Robotic Liver Resection Versus Percutaneous Ablation for Early HCC: Short- and Long-Term Results

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Background
2. Results
2.1. Patient and HCC Characteristics
2.2. Procedure Characteristics
2.3. Short-Term Outcomes
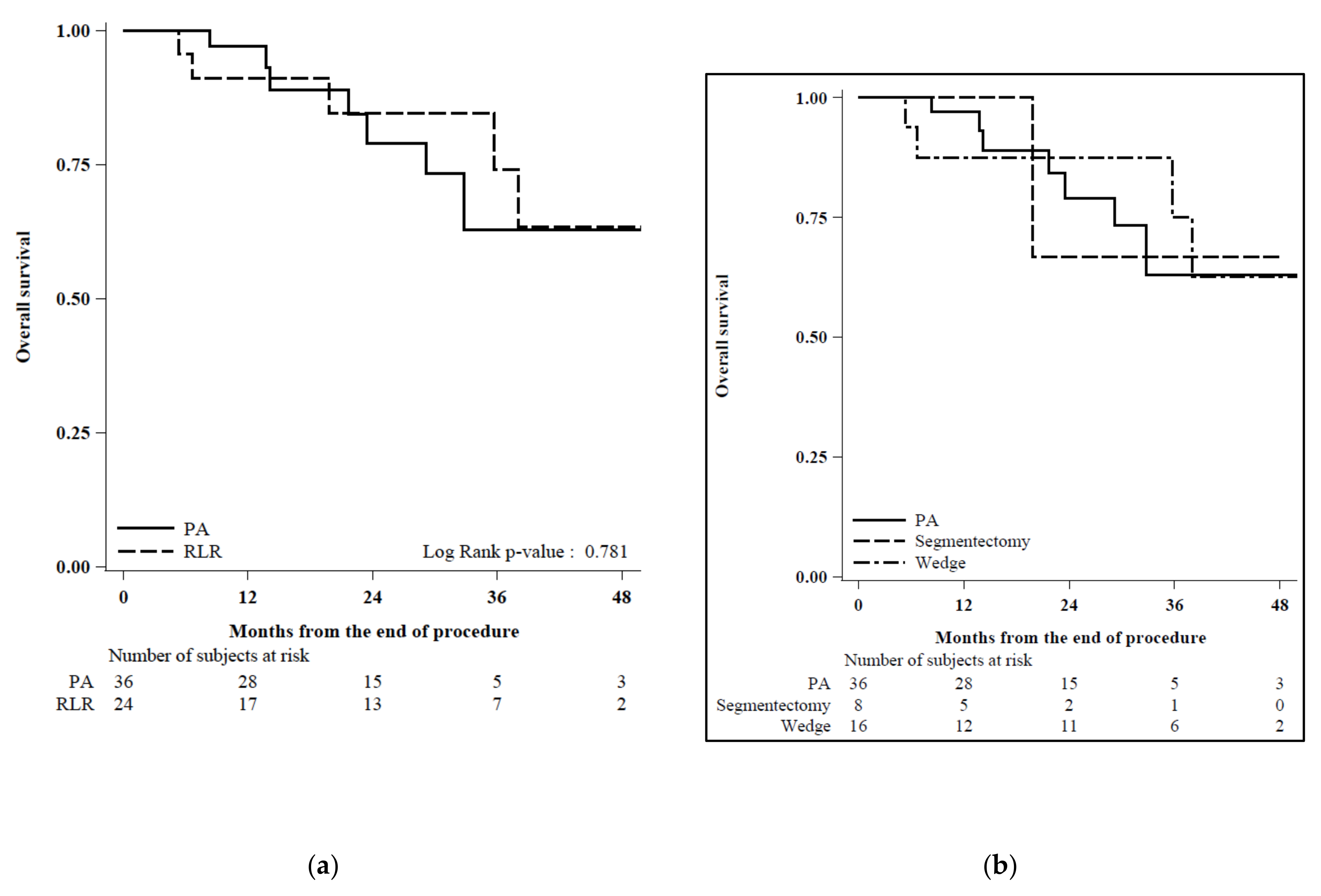
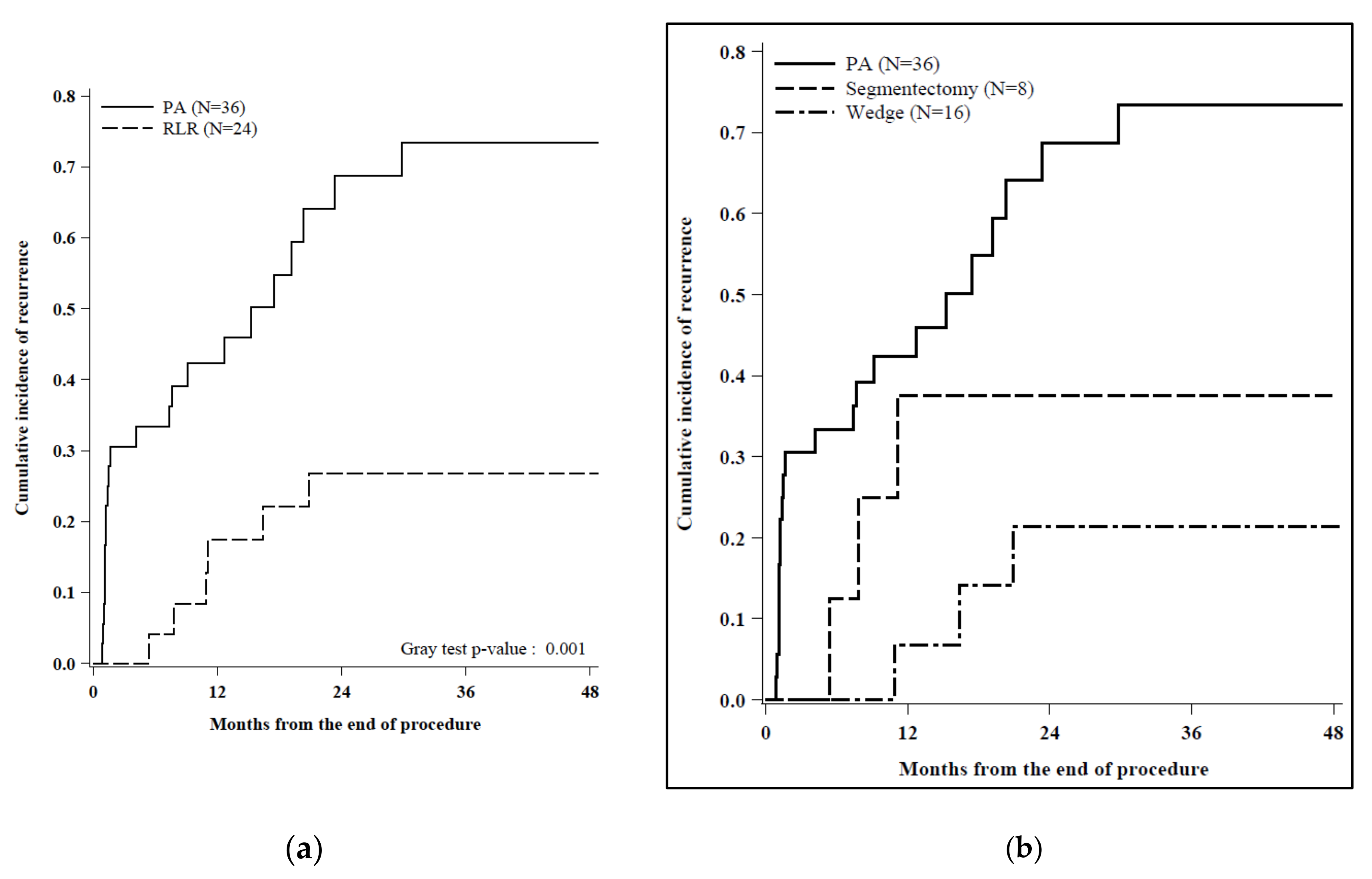
2.4. HCC Recurrence and Survival
3. Discussion
4. Material and Methods
4.1. Study Design
4.2. Variables and Definitions
4.3. Statistical Analysis
4.4. Robotic Liver Resection
4.5. Percutaneous Ablation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Disclaimers
References
- European Association for the Study of the Liver. Electronic address: [email protected]; European Association for the Study of the Liver EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vitali, G.C.; Laurent, A.; Terraz, S.; Majno, P.; Buchs, N.C.; Rubbia-Brandt, L.; Luciani, A.; Calderaro, J.; Morel, P.; Azoulay, D.; et al. Minimally invasive surgery versus percutaneous radio frequency ablation for the treatment of single small (≤3 cm) hepatocellular carcinoma: A case-control study. Surg. Endosc. 2016, 30, 2301–2307. [Google Scholar] [CrossRef] [PubMed]
- Groeschl, R.T.; Gamblin, T.C.; Turaga, K.K. Ablation for Hepatocellular Carcinoma: Validating the 3-cm Breakpoint. Ann. Surg. Oncol. 2013, 20, 3591–3595. [Google Scholar] [CrossRef] [PubMed]
- Di Sandro, S.; Benuzzi, L.; Lauterio, A.; Botta, F.; De Carlis, R.; Najjar, M.; Centonze, L.; Danieli, M.; Pezzoli, I.; Rampoldi, A.; et al. Single Hepatocellular Carcinoma approached by curative-intent treatment: A propensity score analysis comparing radiofrequency ablation and liver resection. Eur. J. Surg. Oncol. 2019, 45, 1691–1699. [Google Scholar] [CrossRef] [PubMed]
