Role of Bruton’s Tyrosine Kinase in Stage III Colorectal Cancer

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Results
2.1. Clinico-Pathological Characteristics
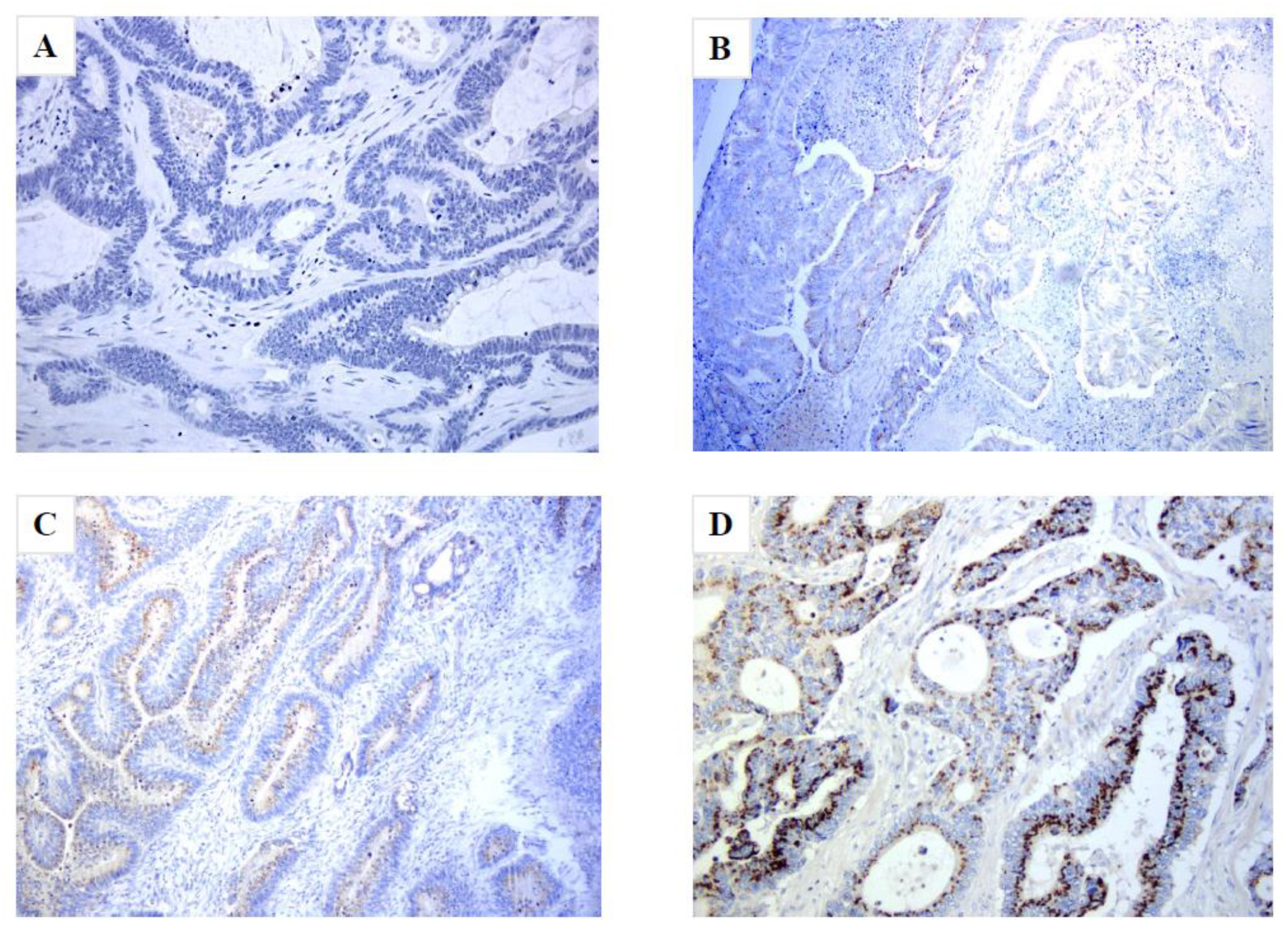
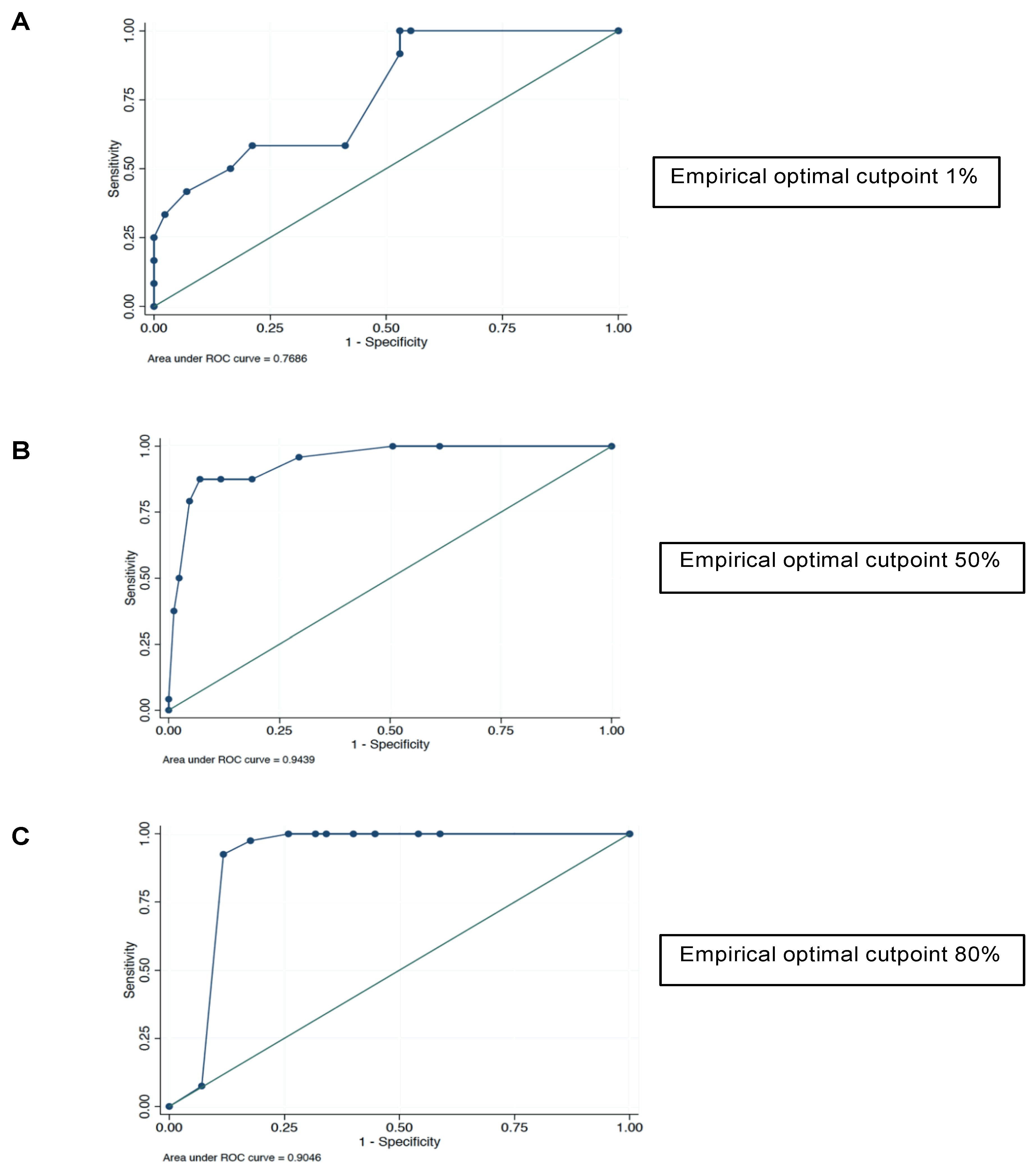
2.2. Expression Analysis
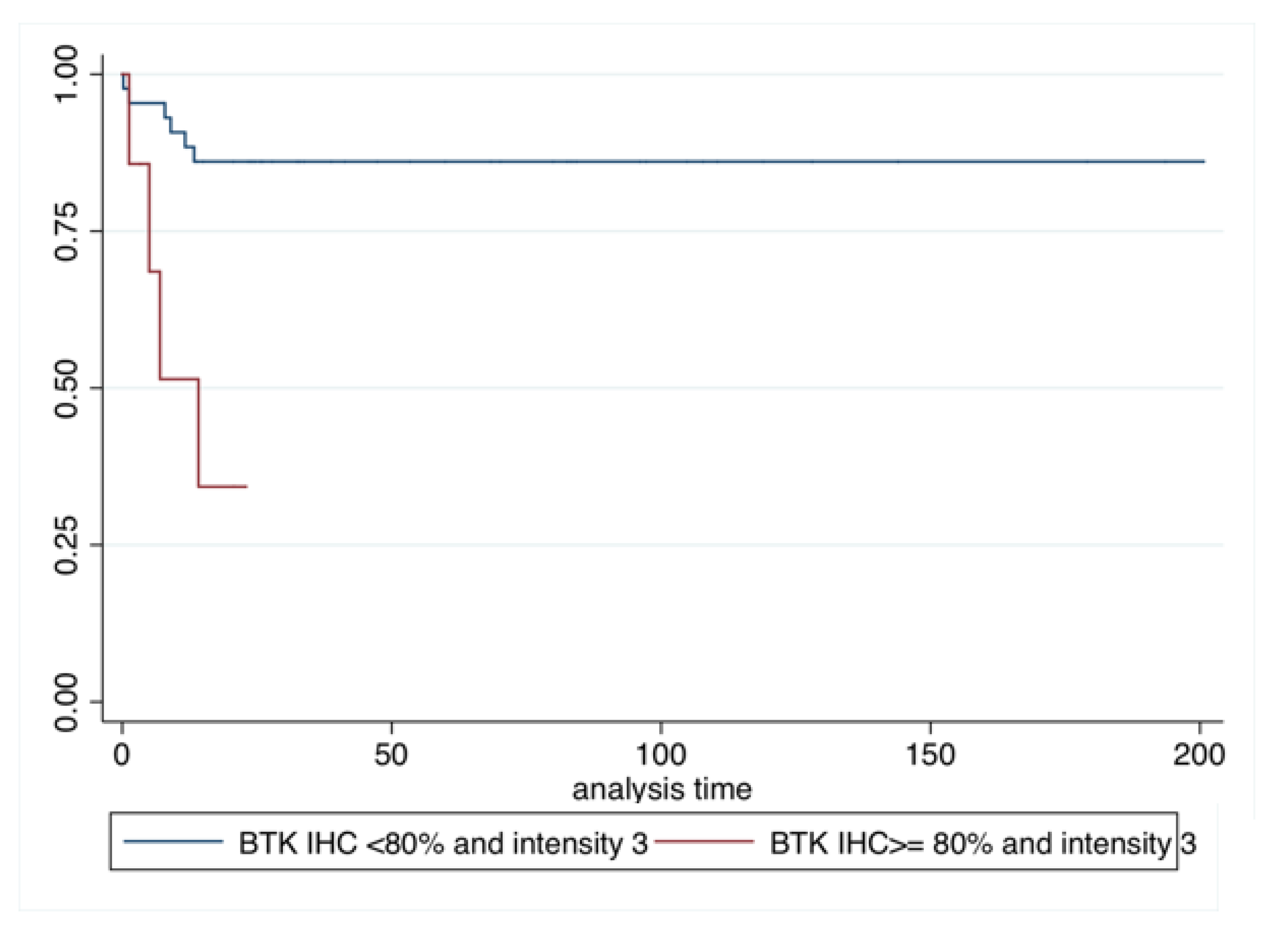
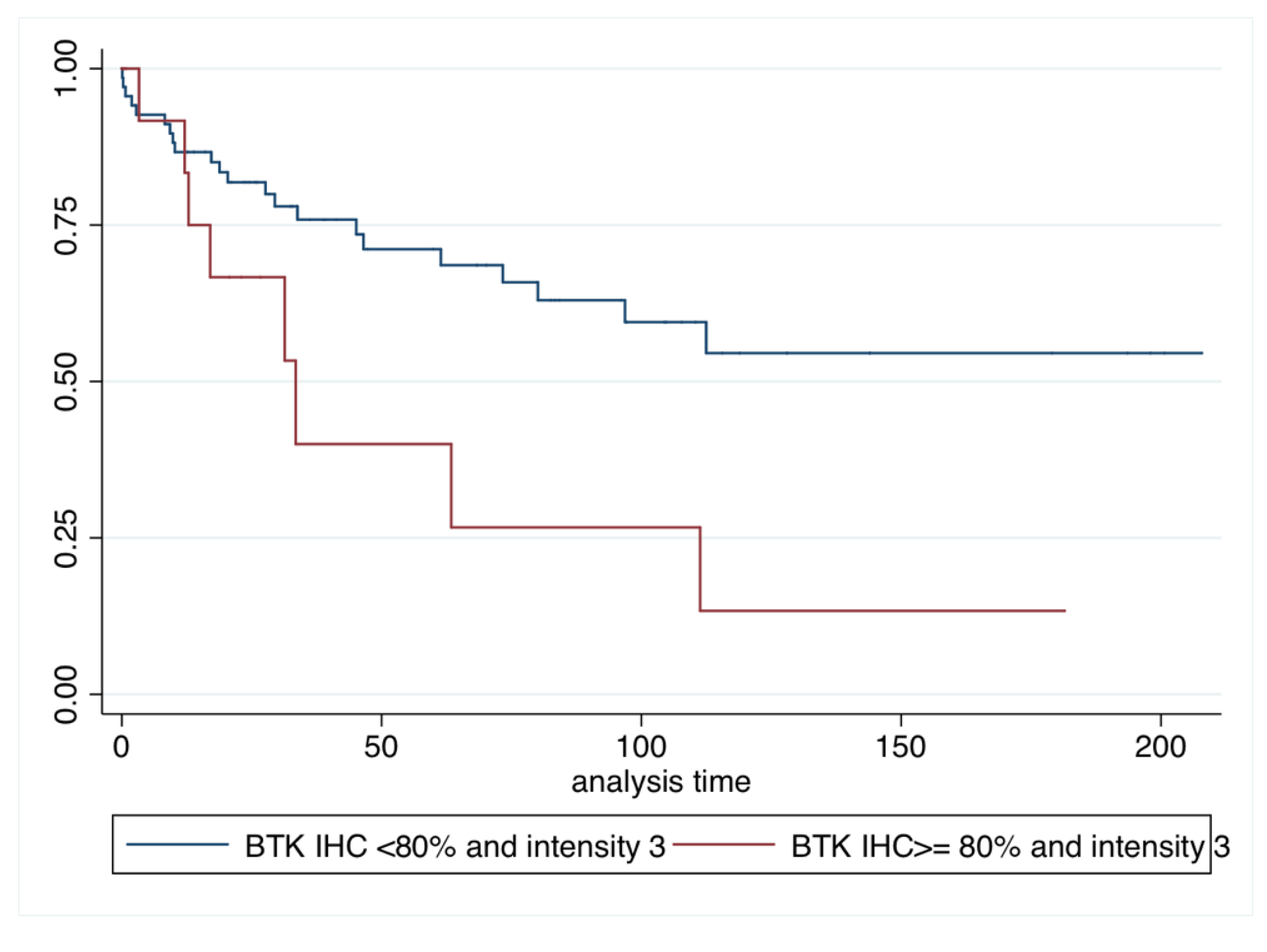
2.3. Survival Analysis
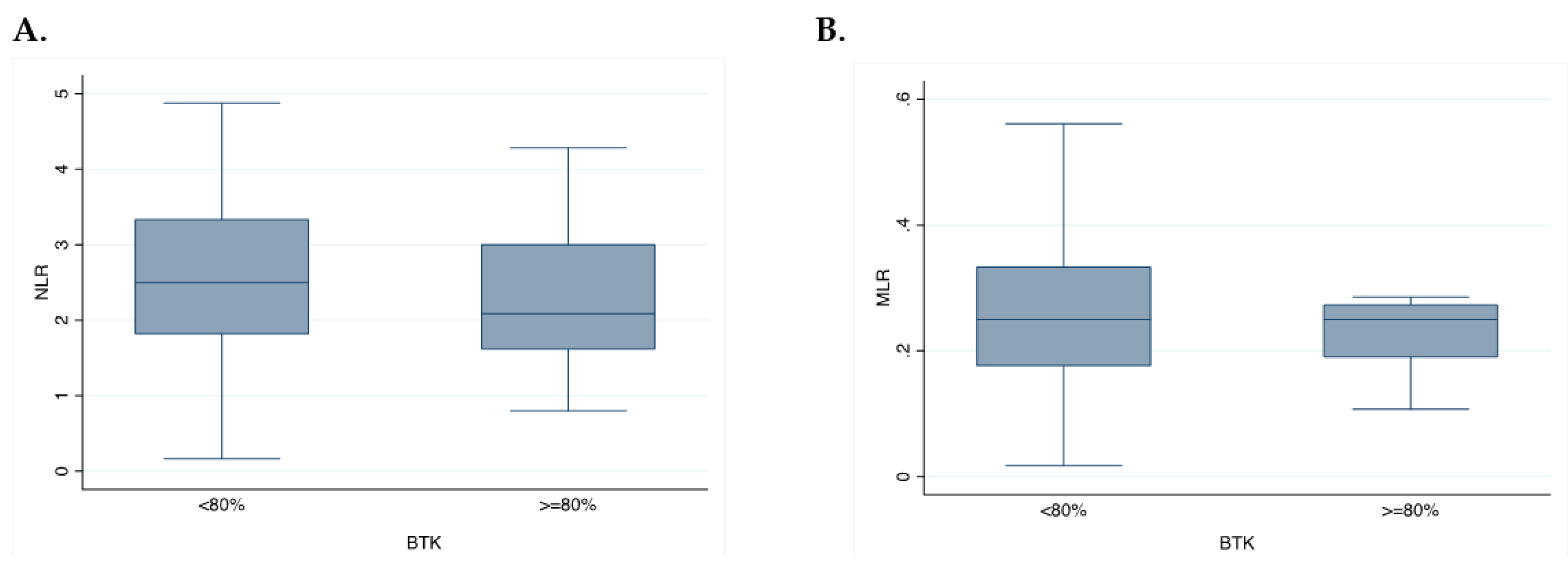
2.4. Exploratory Analysis
3. Discussion
4. Material and Methods
4.1. Study Design
4.2. Tissue Samples
4.3. Immunohistochemistry Assessment of BTK
4.4. Anti-p65BTK Antibody Production and Characterization
4.5. Blood Sample Analysis
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fedewa, S.A.; Ahnen, D.J.; Meester, R.G.S.; Barzi, A.; Jemal, A. Colorectal cancer statistics, 2017. CA Cancer J. Clin. 2017, 67, 177–193. [Google Scholar] [CrossRef]
- Arnold, M.; Sierra, M.S.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2016, 66, 683–691. [Google Scholar] [CrossRef] [Green Version]
- Pietrantonio, F.; Vernieri, C.; Siravegna, G.; Mennitto, A.; Berenato, R.; Perrone, F.; Gloghini, A.; Tamborini, E.; Lonardi, S.; Morano, F.; et al. Heterogeneity of acquired resistance to anti-EGFR monoclonal antibodies in patients with metastatic colorectal cancer. Clin. Cancer Res. 2016, 23, 2414–2422. [Google Scholar] [CrossRef]
- Ogino, S.; Nishihara, R.; VanderWeele, T.J.; Wang, M.; Nishi, A.; Lochhead, P.; Qian, Z.R.; Zhang, X.; Wu, K.; Nan, H.; et al. Review article: The role of molecular pathological epidemiology in the study of neoplastic and non-neoplastic diseases in the era of precision medicine. Epidemiol. Camb. Mass 2016, 27, 602–611. [Google Scholar] [CrossRef]
