Delayed Postoperative Hyponatremia Following Endoscopic Transsphenoidal Surgery for Non-Adenomatous Parasellar Tumors

 ,
,  , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Baseline Characteristics
2.2. Symptomatic and Serological DPH
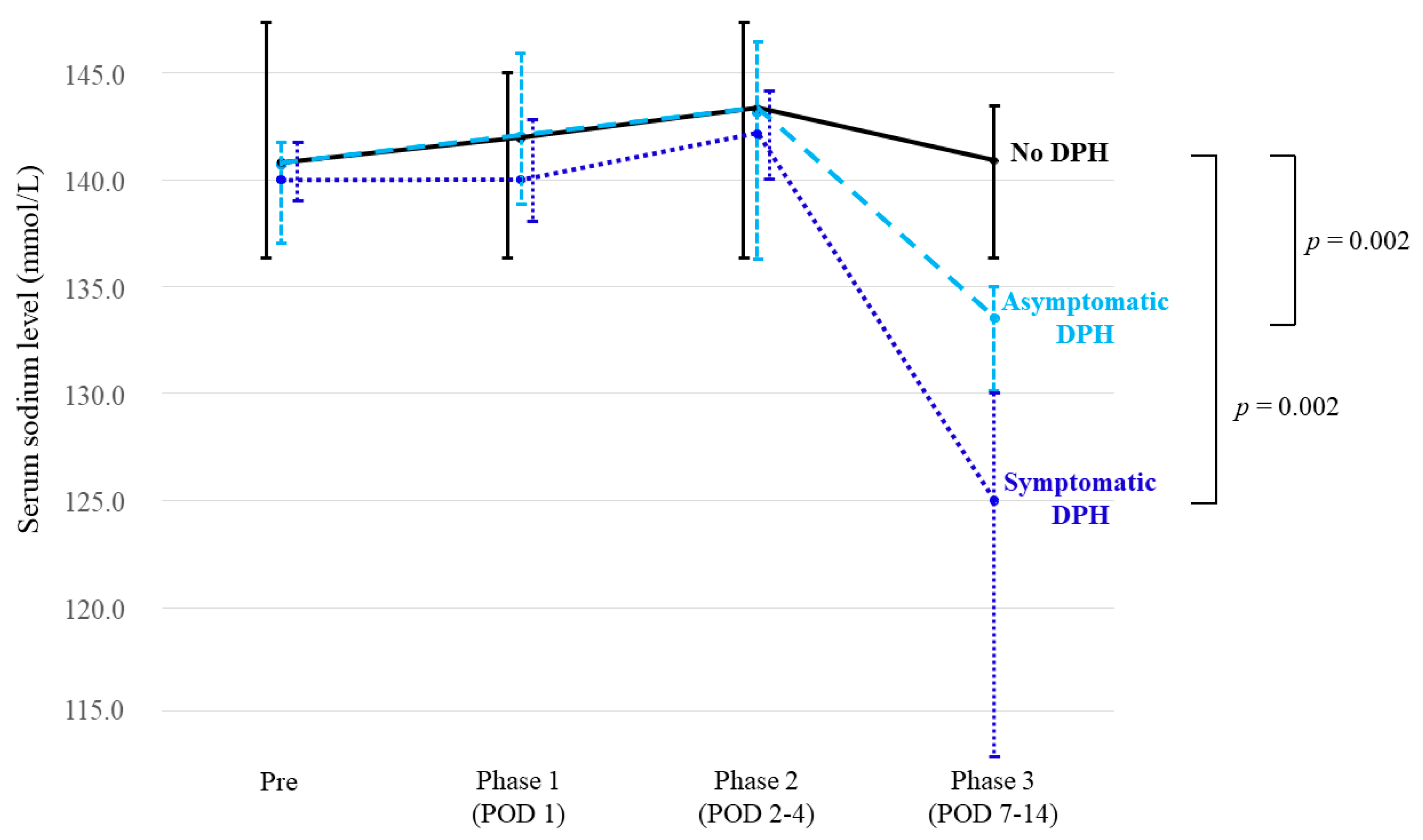
2.3. Detailed Course of Sodium Levels
2.4. Risk Factors Associated with DPH
2.5. Other Electrolytic and Endocrinological Abnormalities
3. Discussion
4. Materials and Methods
4.1. Patient Selection
4.2. Surgical Procedure
4.3. Postoperative Management
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Jho, H.D. Endoscopic transsphenoidal surgery. J. Neurooncol. 2001, 54, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Mortini, P.; Losa, M.; Barzaghi, R.; Boari, N.; Giovanelli, M. Results of transsphenoidal surgery in a large series of patients with pituitary adenoma. Neurosurgery 2005, 56, 1222–1233; discussion 1233. [Google Scholar] [CrossRef] [PubMed]
- Bohl, M.A.; Ahmad, S.; Jahnke, H.; Shepherd, D.; Knecht, L.; White, W.L.; Little, A.S. Delayed Hyponatremia Is the Most Common Cause of 30-Day Unplanned Readmission After Transsphenoidal Surgery for Pituitary Tumors. Neurosurgery 2016, 78, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Cote, D.J.; Alzarea, A.; Acosta, M.A.; Hulou, M.M.; Huang, K.T.; Almutairi, H.; Alharbi, A.; Zaidi, H.A.; Algrani, M.; Alatawi, A.; et al. Predictors and Rates of Delayed Symptomatic Hyponatremia after Transsphenoidal Surgery: A Systematic Review [corrected]. World Neurosurg. 2016, 88, 1–6. [Google Scholar] [CrossRef]
- Hensen, J.; Henig, A.; Fahlbusch, R.; Meyer, M.; Boehnert, M.; Buchfelder, M. Prevalence, predictors and patterns of postoperative polyuria and hyponatraemia in the immediate course after transsphenoidal surgery for pituitary adenomas. Clin. Endocrinol. 1999, 50, 431–439. [Google Scholar] [CrossRef]
- Jahangiri, A.; Wagner, J.; Tran, M.T.; Miller, L.M.; Tom, M.W.; Kunwar, S.; Blevins, L., Jr.; Aghi, M.K. Factors predicting postoperative hyponatremia and efficacy of hyponatremia management strategies after more than 1000 pituitary operations. J. Neurosurg. 2013, 119, 1478–1483. [Google Scholar] [CrossRef]
- Lee, J.I.; Cho, W.H.; Choi, B.K.; Cha, S.H.; Song, G.S.; Choi, C.H. Delayed hyponatremia following transsphenoidal surgery for pituitary adenoma. Neurol. Med. Chir. 2008, 48, 489–492; discussion 484–492. [Google Scholar] [CrossRef] [Green Version]
- Olson, B.R.; Gumowski, J.; Rubino, D.; Oldfield, E.H. Pathophysiology of hyponatremia after transsphenoidal pituitary surgery. J. Neurosurg. 1997, 87, 499–507. [Google Scholar] [CrossRef] [Green Version]
- Tomita, Y.; Kurozumi, K.; Inagaki, K.; Kameda, M.; Ishida, J.; Yasuhara, T.; Ichikawa, T.; Sonoda, T.; Otsuka, F.; Date, I. Delayed postoperative hyponatremia after endoscopic transsphenoidal surgery for pituitary adenoma. Acta Neurochir. 2019, 161, 707–715. [Google Scholar] [CrossRef]