- Ciria, R.; Cherqui, D.; Geller, D.A.; Briceno, J.; Wakabayashi, G. Comparative Short-term Benefits of Laparoscopic Liver Resection: 9000 Cases and Climbing. Ann. Surg. 2016, 263, 761–777. [Google Scholar] [CrossRef]
- Rahbari, N.N.; Garden, O.J.; Padbury, R.; Brooke-Smith, M.; Crawford, M.; Adam, R.; Koch, M.; Makuuchi, M.; Dematteo, R.P.; Christophi, C.; et al. Posthepatectomy liver failure: A definition and grading by the International Study Group of Liver Surgery (ISGLS). Surgery 2011, 149, 713–724. [Google Scholar] [CrossRef]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases: Marrero et al. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [Green Version]
- Karabulut, K.; Aucejo, F.; Akyildiz, H.Y.; Siperstein, A.; Berber, E. Resection and radiofrequency ablation in the treatment of hepatocellular carcinoma: A single-center experience. Surg. Endosc. 2012, 26, 990–997. [Google Scholar] [CrossRef] [PubMed]
- Livraghi, T.; Meloni, F.; Stasi, M.D.; Rolle, E.; Solbiati, L.; Tinelli, C.; Rossi, S. Sustained complete response and complications rates after radiofrequency ablation of very early hepatocellular carcinoma in cirrhosis: Is resection still the treatment of choice? Hepatology 2008, 47, 82–89. [Google Scholar] [CrossRef]
- Liu, P.H.; Hsu, C.Y.; Hsia, C.Y.; Lee, Y.H.; Huang, Y.H.; Chiou, Y.Y.; Lin, H.C.; Huo, T.I. Surgical Resection Versus Radiofrequency Ablation for Single Hepatocellular Carcinoma ≤ 2 cm in a Propensity Score Model. Ann. Surg. 2016, 263, 538–545. [Google Scholar] [CrossRef]
