Mitotic and Proliferative Indices in WHO Grade III Meningioma

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
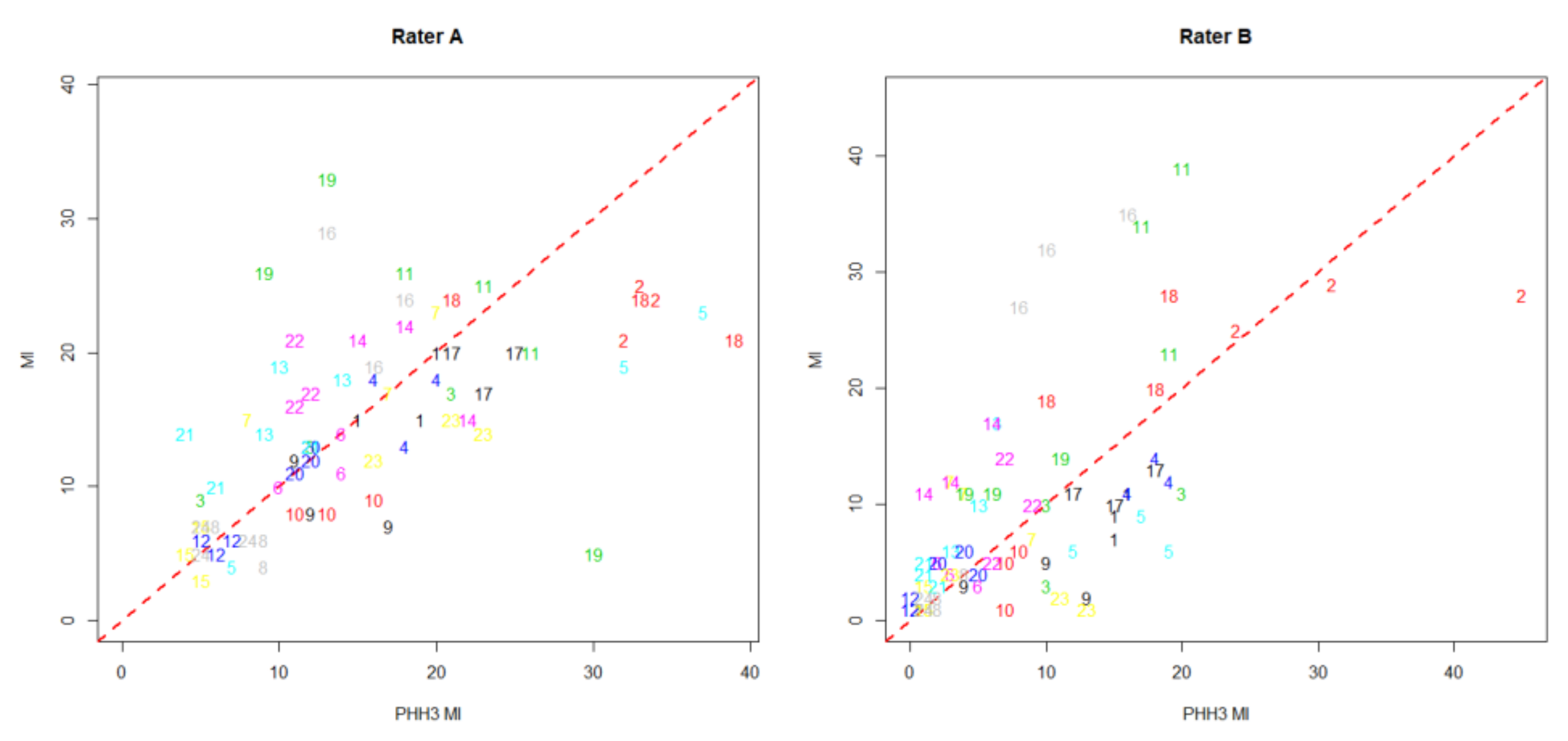
2.1. Repeatability and Agreement of Conventional MI and PHH3 MI
2.2. Association of Mitotic and Proliferative Markers and Progression-Free Survival
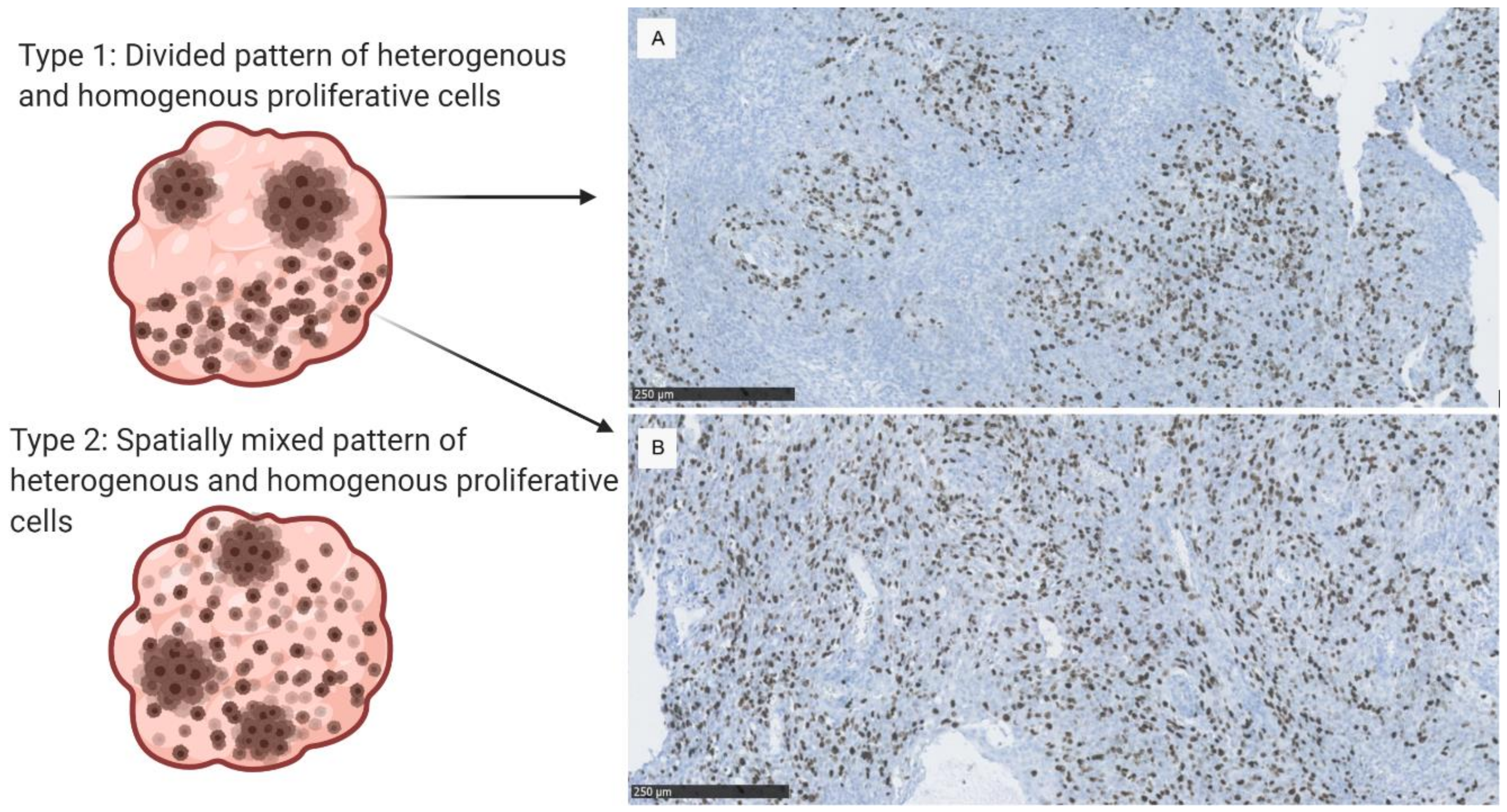
2.3. Proliferative Patterns and Mitotic Indices in Malignant Meningioma
3. Discussion
3.1. Repeatability and Agreement in Quantification of Mitotic Indices
3.2. Association of Mitotic and Proliferative Indices and Progression-Free Survival in WHO Grade III Meningioma
3.3. Study Limitations
4. Materials and Methods
4.1. Patient Data and Clinical Parameters
4.2. Histological Features, WHO-Grading and Mitotic Index
4.3. Immunohistochemistry
4.4. Assessment of Hot Spot and Overall Tumor Staining
4.5. Statistical Analysis
4.6. Ethical Approval
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Yuzawa, S.; Nishihara, H.; Tanaka, S. Genetic landscape of meningioma. Brain Tumor Pathol. 2016, 33, 237–247. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.; Ohgaki, H.; Wiestler, O.; Cavenee, W. WHO Classification of Tumours of the Central Nervous System, 4th ed.; International Agency for Research on Cancer, World Health Organization: Lyon, France, 2016. [Google Scholar]
- Duregon, E.; Cassenti, A.; Pittaro, A.; Ventura, L.; Senetta, R.; Rudà, R.; Cassoni, P. Better see to better agree: Phosphohistone H3 increases interobserver agreement in mitotic count for meningioma grading and imposes new specific thresholds. Neuro Oncol. 2015, 17, 663–669. [Google Scholar] [CrossRef] [Green Version]
- Hendzel, M.J.; Wei, Y.; Mancini, M.A.; Van Hooser, A.; Ranalli, T.; Brinkley, B.R.; Bazett-Jones, D.P.; Allis, C.D. Mitosis-specific phosphorylation of histone H3 initiates primarily within pericentromeric heterochromatin during G2 and spreads in an ordered fashion coincident with mitotic chromosome condensation. Chromosoma 1997, 106, 348–360. [Google Scholar] [CrossRef] [PubMed]