- Parcesepe, P.; Giordano, G.; Laudanna, C.; Febbraro, A.; Pancione, M. Cancer-associated immune resistance and evasion of immune surveillance in colorectal cancer. Gastroenterol. Res. Pract. 2016, 2016, 1–8. [Google Scholar] [CrossRef]
- Lim, B.; Kim, J.-H.; Kim, M.; Kim, S.-Y. Genomic and epigenomic heterogeneity in molecular subtypes of gastric cancer. World J. Gastroenterol. 2016, 22, 1190–1201. [Google Scholar] [CrossRef]
- Galon, J.; Mlecnik, B.; Bindea, G.; Angell, H.K.; Berger, A.; Lagorce, C.; Lugli, A.; Zlobec, I.; Hartmann, A.; Bifulco, C.; et al. Towards the introduction of the “Immunoscore” in the classification of malignant tumours. J. Pathol. 2014, 232, 199–209. [Google Scholar] [CrossRef]
- Basile, D.; Garattini, S.K.; Bonotto, M.; Ongaro, E.; Casagrande, M.; Cattaneo, M.; Fanotto, V.; De Carlo, E.; Loupakis, F.; Urbano, F.; et al. Immunotherapy for colorectal cancer: Where are we heading? Expert Opin. Biol. Ther. 2017, 17, 709–721. [Google Scholar] [CrossRef]
- Markman, J.L.; Shiao, S.L. Impact of the immune system and immunotherapy in colorectal cancer. J. Gastrointest. Oncol. 2015, 6, 208–223. [Google Scholar]
- Grassilli, E.; Pisano, F.; Cialdella, A.; Bonomo, S.; Missaglia, C.; Cerrito, M.G.; Masiero, L.; Ianzano, L.; Giordano, F.; Cicirelli, V.; et al. A novel oncogenic BTK isoform is overexpressed in colon cancers and required for RAS-mediated transformation. Oncogene 2016, 35, 4368–4378. [Google Scholar] [CrossRef] [Green Version]
- Mano, H. Tec family of protein-tyrosine kinases: An overview of their structure and function. Cytokine Growth Factor Rev. 1999, 10, 267–280. [Google Scholar] [CrossRef]