- Sposito, C.; Battiston, C.; Facciorusso, A.; Mazzola, M.; Muscarà, C.; Scotti, M.; Romito, R.; Mariani, L.; Mazzaferro, V. Propensity score analysis of outcomes following laparoscopic or open liver resection for hepatocellular carcinoma. Br. J. Surg. 2016, 103, 871–880. [Google Scholar] [CrossRef] [PubMed]
- Cucchetti, A.; Mazzaferro, V.; Pinna, A.D.; Sposito, C.; Golfieri, R.; Serra, C.; Spreafico, C.; Piscaglia, F.; Cappelli, A.; Bongini, M.; et al. Average treatment effect of hepatic resection versus locoregional therapies for hepatocellular carcinoma. Br. J. Surg. 2017, 104, 1704–1712. [Google Scholar] [CrossRef] [PubMed]
- Di Sandro, S.; Bagnardi, V.; Najjar, M.; Buscemi, V.; Lauterio, A.; De Carlis, R.; Danieli, M.; Pinotti, E.; Benuzzi, L.; De Carlis, L. Minor laparoscopic liver resection for Hepatocellular Carcinoma is safer than minor open resection, especially for less compensated cirrhotic patients: Propensity score analysis. Surg. Oncol. 2018, 27, 722–729. [Google Scholar] [CrossRef] [PubMed]
- Lim, C.; Osseis, M.; Lahat, E.; Doussot, A.; Sotirov, D.; Hemery, F.; Lantéri-Minet, M.; Feray, C.; Salloum, C.; Azoulay, D. Safety of laparoscopic hepatectomy in patients with hepatocellular carcinoma and portal hypertension: Interim analysis of an open prospective study. Surg. Endosc. 2019, 33, 811–820. [Google Scholar] [CrossRef]
- Di Benedetto, F.; Petrowsky, H.; Magistri, P.; Halazun, K.J. Robotic liver resection: Hurdles and beyond. Int. J. Surg. 2020. [Google Scholar] [CrossRef]