- Zada, G.; Liu, C.Y.; Fishback, D.; Singer, P.A.; Weiss, M.H. Recognition and management of delayed hyponatremia following transsphenoidal pituitary surgery. J. Neurosurg. 2007, 106, 66–71. [Google Scholar] [CrossRef] [Green Version]
- Cerda-Esteve, M.; Cuadrado-Godia, E.; Chillaron, J.J.; Pont-Sunyer, C.; Cucurella, G.; Fernandez, M.; Goday, A.; Cano-Perez, J.F.; Rodriguez-Campello, A.; Roquer, J. Cerebral salt wasting syndrome: Review. Eur. J. Intern. Med. 2008, 19, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Fraser, J.F.; Stieg, P.E. Hyponatremia in the neurosurgical patient: Epidemiology, pathophysiology, diagnosis, and management. Neurosurgery 2006, 59, 222–229; discussion 222–229. [Google Scholar] [CrossRef] [PubMed]
- Harrigan, M.R. Cerebral salt wasting syndrome: A review. Neurosurgery 1996, 38, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Hussain, N.S.; Piper, M.; Ludlam, W.G.; Ludlam, W.H.; Fuller, C.J.; Mayberg, M.R. Delayed postoperative hyponatremia after transsphenoidal surgery: Prevalence and associated factors. J. Neurosurg. 2013, 119, 1453–1460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sata, A.; Hizuka, N.; Kawamata, T.; Hori, T.; Takano, K. Hyponatremia after transsphenoidal surgery for hypothalamo-pituitary tumors. Neuroendocrinology 2006, 83, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, Y.; Tominaga, A.; Arita, K.; Sugiyama, K.; Hanaya, R.; Hama, S.; Sakoguchi, T.; Usui, S.; Kurisu, K. Post-operative hyponatremia in patients with pituitary adenoma: Post-operative management with a uniform treatment protocol. Endocr. J. 2011, 58, 373–379. [Google Scholar] [CrossRef] [Green Version]
- Cole, C.D.; Gottfried, O.N.; Liu, J.K.; Couldwell, W.T. Hyponatremia in the neurosurgical patient: Diagnosis and management. Neurosurg. Focus 2004, 16, E9. [Google Scholar] [CrossRef]
- Guerrero, R.; Pumar, A.; Soto, A.; Pomares, M.A.; Palma, S.; Mangas, M.A.; Leal, A.; Villamil, F. Early hyponatraemia after pituitary surgery: Cerebral salt-wasting syndrome. Eur. J. Endocrinol. 2007, 156, 611–616. [Google Scholar] [CrossRef] [Green Version]
- Yee, A.H.; Burns, J.D.; Wijdicks, E.F. Cerebral salt wasting: Pathophysiology, diagnosis, and treatment. Neurosurg. Clin. N. Am. 2010, 21, 339–352. [Google Scholar] [CrossRef]
- d’Avella, E.; Angileri, F.; de Notaris, M.; Enseñat, J.; Stagno, V.; Cavallo, L.M.; Gonzales, J.B.; Weiss, A.; Prats-Galino, A. Extended endoscopic endonasal transclival approach to the ventrolateral brainstem and related cisternal spaces: Anatomical study. Neurosurg. Rev. 2014, 37, 253–260; discussion 260. [Google Scholar] [CrossRef]
