Non-Invasive Diagnostic System Based on Light for Detecting Early-Stage Oral Cancer and High-Risk Precancerous Lesions—Potential for Dentistry


Abstract
:Simple Summary
Abstract
1. Introduction
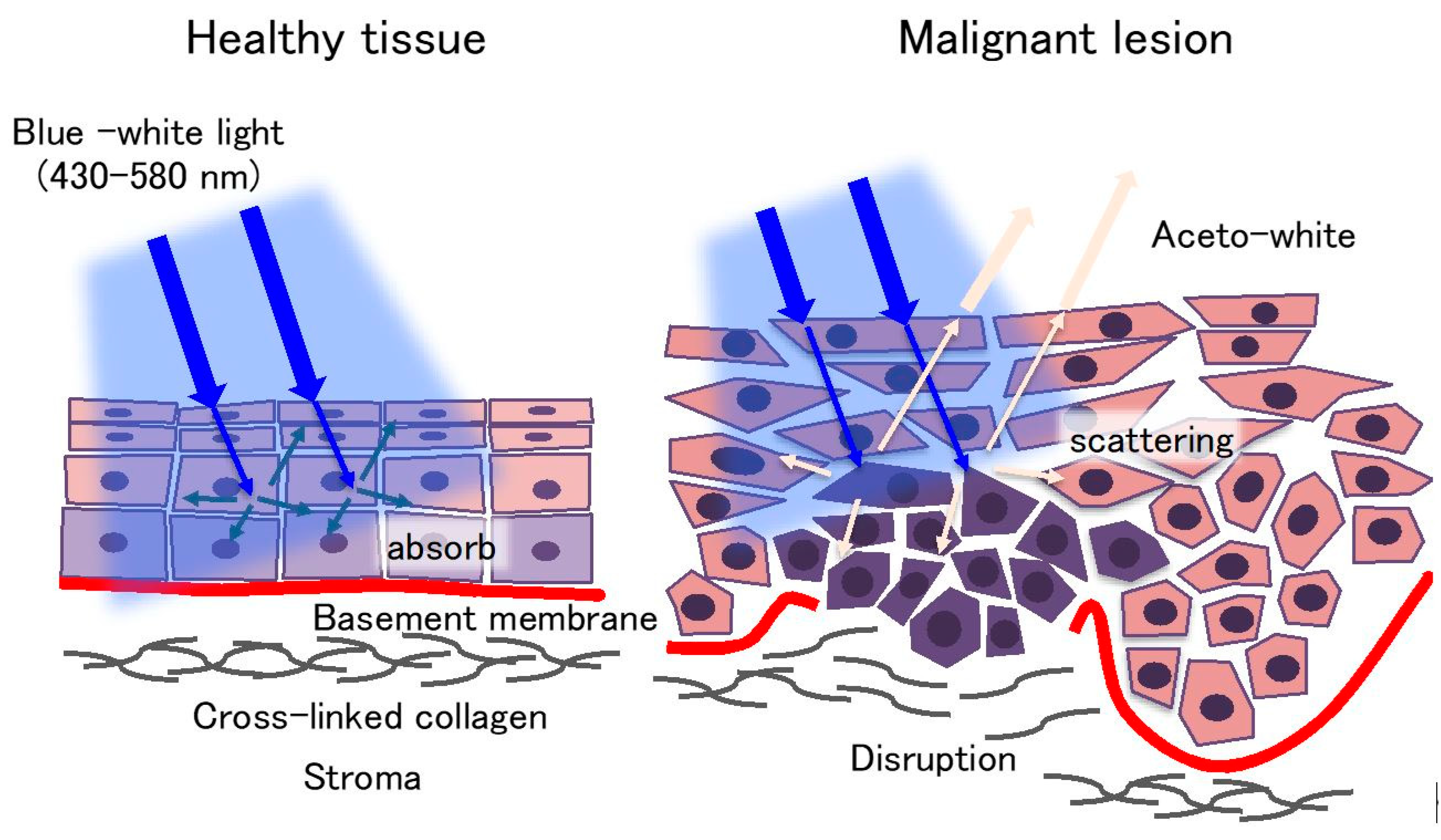
2. Examination under Chemiluminescent Illumination
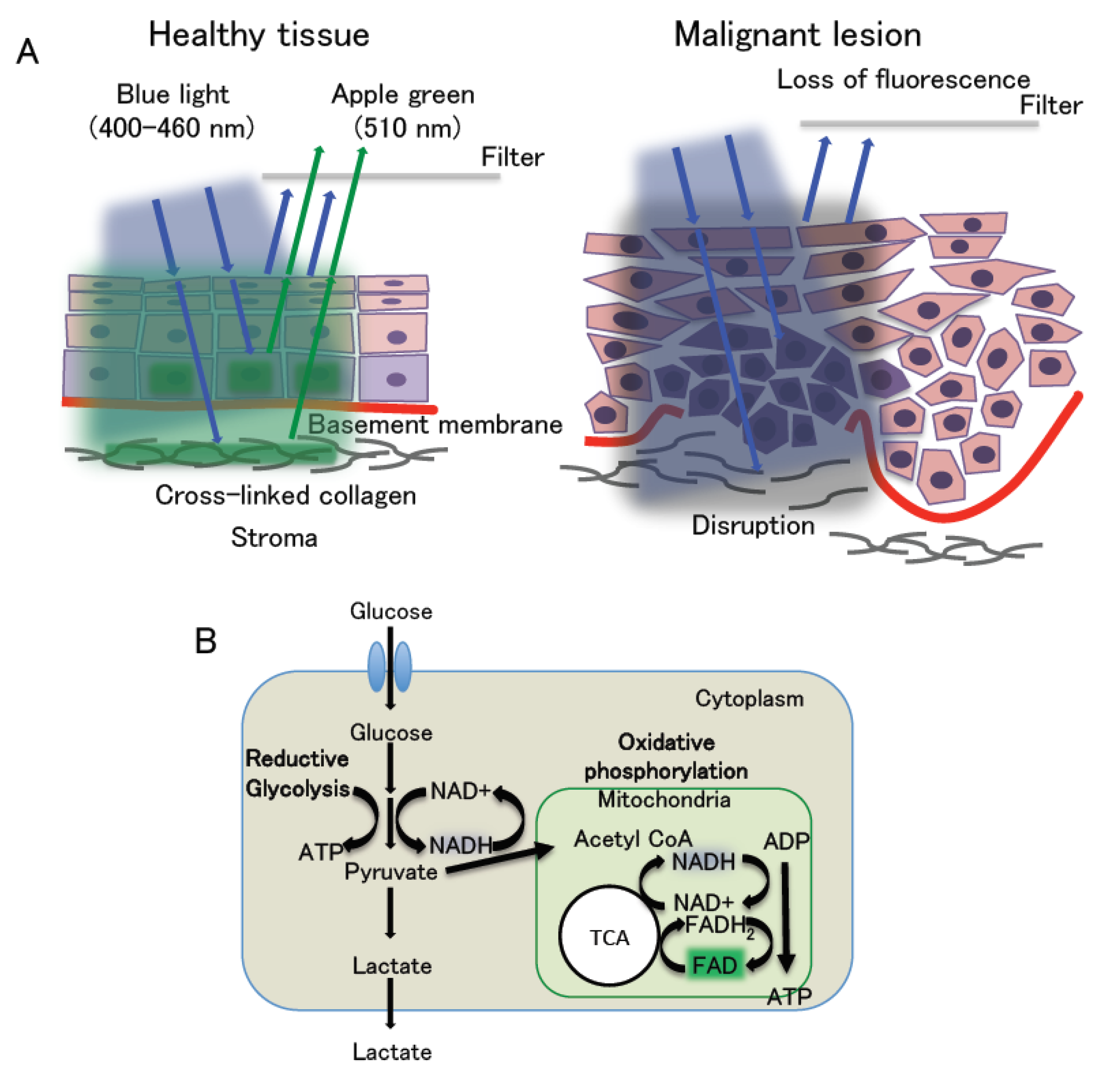
3. Autofluorescence Imaging
4. Photodynamic Diagnosis
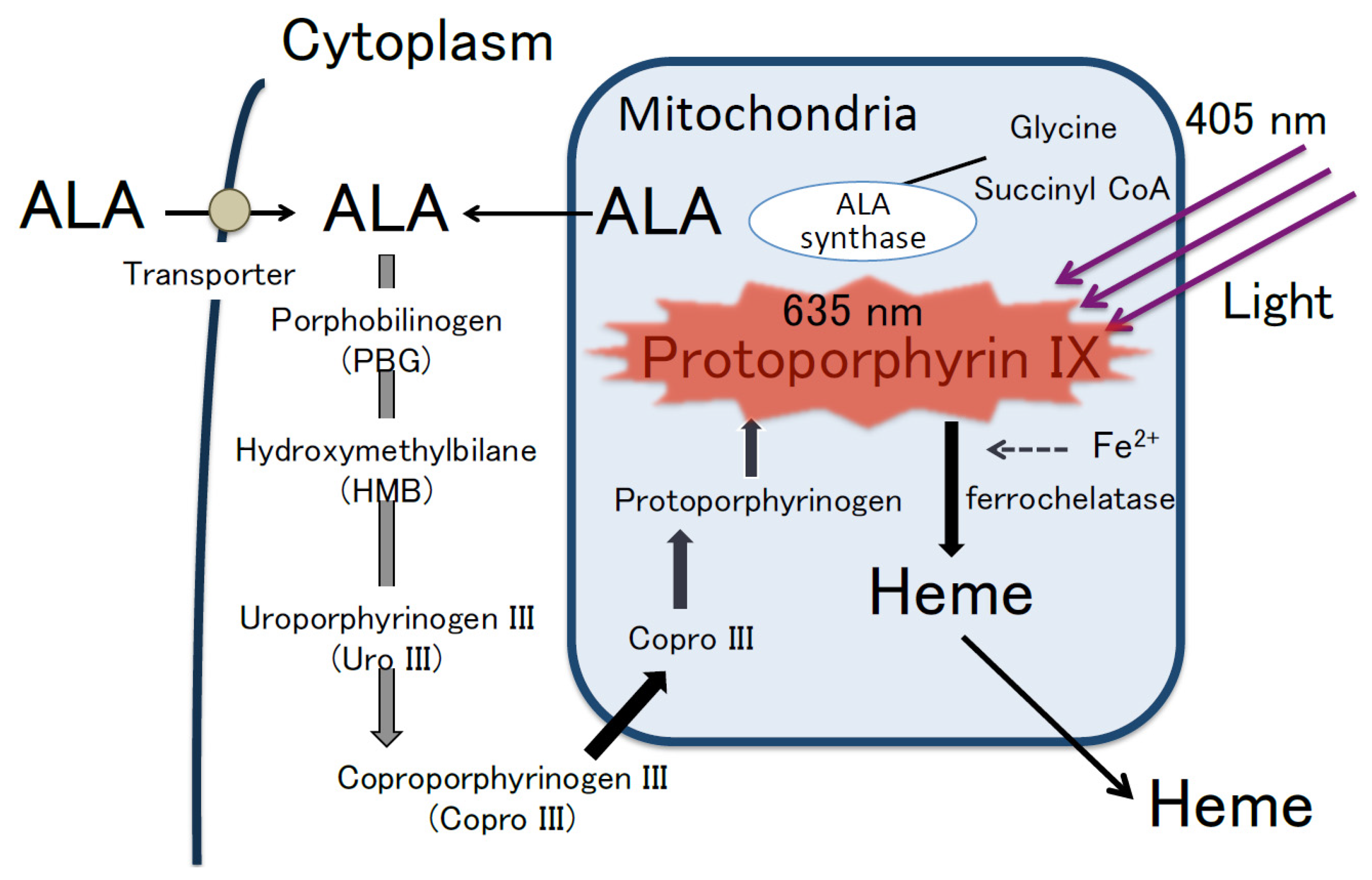
4.1. 5 Aminolevulinic Acid and the Mechanism of ALA-PDD
4.2. ALA Administration Route
4.3. Concentration of ALA
4.4. Side Effects of ALA
4.5. Clinical Application of ALA-PDD
4.5.1. ALA-PDD System
4.5.2. ALA Application for PDD
4.5.3. Clinical Application of ALA-PDD for Visualizing OED in OPMDs and OSCC
5. Issues and Future Perspectives
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Miranda-Filho, A.; Bray, F. Global patterns and trends in cancers of the lip, tongue and mouth. Oral Oncol. 2020, 102, 104551. [Google Scholar] [CrossRef] [PubMed]
- Warnakulasuriya, S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol. 2009, 45, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Sciubba, J.J. Oral cancer. The importance of early diagnosis and treatment. Am. J. Clin. Dermatol. 2001, 2, 239–251. [Google Scholar] [CrossRef] [PubMed]
- Van der Waal, I. Are we able to reduce the mortality and morbidity of oral cancer; Some considerations. Med. Oral Patol. Oral Cir. Bucal 2013, 18, e33–e37. [Google Scholar] [CrossRef] [PubMed]
- Reibel, J.; Gale, N.; Hille, J.; Hunt, J.L.; Lingen, M.; Muller, S.; Sloan, P.; Tilakaratne, W.M.; Westra, W.H.; Willams, M.D.; et al. Oral potentially malignant disorders and oral epithelial dysplasia. In WHO Classification of Head and Neck Tumours, 4th ed.; El-Naggar, A.K., Chan, J.K.C., Grandis, J.R., Takata, T., Slootweg, P.P.J., Eds.; IARC: Lyon, France, 2017; pp. 112–115. [Google Scholar]
- Kuribayashi, Y.; Tsushima, F.; Sato, M.; Morita, K.; Omura, K. Recurrence patterns of oral leukoplakia after curative surgical resection: Important factors that predict the risk of recurrence and malignancy. J. Oral Pathol. Med. 2012, 41, 682–688. [Google Scholar] [CrossRef] [PubMed]
- Mehanna, H.M.; Rattay, T.; Smith, J.; McConkey, C.C. Treatment and follow-up of oral dysplasia—A systematic review and meta-analysis. Head Neck 2009, 31, 1600–1609. [Google Scholar] [CrossRef]
- Sperandio, M.; Brown, A.L.; Lock, C.; Morgan, P.R.; Coupland, V.H.; Madden, P.B.; Warnakulasuriya, S.; Møller, H.; Odell, E.W. Predictive value of dysplasia grading and DNA ploidy in malignant transformation of oral potentially malignant disorders. Cancer Prev. Res. 2013, 6, 822–831. [Google Scholar] [CrossRef] [Green Version]