- Ban, D.; Tanabe, M.; Ito, H.; Otsuka, Y.; Nitta, H.; Abe, Y.; Hasegawa, Y.; Katagiri, T.; Takagi, C.; Itano, O.; et al. A novel difficulty scoring system for laparoscopic liver resection. J. Hepatobiliary Pancreat. Sci. 2014, 21, 745–753. [Google Scholar] [CrossRef]
- Di Benedetto, F.; Tarantino, G.; Magistri, P. Chasing the Right Path: Tips, Tricks and Challenges of Robotic Approach to Posterior Segments. Hepatobiliary Surg. Nutr. 2019, 8, 512–514. [Google Scholar] [CrossRef]
- Magistri, P.; Guerrini, G.P.; Ballarin, R.; Assirati, G.; Tarantino, G.; Di Benedetto, F. Improving Outcomes Defending Patient Safety: The Learning Journey in Robotic Liver Resections. Biomed. Res. Int. 2019, 2019, 1835085. [Google Scholar] [CrossRef] [Green Version]
- Chen, P.D.; Wu, C.Y.; Hu, R.H.; Chen, C.N.; Yuan, R.H.; Liang, J.T.; Lai, H.S.; Wu, Y.M. Robotic major hepatectomy: Is there a learning curve? Surgery 2017, 161, 642–649. [Google Scholar] [CrossRef]
- Magistri, P.; Pecchi, A.; Franceschini, E.; Pesi, B.; Guadagni, S.; Catellani, B.; Assirati, G.; Guidetti, C.; Guerrini, G.P.; Tarantino, G.; et al. Not just minor resections: Robotic approach for cystic echinococcosis of the liver. Infection 2019, 47, 973–979. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE Initiative The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Magistri, P.; Tarantino, G.; Guidetti, C.; Assirati, G.; Olivieri, T.; Ballarin, R.; Coratti, A.; Di Benedetto, F. Laparoscopic versus robotic surgery for hepatocellular carcinoma: The first 46 consecutive cases. J. Surg. Res. 2017, 217, 92–99. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Level | PA (N = 36) | RLR (N = 24) | p-Value 1 |
