BCG Therapy of Bladder Cancer Stimulates a Prolonged Release of the Chemoattractant CXCL10 (IP10) in Patient Urine

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Rationale for Study Design
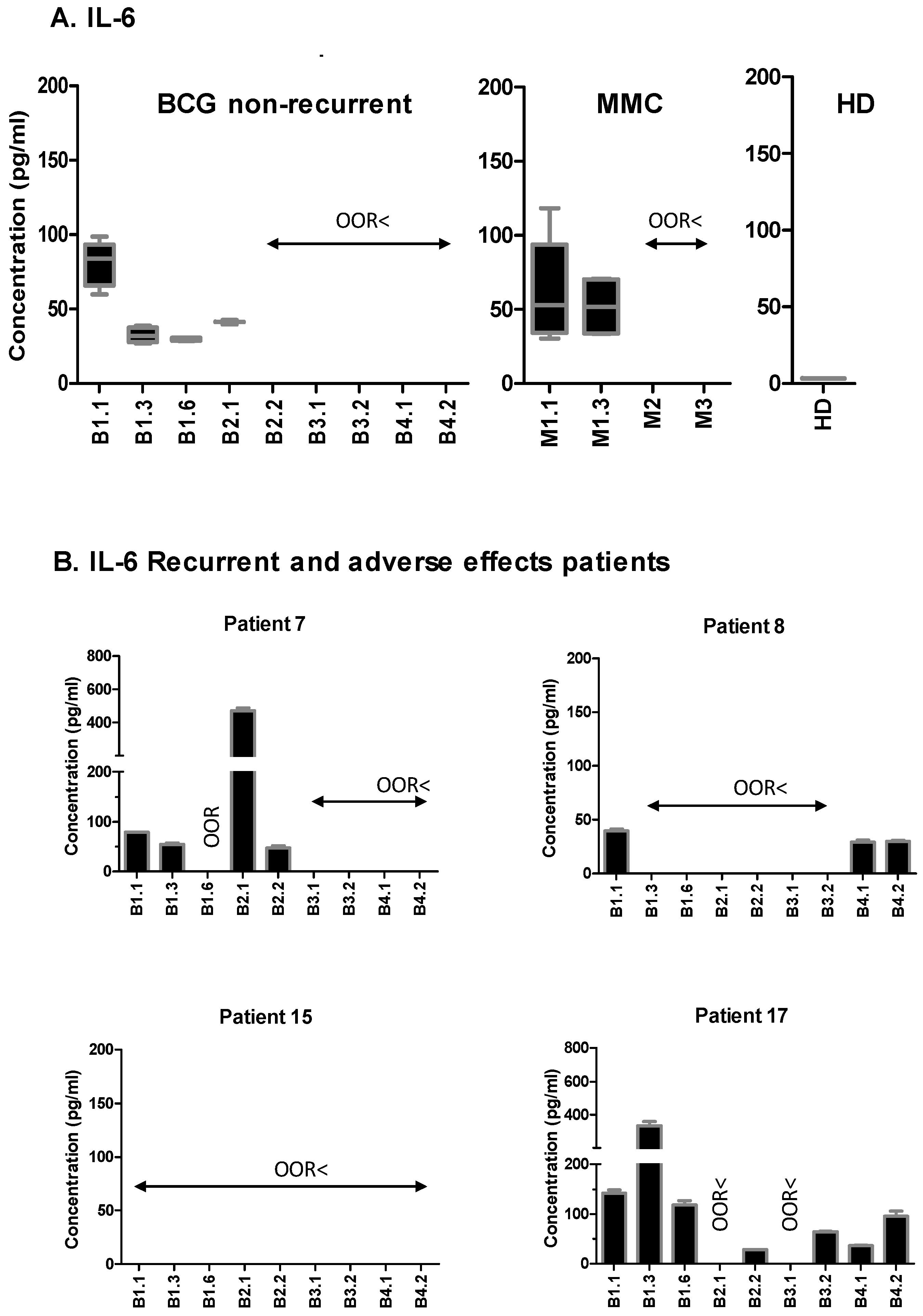
2.2. NMIBC Patients Release Immune Mediators One Week after BCG Instillation
2.3. CXCL10 (IP10) Is Highly Secreted in BCG-Treated NMIBC Patients Seven Days after the Instillations
2.4. Urinary CXCL10 Is Produced by Myeloid Cells
2.5. CXCL10 Does Not Increase the Percentage of Anti-Tumour CD56bright Cells, but Facilitates in the Migration of BCG-Activated Effector Cells
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Sample Handling
4.3. Creatinine Determination
4.4. Cytokine Measurements
4.5. Statistical Analyses
4.6. IP10 Stimulation of PBMCs
4.7. Flow Cytometry
4.8. Peripheral Blood Mononuclear Cell Stimulation with BCG
4.9. Migration Experiments
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gandhi, N.M.; Morales, A.; Lamm, D.L. Bacillus Calmette-Guérin immunotherapy for genitourinary cancer. BJU Int. 2013, 112, 288–297. [Google Scholar] [CrossRef] [PubMed]
- Kamat, A.M.; Li, R.; O’Donnell, M.A.; Black, P.C.; Roupret, M.; Catto, J.W.; Comperat, E.; Ingersoll, M.A.; Witjes, W.P.; McConkey, D.J.; et al. Predicting Response to Intravesical Bacillus Calmette-Guerin Immunotherapy: Are We There Yet? A Systematic Review. Eur. Urol. 2017, 73, 738–748. [Google Scholar] [CrossRef] [PubMed]
- Isharwal, S.; Konety, B. Non-muscle invasive bladder cancer risk stratification. Indian J. Urol. 2015, 31, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Sylvester, R.J. How Well Can You Actually Predict Which Non–Muscle-Invasive Bladder Cancer Patients Will Progress? Eur. Urol. 2011, 60, 431–433. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Gomez, J.; Madero, R.; Solsona, E.; Unda, M.; Martínez-Piñeiro, L.; Ojea, A.; Portillo, J.; Montesinos, M.; Gonzalez, M.; Pertusa, C.; et al. The EORTC Tables Overestimate the Risk of Recurrence and Progression in Patients with Non–Muscle-Invasive Bladder Cancer Treated with Bacillus Calmette-Guérin: External Validation of the EORTC Risk Tables. Eur. Urol. 2011, 60, 423–430. [Google Scholar] [CrossRef] [PubMed]
- García-Cuesta, E.M.; Esteso, G.; Ashiru, O.; López Cobo, S.; Álvarez-Maestro, M.; Linares, A.; Ho, M.M.; Martínez-Piñeiro, L.; Reyburn, H.T.; Valés-Gómez, M. Characterization of a human anti-tumoral NK cell population expanded after BCG treatment of leukocytes. OncoImmunology 2017, 6, e1293212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, J.A.; Rosario, M.; Romee, R.; Berrien-Elliott, M.M.; Schneider, S.E.; Leong, J.W.; Sullivan, R.P.; Jewell, B.A.; Becker-Hapak, M.; Schappe, T.; et al. CD56bright NK cells exhibit potent antitumor responses following IL-15 priming. J. Clin. Investig. 