Extended Texture Analysis of Non-Enhanced Whole-Body MRI Image Data for Response Assessment in Multiple Myeloma Patients Undergoing Systemic Therapy

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Material and Methods
2.1. Patient Characteristics
2.2. Whole-Body DWI Protocol Design
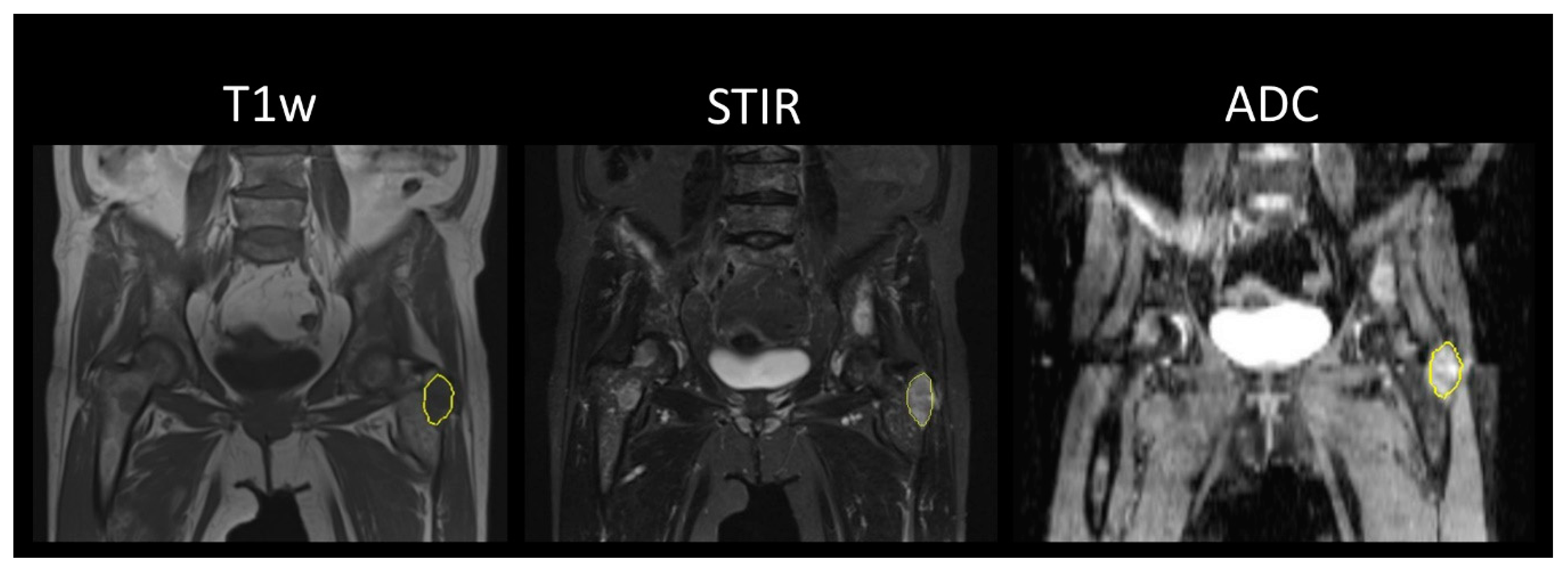
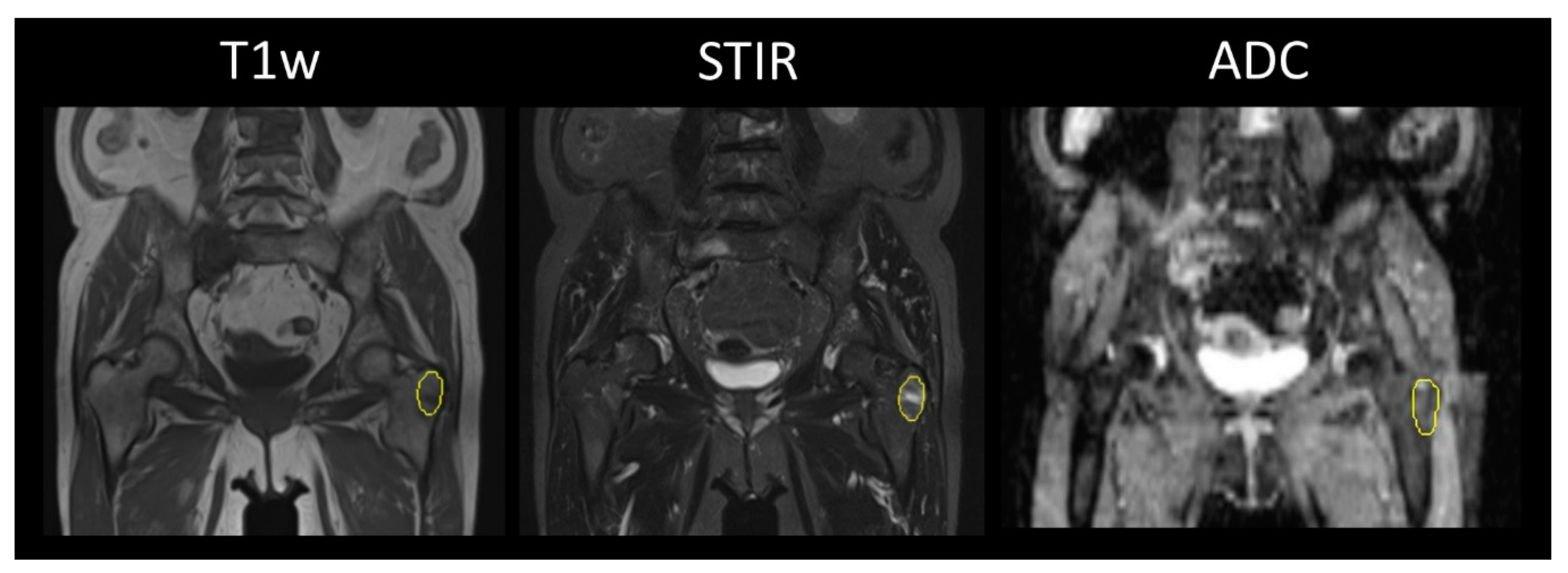
2.3. Image Analysis
2.4. Standard of Reference
2.5. Laboratory Data
2.6. Statistical Analysis
3. Results
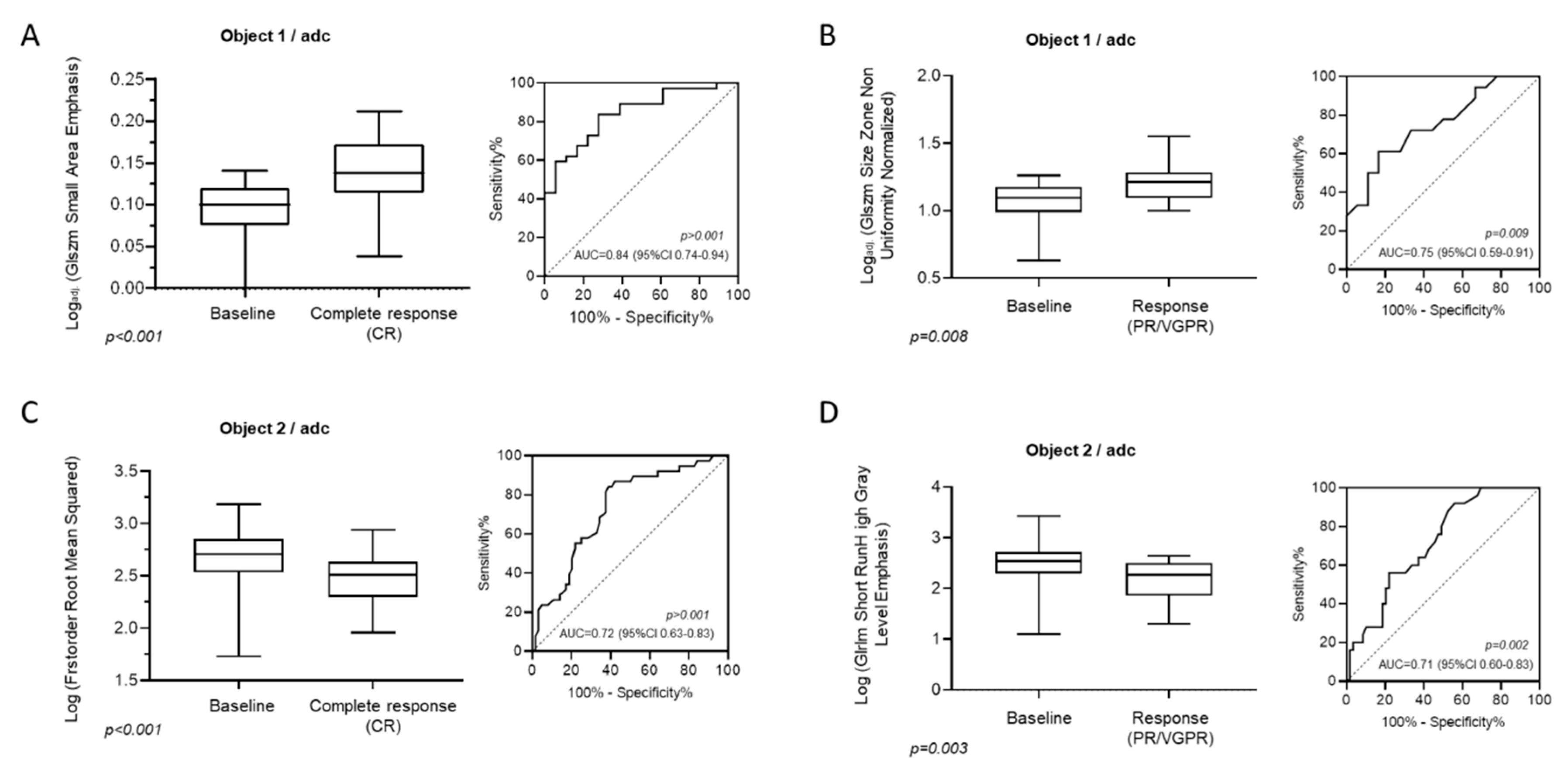
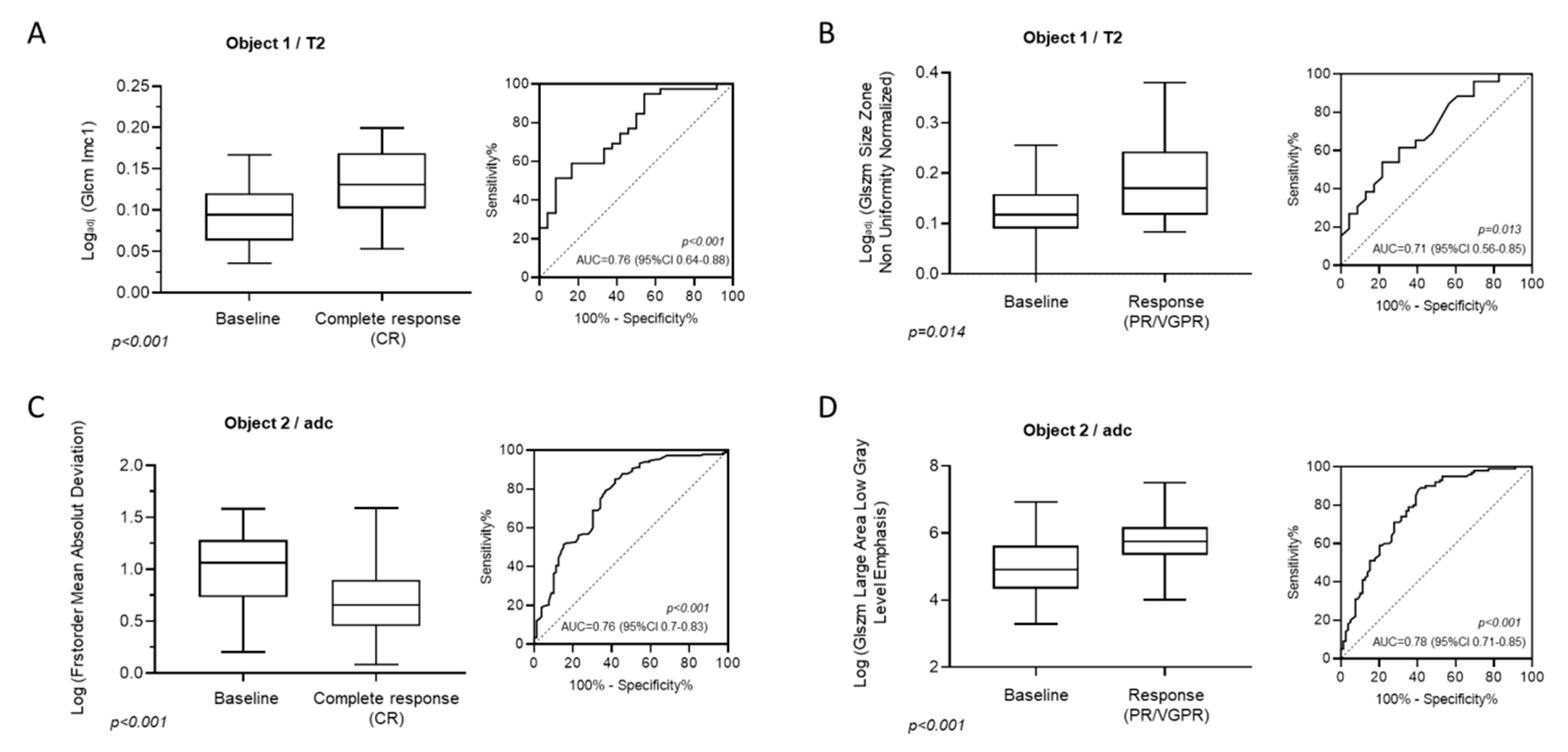
3.1. Identification of MRI-Features (ADC) Associated with Hematological Outcomes (CR, PR, or VGPR)
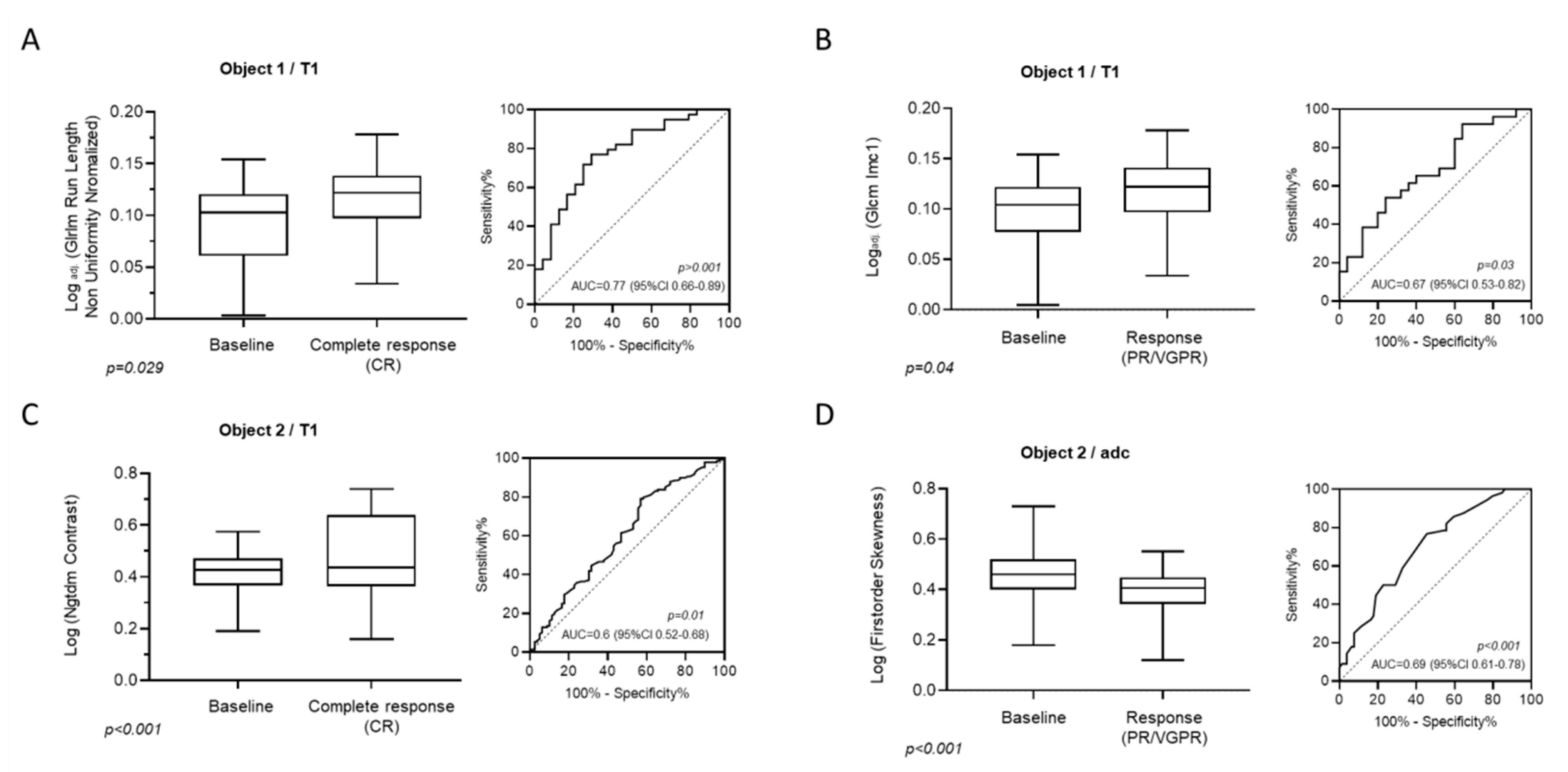
3.2. Identification of MRI-Features (T1w) Associated with Hematological Response Categories (CR, PR, or VGPR)
