The Clinicopathological Features and Genetic Mutations in Gastric Cancer Patients According to EMAST and MSI Status

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Clinicopathological Profiles
2.2. Mutational Profiling of GC Subtypes According to EMAST/MSI Status
2.3. Initial Recurrence Patterns
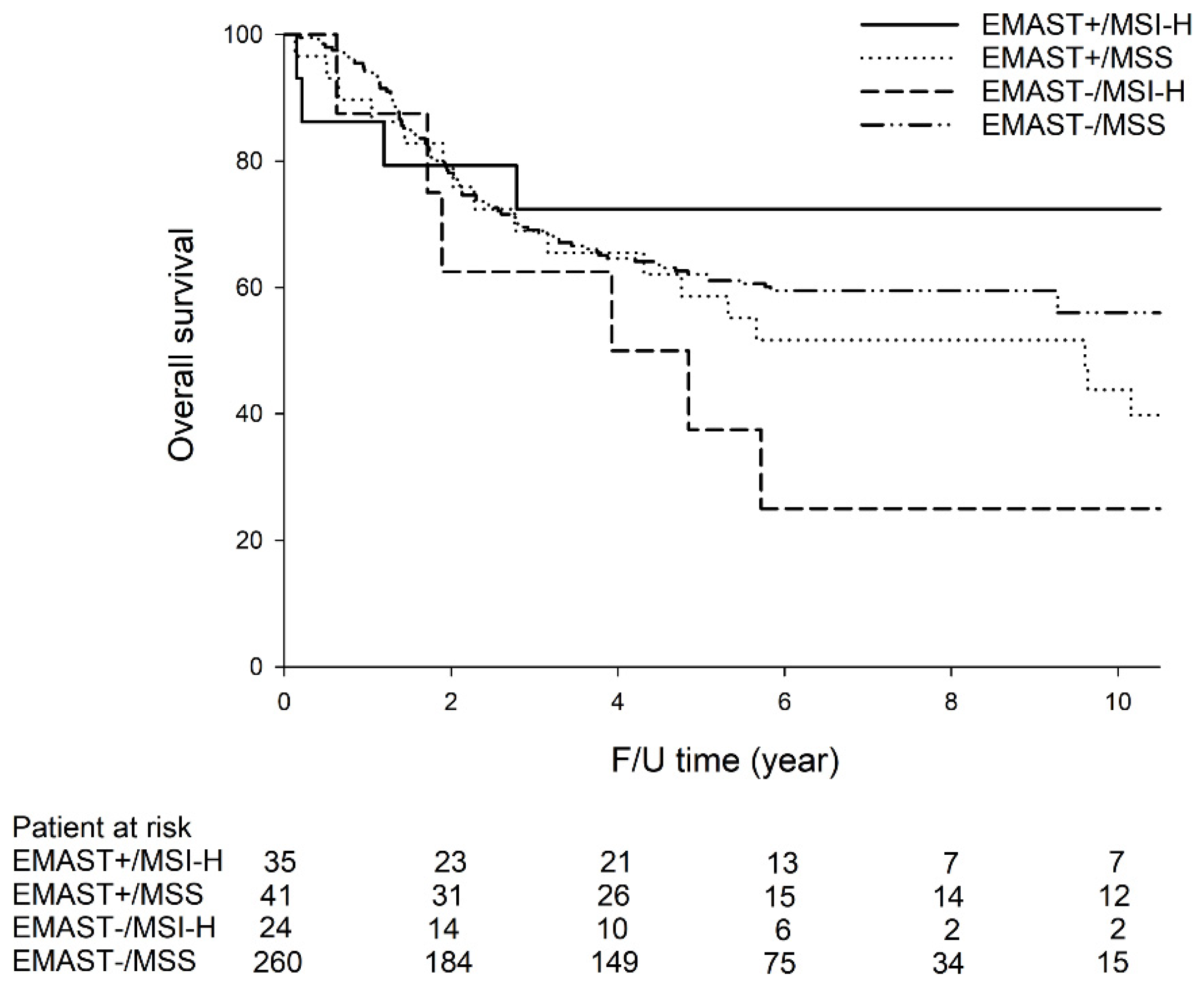
2.4. Survival Analysis
2.5. Subgroup Analysis for MSI-H GC
3. Discussion
4. Materials and Methods
4.1. Patients and Tissue Collection
4.2. Analysis of MSI and EMAST Statuses
4.3. Identification of HP and EBV Infection
4.4. Identification of PIK3CA Amplification
4.5. Mutation Analysis of Common GC-related Genes Based on MassARRAY
4.6. Next-Generation Sequencing
4.7. Immunohistochemical Staining for MSH3
4.8. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [Green Version]
- TCGA. Comprehensive molecular characterization of gastric adenocarcinoma. Nature 2014, 513, 202–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.; Zhang, F.; Zhou, N.; Gu, Y.M.; Zhang, Y.T.; He, Y.D.; Wang, L.; Yang, L.X.; Zhao, Y.; Li, Y.M. Efficacy and safety of immune checkpoint inhibitors in advanced gastric or gastroesophageal junction cancer: A systematic review and meta-analysis. Oncoimmunology 2019, 8, e1581547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watson, M.M.; Berg, M.; Søreide, K. Prevalence and implications of elevated microsatellite alterations at selected tetranucleotides in cancer. Br. J. Cancer 2014, 111, 823–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watson, M.M.; Lea, D.; Rewcastle, E.; Hagland, H.R.; Søreide, K. Elevated microsatellite alterations at selected tetranucleotides in early-stage colorectal cancers with and without high-frequency microsatellite instability: Same, same but different? Cancer Med. 2016, 5, 1580–1587. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.S.; Park, K.U.; Kim, D.W.; Lhn, M.H.; Kim, W.H.; Seo, A.N.; Chang, H.E.; Nam, S.K.; Lee, S.Y.; Oh, H.K.; et al. Elevated Microsatellite Alterations at Selected Tetranucleotide repeats (EMAST) and microsatellite instability in patients with colorectal cancer and its clinical features. Curr. Mol. Med. 2016, 6, 829–839. [Google Scholar] [CrossRef]