2017, 127, 4042–4058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bisiaux, A.; Thiounn, N.; Timsit, M.-O.; Eladaoui, A.; Chang, H.-H.; Mapes, J.; Mogenet, A.; Bresson, J.-L.; Prié, D.; Béchet, S.; et al. Molecular Analyte Profiling of the Early Events and Tissue Conditioning Following Intravesical Bacillus Calmette-Guerin Therapy in Patients with Superficial Bladder Cancer. J. Urol. 2009, 181, 1571–1580. [Google Scholar] [CrossRef] [PubMed]
- Zuiverloon, T.C.; Nieuweboer, A.J.; Vekony, H.; Kirkels, W.J.; Bangma, C.H.; Zwarthoff, E.C. Markers predicting response to bacillus Calmette-Guerin immunotherapy in high-risk bladder cancer patients: a systematic review. Eur. Urol. 2011, 61, 128–145. [Google Scholar] [CrossRef]
- Zuiverloon, T.C.; Zwarthoff, E.C. Predicting Response to Intravesical Bacillus Calmette-Guérin Immunotherapy: Are We Moving Forward? Eur. Urol. 2016, 69, 201–202. [Google Scholar] [CrossRef]
- Urquidi, V.; Goodison, S.; Kim, J.; Chang, M.; Dai, Y.; Rosser, C.J. Vascular endothelial growth factor, carbonic anhydrase 9, and angiogenin as urinary biomarkers for bladder cancer detection. Urology 2012, 79, 1185-e1–1185-e6. [Google Scholar] [CrossRef] [PubMed]
- Kamat, A.M.; Briggman, J.; Urbauer, D.L.; Svatek, R.; Nogueras Gonzalez, G.M.; Anderson, R.; Grossman, H.B.; Prat, F.; Dinney, C.P. Cytokine Panel for Response to Intravesical Therapy (CyPRIT): Nomogram of Changes in Urinary Cytokine Levels Predicts Patient Response to Bacillus Calmette-Guerin. Eur. Urol. 2016, 69, 197–200. [Google Scholar] [CrossRef] [PubMed]
- Gogalic, S.; Sauer, U.; Doppler, S.; Heinzel, A.; Perco, P.; Lukas, A.; Simpson, G.; Pandha, H.; Horvath, A.; Preininger, C. Validation of a protein panel for the noninvasive detection of recurrent non-muscle invasive bladder cancer. Biomarkers 2017, 22, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Müller, C.; Tufa, D.M.; Chatterjee, D.; Muhlradt, P.F.; Schmidt, R.E.; Jacobs, R. The TLR-2/TLR-6 agonist macrophage-activating lipopeptide-2 augments human NK cell cytotoxicity when PGE2 production by monocytes is inhibited by a COX-2 blocker. Cancer Immunol. Immunother. 2015, 64, 1175–1184. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.J.; Kim, E.J.; Kim, S.K.; Kim, Y.J.; Ha, Y.S.; Jeong, P.; Kim, M.J.; Yun, S.J.; Lee, K.M.; Moon, S.K.; et al. Predictive value of progression-related gene classifier in primary non-muscle invasive bladder cancer. Mol. Cancer 2010, 9, 3. [Google Scholar] [CrossRef]
- Hedegaard, J.; Lamy, P.; Nordentoft, I.K.; Algaba, F.; Høyer, S.; Ulhøi, B.P.; Vang, S.; Reinert, T.; Hermann, G.G.; Mogensen, K.; et al. Comprehensive Transcriptional Analysis of Early-Stage Urothelial Carcinoma. Cancer Cell 2016, 30, 27–42. [Google Scholar] [CrossRef]