- Winther, T.L.; Arnli, M.B.; Salvesen, Ø.; Torp, S.H. Phosphohistone-H3 proliferation index is superior to mitotic index and MIB-1 expression as a predictor of recurrence in human meningiomas. Am. J. Clin. Pathol. 2016, 146, 510–520. [Google Scholar] [CrossRef] [PubMed]
- Olar, A.; Wani, K.M.; Sulman, E.P.; Mansouri, A.; Zadeh, G.; Wilson, C.D.; Demonte, F.; Fuller, G.N.; Aldape, K.D. Mitotic index is an independent predictor of recurrence-free survival in meningioma. Brain Pathol. 2015, 25, 266–275. [Google Scholar] [CrossRef] [Green Version]
- Ribalta, T.; McCutcheon, I.E.; Aldape, K.D.; Bruner, J.M.; Fuller, G.N. The mitosis-specific antibody anti-phosphohistone-H3 (PHH3) facilitates rapid reliable grading of meningiomas according to WHO 2000 criteria. Am. J. Surg. Pathol. 2004, 28, 1532–1536. [Google Scholar] [CrossRef]
- Abry, E.; Thomassen, I.T.; Salvesen, Ø.O.; Torp, S.H. The significance of Ki-67/MIB-1 labeling index in human meningiomas: A literature study. Pathol. Res. Pract. 2010, 206, 810–815. [Google Scholar] [CrossRef]
- Pham, D.T.; Skaland, I.; Winther, T.L.; Salvesen, Ø.; Torp, S.H. Correlation Between Digital and Manual Determinations of Ki-67/MIB-1 Proliferative Indices in Human Meningiomas. Int. J. Surg. Pathol. 2020, 28, 273–279. [Google Scholar] [CrossRef]
- Swiderska, Z.; Korzynska, A.; Markiewicz, T.; Lorent, M.; Zak, J.; Wesolowska, A.; Roszkowiak, L.; Slodkowska, J.; Grala, B. Comparison of the Manual, Semiautomatic, and Automatic Selection and Leveling of Hot Spots in Whole Slide Images for Ki-67 Quantification in Meningiomas. Anal. Cell. Pathol. 2015, 2015. [Google Scholar] [CrossRef] [Green Version]
- Swiderska, Z.; Markiewicz, T.; Grala, B.; Slodkowska, J. Hot-spot selection and evaluation methods for whole slice images of meningiomas and oligodendrogliomas. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; IEEE: New York, NY, USA, 2015; Volume 2015, pp. 6252–6256. [Google Scholar] [CrossRef]