|---|---|---|---|---|
| Age (years), median (min–max) | 67 (20–87) | 64 (48–79) | 0.52 | |
| Age (years), N (%) | <75 | 25 (69) | 21 (88) | 0.13 |
| ≥75 | 11 (31) | 3 (13) | ||
| Sex, N (%) | Male | 26 (72) | 16 (67) | 0.78 |
| Female | 10 (28) | 8 (33) | ||
| BMI (Kg/m2), median (min–max) | 28.12 (17.82–38.20) | 27.25 (19.82–33.03) | 0.67 | |
| BMI (Kg/m2), N (%) | Underweight | 1 (4) | 0 (0) | 0.90 |
| Normal | 6 (26) | 7 (29) | ||
| Overweight | 8 (35) | 10 (42) | ||
| Obese | 8 (35) | 7 (29) | ||
| Missing | 13 | 0 | ||
| ASA, N (%) | I | 4 (11) | 0 (0) | 0.13 |
| II | 10 (28) | 11 (46) | ||
| III | 22 (61) | 13 (54) | ||
| CCI score, median (min–max) | 7 (2–10) | 7 (3–9) | 0.62 | |
| Previous abdominal surgeries, N (%) | No | 19 (53) | 14 (58) | 0.79 |
| Yes | 17 (47) | 10 (42) | ||
| Hypertension, N (%) | No | 20 (56) | 8 (33) | 0.12 |
| Yes | 16 (44) | 16 (67) | ||
| Diabetes, N (%) | No | 28 (78) | 20 (83) | 0.75 |
| Yes | 8 (22) | 4 (17) | ||
| Renal failure, N (%) | No | 36 (100) | 22 (92) | 0.16 |
| Yes | 0 (0) | 2 (8) | ||
| Liver cirrhosis, N (%) | No | 15 (42) | 6 (25) | 0.27 |
| Yes | 21 (58) | 18 (75) | ||
| Respiratory insufficiency, N (%) | No | 34 (94) | 23 (96) | 1.00 |
| Yes | 2 (6) | 1 (4) | ||
| Cardiovascular disease, N (%) | No | 29 (81) | 21 (88) | 0.73 |
| Yes | 7 (19) | 3 (13) | ||
| Hepatopathy, N (%) | HCV | 20 (56) | 12 (50) | 0.60 |
| HBV | 8 (22) | 6 (25) | ||
| Alcohol | 3 (8) | 2 (8) | ||
| NASH | 4 (11) | 1 (4) | ||
| HCV+HBV | 1 (3) | 1 (4) | ||
| CBP | 0 (0) | 2 (8) | ||