- Hasegawa, H.; Shin, M.; Kondo, K.; Hanakita, S.; Mukasa, A.; Kin, T.; Saito, N. Role of endoscopic transnasal surgery for skull base chondrosarcoma: A retrospective analysis of 19 cases at a single institution. J. Neurosurg. 2018, 128, 1438–1447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.H.; Jeon, C.; Se, Y.B.; Hong, S.D.; Seol, H.J.; Lee, J.I.; Park, C.K.; Kim, D.G.; Jung, H.W.; Han, D.H.; et al. Clinical outcomes of an endoscopic transclival and transpetrosal approach for primary skull base malignancies involving the clivus. J. Neurosurg. 2018, 128, 1454–1462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulwin, C.; Schwartz, T.H.; Cohen-Gadol, A.A. Endoscopic extended transsphenoidal resection of tuberculum sellae meningiomas: Nuances of neurosurgical technique. Neurosurg. Focus 2013, 35, E6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.K.; Christiano, L.D.; Patel, S.K.; Tubbs, R.S.; Eloy, J.A. Surgical nuances for removal of tuberculum sellae meningiomas with optic canal involvement using the endoscopic endonasal extended transsphenoidal transplanum transtuberculum approach. Neurosurg. Focus 2011, 30, E2. [Google Scholar] [CrossRef]
- Saito, K.; Toda, M.; Tomita, T.; Ogawa, K.; Yoshida, K. Surgical results of an endoscopic endonasal approach for clival chordomas. Acta Neurochir. 2012, 154, 879–886. [Google Scholar] [CrossRef]
- Shin, M.; Kondo, K.; Hanakita, S.; Hasegawa, H.; Yoshino, M.; Teranishi, Y.; Kin, T.; Saito, N. Endoscopic transsphenoidal anterior petrosal approach for locally aggressive tumors involving the internal auditory canal, jugular fossa, and cavernous sinus. J. Neurosurg. 2017, 126, 212–221. [Google Scholar] [CrossRef] [Green Version]
- Shin, M.; Kondo, K.; Hanakita, S.; Suzukawa, K.; Kin, T.; Shojima, M.; Nakagawa, D.; Saito, N. Endoscopic transnasal approach for resection of locally aggressive tumors in the orbit. J. Neurosurg. 2015, 123, 748–759. [Google Scholar] [CrossRef] [Green Version]
- Zanation, A.M.; Snyderman, C.H.; Carrau, R.L.; Gardner, P.A.; Prevedello, D.M.; Kassam, A.B. Endoscopic endonasal surgery for petrous apex lesions. Laryngoscope 2009, 119, 19–25. [Google Scholar] [CrossRef]
- Antunes-Rodrigues, J.; de Castro, M.; Elias, L.L.; Valenca, M.M.; McCann, S.M. Neuroendocrine control of body fluid metabolism. Physiol. Rev. 2004, 84, 169–208. [Google Scholar] [CrossRef] [Green Version]
- Robertson, G.L. Antidiuretic hormone. Normal and disordered function. Endocrinol. Metab. Clin. N. Am. 2001, 30, 671–694. [Google Scholar] [CrossRef]
- Yamamoto, T.; Sasaki, S.; Fushimi, K.; Ishibashi, K.; Yaoita, E.; Kawasaki, K.; Marumo, F.; Kihara, I. Vasopressin increases AQP-CD water channel in apical membrane of collecting duct cells in Brattleboro rats. Am. J. Physiol. 1995, 268, C1546–C1551. [Google Scholar] [CrossRef] [PubMed]