- Swiderska-Chadaj, Z.; Markiewicz, T.; Grala, B.; Lorent, M. Content-based analysis of Ki-67 stained meningioma specimens for automatic hot-spot selection. Diagn. Pathol. 2016, 11, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Focke, C.M.; Decker, T.; van Diest, P.J. Intratumoral heterogeneity of Ki67 expression in early breast cancers exceeds variability between individual tumours. Histopathology 2016, 69, 849–861. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, Y.; Nakamura, Y.; Shibahara, Y.; Konosu-Fukaya, S.; Sato, N.; Kubota-Nakayama, F.; Oki, Y.; Baba, S.; Midorikawa, S.; Morimoto, R.; et al. Comparison of the methods for measuring the Ki-67 labeling index in adrenocortical carcinoma: Manual versus digital image analysis. Hum. Pathol. 2016, 53, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, P.S.; Riber-Hansen, R.; Jensen, T.O.; Schmidt, H.; Steiniche, T. Proliferation indices of phosphohistone H3 and Ki67: Strong prognostic markers in a consecutive cohort with stage I/II melanoma. Mod. Pathol. 2013, 26, 404–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirian, C.; Skyrman, S.; Bartek, J.; Jensen, L.R.; Kihlström, L.; Förander, P.; Orrego, A.; Mathiesen, T. The Ki-67 Proliferation Index as a Marker of Time to Recurrence in Intracranial Meningioma. Neurosurgery 2020, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Maier, A.D.; Bartek, J.; Eriksson, F.; Ugleholdt, H.; Juhler, M.; Broholm, H.; Mathiesen, T.I. Clinical and histopathological predictors of outcome in malignant meningioma. Neurosurg. Rev. 2019. [Google Scholar] [CrossRef]
- Angi, M.; Damato, B.; Kalirai, H.; Dodson, A.; Taktak, A.; Coupland, S.E. Immunohistochemical assessment of mitotic count in uveal melanoma. Acta Ophthalmol. 2011, 89, 155–160. [Google Scholar] [CrossRef]
- Altman, D.G.; Bland, J.M. Measurement in Medicine: The Analysis of Method Comparison Studies. J. R. Stat. Soc. Ser. D 1983, 32, 307–317. [Google Scholar] [CrossRef]
- Berchtold, A. Test-retest: Agreement or reliability? Methodol. Innov. 2016, 9. [Google Scholar] [CrossRef] [Green Version]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.M.; Altman, D.G. Agreement between methods of measurement with multiple observations per individual. J. Biopharm. Stat. 2007, 17, 571–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donhuijsen, K. Mitosis counts: Reproducibility and significance in grading of malignancy. Hum. Pathol. 1986, 17, 1122–1125. [Google Scholar] [CrossRef]