- Warnakulasuriya, S.; Kovacevic, T.; Madden, P.; Coupland, V.H.; Sperandio, M.; Odell, E.; Møller, H. Factors predicting malignant transformation in oral potentially malignant disorders among patients accrued over a 10-year period in South East England. J. Oral Pathol. Med. 2011, 40, 677–683. [Google Scholar] [CrossRef]
- Speight, P.M.; Khurram, S.A.; Kujan, O. Oral potentially malignant disorders: Risk of progression to malignancy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 612–627. [Google Scholar] [CrossRef] [Green Version]
- Napier, S.S.; Speight, P.M. Natural history of potentially malignant oral lesions and conditions: An overview of the literature. J. Oral Pathol. Med. 2008, 37, 1–10. [Google Scholar] [CrossRef]
- Epstein, J.B.; Güneri, P.; Boyacioglu, H.; Abt, E. The limitations of the clinical oral examination in detecting dysplastic oral lesions and oral squamous cell carcinoma. J. Am. Dent. Assoc. 2012, 143, 1332–1342. [Google Scholar] [CrossRef] [PubMed]
- Macey, R.; Walsh, T.; Brocklehurst, P.; Kerr, A.R.; Liu, J.L.; Lingen, M.W.; Ogden, G.R.; Warnakulasuriya, S.; Scully, C. Diagnostic tests for oral cancer and potentially malignant disorders in patients presenting with clinically evident lesions. Cochrane Database Syst. Rev. 2015, 2015, CD010276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, E.C.; Tan, M.T.; Schwarz, R.A.; Richards-Kortum, R.R.; Gillenwater, A.M.; Vigneswaran, N. Noninvasive diagnostic adjuncts for the evaluation of potentially premalignant oral epithelial lesions: Current limitations and future directions. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 670–681. [Google Scholar] [CrossRef]
- Patel, K.J.; De Silva, H.L.; Tong, D.C.; Love, R.M. Concordance between clinical and histopathologic diagnoses of oral mucosal lesions. J. Oral Maxillofac. Surg. 2011, 69, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Warnakulasuriya, S.; Pindborg, J.J. Reliability of oral precancer screening by primary health care workers in Sri Lanka. Commun. Dent. Health 1990, 7, 73–79. [Google Scholar]
- Nagao, T.; Ikeda, N.; Fukano, H.; Miyazaki, H.; Yano, M.; Warnakulasuriya, S. Outcome following a population screening programme for oral cancer and precancer in Japan. Oral Oncol. 2000, 36, 340–346. [Google Scholar] [CrossRef]
- Rashid, A.; Warnakulasuriya, S. The use of light-based (optical) detection systems as adjuncts in the detection of oral cancer and oral potentially malignant disorders: A systematic review. J. Oral Pathol. Med. 2015, 44, 307–328. [Google Scholar] [CrossRef]