3.3. Identification of MRI-Features (T2w) Associated with Clinical Outcomes (CR, PR, or VGPR)
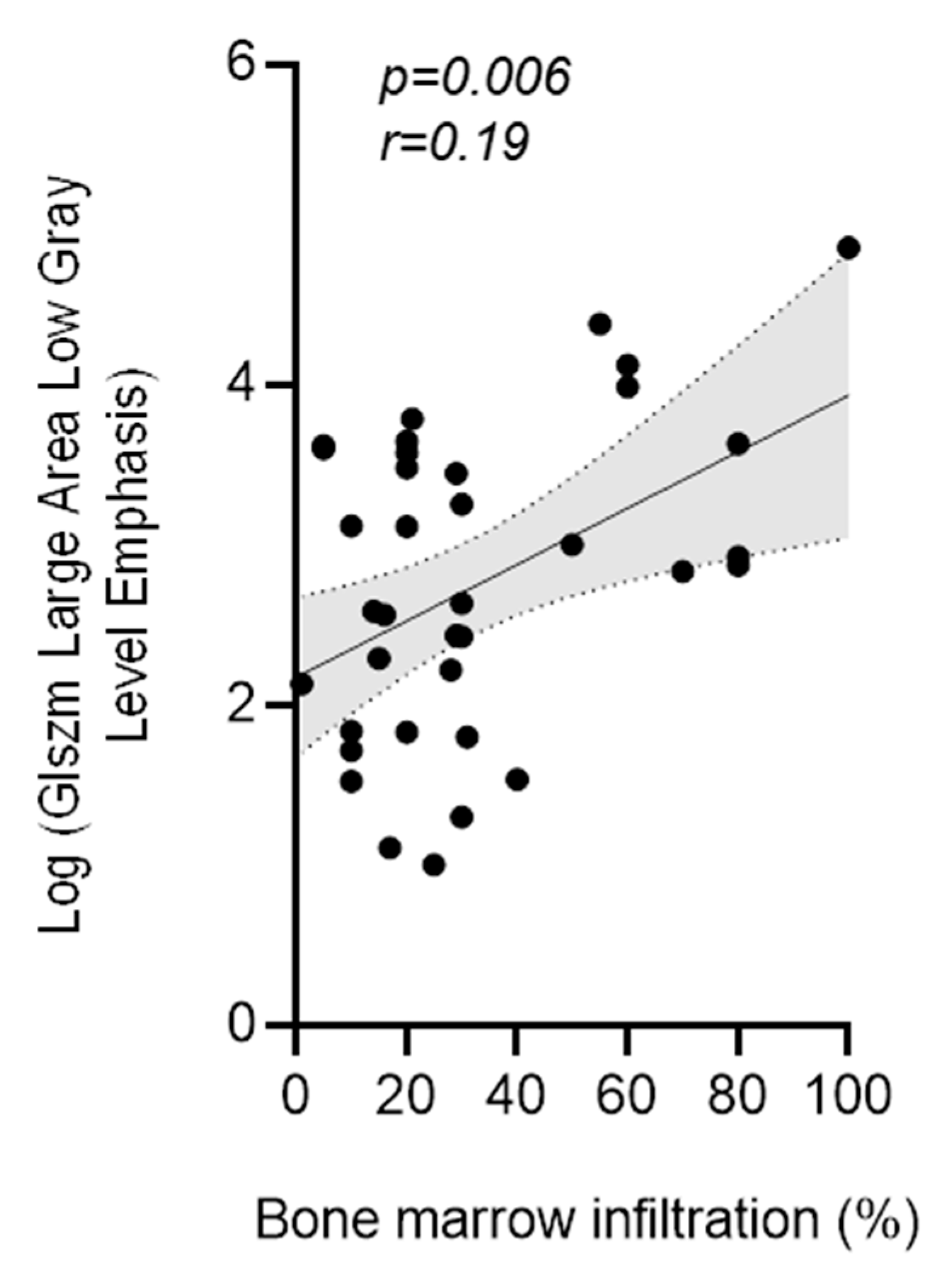
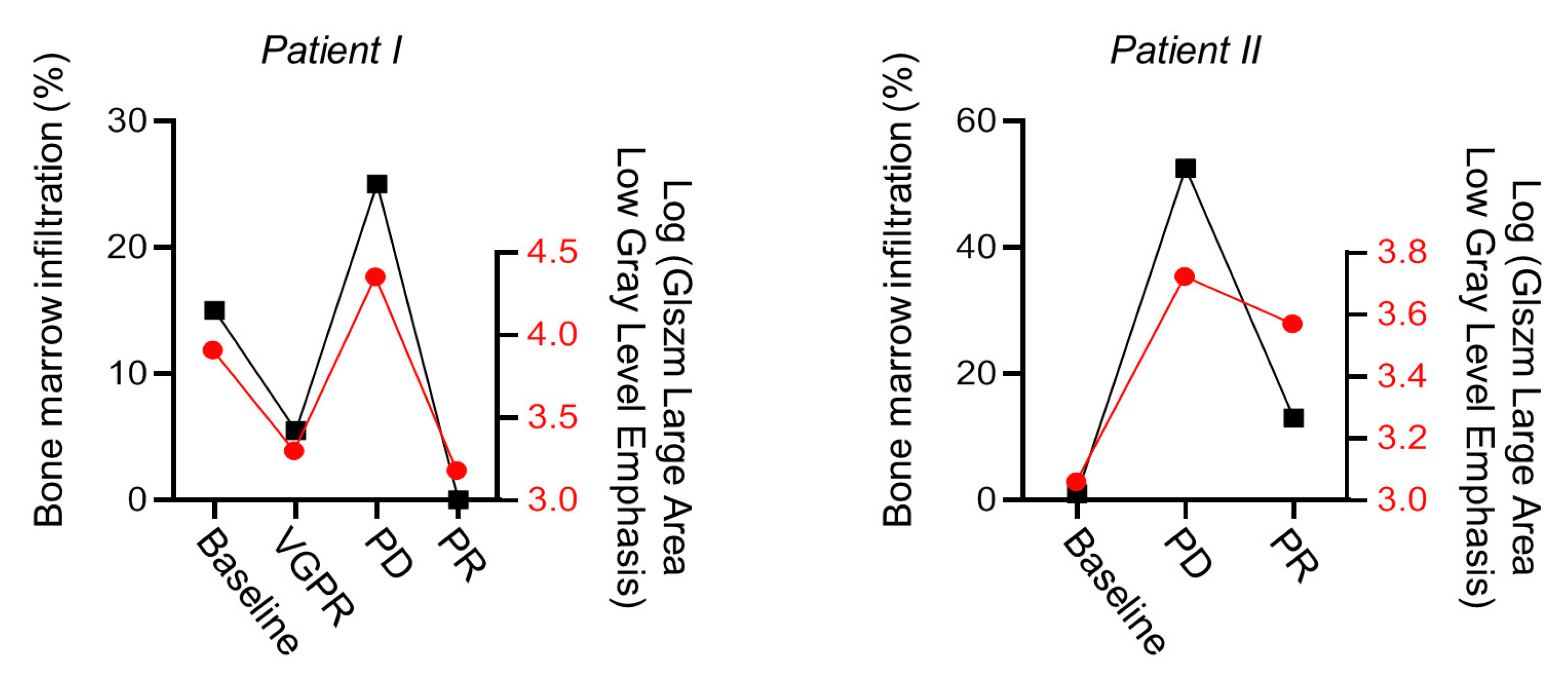
3.4. Correlation of MRI-Features with Biopsy Confirmed Degree of Myeloma Cell Infiltration
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Giralt, S.; Stadtmauer, E.A.; Harousseau, J.L.; Palumbo, A.; Bensinger, W.; Comenzo, R.L.; Kumar, S.; Munshi, N.C.; Dispenzieri, A.; Kyle, R.; et al. International myeloma working group (IMWG) consensus statement and guidelines regarding the current status of stem cell collection and high-dose therapy for multiple myeloma and the role of plerixafor (AMD 3100). Leukemia 2009, 23, 1904–1912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bataille, R.; Harousseau, J.L. Multiple myeloma. N. Engl. J. Med. 1997, 336, 1657–1664. [Google Scholar] [CrossRef]