- Juratli, T.A.; Thiede, C.; Koerner, M.V.A.; Tummala, S.S.; Daubner, D.; Shankar, G.M.; Williams, E.A.; Martinez-Lage, M.; Soucek, S.; Robel, K.; et al. Intratumoral heterogeneity and TERT promoter mutations in progressive/higher-grade meningiomas. Oncotarget 2017, 8, 109228–109237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maier, A.D.; Stenman, A.; Svahn, F.; Mirian, C.; Bartek, J., Jr.; Juhler, M.; Zedenius, J.; Broholm, H.; Mathiesen, T. TERT promoter mutations in primary and secondary WHO grade III meningioma. Brain Pathol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Harmancı, A.S.; Youngblood, M.W.; Clark, V.E.; Coşkun, S.; Henegariu, O.; Duran, D.; Erson-Omay, E.Z.; Kaulen, L.D.; Lee, T.I.; Abraham, B.J.; et al. Integrated genomic analyses of de novo pathways underlying atypical meningiomas. Nat. Commun. 2017, 8. [Google Scholar] [CrossRef]
- Patel, A.J.; Wan, Y.W.; Al-Ouran, R.; Revelli, J.P.; Cardenas, M.F.; Oneissi, M.; Xi, L.; Jalali, A.; Magnotti, J.F.; Muzny, D.M.; et al. Molecular profiling predicts meningioma recurrence and reveals loss of DREAM complex repression in aggressive tumors. Proc. Natl. Acad. Sci. USA 2019, 116, 21715–21726. [Google Scholar] [CrossRef] [Green Version]
- Stålhammar, G.; Robertson, S.; Wedlund, L.; Lippert, M.; Rantalainen, M.; Bergh, J.; Hartman, J. Digital image analysis of Ki67 in hot spots is superior to both manual Ki67 and mitotic counts in breast cancer. Histopathology 2018, 72, 974–989. [Google Scholar] [CrossRef]
- Sahm, F.; Schrimpf, D.; Stichel, D.; Jones, D.T.W.; Hielscher, T.; Schefzyk, S.; Okonechnikov, K.; Koelsche, C.; Reuss, D.E.; Capper, D.; et al. DNA methylation-based classification and grading system for meningioma: A multicentre, retrospective analysis. Lancet Oncol. 2017, 18, 682–694. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Repeatability (Limits of Internal Agreement (95% CI) of the Ratio of Measurements) | ||||
| Rater A | MI | 63–173% | PHH3 MI | 64–178% |
| Rater B | MI | 72–256% | PHH3 MI | 70–229% |
| Agreement between Methods (Limits of Agreement, Ratio between MI and PHH3 MI) | ||||
| Rater A | 64–192% | |||