- Nagi, R.; Reddy-Kantharaj, Y.B.; Rakesh, N.; Janardhan-Reddy, S.; Sahu, S. Efficacy of light based detection systems for early detection of oral cancer and oral potentially malignant disorders: Systematic review. Med. Oral Patol. Oral Cir. Bucal 2016, 21, e447–e455. [Google Scholar] [CrossRef]
- Awan, K.H.; Morgan, P.R.; Warnakulasuriya, S. Utility of chemiluminescence (ViziLite™) in the detection of oral potentially malignant disorders and benign keratoses. J. Oral Pathol. Med. 2011, 40, 541–544. [Google Scholar] [CrossRef]
- Vashisht, N.; Ravikiran, A.; Samatha, Y.; Rao, P.C.; Naik, R.; Vashisht, D. Chemiluminescence and toluidine blue as Diagnostic Tools for Detecting Early Stages of Oral Cancer: An in vivo Study. J. Clin. Diagn. Res. 2014, 8, ZC35–ZC38. [Google Scholar] [CrossRef]
- Kämmerer, P.W.; Rahimi-Nedjat, R.K.; Ziebart, T.; Bemsch, A.; Walter, C.; Al-Nawas, B.; Koch, F.P. A chemiluminescent light system in combination with toluidine blue to assess suspicious oral lesions-clinical evaluation and review of the literature. Clin. Oral Investig. 2015, 19, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Rajmohan, M.; Rao, U.K.; Joshua, E.; Rajasekaran, S.T.; Kannan, R. Assessment of oral mucosa in normal, precancer and cancer using chemiluminescent illumination, toluidine blue supravital staining and oral exfoliative cytology. J. Oral Maxillofac. Pathol. 2012, 16, 325–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farah, C.S.; McCullough, M.J. A pilot case control study on the efficacy of acetic acid wash and chemiluminescent illumination (ViziLite) in the visualisation of oral mucosal white lesions. Oral Oncol. 2007, 43, 820–824. [Google Scholar] [CrossRef]
- Chaudhry, A.; Manjunath, M.; Ashwatappa, D.; Krishna, S.; Krishna, A.G. Comparison of chemiluminescence and toluidine blue in the diagnosis of dysplasia in leukoplakia: A cross-sectional study. J. Investig. Clin. Dent. 2016, 7, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Shukla, A.; Singh, N.N.; Adsul, S.; Kumar, S.; Shukla, D.; Sood, A. Comparative efficacy of chemiluminescence and toluidine blue in the detection of potentially malignant and malignant disorders of the oral cavity. J. Oral Maxillofac. Pathol. 2018, 22, 442. [Google Scholar] [CrossRef]
- Lane, P.M.; Gilhuly, T.; Whitehead, P.; Zeng, H.; Poh, C.F.; Ng, S.; Williams, P.M.; Zhang, L.; Rosin, M.P.; MacAulay, C.E. Simple device for the direct visualization of oral-cavity tissue fluorescence. J. Biomed. Opt. 2006, 11, 024006. [Google Scholar] [CrossRef] [PubMed]