- Arai, H.; Okudela, K.; Oshiro, H.; Komitsu, N.; Mitsui, H.; Nishii, T.; Tsuboi, M.; Nozawa, A.; Noishi, K.; Ohashi, K.; et al. Elevated microsatellite alterations at selected tetra-nucleotide (EMAST) in non-small cell lung cancers—A potential determinant of susceptibility to multiple malignancies. Int. J. Clin. Exp. Pathol. 2013, 6, 395–410. [Google Scholar]
- Venderbosch, S.; van Lent-van Vliet, S.; de Haan, A.F.; Ligtenberg, M.J.; Goossens, M.; Punt, C.J.; Koopman, M.; Nagtegaal, I.D. EMAST is associated with a poor prognosis in microsatellite instable metastatic colorectal cancer. PLoS ONE 2015, 10, e0124538. [Google Scholar] [CrossRef]
- Chen, M.H.; Chang, S.C.; Lin, P.C.; Yang, S.H.; Lin, C.C.; Lan, Y.T.; Lin, H.H.; Lin, C.H.; Lai, J.I.; Liang, W.Y.; et al. Combined microsatellite instability and Elevated Microsatellite Alterations at Selected Tetranucleotide repeats (EMAST) might be a more promising immune biomarker in colorectal cancer. Oncologist 2019, 24, 1534–1542. [Google Scholar] [CrossRef] [Green Version]
- Benatti, P.; Gafa, R.; Barana, D.; Marino, M.; Scarselli, A.; Pedroni, M.; Maestri, I.; Guerzoni, L.; Roncucci, L.; Menigatti, M.; et al. Microsatellite instability and colorectal cancer prognosis. Clin. Cancer Res. 2005, 11, 8332–8340. [Google Scholar] [CrossRef] [Green Version]
- Mori, T.; Hamaya, Y.; Uotani, T.; Yamade, M.; Iwaizumi, M.; Furuta, T.; Miyajima, H.; Osawa, S.; Sugimoto, K. Prevalence of elevated microsatellite alterations at selected tetranucleotide repeats in pancreatic ductal adenocarcinoma. PLoS ONE 2018, 13, e0208557. [Google Scholar] [CrossRef] [PubMed]
- Le, D.T.; Uram, J.N.; Wang, H.; Bartlett, B.R.; Kemberling, H.; Eyring, A.D.; Skora, A.D.; Luber, B.S.; AZAD, N.S.; Laheru, D.; et al. Pd-1 blockade in tumors with mismatch-repair deficiency. N. Engl. J. Med. 2015, 372, 2509–2520. [Google Scholar] [CrossRef] [PubMed]
- Overman, M.J.; McDermott, R.; Leach, J.L.; Lonardi, S.; Lenz, H.J.; Morse, M.A.; Desai, J.; Hill, A.; Axelson, M.; Moss, R.A.; et al. Nivolumab in patients with metastatic DNA mismatch repair-deficient or microsatellite instability-high colorectal cancer (checkmate 142): An open-label, multicentre, phase 2 study. Lancet Oncol. 2017, 18, 1182–1191. [Google Scholar] [CrossRef]