- Panaroni, C.; Yee, A.J.; Raje, N. Myeloma and Bone Disease. Curr. Osteoporos. Rep. 2017, 15, 483–498. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, E.K.; Raje, N.S. Myeloma bone disease: Pathogenesis and treatment. Clin. Adv. Hematol. Oncol. 2017, 15, 285–295. [Google Scholar]
- Song, M.-K.; Chung, J.-S.; Lee, J.-J.; Min, C.-K.; Ahn, J.-S.; Lee, S.-M.; Shin, D.-Y.; Bae, S.-H.; Hong, J.; Lee, G.-W.; et al. Magnetic resonance imaging pattern of bone marrow involvement as a new predictive parameter of disease progression in newly diagnosed patients with multiple myeloma eligible for autologous stem cell transplantation. Br. J. Haematol. 2014, 165, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Lai, A.Y.T.; Riddell, A.; Barwick, T.; Boyd, K.; Rockall, A.; Kaiser, M.; Koh, D.-M.; Saffar, H.; Yusuf, S.; Messiou, C. Interobserver agreement of whole-body magnetic resonance imaging is superior to whole-body computed tomography for assessing disease burden in patients with multiple myeloma. Eur. Radiol. 2019, 30, 320–327. [Google Scholar] [CrossRef] [Green Version]
- Dupuis, M.M.; Tuchman, S. Non-secretory multiple myeloma: From biology to clinical management. Onco Targets Ther. 2016, 9, 7583–7590. [Google Scholar] [CrossRef] [Green Version]
- Ågren, B.; Rudberg, U.; Isberg, B.; Al, E. Mr imaging of multiple myeloma patients with bone-marrow transplants. Clin. Imaging 1998, 22, 382. [Google Scholar] [CrossRef]