- Skala, M.; Ramanujam, N. Multiphoton redox ratio imaging for metabolic monitoring in vivo. Methods Mol. Biol. 2010, 594, 155–162. [Google Scholar]
- Van der Heiden, M.G.; Cantley, L.C.; Thompson, C.B. Understanding the Warburg effect: The metabolic requirements of cell proliferation. Science 2009, 324, 1029–1033. [Google Scholar] [CrossRef] [Green Version]
- Awan, K.H.; Morgan, P.R.; Warnakulasuriya, S. Evaluation of an autofluorescence based imaging system (VELscope™) in the detection of oral potentially malignant disorders and benign keratoses. Oral Oncol. 2011, 47, 274–277. [Google Scholar] [CrossRef]
- Hanken, H.; Kraatz, J.; Smeets, R.; Heiland, M.; Blessmann, M.; Eichhorn, W.; Clauditz, T.S.; Gröbe, A.; Kolk, A.; Rana, M. The detection of oral pre- malignant lesions with an autofluorescence based imaging system (VELscope™)—A single blinded clinical evaluation. Head Face Med. 2013, 9, 23. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, N.; Kawaguchi, K.; Fujihara, H.; Hasebe, M.; Kishi, Y.; Yasukawa, M.; Kumagai, K.; Hamada, Y. Detection accuracy for epithelial dysplasia using an objective autofluorescence visualization method based on the luminance ratio. Int. J. Oral Sci. 2017, 9, e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farah, C.S.; McIntosh, L.; Georgiou, A.; McCullough, M.J. Efficacy of tissue autofluorescence imaging (VELScope) in the visualization of oral mucosal lesions. Head Neck 2012, 34, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Rana, M.; Zapf, A.; Kuehle, M.; Gellrich, N.C.; Eckardt, A.M. Clinical evaluation of an autofluorescence diagnostic device for oral cancer detection: A prospective randomized diagnostic study. Eur. J. Cancer Prev. 2012, 21, 460–466. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.T.; Huang, J.S.; Wang, Y.Y.; Chen, K.C.; Wong, T.Y.; Chen, Y.C.; Wu, C.W.; Chan, L.P.; Lin, Y.C.; Kao, Y.H.; et al. Novel quantitative analysis of autofluorescence images for oral cancer screening. Oral Oncol. 2017, 68, 20–26. [Google Scholar] [CrossRef]
- Leunig, A.; Rick, K.; Stepp, H.; Goetz, A.; Baumgartner, R.; Feyh, J. Photodynamic diagnosis of neoplasms of the mouth cavity after local administration of 5-aminolevulinic acid. Laryngorhinootologie 1996, 75, 459–464. [Google Scholar] [CrossRef]
- Leunig, A.; Rick, K.; Stepp, H.; Gutmann, R.; Alwin, G.; Baumgartner, R.; Feyh, J. Fluorescence imaging and spectroscopy of 5-aminolevulinic acid induced protoporphyrin IX for the detection of neoplastic lesions in the oral cavity. Am. J. Surg. 1996, 172, 674–677. [Google Scholar] [CrossRef]
