Obesity Epidemic—The Underestimated Risk of Endometrial Cancer



{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Adipose-Derived Pathophysiological Mechanisms Linking EC to Adiposity
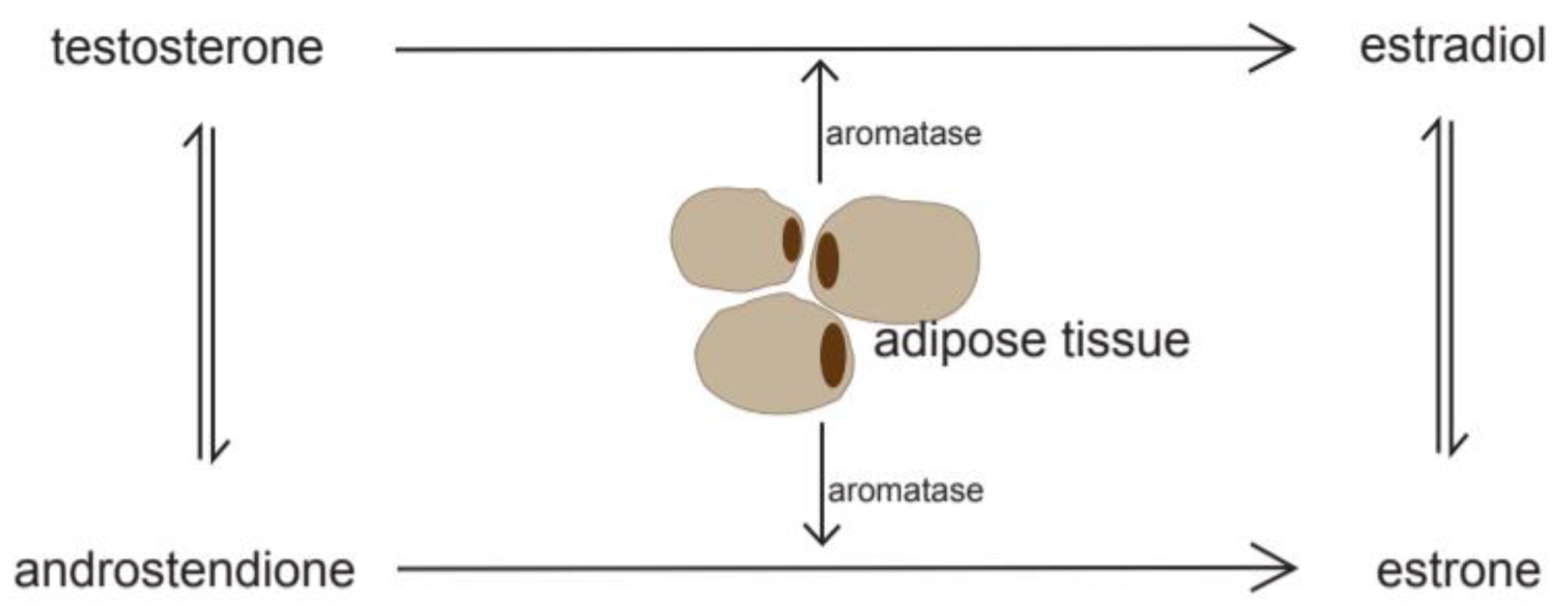
2.1. Estrogen-Driven Tumorigenesis
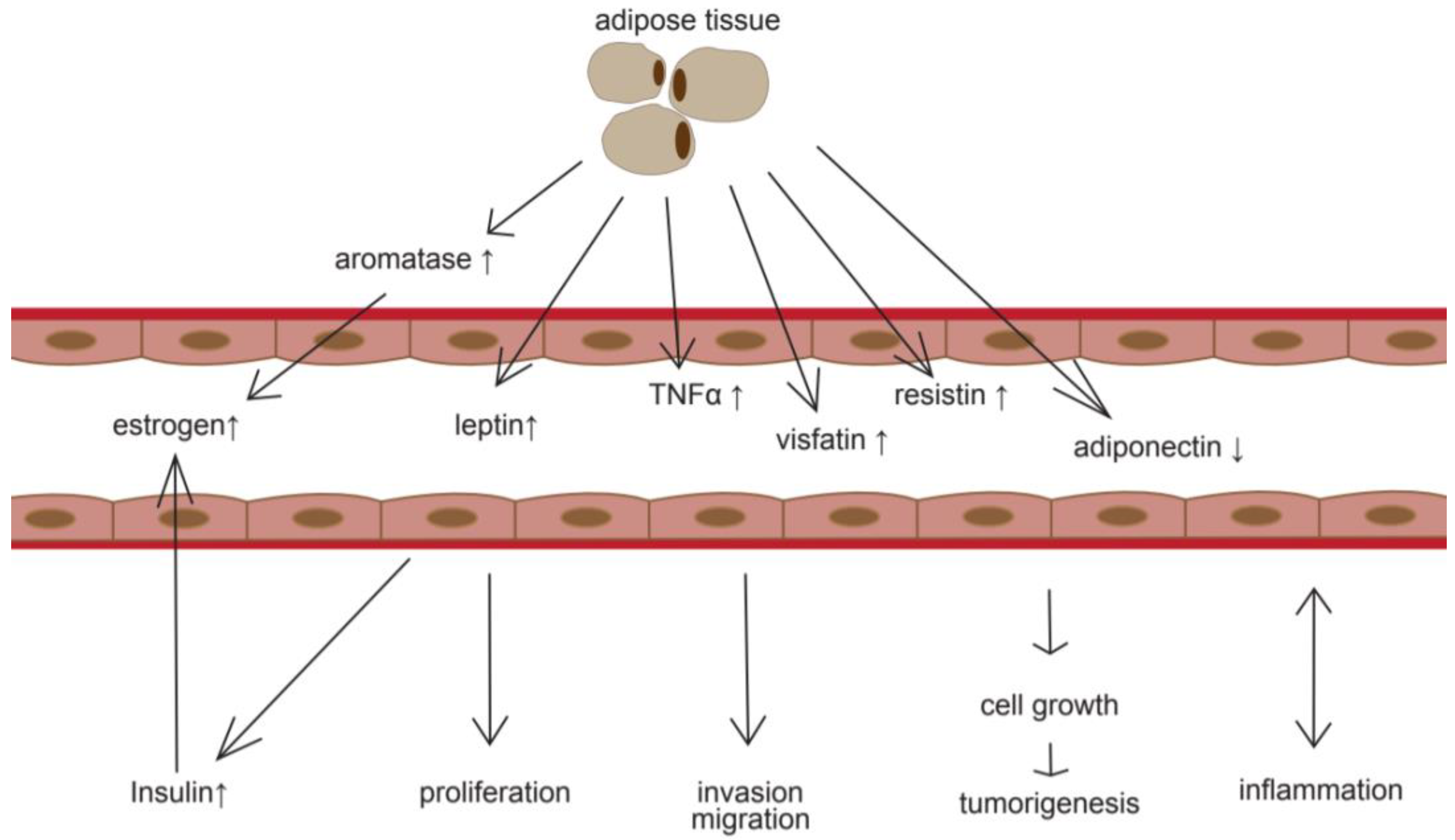
2.2. Adipose Tissue—An Endocrine Organ
2.3. The Link between Estrogen, Insulin Resistance, and Cancer
3. Clinical Management and Treatment
3.1. Metformin
3.2. Obesity and Its Consequences for Surgical Treatment
3.3. Possible Complications of Chemotherapy and Radiotherapy Due to Obesity
4. Weight Reduction and Its Value as Prevention Measure
4.1. Lifestyle
4.2. Bariatric Surgery
4.3. Implications of Weight Loss after Diagnosis of Endometrial Cancer
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- GBD 2015 Obesity Collaborators; Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; et al. Health effects of overweight and obesity in 195 countries over 25 years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar]