- Molina-Cerrillo, J.; Alonso-Gordoa, T.; Gajate, P.; Grande, E. Bruton’s tyrosine kinase (BTK) as a promising target in solid tumors. Cancer Treat. Rev. 2017, 58, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Vega, I.; Quirós, L.M.; Santos-Juanes, J.; Pane-Foix, M.; Marafioti, T. Bruton’s tyrosine kinase (Btk) is a useful marker for Hodgkin and B cell non-Hodgkin lymphoma. Virchows Arch. Int. J. Pathol. 2015, 466, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Ianzano, L.; Bonomo, S.; Cialdella, A.; Pisano, F.; Cerrito, M.G.; Carola, M.; McLean, C.; Romano, G.; Giovannoni, R.; Agostini, M.; et al. p65BTK targeting restores the apoptotic response to chemotherapy of p53-null drug-resistant colon cancer cells. Eur. J. Cancer 2016, 69, S140. [Google Scholar] [CrossRef]
- Dienstmann, R.; Salazar, R.; Tabernero, J. Personalizing colon cancer adjuvant therapy: Selecting optimal treatments for individual patients. J. Clin. Oncol. J. Am. Soc. Clin. Oncol. 2015, 33, 1787–1796. [Google Scholar] [CrossRef] [PubMed]
- Hammond, W.A.; Swaika, A.; Mody, K. Pharmacologic resistance in colorectal cancer: A review. Ther. Adv. Med. Oncol. 2016, 8, 57–84. [Google Scholar] [CrossRef] [PubMed]
- Guinney, J.; Dienstmann, R.; Wang, X.; de Reyniès, A.; Schlicker, A.; Soneson, C.; Marisa, L.; Roepman, P.; Nyamundanda, G.; Angelino, P.; et al. The consensus molecular subtypes of colorectal cancer. Nat. Med. 2015, 21, 1350–1356. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.-M.; Lv, J.-F.; Gong, L.; Yu, L.-Y.; Chen, X.-P.; Zhou, H.-H.; Fan, L. Role of deficient mismatch repair in the personalized management of colorectal cancer. Int. J. Environ. Res. Public. Health 2016, 13, 892. [Google Scholar] [CrossRef] [PubMed]
- Pal Singh, S.; Dammeijer, F.; Hendriks, R.W. Role of Bruton’s tyrosine kinase in B cells and malignancies. Mol. Cancer 2018, 17, 57. [Google Scholar] [CrossRef]