- Leunig, A.; Betz, C.S.; Mehlmann, M.; Stepp, H.; Arbogast, S.; Grevers, G.; Baumgartner, R. Detection of squamous cell carcinoma of the oral cavity by imaging 5-aminolevulinic acid-induced protoporphyrin IX fluorescence. Laryngoscope 2000, 110, 78–83. [Google Scholar] [CrossRef]
- Leunig, A.; Mehlmann, M.; Betz, C.; Stepp, H.; Arbogast, S.; Grevers, G.; Baumgartner, R. Fluorescence staining of oral cancer using a topical application of 5-aminolevulinic acid: Fluorescence microscopic studies. J. Photochem. Photobiol. B Biol. 2001, 60, 44–49. [Google Scholar] [CrossRef]
- Betz, C.S.; Stepp, H.; Janda, P.; Arbogast, S.; Grevers, G.; Baumgartner, R.; Leunig, A. A comparative study of normal inspection, autofluorescence and 5-ALA-induced PPIX fluorescence for oral cancer diagnosis. Int. J. Cancer 2002, 97, 245–252. [Google Scholar] [CrossRef]
- Zheng, W.; Soo, K.C.; Sivanandan, R.; Olivo, M. Detection of neoplasms in the oral cavity by digitized endoscopic imaging of 5-aminolevulinic acid-induced protoporphyrin IX fluorescence. Int. J. Oncol. 2002, 21, 763–768. [Google Scholar] [CrossRef]
- Zheng, W.; Soo, K.C.; Sivanandan, R.; Olivo, M. Detection of squamous cell carcinomas and pre-cancerous lesions in the oral cavity by quantification of 5-aminolevulinic acid induced fluorescence endoscopic images. Lasers Surg. Med. 2002, 31, 151–157. [Google Scholar] [CrossRef]
- Zheng, W.; Olivo, M.; Soo, K.C. The use of digitized endoscopic imaging of 5-ALA-induced PPIX fluorescence to detect and diagnose oral premalignant and malignant lesions in vivo. Int. J. Cancer 2004, 110, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Sharwani, A.; Jerjes, W.; Salih, V.; MacRobert, A.J.; El-Maaytah, M.; Khalil, H.S.; Hopper, C. Fluorescence spectroscopy combined with 5-aminolevulinic acid-induced protoporphyrin IX fluorescence in detecting oral premalignancy. J. Photochem. Photobiol. B Biol. 2006, 83, 27–33. [Google Scholar] [CrossRef]
- Green, B.; Cobb, A.R.; Brennan, P.A.; Hopper, C. Optical diagnostic techniques for use in lesions of the head and neck: Review of the latest developments. Br. J. Oral Maxillofac. Surg. 2014, 52, 675–680. [Google Scholar] [CrossRef]
- Moore, C.; Mehta, V.; Ma, X.; Chaudhery, S.; Shi, R.; Moore-Medlin, T.; Lian, T.; Nathan, C.A. Interobserver agreement of confocal laser endomicroscopy for detection of head and neck neoplasia. Laryngoscope 2016, 126, 632–637. [Google Scholar] [CrossRef] [PubMed]
- Jeng, M.J.; Sharma, M.; Sharma, L.; Chao, T.Y.; Huang, S.F.; Chang, L.B.; Wu, S.L.; Chow, L. Raman spectroscopy analysis for optical diagnosis of oral cancer detection. J. Clin. Med. 2019, 27, 1313. [Google Scholar] [CrossRef] [PubMed]