- Friedenreich, C.M.; Ryder-Burbidge, C.; McNeil, J. Physical activity, obesity and sedentary behavior in cancer etiology: Epidemiologic evidence and biologic mechanisms. Mol. Oncol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Haggerty, A.F.; Sarwer, D.B.; Schmitz, K.H.; Ko, E.M.; Allison, K.C.; Chu, C.S. Obesity and Endometrial Cancer: A Lack of Knowledge but Opportunity for Intervention. Nutr. Cancer 2017, 69, 990–995. [Google Scholar] [CrossRef] [PubMed]
- Reeves, G.K.; Pirie, K.; Beral, V.; Green, J.; Spencer, E.; Bull, D. Cancer incidence and mortality in relation to body mass index in the Million Women Study: Cohort study. BMJ 2007, 335, 1134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onstad, M.A.; Schmandt, R.E.; Lu, K.H. Addressing the Role of Obesity in Endometrial Cancer Risk, Prevention, and Treatment. J. Clin. Oncol. 2016, 34, 4225–4230. [Google Scholar] [CrossRef]
- World Cancer Research Fund/American Institute for Cancer Research: Continuous Update Project Report. Food: Nutrition, Physical Activity, and the Prevention of Endometrial Cancer. 2013. Available online: http://www.dietandcancerreport.org (accessed on 1 November 2020).