- Kristof, R.A.; Rother, M.; Neuloh, G.; Klingmuller, D. Incidence, clinical manifestations, and course of water and electrolyte metabolism disturbances following transsphenoidal pituitary adenoma surgery: A prospective observational study. J. Neurosurg. 2009, 111, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Barber, S.M.; Liebelt, B.D.; Baskin, D.S. Incidence, Etiology and Outcomes of Hyponatremia after Transsphenoidal Surgery: Experience with 344 Consecutive Patients at a Single Tertiary Center. J. Clin. Med. 2014, 3, 1199–1219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antunes-Rodrigues, J.; Picanco-Diniz, D.W.; Favaretto, A.L.; Gutkowska, J.; McCann, S.M. Brain atrial natriuretic peptide neurons play an essential role in volume expansion-induced release of atrial natriuretic peptide and natriuresis. Neuroendocrinology 1993, 58, 696–700. [Google Scholar] [CrossRef]
- Favaretto, A.L.; Ballejo, G.O.; Albuquerque-Araujo, W.I.; Gutkowska, J.; Antunes-Rodrigues, J.; McCann, S.M. Oxytocin releases atrial natriuretic peptide from rat atria in vitro that exerts negative inotropic and chronotropic action. Peptides 1997, 18, 1377–1381. [Google Scholar] [CrossRef]
- Gutkowska, J.; Antunes-Rodrigues, J.; McCann, S.M. Atrial natriuretic peptide in brain and pituitary gland. Physiol. Rev. 1997, 77, 465–515. [Google Scholar] [CrossRef]
- Haanwinckel, M.A.; Elias, L.K.; Favaretto, A.L.; Gutkowska, J.; McCann, S.M.; Antunes-Rodrigues, J. Oxytocin mediates atrial natriuretic peptide release and natriuresis after volume expansion in the rat. Proc. Natl. Acad. Sci. USA 1995, 92, 7902–7906. [Google Scholar] [CrossRef] [Green Version]
- Li, C.; Wang, W.; Summer, S.N.; Westfall, T.D.; Brooks, D.P.; Falk, S.; Schrier, R.W. Molecular mechanisms of antidiuretic effect of oxytocin. J. Am. Soc. Nephrol. 2008, 19, 225–232. [Google Scholar] [CrossRef] [Green Version]
- Andrews, B.T.; Fitzgerald, P.A.; Tyrell, J.B.; Wilson, C.B. Cerebral salt wasting after pituitary exploration and biopsy: Case report. Neurosurgery 1986, 18, 469–471. [Google Scholar] [CrossRef]
- Sane, T.; Rantakari, K.; Poranen, A.; Tahtela, R.; Valimaki, M.; Pelkonen, R. Hyponatremia after transsphenoidal surgery for pituitary tumors. J. Clin. Endocrinol. Metab. 1994, 79, 1395–1398. [Google Scholar] [CrossRef]
- Singer, P.A.; Sevilla, L.J. Postoperative endocrine management of pituitary tumors. Neurosurg. Clin. N. Am. 2003, 14, 123–138. [Google Scholar] [CrossRef]
- Staiger, R.D.; Sarnthein, J.; Wiesli, P.; Schmid, C.; Bernays, R.L. Prognostic factors for impaired plasma sodium homeostasis after transsphenoidal surgery. Br. J. Neurosurg. 2013, 27, 63–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nemergut, E.C.; Zuo, Z.; Jane, J.A., Jr.; Laws, E.R., Jr. Predictors of diabetes insipidus after transsphenoidal surgery: A review of 881 patients. J. Neurosurg. 2005, 103, 448–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burke, W.T.; Cote, D.J.; Penn, D.L.; Iuliano, S.; McMillen, K.; Laws, E.R. Diabetes Insipidus After Endoscopic Transsphenoidal Surgery. Neurosurgery 2020, 87, 949–955. [Google Scholar] [CrossRef]