- Poppas, D.P.; Pavlovich, C.P.; Folkman, J.; E Voest, E.; Chen, X.; Luster, A.D.; O’Donnell, M.A. Intravesical bacille calmette-guérin induces the antiangiogenic chemokine interferon-inducible protein 10. Urology 1998, 52, 268–276. [Google Scholar] [CrossRef]
- De Boer, E.C.; Somogyi, L.; De Ruiter, G.J.W.; De Reijke, T.M.; Kurth, K.-H.; Schamhart, D.H.J.; Boer, E.C.; Ruiter, G.J.W.; Reijke, T.M. Role of interleukin-8 in onset of the immune response in intravesical BCG therapy for superficial bladder cancer. Urol. Res. 1997, 25, 31–34. [Google Scholar] [CrossRef] [Green Version]
- Thalmann, G.N.; Sermier, A.; Rentsch, C.; Möhrle, K.; Cecchini, M.G.; Studer, U.E. Urinary Interleukin-8 and 18 predict the response of superficial bladder cancer to intravesical therapy with bacillus Calmette-Guerin. J. Urol. 2000, 164, 2129–2133. [Google Scholar] [CrossRef]
- Qu, K.; Gu, J.; Ye, Y.; Williams, S.B.; Dinney, C.P.; Wu, X.; Kamat, A. High baseline levels of interleukin-8 in leukocytes and urine predict tumor recurrence in non-muscle invasive bladder cancer patients receiving bacillus Calmette–Guerin therapy: A long-term survival analysis. OncoImmunology 2017, 6, e1265719. [Google Scholar] [CrossRef]
- Taub, D.D.; Sayers, T.J.; Carter, C.R.; Ortaldo, J.R. Alpha and beta chemokines induce NK cell migration and enhance NK-mediated cytolysis. J. Immunol. 1995, 155, 3877–3888. [Google Scholar] [PubMed]
- O’Flaherty, S.M.; Sutummaporn, K.; Häggtoft, W.L.; Worrall, A.P.; Rizzo, M.; Braniste, V.; Höglund, P.; Kadri, N.; Chambers, B.J. TLR stimulated eosinophils mediate recruitment and activation of NK cells in vivo. Scand. J. Immunol. 2017, 85, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Spranger, S.; Gajewski, T.F. Impact of oncogenic pathways on evasion of antitumour immune responses. Nat. Rev. Cancer 2018, 18, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Wendel, M.; Galani, I.E.; Suri-Payer, E.; Cerwenka, A. Natural Killer Cell Accumulation in Tumors Is Dependent on IFN-γ and CXCR3 Ligands. Cancer Res. 2008, 68, 8437–8445. [Google Scholar] [CrossRef]
- Wennerberg, E.; Kremer, V.; Childs, R.; Lundqvist, A. CXCL10-induced migration of adoptively transferred human natural killer cells toward solid tumors causes regression of tumor growth in vivo. Cancer Immunol. Immunother. 2015, 64, 225–235. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BCG | MMC | ||||
|---|---|---|---|---|---|
| N | % | N | % | ||
| Gender | Male | 10 | 83.3 | 4 | 66.7 |
| Female | 2 | 16.7 | 2 | 33.3 | |
| Age | 60 or less | 2 | 16.7 | 0 | 0.0 |
| 61–70 | 6 | 50.0 | 5 | 83.3 | |
| more than 71 | 4 | 33.3 | 1 | 16.7 | |
| Size | <3 cm | 8 | 66.7 | 2 | 33.3 |
| ≥3 cm | 3 | 25.0 | 4 | 66.7 | |
| N/A | 1 | 8.3 | |||
| Number | <3 | 7 | 58.3 | 5 | 83.3 |
| ≥3 | 4 | 33.3 | 1 | 16.7 | |
| N/A | 1 | 8.3 | |||
| Primary | 11 | 91.7 | 6 | 100.0 | |