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Moore, K.; Brewer, M.A. Endometrial Cancer: Is This a New Disease? Am. Soc. Clin. Oncol. Educ. Book 2017, 37, 435–442. [Google Scholar] [CrossRef]
- Connor, E.V.; Raker, C.A.; Clark, M.A.; Stuckey, A.R. Obesity risk awareness in women with endometrial cancer. Arch. Gynecol. Obstet. 2017, 295, 965–969. [Google Scholar] [CrossRef]
- Simpson, E.R.; Mahendroo, M.S.; Means, G.D.; Kilgore, M.W.; Hinshelwood, M.M.; Graham-Lorence, S.; Amarneh, B.; Ito, Y.; Fisher, C.R.; Michael, M.D.; et al. Aromatase Cytochrome P450, The Enzyme Responsible for Estrogen. Biosynthesis. Endocr. Rev. 1994, 15, 342–355. [Google Scholar]
- Potischman, N.; Hoover, R.N.; Brinton, L.A.; Siiteri, P.; Dorgan, J.F.; Swanson, C.A.; Berman, M.L.; Mortel, R.; Twiggs, L.B.; Barrett, R.J.; et al. Case—Control Study of Endogenous Steroid Hormones and Endometrial Cancer. J. Natl. Cancer Inst. 1996, 88, 1127–1135. [Google Scholar] [CrossRef]
- Brinton, L.A.; Trabert, B.; Anderson, G.L.; Falk, R.T.; Felix, A.S.; Fuhrman, B.J.; Gass, M.L.; Kuller, L.H.; Pfeiffer, R.M.; Rohan, T.E.; et al. Serum Estrogens and Estrogen Metabolites and Endometrial Cancer Risk among Postmenopausal Women. Cancer Epidemiol. Biomark. Prev. 2016, 25, 1081–1089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedenreich, C.M.; Derksen, J.; Speidel, T.; Brenner, D.R.; Heer, E.; Courneya, K.S.; Cook, L.S. Case—control study of endogenous sex steroid hormones and risk of endometrial cancer. Cancer Causes Control 2020, 31, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Lukanova, A.; Lundin, E.; Micheli, A.; Arslan, A.; Ferrari, P.; Rinaldi, S.; Krogh, V.; Lenner, P.; Shore, R.E.; Biessy, C.; et al. Circulating levels of sex steroid hormones and risk of endometrial cancer in postmenopausal women. Int. J. Cancer 2004, 108, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, A.C.; Blanchard, Z.; Maurer, K.A.; Gertz, J. Estrogen Signaling in Endometrial Cancer: A Key Oncogenic Pathway with Several Open Questions. Horm. Cancer 2019, 10, 51–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hou, X.; Zhao, M.; Wang, T.; Zhang, G. Upregulation of estrogen receptor mediates migration, invasion and proliferation of endometrial carcinoma cells by regulating the PI3K/AKT/mTOR pathway. Oncol. Rep. 2014, 31, 1175–1182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, R.X.; Wei, L.H.; Tu, Z.; Sun, P.M.; Wang, J.L.; Zhao, D.; Li, X.P.; Tang, J.M. 17 beta-estradiol activates PI3K/Akt signaling pathway by estrogen receptor (ER)-dependent and ER-independent mechanisms in endometrial cancer cells. J. Steroid Biochem. Mol. Biol. 2006, 99, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Chen, R.; Liang, X.; Shi, J.; Wu, X.; Zhang, Z.; Chen, X. Estrogen Enhances Endometrial Cancer Cells Proliferation by Upregulation of Prohibitin. J. Cancer 2019, 10, 1616–1621. [Google Scholar] [CrossRef] [Green Version]
- Lurie, G.; Gaudet, M.M.; Spurdle, A.B.; Carney, M.E.; Wilkens, L.R.; Yang, H.P.; Weiss, N.S.; Webb, P.M.; Thompson, P.J.; Terada, K.; et al. The obesity-associated polymorphisms FTO rs9939609 and MC4R rs17782313 and endometrial cancer risk in non-Hispanic white women. PLoS ONE 2011, 6, e16756. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Zhou, D.; Lai, Y.; Liu, Y.; Tao, X.; Wang, Q.; Zhao, G.; Gu, H.; Liao, H.; Zhu, Y.; et al. Estrogen induces endometrial cancer cell proliferation and invasion by regulating the fat mass and obesity-associated gene via PI3K/AKT and MAPK signaling pathways. Cancer Lett. 2012, 319, 89–97. [Google Scholar] [CrossRef]