- Leonard, J.R.; Beck, W.L. Hematoporphyrin fluorescence: An aid in diagnosis of malignant neoplasms. Laryngoscope 1971, 81, 365–372. [Google Scholar] [CrossRef]
- Baskaran, R.; Lee, J.; Yang, S.G. Clinical development of photodynamic agents and therapeutic applications. Biomater. Res. 2018, 26, 22–25. [Google Scholar] [CrossRef]
- Castano, A.P.; Demidova, T.N.; Hamblin, M.R. Mechanisms in photodynamic therapy: Part three-Photosensitizer pharmacokinetics, biodistribution, tumor localization and modes of tumor destruction. Photodiagnosis Photodyn. Ther. 2005, 2, 91–106. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, J.C.; Pottier, R.H.; Pross, D.C. Photodynamic therapy with endogenous protoporphyrin IX: Basic principles and present clinical experience. J. Photochem. Photobiol. B Biol. 1990, 6, 143–148. [Google Scholar] [CrossRef]
- Peng, Q.; Moan, J.; Warloe, T.; Nesland, J.M.; Rimington, C. Distribution and photosensitizing efficiency of porphyrins induced by application of exogenous 5-aminolevulinic acid in mice bearing mammary carcinoma. Int. J. Cancer 1992, 52, 433–443. [Google Scholar] [CrossRef] [PubMed]
- Ishizuka, M.; Abe, F.; Sano, Y.; Takahashi, K.; Inoue, K.; Nakajima, M.; Kohda, T.; Komatsu, N.; Ogura, S.; Tanaka, T. Novel development of 5-aminolevurinic acid (ALA) in cancer diagnoses and therapy. Int. Immunopharmacol. 2011, 11, 358–365. [Google Scholar] [CrossRef]
- Yang, X.; Palasuberniam, P.; Kraus, D.; Chen, B. Aminolevulinic acid-based tumor detection and therapy: Molecular mechanisms and strategies for enhancement. Int. J. Mol. Sci. 2015, 16, 25865–25880. [Google Scholar] [CrossRef] [Green Version]
- Kitajima, Y.; Ishii, T.; Kohda, T.; Ishizuka, M.; Yamazaki, K.; Nishimura, Y.; Tanaka, T.; Dan, S.; Nakajima, M. Mechanistic study of PpIX accumulation using the JFCR39 cell panel revealed a role for dynamin 2-mediated exocytosis. Sci. Rep. 2019, 9, 8666. [Google Scholar] [CrossRef] [Green Version]
- Casas, A. Clinical uses of 5-aminolaevulinic acid in photodynamic treatment and photodetection of cancer: A review. Cancer Lett. 2020, 490, 165–173. [Google Scholar] [CrossRef]
- Ramanujam, N. Fluorescence spectroscopy of neoplastic and non-neoplastic tissues. Neoplasia 2000, 2, 89–117. [Google Scholar] [CrossRef] [Green Version]