| Rater B | 85–454% | |||
| Overall Staining in Relation to PFS | No. of Patients | HR (95% CI) | p-Value |
| Mitoses in 10 HPF (MI) | 24 | 1.08 (1.01–1.15) | 0.0221 * |
| PHH3 mitoses in 10 HPF (PHH3 MI) | 24 | 1.09 (1.03–1.15) | 0.0032 * |
| Ki-67 overall expression < 10% | 9 | 1.00 | |
| Ki-67 overall expression > 10% | 15 | 5.40 (1.79–16.27) | 0.0028 * |
| Hot Spot Staining in Relation to PFS | No. of Patients | HR (95% CI) | p-Value |
| Max. no. mitoses in 1 HPF | 24 | 1.61 (1.12–2.31) | 0.0103 * |
| Max. no. PHH3 mitoses in 1 HPF | 24 | 1.59 (1.15–2.21) | 0.0056 * |
| Max. no. Ki-67 positive nuclei/100 nuclei | 24 | 1.06 (1.02–1.11) | 0.0040 * |
| Continuous Counts | Median, All Types (Range) | Anaplastic n = 16 | Rhabdoid n = 4 | Papillary n = 4 | Kruskal-Wallis ꭓ2 p-Value |
|---|---|---|---|---|---|
| Mitosis overall/HPF 1 | 1.2 (0.3–2.8) | 1.4 | 0.6 | 0.7 | 0.049 * |
| Mitosis hotspot/HPF 2 | 2.8 (1.2–6.2) | 3.4 | 1.8 | 1.9 | 0.034 * |
| PHH3 overall/HPF 1 | 1.1 (0.3–3.3) | 1.3 | 0.7 | 0.8 | 0.184 |
| PHH3 hotspot/HPF 2 | 3.0 (1.0–6.3) | 3.3 | 2.3 | 2.3 | 0.263 |
| Ki-67 hot spot/100 cells 4 | 31% (8–52%) | 34% | 18% | 18% | 0.035 * |
| Overall Ki-67 Categories | 1–10% | 10–25% | 25–50% | >50% | |
| No. of samples (% of total) 3 | 9 (38%) | 7 (29%) | 6 (25%) | 2 (8%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Daniela Maier, A.; Brøchner, C.B.; Bartek Jr., J.; Eriksson, F.; Ugleholdt, H.; Broholm, H.; Mathiesen, T. Mitotic and Proliferative Indices in WHO Grade III Meningioma. Cancers 2020, 12, 3351. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12113351
Daniela Maier A, Brøchner CB, Bartek Jr. J, Eriksson F, Ugleholdt H, Broholm H, Mathiesen T. Mitotic and Proliferative Indices in WHO Grade III Meningioma. Cancers. 2020; 12(11):3351. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12113351
Chicago/Turabian StyleDaniela Maier, Andrea, Christian Beltoft Brøchner, Jiri Bartek Jr., Frank Eriksson, Heidi Ugleholdt, Helle Broholm, and Tiit Mathiesen. 2020. "Mitotic and Proliferative Indices in WHO Grade III Meningioma" Cancers 12, no. 11: 3351. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12113351