- Mohamed, A.J.; Yu, L.; Bäckesjö, C.-M.; Vargas, L.; Faryal, R.; Aints, A.; Christensson, B.; Berglöf, A.; Vihinen, M.; Nore, B.F.; et al. Bruton’s tyrosine kinase (Btk): Function, regulation, and transformation with special emphasis on the PH domain. Immunol. Rev. 2009, 228, 58–73. [Google Scholar] [CrossRef]
- Sala, L.; Cirillo, G.; Riva, G.; Romano, G.; Giussani, C.; Cialdella, A.; Todisco, A.; Virtuoso, A.; Cerrito, M.G.; Bentivegna, A.; et al. Specific expression of a new Bruton tyrosine kinase isoform (p65BTK) in the glioblastoma gemistocytic histotype. Front. Mol. Neurosci. 2019, 12, 2. [Google Scholar] [CrossRef] [PubMed]
- Giordano, F.; Vaira, V.; Cortinovis, D.; Bonomo, S.; Goedmakers, J.; Brena, F.; Cialdella, A.; Ianzano, L.; Forno, I.; Cerrito, M.G.; et al. Targeting p65BTK is a novel strategy for KRAS-mutated/EGFR-wild type lung adenocarcinoma. J. Exp. Clin Cancer Res. 2019, in press. [Google Scholar] [CrossRef] [PubMed]
- Schiavoni, G.; Gabriele, L.; Mattei, F. The tumor microenvironment: A pitch for multiple players. Front. Oncol. 2013, 3, 90. [Google Scholar] [CrossRef] [PubMed]
- Smyth, M.J.; Godfrey, D.I.; Trapani, J.A. A fresh look at tumor immunosurveillance and immunotherapy. Nat. Immunol. 2001, 2, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Voena, C.; Chiarle, R. Advances in cancer immunology and cancer immunotherapy. Discov. Med. 2016, 21, 125–133. [Google Scholar] [PubMed]
- Gabrilovich, D.I.; Nagaraj, S. Myeloid-derived suppressor cells as regulators of the immune system. Nat. Rev. Immunol. 2009, 9, 162–174. [Google Scholar] [CrossRef] [PubMed]
- Trikha, P.; Carson, W.E. Signaling pathways involved in MDSC regulation. Biochim. Biophys. Acta 2014, 1846, 55–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edin, S.; Wikberg, M.L.; Dahlin, A.M.; Rutegård, J.; Öberg, Å.; Oldenborg, P.-A.; Palmqvist, R. The distribution of macrophages with a M1 or M2 phenotype in relation to prognosis and the molecular characteristics of colorectal cancer. PLoS ONE 2012, 7, e47045. [Google Scholar] [CrossRef]