- Webber, J.; Kessel, D.; Fromm, D. Side effects and photosensitization of human tissues after aminolevulinic acid. J. Surg. Res. 1997, 68, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Kamp, M.A.; Fischer, I.; Bühner, J.; Tyrowski, B.; Cornelius, J.F.; Steiger, H.-J.; Rapp, M.; Slotty, P.J.; Sabel, M. 5-ALA fluorescence of cerebral metastases and its impact for the local-in-brain progression. Oncotarget 2016, 7, 66776–66789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warnakulasuriya, S.; Reibel, J.; Bouquot, J.; Dabelsteen, E. Oral epithelial dysplasia classification systems: Predictive value, utility, weaknesses and scope for improvement. J. Oral Pathol. Med. 2008, 37, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Dost, F.; Lê Cao, K.; Ford, P.J.; Ades, C.; Farah, C.S. Malignant transformation of oral epithelial dysplasia: A real-world evaluation of histopathologic grading. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 117, 343–352. [Google Scholar] [CrossRef] [Green Version]
- Kujan, O.; Oliver, R.J.; Khattab, A.; Roberts, S.A.; Thakker, N.; Sloan, P. Evaluation of a new binary system of grading oral epithelial dysplasia for prediction of malignant transformation. Oral Oncol. 2006, 42, 987–993. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Bao, Z.X.; Shi, L.J.; Tang, G.Y.; Zhou, Z.T. Malignant transformation of oral epithelial dysplasia: Clinicopathological risk factors and outcome analysis in a retrospective cohort of 138 cases. Histopathology 2011, 59, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Nankivell, P.P.; Williams, H.; Matthews, P.P.; Suortamo, S.; Snead, D.; McConkey, C.; Mehanna, H. The binary oral dysplasia grading system: Validity testing and suggested improvement. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Fukuhara, H.; Yamamoto, S.; Karashima, T.; Inoue, K. Photodynamic diagnosis and therapy for urothelial carcinoma and prostate cancer: New imaging technology and therapy. Int. J. Clin. Oncol. 2020. Epub ahead of print. [Google Scholar] [CrossRef]
- Messmann, H.; Knüchel, R.; Bäumler, W.; Holstege, A.; Schölmerich, J. Endoscopic fluorescence detection of dysplasia in patients with Barrett’s esophagus, ulcerative colitis, or adenomatous polyps after 5-aminolevulinic acid-induced protoporphyrin IX sensitization. Gastrointest Endosc. 1999, 49, 97–101. [Google Scholar] [CrossRef]
- Kraft, M.; Betz, C.S.; Leunig, A.; Arens, C. Value of fluorescence endoscopy for the early diagnosis of laryngeal cancer and its precursor lesions. Head Neck 2011, 33, 941–948. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author | Malignant Transformation Rate (%) | Follow up Period (Years) | |||
|---|---|---|---|---|---|
| Initial Histopathological Diagnosis | |||||
| Severe | Moderate | Mild | No Dysplasia | ||