- Durie, B.G.; Salmon, S.E. A clinical staging system for multiple myeloma. Correlation of measured myeloma cell mass with presenting clinical features, response to treatment, and survival. Cancer 1975, 36, 842–854. [Google Scholar] [CrossRef]
- Wale, A.; Pawlyn, C.; Kaiser, M.; Messiou, C. Frequency, distribution and clinical management of incidental findings and extramedullary plasmacytomas in whole body diffusion weighted magnetic resonance imaging in patients with multiple myeloma. Haematologica 2016, 101, e142–e144. [Google Scholar] [CrossRef] [Green Version]
- Shah, L.M.; Hanrahan, C.J. MRI of Spinal Bone Marrow: Part 1, Techniques and Normal Age-Related Appearances. Am. J. Roentgenol. 2011, 197, 1298–1308. [Google Scholar] [CrossRef] [PubMed]
- Dutoit, J.C.; Verstraete, K.L. Whole-body MRI, dynamic contrast-enhanced MRI, and diffusion-weighted imaging for the staging of multiple myeloma. Skelet. Radiol. 2017, 46, 733–750. [Google Scholar] [CrossRef] [PubMed]
- Meyer, H.-J.; Renatus, K.; Höhn, A.K.; Hamerla, G.; Schopow, N.; Fakler, J.; Josten, C.; Surov, A. Texture analysis parameters derived from T1-and T2-weighted magnetic resonance images can reflect Ki67 index in soft tissue sarcoma. Surg. Oncol. 2019, 30, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Zhu, H.; Qian, X.; Chen, N.; Lin, X.-Z. MRI Texture Analysis for Differentiating Nonfunctional Pancreatic Neuroendocrine Neoplasms from Solid Pseudopapillary Neoplasms of the Pancreas. Acad. Radiol. 2019, S1076-6332(19)30361-7. [Google Scholar] [CrossRef]
- Schick, U.; Lucia, F.; Dissaux, G.; Visvikis, D.; Badic, B.; Masson, I.; Pradier, O.; Bourbonne, V.; Hatt, M. MRI-derived radiomics: Methodology and clinical applications in the field of pelvic oncology. Br. J. Radiol. 2019, 92, 20190105. [Google Scholar] [CrossRef]