- Henze, A.-T.; Mazzone, M. The impact of hypoxia on tumor-associated macrophages. J. Clin. Investig. 2016, 126, 3672–3679. [Google Scholar] [CrossRef]
- Stiff, A.; Trikha, P.; Wesolowski, R.; Kendra, K.; Hsu, V.; Uppati, S.; McMichael, E.; Duggan, M.; Campbell, A.; Keller, K.; et al. Myeloid-derived suppressor cells express Bruton’s tyrosine kinase and can be depleted in tumor-bearing hosts by ibrutinib treatment. Cancer Res. 2016, 76, 2125–2136. [Google Scholar] [CrossRef]
- Ren, L.; Campbell, A.; Fang, H.; Gautam, S.; Elavazhagan, S.; Fatehchand, K.; Mehta, P.; Stiff, A.; Reader, B.F.; Mo, X.; et al. Analysis of the effects of the Bruton’s tyrosine kinase (Btk) inhibitor ibrutinib on monocyte Fcγ receptor (FcγR) function. J. Biol. Chem. 2016, 291, 3043–3052. [Google Scholar] [CrossRef] [PubMed]
- Kehlet, S.N.; Sanz-Pamplona, R.; Brix, S.; Leeming, D.J.; Karsdal, M.A.; Moreno, V. Excessive collagen turnover products are released during colorectal cancer progression and elevated in serum from metastatic colorectal cancer patients. Sci. Rep. 2016, 6, 30599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guthrie, G.J.K.; Charles, K.A.; Roxburgh, C.S.D.; Horgan, P.G.; McMillan, D.C.; Clarke, S.J. The systemic inflammation-based neutrophil-lymphocyte ratio: Experience in patients with cancer. Crit. Rev. Oncol. Hematol. 2013, 88, 218–230. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Zhao, R.; Cui, Y.; Zhou, Y.; Wu, X. The dynamic change of neutrophil to lymphocyte ratio can predict clinical outcome in stage I-III colon cancer. Sci. Rep. 2018, 8, 9453. [Google Scholar] [CrossRef] [PubMed]