- Corso, G.; Velho, S.; Paredes, J.; Pedrazzani, C.; Martins, D.; Milanezi, F.; Pascale, V.; Vindigni, C.; Pinheiro, H.; Leite, M.; et al. Oncogenic mutations in gastric cancer with microsatellite instability. Eur. J. Cancer 2011, 47, 443–451. [Google Scholar] [CrossRef]
- Corso, G.; Pedrazzani, C.; Marrelli, D.; Pascale, V.; Pinto, E.; Roviello, F. Correlation of microsatellite instability at multiple loci with long-term survival in advanced gastric carcinoma. Arch. Surg. 2009, 144, 722–727. [Google Scholar] [CrossRef] [Green Version]
- Kucherlapati, M.H.; Esfahani, S.; Habibollahi, P.; Wang, J.; Still, E.R.; Bronson, R.T.; Mahmood, U.; Kucheriapati, R.S. Genotype directed therapy in murine mismatch repair deficient tumors. PLoS ONE 2013, 8, e68817. [Google Scholar] [CrossRef]
- Xu, H.; Feng, Y.; Jia, Z.; Yang, J.; Lu, X.; Li, J.; Xia, M.; Wu, C.; Zhang, Y.; Chen, J. AXIN1 protects against testicular germ cell tumors via the PI3K/AKT/mTOR signaling pathway. Oncol. Lett. 2017, 14, 981–986. [Google Scholar] [CrossRef] [Green Version]
- Fang, W.L.; Chang, S.C.; Lan, Y.T.; Huang, K.H.; Chen, J.H.; Lo, S.S.; Hsieh, M.C.; Li, A.F.; Wu, C.W.; Chiou, S.H. Microsatellite instability is associated with a better prognosis for gastric cancer patients after curative surgery. World J. Surg. 2012, 36, 2131–2138. [Google Scholar] [CrossRef]
- Devaraj, B.; Lee, A.; Cabrera, B.L.; Miyai, K.; Luo, L.; Ramamoorthy, S.; Keku, T.; Sandler, R.S.; McGuire, K.L.; Carethers, J.M. Relationship of EMAST and microsatellite instability among patients with rectal cancer. J. Gastrointest. Surg. 2010, 14, 1521–1528. [Google Scholar] [CrossRef] [Green Version]
- Fang, W.L.; Huang, K.H.; Chang, S.C.; Lin, C.H.; Chen, M.H.; Chao, Y.; Lo, S.S.; Li, A.F.; Wu, C.W.; Shyr, Y.M. Comparison of the clinicopathological characteristics and genetic alterations between patients with gastric cancer with or without helicobacter pylori infection. Oncologist 2019, 24, e845–e853. [Google Scholar] [CrossRef] [Green Version]
- Fang, W.L.; Huang, K.H.; Lan, Y.T.; Lin, C.H.; Chang, S.C.; Chen, M.H.; Chao, Y.; Lin, W.C.; Lo, S.S.; Li, A.F.; et al. Mutations in PI3K/AKT pathway genes and amplifications of PIK3CA are associated with patterns of recurrence in gastric cancers. Oncotarget 2016, 7, 6201–6220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carethers, J.M.; Koi, M.; Tseng-Rogenski, S.S. EMAST is a form