| Mehanna HM (7) | 24.1 | 10.3 (Moderate + Mild) | 0.5–16 | ||
| Warnakulasuriya S (9) | 26.7 | 15.7 | 4.8 | - | 10 |
| 5.6 (annual) | 1.8 (annual) | 0.3 (annual) | |||
| Speradio M (8) | 39.0 | 18.0 | 6.0 | 0.012 | 5–15 |
| Author | Subject | Case | Oral Rinse Time (m) | Incubation Time (h) | PDD System | Sensitivity (%) | Specificity (%) |
|---|---|---|---|---|---|---|---|
| Leunig 1996 | Oral squamous cell carcinoma | 16 | 15 | 1–2 | Endoscope type | - | - |
| Leunig 1996 | Neoplastic lesion | 11 | 15 | 1–2 | Endoscope type | - | - |
| Leunig 2000 | Suspicious oral cancer | 58 | 15 | 1–2.5 | Endoscope type | 99 | 60 |
| for detection of OSCC, CIS, severe and moderate dysplasia | |||||||
| Betz 2002 | Suspicious or malignant Oral and oropharynx lesion | 58 | 15 | 1–2 | Endoscope type Spectroscopy | 100 | 51.3 |
| Zheng 2002 | Premalignant or malignant lesion | 16 | 15 | 1–2 | Endoscope type | - | - |
| Fluorescence qualification | Discrimination between malignant lesions and benign tissues | ||||||
| Zheng 2002 | Premalignant or malignant lesion | 70 | 15 | 1–2 | Endoscope type | 95 | 97 |
| Fluorescence qualification | Discrimination between malignant lesions and benign tissues | ||||||
| Zheng 2004 | Suspicious Premalignant or malignant lesion | 118 | 15 | 1.5–2 | Endoscope type Fluorescence qualification | 92 | 96 |
| for dysplasia | |||||||
| 98 | 96 | ||||||
| for cancer | |||||||
| Good differentiation between the different stages of dysplasia and cancer | |||||||
| Sharwani 2006 | Suspicious oral leukoplakia | 71 | 15 | 1–2 | Endoscope type Fluorescence qualification | 83–90.3 | 79–89.5 |
| for dysplasia or CIS | |||||||
| Discrimination between normal and dysplastic lesions | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tatehara, S.; Satomura, K. Non-Invasive Diagnostic System Based on Light for Detecting Early-Stage Oral Cancer and High-Risk Precancerous Lesions—Potential for Dentistry. Cancers 2020, 12, 3185. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12113185
Tatehara S, Satomura K. Non-Invasive Diagnostic System Based on Light for Detecting Early-Stage Oral Cancer and High-Risk Precancerous Lesions—Potential for Dentistry. Cancers. 2020; 12(11):3185. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12113185
Chicago/Turabian StyleTatehara, Seiko, and Kazuhito Satomura. 2020. "Non-Invasive Diagnostic System Based on Light for Detecting Early-Stage Oral Cancer and High-Risk Precancerous Lesions—Potential for Dentistry" Cancers 12, no. 11: 3185. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12113185