- Che, Q.; Xiao, X.; Xu, J.; Liu, M.; Lu, Y.; Liu, S.; Dong, X. 17β-Estradiol promotes endometrial cancer proliferation and invasion through IL-6 pathway. Endocr. Connect. 2019, 8, 961–968. [Google Scholar] [CrossRef] [Green Version]
- Prossnitz, E.R.; Barton, M. The G-protein-coupled estrogen receptor GPER in health and disease. Nat. Rev. Endocr. 2011, 7, 715–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dossus, L.; Lukanova, A.; Rinaldi, S.; Allen, N.; Cust, A.E.; Becker, S.; Tjonneland, A.; Hansen, L.; Overvad, K.; Chabbert-Buffet, N.; et al. Hormonal, metabolic, and inflammatory profiles and endometrial cancer risk within the EPIC cohort--a factor analysis. Am. J. Epidemiol. 2013, 177, 787–799. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Gao, S.; Sun, C.; Li, J.; Gao, W.; Yu, L. Clinical significance of serum adiponectin and visfatin levels in endometrial cancer. Int. J. Gynaecol. Obstet. 2019, 145, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Tian, W.; Zhu, Y.; Wang, Y.; Teng, F.; Zhang, H.; Liu, G.; Ma, X.; Sun, D.; Rohan, T.; Xue, F. Visfatin, a potential biomarker and prognostic factor for endometrial cancer. Gynecol. Oncol. 2013, 129, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Dallal, C.M.; Brinton, L.A.; Bauer, D.C.; Buist, D.S.; Cauley, J.A.; Hue, T.F.; Lacroix, A.; Tice, J.A.; Chia, V.M.; Falk, R.; et al. Obesity-related hormones and endometrial cancer among postmenopausal women: A nested case—control study within the B~FIT cohort. Endocr.-Relat. Cancer 2013, 20, 151–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atoum, M.F.; Alzoughool, F.; Al-Hourani, H. Linkage Between Obesity Leptin and Breast Cancer. Breast Cancer Basic Clin. Res. 2020, 14. [Google Scholar] [CrossRef]
- Tumminia, A.; Vinciguerra, F.; Parisi, M.; Graziano, M.; Sciacca, L.; Baratta, R.; Frittitta, L. Adipose Tissue, Obesity and Adiponectin: Role in Endocrine Cancer Risk. Int. J. Mol. Sci. 2019, 20, 2863. [Google Scholar] [CrossRef] [Green Version]
- Soliman, P.T.; Wu, D.; Tortolero-Luna, G.; Schmeler, K.M.; Slomovitz, B.M.; Bray, M.S.; Gershenson, D.M.; Lu, K.H. Association between adiponectin, insulin resistance, and endometrial cancer. Cancer 2006, 106, 2376–2381. [Google Scholar] [CrossRef]
- Ashizawa, N.; Yahata, T.; Quan, J.; Adachi, S.; Yoshihara, K.; Tanaka, K. Serum leptin-adiponectin ratio and endometrial cancer risk in postmenopausal female subjects. Gynecol. Oncol. 2010, 119, 65–69. [Google Scholar] [CrossRef]
- Reneau, J.; Goldblatt, M.; Gould, J.; Kindel, T.; Kastenmeier, A.; Higgins, R.; Rengel, L.R.; Schoyer, K.; James, R.; Obi, B.; et al. Effect of adiposity on tissue-specific adiponectin secretion. PLoS ONE 2018, 13, e0198889. [Google Scholar] [CrossRef]
- Weyer, C.; Funahashi, T.; Tanaka, S.; Hotta, K.; Matsuzawa, Y.; Pratley, R.E.; Tataranni, P.A. Hypoadiponectinemia in obesity and type 2 diabetes: Close association with insulin resistance and hyperinsulinemia. J. Clin. Endocrinol. Metab. 2001, 86, 1930–1935. [Google Scholar] [CrossRef] [PubMed]
- Wajchenberg, B.L. Subcutaneous and visceral adipose tissue: Their relation to the metabolic syndrome. Endocr. Rev. 2000, 21, 697–738. [Google Scholar] [CrossRef] [PubMed]