| Recurrent | 1 | 8.3 | 0 | 0.0 | |
| CIS | 5 | 41.7 | |||
| T1 | 7 | 58.3 | 4 | 66.7 | |
| Ta | 3 | 25.0 | 2 | 33.3 | |
| G1 | 0 | 0.0 | 1 | 16.7 | |
| G2 | 1 | 8.3 | 5 | 83.3 | |
| G3 | 10 | 83.3 | 0 | 0.0 | |
| Treatment delayed as a result of side effects | 4 | 33.3 | 0 | 0.0 | |
| Stop as a result of side effects | 1 | 8.3 | 0 | 0.0 | |
| Recurrence—n (%) | 4 | 33.3 | 0 | 0.0 | |
| Progression | 1 | 8.3 | 0 | 0.0 | |
| Patient | Tumor | Stop/Delay | Recurrence | Progression |
|---|---|---|---|---|
| P7 | Primary | After B1.6 as a result of discomfort | After B1.6, TUR Restart BCG with delay | |
| P8 | Previous tumors in 1990, 1995 | 2.7 years after B1.1 T4a | ||
| P15 | Primary | Delay after B3.2 as a result of prostate treatment | 2.4 years from B1.1: 2 × T1G2; 5 years from B1.1: 3 × TxGx | |
| P17 | Previous TaG2 | After B6.1 as a result of cystitis | 3.1 years from B1.1 TxGx |
| Cytokine/Chemokine | Limit * (pg/mL) | BCG # | Mitomycin # | Healthy |
|---|---|---|---|---|
| IL-1β | 10.0 | 3/12 | - | - |
| IL-2 | 28.03 | 5/12 | 4/6 | - |
| IL-4 | 16.87 | - | - | - |
| IL-5 | 14.59 | - | - | - |
| IL-6 | 20.08 | 6/12 | 3/6 | - |
| IL-8 | 17.74 | 7/12 | 5/6 | - |
| IL-9 | 2414.91 | - | - | - |
| IL-10 | 14.81 | - | - | - |
| IL-12p70 | 249.14 | - | - | - |
| IL-15 | 8.18 | - | - | - |
| IL-17 | 18.64 | - | - | - |
| IL-18BPa | 32.55 | + | + | + |
| IL-22 | 17.49 | 2/12 | - | + |
| IL-23 | 293.58 | 1/12 | - | - |
| TNF-α | 19.75 | - | - | - |
| IFN-γ | 6.3 | - | - | - |
| MIP1β | 48.23 | - | - | - |
| MIG | 843.21 | - | - | - |
| CXCL10 | 3.54 | 11/12 | 2/6 | - |
| RANTES | 14.53 | 5/12 | 1/6 | - |
| TRAIL | 34.98 | + | + | + |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ashiru, O.; Esteso, G.; García‐Cuesta, E.M.; Castellano, E.; Samba, C.; Escudero-López, E.; López‐Cobo, S.; Álvarez-Maestro, M.; Linares, A.; Ho, M.M.; et al. BCG Therapy of Bladder Cancer Stimulates a Prolonged Release of the Chemoattractant CXCL10 (IP10) in Patient Urine. Cancers 2019, 11, 940. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11070940
Ashiru O, Esteso G, García‐Cuesta EM, Castellano E, Samba C, Escudero-López E, López‐Cobo S, Álvarez-Maestro M, Linares A, Ho MM, et al. BCG Therapy of Bladder Cancer Stimulates a Prolonged Release of the Chemoattractant CXCL10 (IP10) in Patient Urine. Cancers. 2019; 11(7):940. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11070940
Chicago/Turabian StyleAshiru, Omodele, Gloria Esteso, Eva M. García‐Cuesta, Eva Castellano, Celia Samba, Eva Escudero-López, Sheila López‐Cobo, Mario Álvarez-Maestro, Ana Linares, Mei M. Ho, and et al. 2019. "BCG Therapy of Bladder Cancer Stimulates a Prolonged Release of the Chemoattractant CXCL10 (IP10) in Patient Urine" Cancers 11, no. 7: 940. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11070940