- Peng, J.; Li, H.; Ou, Q.; Lin, J.; Wu, X.; Lu, Z.; Yuan, Y.; Wan, D.; Fang, Y.; Pan, Z. Preoperative lymphocyte-to-monocyte ratio represents a superior predictor compared with neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios for colorectal liver-only metastases survival. OncoTargets Ther. 2017, 10, 3789–3799. [Google Scholar] [CrossRef] [PubMed]
- Lavitrano, M.; Cerrito, M.G.; Bonomo, S.; Ianzano, L.; Cialdella, A.; Pisano, F.; Missaglia, C.; Giovannoni, R.; Romano, G.; McLean, C.M.; et al. BTK inhibitors synergize with 5-FU to treat drug-resistant p53-null colon cancers. J. Pathol. (under review).
- Liu, H.; Wu, T. Estimating the area under a receiver operating characteristic curve for repeated measures design. J. Stat. Softw. 2003, 8, 1–18. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | N = 87 | % |
|---|---|---|
| Age | ||
| <70 | 61 | 70.11 |
| ≥70 | 26 | 29.89 |
| Sex | ||
| M | 51 | 58.62 |
| F | 36 | 41.38 |
| Sidedness | ||
| Right | 50 | 57.47 |
| Left | 37 | 42.53 |
| Grading | ||
| G2 | 65 | 74.71 |
| G3 | 22 | 25.29 |
| Histology | ||
| Adenocarcinoma | 77 | 88.51 |
| Mucinous adenocarcinoma | 10 | 11.49 |
| Adj CT | ||
| No | 25 | 28.73 |
| Yes | 53 | 60.91 |
| PD (metastatic disease) | ||
| No | 43 | 49.42 |
| Yes | 25 | 28.73 |
| Rapid disease | ||
| No | 75 | 86.21 |
| Yes | 12 | 13.79 |
| KRAS | ||
| WT | 9 | 10.34 |
| Mut | 10 | 11.49 |
| BRAF | ||
| WT | 13 | 14.94 |
| Mut | 3 | 3.44 |
| BTK 0% | 9 | 10.34 |
| BTK IHC ≥ 1% and intensity 1 | ||
| No | 38 | 43.68 |
| Yes | 47 | 54.02 |
| Missing (lack of sample) | 2 | 2.30 |
| BTK IHC ≥ 50% and intensity 2 | ||
| No | 75 | 86.2 |
| Yes | 10 | 11.5 |
| Missing (lack of sample) | 2 | 2.30 |
| BTK IHC ≥ 80% and intensity 3 | ||