- Gunter, M.J.; Hoover, D.R.; Yu, H.; Wassertheil-Smoller, S.; Manson, J.E.; Li, J.; Harris, T.G.; Rohan, T.E.; Xue, X.; Ho, G.Y.; et al. A prospective evaluation of insulin and insulin-like growth factor-I as risk factors for endometrial cancer. Cancer Epidemiol. Biomark. Prev. 2008, 17, 921–929. [Google Scholar] [CrossRef] [Green Version]
- Kluge, A.; Zimmermann, R.; Münkel, B.; Mohri, M.; Sack, S.; Schaper, J.; Schaper, W. Insulin-like growth factor I is involved in inflammation linked angiogenic processes after microembolisation in porcine heart. Cardiovasc. Res. 1995, 29, 407–415. [Google Scholar] [CrossRef]
- Khandwala, H.M.; McCutcheon, I.E.; Flyvbjerg, A.; Friend, K.E. The effects of insulin-like growth factors on tumorigenesis and neoplastic growth. Endocr. Rev. 2000, 21, 215–244. [Google Scholar] [CrossRef]
- Vrachnis, N.; Iavazzo, C.; Iliodromiti, Z.; Sifakis, S.; Alexandrou, A.; Siristatidis, C.; Grigoriadis, C.; Botsis, D.; Creatsas, G. Diabetes mellitus and gynecologic cancer: Molecular mechanisms, epidemiological, clinical and prognostic perspectives. Arch. Gynecol. Obstet. 2016, 293, 239–246. [Google Scholar] [CrossRef]
- Nead, K.T.; Sharp, S.J.; Thompson, D.J.; Painter, J.N.; Savage, D.B.; Semple, R.K.; Barker, A.; Australian National Endometrial Cancer Study Group (ANECS); Perry, J.R.; Attia, J.; et al. Evidence of a Causal Association Between Insulinemia and Endometrial Cancer: A Mendelian Randomization Analysis. J. Nat. Cancer Inst. 2015, 107, djv178. [Google Scholar] [CrossRef] [PubMed]
- Troisi, R.; Potischman, N.; Hoover, R.N.; Siiteri, P.; Brinton, L.A. Insulin and Endometrial Cancer. Am. J. Epidemiol. 1997, 146, 476–482. [Google Scholar] [CrossRef] [Green Version]
- Asghari, A.; Umetani, M. Obesity and Cancer: 27-Hydroxycholesterol, the Missing Link. Int. J. Mol. Sci. 2020, 21, E4822. [Google Scholar] [CrossRef]
- Weihe, P.; Spielmann, J.; Kielstein, H.; Henning-Klusmann, J.; Weihrauch-Blüher, S. Childhood Obesity and Cancer Risk in Adulthood. Curr. Obes. Rep. 2020. Advance online publication. [Google Scholar] [CrossRef]
- Zhao, Y.; Sun, H.; Feng, M.; Zhao, J.; Zhao, X.; Wan, Q.; Cai, D. Metformin is associated with reduced cell proliferation in human endometrial cancer by inbibiting PI3K/AKT/mTOR signaling. Gynecol. Endocrinol. 2018, 34, 428–432. [Google Scholar] [CrossRef] [PubMed]
- Qiang, P.; Shao, Y.; Sun, Y.P.; Zhang, J.; Chen, L.J. Metformin inhibits proliferation and migration of endometrial cancer cells through regulating PI3K/AKT/MDM2 pathway. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 1778–1785. [Google Scholar] [PubMed]
- Liu, Z.; Qi, S.; Zhao, X.; Li, M.; Ding, S.; Lu, J.; Zhang, H. Metformin inhibits 17β-estradiol-induced epithelial-to-mesenchymal transition via βKlotho-related ERK1/2 signaling and AMPKα signaling in endometrial adenocarcinoma cells. Oncotargets 2016, 19, 21315–21331. [Google Scholar] [CrossRef]
- Xue, J.; Li, L.; Li, N.; Li, F.; Qin, X.; Li, T.; Liu, M. Metformin suppresses cancer cell growth i n endometrial carcinoma by inhibiting PD-L1. Eur. J. Pharmacol. 2019, 15, 859. [Google Scholar] [CrossRef]
- Byrne, F.L.; Martin, A.R.; Kosasih, M.; Caruana, B.T.; Farrell, R. The Role of Hyperglycemia in Endometrial Cancer Pathogenesis. Cancers 2020, 8, 1191. [Google Scholar] [CrossRef]
