, Missale F, Parrinello G, Incandela F, Bacigalupo A, Vecchio S, Piazza C, Peretti G. A Multidisciplinary Team Guided Approach to the Management of cT3 Laryngeal Cancer: A Retrospective Analysis of 104 Cases. Cancers. 2019; 11(5):717. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11050717
Chicago/Turabian StyleMarchi, Filippo, Marta Filauro, Francesco Missale, Giampiero Parrinello, Fabiola Incandela, Almalina Bacigalupo, Stefania Vecchio, Cesare Piazza, and Giorgio Peretti. 2019. "A Multidisciplinary Team Guided Approach to the Management of cT3 Laryngeal Cancer: A Retrospective Analysis of 104 Cases" Cancers 11, no. 5: 717. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11050717