| No | 70 | 80.45 |
| Yes | 15 | 17.25 |
| Missing (lack of sample) | 2 | 2.30 |
| Variables | BTK Intensity 1 | BTK Intensity 2 | BTK Intensity 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| IHC < 1% | IHC ≥ 1% | p | IHC < 50% | IHC ≥ 50% | p | IHC < 80% | IHC ≥ 80% | p | |
| N = 38 | N = 47 | N = 75 | N = 11 | N = 70 | N = 15 | ||||
| Sidedness | |||||||||
| Right | 23 | 26 | 0.629 | 42 | 7 | 0.400 | 42 | 7 | 0.343 |
| Left | 15 | 21 | 33 | 3 | 28 | 8 | |||
| Grading | |||||||||
| G2 | 20 | 26 | 0.813 | 38 | 8 | 0.083 | 40 | 6 | 0.977 |
| G3 | 6 | 9 | 15 | 0 | 13 | 2 | |||
| Histotype | |||||||||
| Adenocarcinoma | 21 | 27 | 0.732 | 44 | 4 | 0.034 | 40 | 8 | 0.114 |
| Mucinous adenocarcinoma | 5 | 8 | 9 | 4 | 13 | 0 | |||
| KRAS | |||||||||
| Wild type | 5 | 4 | 0.498 | 37 | 6 | 0.533 | 39 | 4 | 0.161 |
| Mutated | 4 | 6 | 21 | 2 | 18 | 5 | |||
| Metastatic disease | |||||||||
| No | 16 | 27 | 0.241 | 8 | 1 | 0.596 | 8 | 1 | 0.937 |
| Yes | 12 | 11 | 8 | 2 | 9 | 1 | |||
| Age | |||||||||
| <70 | 28 | 30 | 0.403 | 49 | 9 | 0.127 | 48 | 10 | 0.826 |
| ≥70 | 10 | 16 | 25 | 1 | 21 | 5 | |||
| Sex | |||||||||
| M | 21 | 30 | 0.423 | 47 | 4 | 0.169 | 42 | 9 | 1.000 |
| F | 17 | 17 | 28 | 6 | 28 | 6 | |||
| Variables | N = 15 | % |
|---|---|---|
| OS | ||
| Uncensored | 9 | 60.00 |
| Censored | 6 | 40.00 |
| Rapid disease | ||
| Yes | 3 | 20.00 |
| No | 12 | 80.00 |
| Metastatic recurrence | ||
| Yes | 5 | 33.00 |
| No | 4 | 26.66 |
| Missing | 6 | 40.00 |
| Adj chemotherapy received | ||
| Fluoropyrimidenes (only) | 3 | 20.00 |
| Fluoropyrimidines plus oxaliplatin | 6 | 40.00 |
| Missing | 6 | 40.00 |
| Variables | HR | p | 95%CI |
|---|---|---|---|
| Age | |||
| ≥70 | 0.81 | 0.753 | 0.21–2.99 |
| Sidedness | |||
| Left | 1.18 | 0.769 | 0.37–3.74 |