of microsatellite instability that is initiated by inflammation and modulates colorectal cancer progression. Genes (Basel) 2015, 6, 185–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haugen, A.C.; Goel, A.; Yamada, K.; Marra, G.; Nguyen, T.P.; Nagasaka, T.; Kanazawa, S.; Koike, J.; Kikuchi, Y.; Zhong, X.; et al. Genetic instability caused by loss of MutS homologue 3 in human colorectal cancer. Cancer Res. 2008, 68, 8465–8472. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Clinical Profiles | EMAST Status | MSI Status | ||||
|---|---|---|---|---|---|---|
| Variables | − n = 284 n (%) | + n = 76 n (%) | p-Value | MSS n = 301 n (%) | MSI-H n = 59 n (%) | p-Value |
| Age (y/o) | 0.327 | 0.028 | ||||
| <45 | 20 (7.0) | 3 (3.9) | 23 (7.6) | 0 | ||
| ≥45 | 264 (93.0) | 73 (96.1) | 278 (92.4) | 59 (100) | ||
| Gender (M/F) | 189/95 | 56/20 | 0.236 | 204/97 | 41/18 | 0.796 |
| Tumor size (<5/≥5 cm) | 98/186 | 21/55 | 0.258 | 107/194 | 12/47 | 0.023 |
| Cell differentiation | 0.929 | 0.559 | ||||
| Poor | 162 (57.0) | 43 (56.6) | 174 (57.8) | 31 (52.5) | ||
| Moderate | 119 (41.9) | 44 (43.4) | 124 (41.2) | 28 (47.5) | ||
| Well | 3 (1.1) | 0 | 3 (1.0) | 0 | ||
| Gross appearance | 0.005 | 0.510 | ||||
| Superficial type | 18 (6.3) | 8 (10.5) | 24 (8.0) | 2 (3.4) | ||
| Borrmann type 1 and 2 | 74 (26.1) | 32 (42.1) | 87 (28.9) | 19 (32.2) | ||
| Borrmann type 3 and 4 | 192 (67.6) | 36 (47.4) | 190 (63.1) | 38 (64.4) | ||
| Lymphovascular invasion | 201 (70.8) | 52 (68.4) | 0.690 | 208 (69.1) | 45 (76.3) | 0.271 |
| Lymphoid stroma | 27 (9.5) | 12 (15.8) | 0.118 | 30 (10.0) | 9 (15.3) | 0.232 |
| EBV infection | 33 (11.6) | 12 (15.8) | 0.329 | 33 (11.0) | 12 (20.3) | 0.046 |
| HP infection | 104 (36.6) | 11 (14.5) | <0.001 | 105 (34.9) | 10 (16.9) | 0.007 |
| PIK3CA amplification | 76 (26.8) | 16 (21.1) | 0.311 | 78 (25.9) | 14 (23.7) | 0.725 |
| Pathological T category | 0.049 | 0.232 | ||||
| T1 | 32 (11.3) | 11 (14.5) | 37 (12.3) | 6 (10.2) | ||
| T2 | 30 (10.6) | 16 (21.1) | 34 (11.3) | 12 (20.3) | ||
| T3 | 125 (44.0) | 31 (40.8) | 130 (43.2) | 26 (44.1) | ||
| T4 | 97 (34.2) | 18 (23.7) | 100 (33.2) | 15 (25.4) | ||
| Pathological N category | 0.121 | 0.911 | ||||
| N0 | 65 (22.9) | 26 (34.2) | 77 (25.6) | 14 (23.7) | ||