| HIV coinfection, N (%) | No | 35 (97) | 21 (88) | 0.29 |
| Yes | 1 (3) | 3 (13) |
| Variable | Level | PA (N = 36) | RLR (N = 24) | p-Value 1 |
|---|---|---|---|---|
| Ishak fibrosis score, N (%) | F0 (none to moderate fibrosis) | 14 (39) | 6 (25) | 0.40 |
| F1 (severe fibrosis or cirrhosis) | 22 (61) | 18 (75) | ||
| Portal hypertension, N (%) | No | 13 (36) | 10 (42) | 0.79 |
| Yes | 23 (64) | 14 (58) | ||
| Esophageal varices, N (%) | No | 14 (39) | 13 (54) | 0.30 |
| Yes | 22 (61) | 11 (46) | ||
| PLT (migl/mmc), N (%) | <100.000 | 22 (61) | 9 (38) | 0.11 |
| ≥100.000 | 14 (39) | 15 (63) | ||
| Bilirubin (mg/dl), N (%) | ≤1 | 17 (47) | 19 (79) | 0.017 |
| >1 | 19 (53) | 5 (21) | ||
| Creatinine (mg/dl), N (%) | ≤1.4 | 36 (100) | 23 (96) | 0.40 |
| >1.4 | 0 (0) | 1 (4) | ||
| Albumin (g/dl), N (%) | <3.5 | 10 (28) | 4 (17) | 0.37 |
| ≥3.5 | 26 (72) | 20 (83) | ||
| INR, N (%) | ≤1.25 | 19 (53) | 18 (75) | 0.11 |
| >1.25 | 17 (47) | 6 (25) | ||
| AFP (ng/mL.), median (min–max) | 6.1 (1.5–497.9) | 4.3 (1.2–1063.0) | 0.34 | |
| MELD score, median (min–max) | 9 (6–18) | 9 (6–17) | 0.38 | |
| CTP score, N (%) | A | 28 (78) | 19 (79) | 1.00 |
| B | 7 (19) | 5 (21) | ||
| C | 1 (3) | 0 (0) | ||
| ALBI score, N (%) | 1 | 9 (25) | 15 (63) | 0.012 |
| 2 | 21 (58) | 8 (33) | ||
| 3 | 6 (17) | 1 (4) | ||
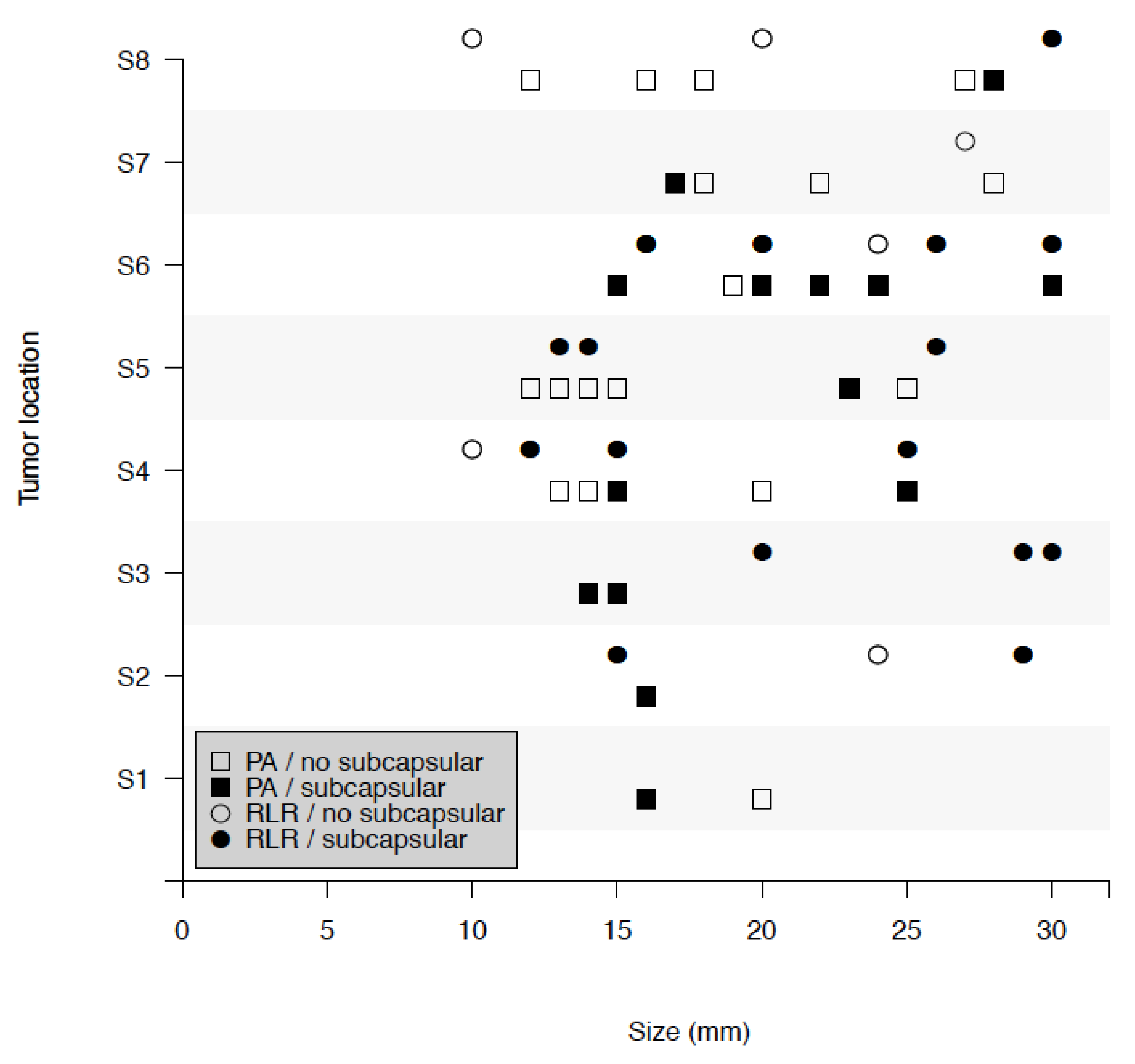
| Tumor size (mm), median (min-max) | 19.5 (12.0–30.0) | 20.0 (10.0–30.0) | 0.35 | |
| Tumor size (mm), N (%) | ≤20 | 24 (67) | 13 (54) | 0.42 |
| >20 | 12 (33) | 11 (46) | ||
| Subcapsular HCC, N (%) | No | 20 (56) | 6 (25) | 0.033 |
| Yes | 16 (44) | 18 (75) | ||