- Meireles, C.G.; Pereira, S.A.; Valadares, L.P.; Rego, D.F.; Simeoni, L.A.; Guerra, E.N.S.; Lofrano-Porto, A. Effects of metformin on endometrial cancer: Systematic review and meta-analysis. Gynecol. Oncol. 2017, 147, 167–180. [Google Scholar] [CrossRef]
- Perez-Lopez, F.R.; Pasupuleti, V.; Gianuzzi, X.; Palma-Ardiles, G.; Hernandez-Fernandez, W.; Adrian, V.H. Systematic review and meta-analysis of the effect of metformin treatment on overall mortality rates in women with endometrial cancer and type 2 diabetes mellitus. Maturitas 2017, 101, 6–11. [Google Scholar] [CrossRef]
- Chu, D.; Wu, J.; Wang, K.; Zhao, M.; Wang, C.; Li, L.; Guo, R. Effect of metformin use on the risk and prognosis of endometrial cancer: A systematic review and meta-analysis. BMC Cancer 2018, 18, 438. [Google Scholar] [CrossRef] [Green Version]
- Nevadunsky, N.S.; Van Arsdale, A.; Strickler, H.D.; Moadel, A.; Kaur, G.; Frimer, M.; Conroy, E.; Goldberg, G.L.; Einstein, M.H. Metformin use and endometrial cancer survival. Gynecol. Oncol. 2014, 132, 236–240. [Google Scholar] [CrossRef]
- Ko, E.M.; Walter, P.; Jackson, A.; Clark, L.; Franasiak, J.; Bolac, C.; Havrilesky, L.J.; Secord, A.A.; Moore, D.T.; Gehrig, P.A.; et al. Metformin is associated with improved survival in endometrial cancer. Gynecol. Oncol. 2014, 132, 438–442. [Google Scholar] [CrossRef]
- Al Hilli, M.M.; Bakkum-Gamez, J.N.; Mariani, A.; Cliby, W.A.; Mc Gree, M.E.; Weaver, A.L.; Dowdy, S.C.; Podratz, K.C. The effect of diabetes and metformin on clinical outcomes is negligible in risk-adjusted endometrial cancer cohorts. Gynecol. Oncol. 2016, 140, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Lemanska, A.; Zaborowski, M.; Spaczynski, M.; Nowak-Markwitz, E. Do endometrial cancer patients benefit from metformin intake? Ginekol. Pol. 2015, 86, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Seebacher, V.; Bergmeister, B.; Grimm, C.; Koelbl, H.; Reinthaller, A.; Polterauer, S. The prognostic role of metformin in patients with endometrial cancer: A retrospective study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 203, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Arima, R.; Hautakoski, A.; Marttila, M.; Arffman, M.; Sund, R.; Ilanne-Parikka, P.; Kangaskokko, J.; Hinkula, M.; Puistola, U.; Läärä, E. Cause-specific mortality in endometrioid endometrial cancer patients with type 2 diabetes using metformin or other types of antidiabetic medication. Gynecol. Oncol. 2017, 147, 678–683. [Google Scholar] [CrossRef] [Green Version]
- Janda, M.; Gebski, V.; Davies, L.C.; Forder, P.; Brand, A.; Hogg, R.; Jobling, T.W.; Land, R.; Manolitsas, T.; Nascimento, M.; et al. Effect of Total Laparoscopic Hysterectomy vs. Total Abdominal Hysterectomy on Disease-Free Survival Among Women with Stage I Endometrial Cancer: A Randomized Clinical Trial. JAMA 2017, 317, 1224–1233. [Google Scholar] [CrossRef] [Green Version]
- Mahdi, H.; Jernigan, A.M.; Aljebori, Q.; Lockhart, D.; Moslemi-Kebria, M. The impact of obesity on the 30-day morbidity and mortality after surgery for endometrial cancer. J. Minim. Invasive Gynecol. 2015, 22, 94–102. [Google Scholar] [CrossRef]
- Al Sawah, E.; Salemi, J.L.; Hoffman, M.; Imudia, A.N.; Mikhail, E. Association between Obesity, Surgical Route, and Perioperative Outcomes in Patients with Uterine Cancer. Minim. Invasive Surg. 2018, 19, 5130856. [Google Scholar] [CrossRef] [Green Version]