| N1 | 42 (14.8) | 14 (18.4) | 45 (15.0) | 11 (18.6) | ||
| N2 | 53 (18.7) | 11 (14.5) | 54 (17.9) | 10 (16.9) | ||
| N3 | 124 (43.7) | 25 (32.9) | 125 (41.5) | 24 (40.7) | ||
| Pathological TNM Stage | 0.050 | 0.507 | ||||
| I | 40 (14.1) | 20 (26.3) | 48 (15.9) | 12 (20.3) | ||
| II | 68 (23.9) | 17 (22.4) | 75 (24.9) | 10 (16.9) | ||
| III | 113 (48.9) | 34 (44.7) | 142 (47.2) | 31 (52.5) | ||
| IV | 37 (13.0) | 5 (6.6) | 36 (12.0) | 6 (10.2) | ||
| Genetic mutation | ||||||
| PI3K/AKT pathway | 22 (7.7) | 19 (25.0) | <0.001 | 25 (8.3) | 16 (27.1) | <0.001 |
| ARID1A | 11 (3.9) | 11 (14.5) | 0.001 | 18 (6.0) | 4 (6.8) | 0.815 |
| TP53 | 27 (9.5) | 5 (6.6) | 0.426 | 30 (10.0) | 2 (3.4) | 0.105 |
| KRAS | 8 (2.8) | 3 (3.9) | 0.611 | 7 (2.3) | 4 (6.8) | 0.069 |
| BRAF | 0 | 1 (1.3) | 0.053 | 1 (0.3) | 0 | 0.658 |
| Clinical Profiles | EMAST/MSI Status | ||||
|---|---|---|---|---|---|
| Variables | +/MSI-H n = 35 n (%) | +/MSS n = 41 n (%) | −/MSI-H n = 24 n (%) | −/MSS n =2 60 n (%) | p-Value |
| Age | 0.117 | ||||
| <45 years | 0 | 3 (7.3) | 0 | 20 (7.7) | |
| ≥45 years | 35 (100) | 38 (92.7) | 24 (100) | 240 (92.3) | |
| Gender (M/F) | 25/10 | 31/10 | 16/8 | 173/87 | 0.669 |
| Tumor size (<5/≥5 cm) | 8/27 | 13/28 | 4/20 | 94/166 | 0.126 |
| Cell differentiation | 0.889 | ||||
| Poor | 23 (65.7) | 20 (48.8) | 8 (33.3) | 154 (59.2) | |
| Moderate | 12 (34.3) | 21 (51.2) | 16 (66.7) | 103 (39.6) | |
| Well | 0 | 0 | 0 | 3 (1.2) | |
| Gross appearance | 0.030 | ||||
| Superficial type | 2 (5.7) | 6 (14.6) | 0 | 18 (6.9) | |
| Borrmann type 1 and 2 | 17 (48.6) | 15 (36.6) | 2 (8.3) | 72 (27.7) | |
| Borrmann type 3 and 4 | 16 (45.7) | 20 (48.8) | 22 (91.7) | 170 (65.4) | |
| Lymphovascular invasion | 23 (65.7) | 29 (70.7) | 22 (91.7) | 179 (68.8) | 0.118 |
| Lymphoid stroma | 9 (25.7) | 3 (7.3) | 0 | 27 (10.4) | 0.094 |
| EBV infection | 6 (17.1) | 6 (14.6) | 6 (25.0) | 27 (10.4) | 0.197 |
| HP infection | 6 (17.1) | 5 (12.2) | 4 (16.7) | 100 (38.5) | <0.001 |
| PIK3CA amplification | 6 (17.1) | 10 (24.4) | 8 (33.3) | 68 (26.2) | 0.543 |
| Pathological T category | 0.037 | ||||
| T1 | 6 (17.1) | 5 (12.2) | 0 | 32 (12.3) | |
| T2 | 8 (22.9) | 8 (19.5) | 4 (16.7) | 26 (10.0) | |
| T3 | 14 (40.0) | 17 (41.5) | 12 (50.0) | 113 (43.5) | |
| T4 | 7 (20.0) | 11 (26.8) | 8 (33.3) | 89 (34.2) | |