| Tumor location, N (%) | S1 | 2 (6) | 0 (0) | 0.25 2 |
| S2 | 1 (3) | 3 (13) | ||
| S3 | 2 (6) | 3 (13) | ||
| S4 | 6 (17) | 4 (17) | ||
| S5 | 7 (19) | 3 (13) | ||
| S6 | 8 (22) | 7 (29) | ||
| S7 | 4 (11) | 1 (4) | ||
| S8 | 6 (17) | 3 (13) | ||
| BCLC, N (%) | Stage 0 | 14 (39) | 8 (33) | 0.79 |
| Stage A | 22 (61) | 16 (67) |
| Variable | Level | PA (N = 36) | RLR (N = 24) | p-Value 1 |
|---|---|---|---|---|
| In-hospital stay (days), median (min–max) | 2 (1–6) | 4 (1–18) | <0.001 | |
| Max bilirubin (mg/dL), median (min–max) | 1.45 (0.33–9.88) | 1.41 (0.52–9.17) | 0.59 | |
| Max INR, median (min–max) | 1.29 (0.77–1.92) | 1.35 (1.07–2.11) | 0.12 | |
| Max creatinine (mg/dL), median (min–max) | 0.86 (0.59–1.29) | 0.79 (0.52–2.32) | 0.37 | |
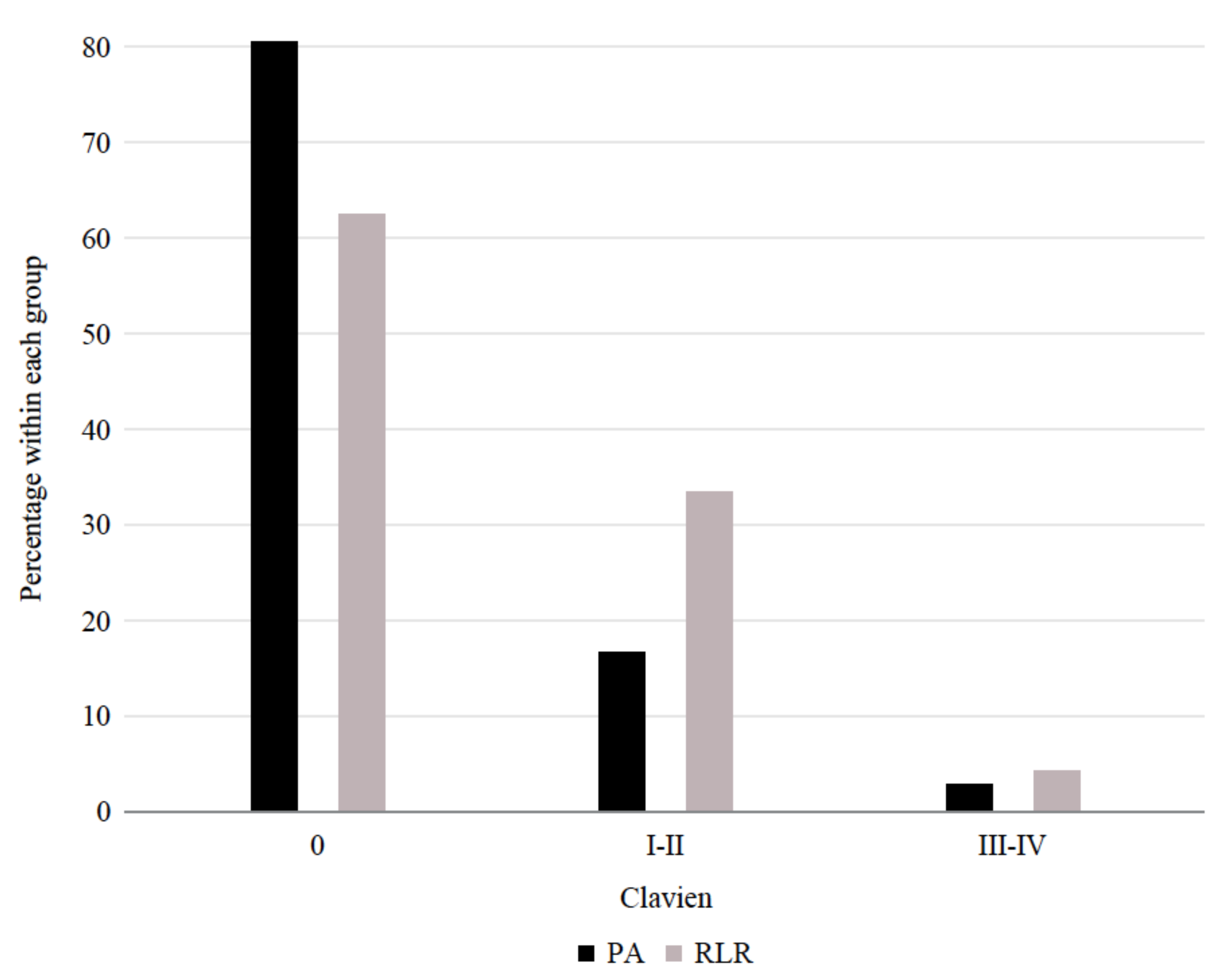
| Morbidity, N (%) 2 3 | Clavien 0 | 29 (81) | 15 (63) | 0.15 |
| Clavien > 0 | 7 (19) | 9 (38) | ||
| Clavien 0 | 29 (81) | 15 (63) | 0.34 | |
| Clavien I–II | 6 (17) | 8 (33) | ||
| Clavien III–IV | 1 (3) | 1 (4) | ||
| Liver failure, N (%) | No | 36 (100) | 23 (96) | 0.40 |
| Yes | 0 (0) | 1 (4) | ||
| Readmission within 30 days, N (%) | No | 34 (94) | 23 (96) | 1.00 |
| Yes | 2 (6) | 1 (4) |
| Variable | Level | PA (N = 36) | Segmentectomy (N = 8) | Wedge (N = 16) |
|---|---|---|---|---|
| In-hospital stay (days), median (min–max) | 2 (1–6) | 4 (1–5) | 4 (2–18) | |
| Max bilirubin (mg/dL), median (min–max) | 1.45 (0.33–9.88) | 1.97 (0.74–4.69) | 1.38 (0.52–9.17) | |
| Max INR, median (min–max) | 1.29 (0.77–1.92) | 1.29 (1.07–1.77) | 1.36 (1.14–2.11) | |