- Gambacorti-Passerini, Z.M.; López-De la Manzanara Cano, C.; Pérez Parra, C.; Cespedes Casas, M.C.; Sánchez Hipólito, L.; Martín Francisco, C.; Muñoz-Rodríguez, J.R. Obesity in Patients with Endometrial Cancer: May It Affect the Surgical Outcomes of Laparoscopic Approach? Obes. Surg. 2019, 29, 3285–3290. [Google Scholar] [CrossRef]
- Cusimano, M.C.; Simpson, A.N.; Dossa, F.; Liani, V.; Kaur, Y.; Acuna, S.A.; Robertson, D.; Satkunaratnam, A.; Bernardini, M.Q.; Ferguson, S.E.; et al. Laparoscopic and robotic hysterectomy in endometrial cancer patients with obesity: A systematic review and meta-analysis of conversions and complications. Arch. Gynecol. Obstet. 2017, 295, 965–969. [Google Scholar]
- Orekoya, O.; Samson, M.E.; Trivedi, T.; Vyas, S.; Steck, S.E. The impact of obesity on surgical outcome in endometrial cancer patients: A systematic review. J. Gynecol. Surg. 2016, 32, 149–157. [Google Scholar] [CrossRef] [Green Version]
- Horowitz, N.S.; Wright, A.A. Impact of obesity on chemotherapy management and outcomes in women with gynecologic malignancies. Gynecol. Oncol. 2015, 138, 201–206. [Google Scholar] [CrossRef] [Green Version]
- Ottaiano, A.; De Divitiis, C.; Capozzi, M.; Avallone, A.; Pisano, C.; Pignata, S.; Tafuto, S. Obesity and Cancer: Biological Links and Treatment Implications. Curr. Cancer Drug Targ. 2018, 18, 231–238. [Google Scholar] [CrossRef]
- Griggs, J.J.; Mangu, P.B.; Anderson, H.; Balaban, E.P.; Dignam, J.J.; Hryniuk, W.M.; Morrison, V.A.; Pini, T.M.; Runowicz, C.D.; Rosner, G.L.; et al. American Society of Clinical Oncology. Appropriate chemotherapy dosing for obese adult patients with cancer: American Society of Clinical Oncology clinical practice guideline. J. Clin. Oncol. 2012, 30, 1553–1561. [Google Scholar] [CrossRef]
- Schwartz, J.; Toste, B.; Dizon, D.S. Chemotherapy toxicity in gynecologic cancer patients with a body surface area (BSA)>2 m2. Gynecol. Oncol. 2009, 114, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Smits, A.; McGrane, J.; Lopes, A.; Kent, E.; Bekkers, R.; Massuger, L.; Simpson, N.; Galaal, K. Radiation-related toxicities and outcomes in endometrial cancer: Are obese women at a disadvantage? Int. J. Clin. Oncol. 2017, 22, 945–953. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Chlebowski, R.T.; Hendryx, M.; Rohan, T.; Wactawski-Wende, J.; Thomson, C.A.; Felix, A.S.; Chen, C.; Barrington, W.; Coday, M.; et al. Intentional weight loss and endometrial cancer risk. J. Clin. Oncol. 2017, 35, 1189–1193. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Hendryx, M.; Manson, J.E.; Figueiredo, J.C.; LeBlanc, E.S.; Barrington, W.; Rohan, T.E.; Howard, B.V.; Reding, K.; Ho, G.Y.; et al. Intentional weight loss and obesity-related cancer risk. JNCI Cancer Spectr. 2019, 3, pkz054. [Google Scholar] [CrossRef]
- Zhang, X.; Rhoades, J.; Caan, B.J.; Cohn, D.E.; Salani, R.; Noria, S.; Suarez, A.A.; Paskett, E.D.; Felix, A.S. Intentional weight loss, weight cycling, and endometrial cancer risk: A systematic review and meta-analysis. Int. J. Gynecol. Cancer 2019, 29, 1361–1371. [Google Scholar] [CrossRef]
- Moore, S.C.; Lee, I.; Weiderpass, E.; Campbell, P.T.; Sampson, J.N.; Kitahara, C.M.; Keadle, S.K.; Arem, H.; Berrington de Gonzalez, A.; Hartge, P.; et al. Association of leisure-time physical activity with risk of 26 types of cancer in 1.44 million adults. Complement Ther. Med. 2019, 44, 9–13. [Google Scholar] [CrossRef]