| Pathological N category | 0.062 | ||||
| N0 | 12 (34.3) | 14 (34.1) | 2 (8.3) | 63 (24.2) | |
| N1 | 7 (20.0) | 7 (17.1) | 4 (16.7) | 38 (14.6) | |
| N2 | 6 (17.1) | 5 (12.2) | 4 (16.7) | 49 (18.8) | |
| N3 | 10 (28.6) | 15 (36.6) | 14 (58.3) | 110 (42.3) | |
| Pathological TNM Stage | 0.038 | ||||
| I | 10 (28.6) | 10 (24.4) | 2 (8.3) | 38 (14.6) | |
| II | 8 (22.9) | 9 (22.0) | 2 (8.3) | 66 (25.4) | |
| III | 15 (42.9) | 19 (46.3) | 16 (66.7) | 123 (47.3) | |
| IV | 2 (5.7) | 3 (7.3) | 4 (16.7) | 33 (12.7) | |
| Genetic mutation | |||||
| PI3K/AKT pathway | 8 (22.9) | 11 (26.8) | 8 (33.3) | 14 (5.4) | <0.001 |
| ARID1A | 2 (5.7) | 9 (22.0) | 2 (8.3) | 9 (3.5) | 0.002 |
| TP53 | 0 | 5 (12.2) | 2 (8.3) | 25 (9.6) | 0.066 |
| KRAS | 2 (5.7) | 1 (2.4) | 2 (8.3) | 6 (2.3) | 0.422 |
| BRAF | 0 | 1 | 0 | 0 | 0.224 |
| EMAST Status | MSI Status | |||||
|---|---|---|---|---|---|---|
| Genes | − n = 76 | + n = 74 | p-Value | MSS n = 92 | MSI-H n = 58 | p-Value |
| EXO1 | 2 (2.6) | 9 (12.2) | 0.025 | 1 (1.1) | 10 (17.2) | <0.001 |
| EPCAM | 0 | 4 (5.4) | 0.040 | 0 | 4 (6.9) | 0.011 |
| MSH2 | 0 | 17 (23.0) | <0.001 | 9 (9.8) | 8 (13.8) | 0.451 |
| MSH6 | 6 (7.9) | 12 (16.2) | 0.117 | 8 (8.7) | 10 (17.2) | 0.117 |
| PCNA | 0 | 0 | - | 0 | 0 | - |
| PMS1 | 2 (2.6) | 2 (2.7) | 0.978 | 0 | 4 (6.9) | 0.011 |
| PMS2 | 2 (2.6) | 1 (1.4) | 0.576 | 3 (3.3) | 0 | 0.165 |
| TGFBR2 | 5 (6.6) | 15 (20.3) | 0.014 | 8 (8.7) | 12 (20.7) | 0.035 |
| MLH1 | 0 | 4 (5.4) | 0.040 | 4 (4.3) | 0 | 0.107 |
| CTNNB1 | 3 (3.9) | 4 (5.4) | 0.672 | 7 (7.6) | 0 | 0.031 |
| MSH3 | 4 (5.3) | 19 (25.7) | 0.001 | 13 (14.1) | 10 (17.2) | 0.607 |
| POLE | 2 (2.6) | 11 (14.9) | 0.008 | 9 (9.8) | 4 (6.9) | 0.541 |
| AXIN1 | 1 (1.3) | 11 (14.9) | 0.002 | 6 (6.5) | 6 (10.3) | 0.401 |
| AXIN2 | 0 | 4 (5.4) | 0.040 | 4 (4.3) | 0 | 0.107 |
| BAX | 3 (3.9) | 15 (20.3) | 0.002 | 6 (6.5) | 12 (20.7) | 0.009 |
| POLD1 | 3 (3.9) | 9 (12.2) | 0.064 | 6 (6.5) | 6 (10.3) | 0.401 |
| EMAST/MSI Status | p-Value | ||||
|---|---|---|---|---|---|
| Genes | +/MSI-H (n = 34) | +/MSS (n = 40) | −/MSI-H (n = 24) | −/MSS (n = 52) | |
| EXO1 | 8 (23.5) | 1 (2.5) | 2 (8.3) | 0 | 0.001 |
| EPCAM | 4 (11.8) | 0 | 0 | 0 | 0.005 |
| MSH2 | 8 (23.5) | 9 (22.5) | 0 | 0 | <0.001 |
| MSH6 | 8 (23.5) | 4 (10.0) | 2 (8.3) | 4 (7.7) | 0.048 |