- Shin, M.; Kenji, K.; Suzukawa, K.; Saito, N. Endoscopic transnasal interseptal approach for invasive clival tumors: Development of an approach method regarding maximal preservation of the nasal anatomy. Neurol. Med. Chir. 2015, 55, 336–344. [Google Scholar] [CrossRef] [Green Version]
- Shin, M.; Kondo, K.; Saito, N. Neuroendoscopic transnasal surgery for skull base tumors: Basic approaches, avoidance of pitfalls, and recent innovations. Neurol. Med. Chir. 2012, 52, 697–703. [Google Scholar] [CrossRef] [Green Version]
- Haldane, J.B. The estimation and significance of the logarithm of a ratio of frequencies. Ann. Hum. Genet. 1956, 20, 309–311. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Value | |
|---|---|---|
| Median age, years (range) | 47 (19–85) | |
| Median preoperative sodium level, mmol/L (range) | 141 (136–148) | |
| Median tumor diameter, mm (range) | 31 (15–48) | |
| Male sex, n (%) | 12 (40) | |
| Comorbidity *, n (%) | ACTH-deficiency | 0 (0) |
| DM | 2 (6) | |
| HL | 3 (10) | |
| HTN | 7 (23) | |
| Pathological diagnosis, n (%) | Chordoma | 15 (50) |
| Meningioma | 8 (27) | |
| Chondrosarcoma | 5 (17) | |
| Neurenteric cyst | 1 (3) | |
| Neurinoma | 1 (3) | |
| Previous intervention, n (%) | Resection | 10 (32) |
| Radiotherapy | 5 (16) | |
| Location *, n (%) | Sellar region | 10 (33) |
| Cavernous sinus | 19 (63) | |
| Suprasellar region | 11 (37) | |
| Dorsum sellae | 19 (63) | |
| Sphenoid sinus | 3 (10) | |
| Petrous apex | 12 (40) | |
| Clivus | 22 (73) | |
| Anterior skull base | 4 (13) | |
| Posterior fossa (intradural) | 12 (40) | |
| Third ventricle | 0 (0) | |
| No. | Age, Sex | Dx | Main Location | Extradural Retraction * | Contact to Stalk | Serum Sodium Level (mmol/L) | Body Weight (kg) | Hematocrit (%) | Symptomatic Hyponatremia | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Phase 1 | Phase 2 | Phase 3 | Δ ** | Pre | Phase 3 | Δ% † | Phase 1 | Phase 3 | Δ% ‡ | |||||||
| 1 | 70, F | Mgm | Ptcl | Yes | No | 139 | 138 | 140 | 112 | −27 | 54.4 | 57.3 | 5.4 | 38.2 | 36.1 | −5.5 | Yes |
| 2 | 69, F | Cho | Cli | Yes | No | 140 | 143 | 144 | 123 | −17 | 51.0 | 49.2 | −3.6 | 26.2 | 27.1 | +3.4 | Yes |
| 3 | 38, F | Cho | Cli | Yes | No | 140 | 139 | 140 | 126 | −14 | 84.3 | 86.3 | 2.4 | 29.9 | 30.1 | +0.3 | Yes |
| 4 | 75, F | Mgm | ITF-Sph | Yes | No | 142 | 141 | 144 | 130 | −12 | 43.2 | 43 | −0.5 | 25.1 | 31.8 | +26.7 | Yes |
| 5 | 58, F | Mgm | TS | No | Yes | 141 | 146 | 147 | 130 | −11 | 53.1 | 57.2 | 7.7 | 29.5 | 25.4 | −13.9 | No |
| 6 | 55, F | Mgm | Ptcl | Yes | No | 142 | 139 | 142 | 134 | −8 | 60.2 | 57.7 | −4.2 | 26.3 | 24.7 | −6.1 | No |
| 7 | 59, M | Chs | PA-PF | Yes | No | 141 | 140 | 136 | 135 | −6 | 76.7 | 71.4 | −6.9 | 37.7 | 43.6 | +15.6 | No |
| 8 | 34, M | Cho | DS | Yes | No | 137 | 143 | 143 | 134 | −3 | 83.0 | 77.6 | −6.5 | 38.8 | 44.1 | +13.7 | No |
| Clinical Course | Median Serum Sodium Level (Range), mmol/L | |||
|---|---|---|---|---|
| Pre | Phase 1 | Phase 2 | Phase 3 | |
| No DPH | 141 | 142 | 143 | 141 |