- Lugo, D.; Pulido, A.L.; Mihos, C.G.; Issa, O.; Cusnir, M.; Horvath, S.A.; Lin, J.; Santana, O. The effects of physical activity on cancer prevention, treatment and prognosis: A review of the literature. JAMA Intern. Med. 2016, 176, 816–825. [Google Scholar] [CrossRef]
- Kerr, J.; Anderson, C.; Lippman, S.M. Physical activity, sedentary behaviour, diet, and cancer: An update and emerging new evidence. Lancet Oncol. 2017, 18, e457–e471. [Google Scholar] [CrossRef]
- Koutoukidis, D.A.; Knobf, M.T.; Lanceley, A. Obesity, diet, physical activity, and health-related quality of life in endometrial cancer survivors. Nutr. Rev. 2015, 73, 399–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demark-Wahnefried, W.; Morey, M.C.; Sloane, R.; Snyder, D.C.; Miller, P.E.; Hartman, T.J.; Cohenet, H.J. Reach out to enhance wellness home-based diet-exercise intervention promotes reproducible and sustainable long-term improvements in health behaviors, body weight, and physical functioning in older, overweight/obese cancer survivors. J. Clin. Oncol. 2012, 30, 2354–2361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sjostrom, L.; Narbro, K.; Sjostrom, C.D.; Karason, K.; Larsson, B.; Wedel, H.; Lystig, T.; Sullivan, M.; Bouchard, C.; Carlsson, B.; et al. Effects of bariatric surgery on mortality in Swedish obese subjects. N. Engl. J. Med. 2007, 357, 741–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anveden, Å.; Taube, M.; Peltonen, M.; Jacobson, P.; Andersson-Assarsson, J.C.; Sjöholm, K.; Svensson, P.-A.; Carlsson, L.M.S. Long-term incidence of female-specific cancer after bariatric surgery or usual care in the Swedish Obese Subjects Study. Gynecol. Oncol. 2017, 145, 224–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winder, A.A.; Kularatna, M.; MacCormick, A.D. Does bariatric surgery affect the incidence of endometrial cancer development? A systematic review. Obes. Surg. 2018, 28, 1433–1440. [Google Scholar] [CrossRef]
- Izquierdo, A.G.; Carreira, M.C.; Rodriguez-Carnero, G.; Fernandez-Quintela, A.; Sueiro, A.M.; Martinez-Olmos, M.A.; Guzman, G.; De Luis, D.; Pinhel, M.A.S.; Nicoletti, C.F.; et al. Weight loss normalizes enhanced expression of the oncogene survivin in visceral adipose tissue and blood leukocytes from individuals with obesity. Int. J. Obes. 2020. Online ahead of print. [Google Scholar] [CrossRef]
- El-Safadi, S.; Sauerbier, A.; Hackethal, A.; Münstedt, K. Body weight changes after the diagnosis of endometrial cancer and their influences on disease-related prognosis. Arch. Gynecol. Obstet. 2012, 285, 1725–1729. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiesel, L.; Eichbaum, C.; Baumeier, A.; Eichbaum, M. Obesity Epidemic—The Underestimated Risk of Endometrial Cancer. Cancers 2020, 12, 3860. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12123860
Kiesel L, Eichbaum C, Baumeier A, Eichbaum M. Obesity Epidemic—The Underestimated Risk of Endometrial Cancer. Cancers. 2020; 12(12):3860. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12123860
Chicago/Turabian StyleKiesel, Ludwig, Christine Eichbaum, Ariane Baumeier, and Michael Eichbaum. 2020. "Obesity Epidemic—The Underestimated Risk of Endometrial Cancer" Cancers 12, no. 12: 3860. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12123860