| PCNA | 0 | 0 | 0 | 0 | - |
| PMS1 | 2 (5.9) | 0 | 2 (8.3) | 0 | 0.281 |
| PMS2 | 0 | 1 (2.5) | 0 | 2 (3.8) | 0.294 |
| TGFBR2 | 10 (29.4) | 5 (12.5) | 2 (8.3) | 3 (5.8) | 0.003 |
| MLH1 | 0 | 4 (10.0) | 0 | 0 | 0.281 |
| CTNNB1 | 0 | 4 (10.0) | 0 | 3 (5.8) | 0.596 |
| MSH3 | 8 (23.5) | 11 (27.5) | 2 (8.3) | 2 (3.8) | 0.002 |
| POLE | 4 (11.8) | 7 (17.5) | 0 | 2 (3.8) | 0.045 |
| AXIN1 | 6 (17.6) | 5 (12.5) | 0 | 1 (1.9) | 0.003 |
| AXIN2 | 0 | 4 (10.0) | 0 | 0 | 0.281 |
| BAX | 10 (29.4) | 5 (12.5) | 2 (8.3) | 1 (1.9) | <0.001 |
| POLD1 | 6 (17.6) | 3 (7.5) | 0 | 3 (5.8) | 0.055 |
| Recurrence Patterns | EMAST (−) n = 217 | EMAST (+) n = 58 | p-Value | MSS n = 230 | MSI-H n = 45 | p-Value |
|---|---|---|---|---|---|---|
| Total recurrence | 60 (27.6) | 9 (15.5) | 0.058 | 61 (26.5) | 8 (17.8) | 0.216 |
| Locoregional recurrence | 13 (6.0) | 4 (6.9) | 0.763 | 15 (6.5) | 2 (4.4) | 0.597 |
| Distant metastasis | 45 (20.7) | 5 (8.6) | 0.034 | 44 (19.1) | 6 (13.3) | 0.356 |
| Peritoneal dissemination | 20 (9.2) | 1 (1.7) | 0.090 | 17 (7.4) | 4 (8.9) | 0.759 |
| Hematogenous metastasis | 23 (10.6) | 3 (5.2) | 0.210 | 22 (9.6) | 4 (8.9) | 0.887 |
| Liver | 18 (8.3) | 2 (3.4) | 16 (7.0) | 4 (8.9) | ||
| Lung | 1 (0.5) | 2 (3.4) | 3 (1.3) | 0 | ||
| Bone | 3 (1.4) | 0 | 3 (1.3) | 0 | ||
| Skin | 1 (0.5) | 0 | 1 (0.4) | 0 | ||
| Distant lymphatic recurrence | 12 (5.5) | 1 (1.7) | 0.313 | 13 (5.7) | 0 | 0.136 |
| Virchow’s node | 1 (0.5) | 0 | 1 (0.4) | 0 | ||
| Para-aortic lymph node | 12 (5.7) | 1 (2.3) | 13 (5.7) | 0 |
| Recurrence Patterns | EMAST/MSI Status | ||||
|---|---|---|---|---|---|
| +/MSI-H n = 29 | +/MSS n = 29 | −/MSI-H n = 16 | −/MSS n = 201 | p-Value | |
| Total recurrence | 0 | 9 (31.0) | 8 (50.0) | 52 (25.9) | 0.001 |
| Locoregional recurrence | 0 | 4 (13.8) | 2 (12.5) | 11 (5.5) | 0.991 |
| Distant metastasis | 0 | 5 (17.2) | 6 (37.5) | 39 (19.4) | 0.014 |
| Peritoneal dissemination | 0 | 1 (3.4) | 4 (25.0) | 16 (8.0) | 0.019 |
| Hematogenous metastasis | 0 | 3 (10.3) | 4 (25.0) | 19 (9.5) | 0.056 |
| Liver | 0 | 2 (3.4) | 4 (25.0) | 14 (7.0) | |
| Lung | 0 | 2 (6.9) | 0 | 1 (0.5) | |
| Bone | 0 | 0 | 0 | 3 (1.5) | |
| Skin | 0 | 0 | 0 | 1 (0.5) | |
| Distant lymphatic recurrence | 0 | 1 (3.4) | 0 | 12 (6.0) | 0.127 |