| KRAS | |||
| Mut | 0.31 | 0.210 | 0.05–1.92 |
| BRAF | |||
| Mut | 1.33 | 0.814 | 0.11–15.06 |
| BTK IHC ≥ 1% and intensity 1 | |||
| Yes | 0.71 | 0.601 | 0.20–2.48 |
| BTK IHC ≥ 50% and intensity 2 | |||
| Yes | 1.83 | 0.953 | 0.52–4.65 |
| BTK IHC ≥ 80% and intensity 3 | |||
| Yes | 1.18 | 0.005 | 1.75–22.79 |
| Variables | HR | p-Value | 95%CI |
|---|---|---|---|
| Age | |||
| ≥70 | 1.49 | 0.278 | 0.72–3.11 |
| Sidedness | |||
| Left | 0.95 | 0.910 | 0.46–1.96 |
| KRAS | |||
| Mut | 0.39 | 0.213 | 0.09–1.69 |
| BRAF | |||
| Mut | 7.59 | 0.099 | 0.68–84.41 |
| BTK IHC ≥ 1% and intensity 1 | |||
| Yes | 0.61 | 0.190 | 0.30–1.26 |
| BTK IHC ≥ 50% and intensity 2 | |||
| Yes | 0.89 | 0.843 | 0.31–2.58 |
| BTK IHC ≥ 80% and intensity 3 | |||
| Yes | 2.54 | 0.025 | 1.12–5.76 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Basile, D.; Gerratana, L.; Buonadonna, A.; Garattini, S.K.; Perin, T.; Grassilli, E.; Miolo, G.; Cerrito, M.G.; Belluco, C.; Bertola, G.; et al. Role of Bruton’s Tyrosine Kinase in Stage III Colorectal Cancer. Cancers 2019, 11, 880. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11060880
Basile D, Gerratana L, Buonadonna A, Garattini SK, Perin T, Grassilli E, Miolo G, Cerrito MG, Belluco C, Bertola G, et al. Role of Bruton’s Tyrosine Kinase in Stage III Colorectal Cancer. Cancers. 2019; 11(6):880. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11060880
Chicago/Turabian StyleBasile, Debora, Lorenzo Gerratana, Angela Buonadonna, Silvio Ken Garattini, Tiziana Perin, Emanuela Grassilli, Gianmaria Miolo, Maria Grazia Cerrito, Claudio Belluco, Giulio Bertola, and et al. 2019. "Role of Bruton’s Tyrosine Kinase in Stage III Colorectal Cancer" Cancers 11, no. 6: 880. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11060880