| Max creatinine (mg/dL), median (min–max) | 0.86 (0.59–1.29) | 0.87 (0.59–1.25) | 0.76 (0.52–2.32) | |
| Morbidity, N (%) | Clavien 0 | 29 (81) | 6 (75) | 9 (56) |
| Clavien > 0 | 7 (19) | 2 (25) | 7 (44) | |
| Clavien 0 | 29 (81) | 6 (75) | 9 (56) | |
| Clavien I and II | 6 (17) | 2 (25) | 6 (38) | |
| Clavien III and IV | 1 (3) | 0 (0) | 1 (6) | |
| Liver failure, N (%) | No | 36 (100) | 8 (100) | 15 (94) |
| Yes | 0 (0) | 0 (0) | 1 (6) | |
| Readmission within 30 days, N (%) | No | 34 (94) | 8 (100) | 15 (94) |
| Yes | 2 (6) | 0 (0) | 1 (6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magistri, P.; Catellani, B.; Frassoni, S.; Guidetti, C.; Olivieri, T.; Assirati, G.; Caporali, C.; Pecchi, A.; Serra, V.; Ballarin, R.; et al. Robotic Liver Resection Versus Percutaneous Ablation for Early HCC: Short- and Long-Term Results. Cancers 2020, 12, 3578. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12123578
Magistri P, Catellani B, Frassoni S, Guidetti C, Olivieri T, Assirati G, Caporali C, Pecchi A, Serra V, Ballarin R, et al. Robotic Liver Resection Versus Percutaneous Ablation for Early HCC: Short- and Long-Term Results. Cancers. 2020; 12(12):3578. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12123578
Chicago/Turabian StyleMagistri, Paolo, Barbara Catellani, Samuele Frassoni, Cristiano Guidetti, Tiziana Olivieri, Giacomo Assirati, Cristian Caporali, Annarita Pecchi, Valentina Serra, Roberto Ballarin, and et al. 2020. "Robotic Liver Resection Versus Percutaneous Ablation for Early HCC: Short- and Long-Term Results" Cancers 12, no. 12: 3578. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12123578