| Virchow’s node | 0 | 0 | 0 | 1 (0.5) | |
| Para-aortic lymph node | 0 | 1 (3.4) | 0 | 12 (6.0) | |
| Risk Factors | Overall Survival | Disease-free Survival | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age (y/o) | 0.204 | 0.305 | ||||
| <45 | 1.00 | 1.00 | ||||
| ≥45 | 1.66 | 0.759–3.616 | 1.47 | 0.705–3.054 | ||
| Gender | 0.068 | 0.206 | ||||
| M | 1.00 | 1.00 | ||||
| F | 0.67 | 0.435–1.030 | 0.77 | 0.505–1.159 | ||
| Tumor size (cm) | 0.590 | 0.622 | ||||
| <5 | 1.00 | 1.00 | ||||
| ≥5 | 1.11 | 0.755–1.638 | 1.10 | 0.755–1.601 | ||
| Lymphovascular invasion | 0.046 | 0.045 | ||||
| Absent | 1.00 | 1.00 | ||||
| Present | 1.58 | 1.009–2.487 | 1.57 | 1.010–2.433 | ||
| Lauren’s classification | 0.022 | 0.033 | ||||
| Intestinal type | 1.00 | 1.00 | ||||
| Diffuse type | 1.55 | 1.064–2.268 | 1.50 | 1.032–2.169 | ||
| Pathological TNM stage | 0.001 | 0.002 | ||||
| I | 1.00 | 1.00 | ||||
| II | 1.02 | 0.555–1.867 | 1.05 | 0.581–1.895 | ||
| III | 2.18 | 1.184–4.011 | 2.18 | 1.208–3.935 | ||
| EMAST status | 0.384 | 0.490 | ||||
| − | 1.00 | 1.00 | ||||
| + | 1.22 | 0.781–1.900 | 1.17 | 0.748–1.831 | ||
| MSI status | 0.854 | 0.986 | ||||
| MSI-H | 1.00 | 1.00 | ||||
| MSS | 1.05 | 0.627–1.758 | 1.01 | 0.598–1.688 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fang, W.-L.; Chen, M.-H.; Huang, K.-H.; Chang, S.-C.; Lin, C.-H.; Chao, Y.; Lo, S.-S.; Li, A.F.-Y.; Wu, C.-W.; Shyr, Y.-M. The Clinicopathological Features and Genetic Mutations in Gastric Cancer Patients According to EMAST and MSI Status. Cancers 2020, 12, 551. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12030551
Fang W-L, Chen M-H, Huang K-H, Chang S-C, Lin C-H, Chao Y, Lo S-S, Li AF-Y, Wu C-W, Shyr Y-M. The Clinicopathological Features and Genetic Mutations in Gastric Cancer Patients According to EMAST and MSI Status. Cancers. 2020; 12(3):551. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12030551
Chicago/Turabian StyleFang, Wen-Liang, Ming-Huang Chen, Kuo-Hung Huang, Shih-Ching Chang, Chien-Hsing Lin, Yee Chao, Su-Shun Lo, Anna Fen-Yau Li, Chew-Wun Wu, and Yi-Ming Shyr. 2020. "The Clinicopathological Features and Genetic Mutations in Gastric Cancer Patients According to EMAST and MSI Status" Cancers 12, no. 3: 551. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12030551