| (136–148) | (136–145) | (136–148) | (136–143) | |
| Asymptomatic DPH | 141 | 142 | 143 | 134 |
| (137–142) | (139–146) | (136–147) | (130–135) | |
| Symptomatic DPH | 140 | 140 | 142 | 125 |
| (139–142) | (138–143) | (140–144) | (112–130) | |
| Variables | Symptomatic DPH | Serologic DPH | |||
|---|---|---|---|---|---|
| p Value | OR (95%CI) | p Value | OR (95%CI) | ||
| Age (cont.) | 0.098 | 0.94 (0.86–1.01) * | 0.124 | 0.96 (0.91–1.01) * | |
| Preoperative sodium level (cont.) | 0.749 | 1.09 (0.65–1.82) * | 0.624 | 1.10 (0.74–1.64) * | |
| Tumor diameter (cont.) | 0.206 | 0.93 (0.83–1.04) * | 0.413 | 0.97 (0.89–1.05) * | |
| Male sex | 0.120 | 0.13 (0.01–2.64) | 0.419 | 0.40 (0.07–2.44) | |
| Comorbidity | Diabetes mellitus | 1.000 | 1.09 (0.04–26.67) | 1.000 | 0.48 (0.02–11.14) |
| Hyperlipidemia | 0.454 | 2.88 (0.31–26.44) | 0.284 | 3.33 (0.38–28.96) | |
| Hypertension | 1.000 | 1.68 (0.20–14.09) | 0.645 | 1.50 (0.22–10.36) | |
| Previous intervention | Surgery | 0.270 | 0.15 (0.01–3.07) | 0.199 | 0.17 (0.02–1.64) |
| Radiotherapy | 0.557 | 0.35 (0.02–7.41) | 1.000 | 0.49 (0.05–4.94) | |
| Location | Sella | 0.095 | 8.14 (0.72–91.89) | 1.000 | 1.29 (0.24–6.96) |
| Cavernous sinus | 0.268 | 6.68 (0.33–136.79) | 1.000 | 0.95 (0.18–5.08) | |
| Suprasellar region | 1.000 | 0.53 (0.05–5.86) | 0.972 | 0.48 (0.08–2.95) | |
| Dorsum sellae | 0.268 | 6.68 (0.33–136.79) | 0.672 | 2.08 (0.34–12.72) | |
| Sphenoid sinus | 0.360 | 4.00 (0.27–58.56) | 0.166 | 7.00 (0.54–91.11) | |
| Petrous apex | 0.632 | 0.45 (0.04–4.98) | 1.000 | 0.87 (0.16–4.58) | |
| Clivus | 1.000 | 1.11 (0.10–12.47) | 1.000 | 1.13 (0.18–7.19) | |
| Anterior skull base | 1.000 | 0.56 (0.03–12.24) | 1.000 | 0.90 (0.08–10.21) | |
| Posterior fossa (intradural) | 0.130 | 0.13 (0.01–2.64) | 0.433 | 0.40 (0.07–2.44) | |
| Extradural retraction of the gland | 0.100 | 12.13 (0.59–248.50) | 0.035 ** | 12.25 (1.27–118.36) | |
| Physical contact with the stalk | 1.000 | 0.43 (0.02–9.34) | 1.000 | 0.64 (0.06–6.80) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hasegawa, H.; Shin, M.; Makita, N.; Shinya, Y.; Kondo, K.; Saito, N. Delayed Postoperative Hyponatremia Following Endoscopic Transsphenoidal Surgery for Non-Adenomatous Parasellar Tumors. Cancers 2020, 12, 3849. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12123849
Hasegawa H, Shin M, Makita N, Shinya Y, Kondo K, Saito N. Delayed Postoperative Hyponatremia Following Endoscopic Transsphenoidal Surgery for Non-Adenomatous Parasellar Tumors. Cancers. 2020; 12(12):3849. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12123849
Chicago/Turabian StyleHasegawa, Hirotaka, Masahiro Shin, Noriko Makita, Yuki Shinya, Kenji Kondo, and Nobuhito Saito. 2020. "Delayed Postoperative Hyponatremia Following Endoscopic Transsphenoidal Surgery for Non-Adenomatous Parasellar Tumors" Cancers 12, no. 12: 3849. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12123849