- Kumar, S.K.; Paiva, B.D.L.; Anderson, K.C.; Durie, B.; Landgren, O.; Moreau, P.; Munshi, N.V.; Lonial, S.; Bladé, J.; Mateos, M.-V.; et al. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol. 2016, 17, e328–e346. [Google Scholar] [CrossRef]
- Daffner, R.; Lupetin, A.; Dash, N.; Deeb, Z.; Sefczek, R.; Schapiro, R. MRI in the detection of malignant infiltration of bone marrow. Am. J. Roentgenol. 1986, 146, 353–358. [Google Scholar] [CrossRef]
- Baur, A.; Stäbler, A.; Nagel, D.; Lamerz, R.; Bartl, R.; Hiller, E.; Wendtner, C.; Bachner, F.; Reiser, M. Magnetic resonance imaging as a supplement for the clinical staging system of Durie and Salmon? Cancer 2002, 95, 1334–1345. [Google Scholar] [CrossRef]
- Wasser, K.; Moehler, T.; Nosas-Garcia, S.; Rehm, C.; Bartl, R.; Goldschmidt, H.; Düber, C.; Kauczor, H.U.; Delorme, S. [Correlation of MRI and histopathology of bone marrow in patients with multiple myeloma]. RoFo 2005, 177, 1116–1122. [Google Scholar] [CrossRef]
- Moulopoulos, L.A.; Dimopoulos, M.; Christoulas, D.; Kastritis, E.; Anagnostou, D.; Koureas, A.; Roussou, M.; Gavriatopoulou, M.; Migkou, M.; Iakovaki, M.; et al. Diffuse MRI marrow pattern correlates with increased angiogenesis, advanced disease features and poor prognosis in newly diagnosed myeloma treated with novel agents. Leukemia 2010, 24, 1206–1212. [Google Scholar] [CrossRef] [Green Version]
- Stecco, A.; Buemi, F.; Iannessi, A.; Carriero, A.; Gallamini, A. Current concepts in tumor imaging with whole-body MRI with diffusion imaging (WB-MRI-DWI) in multiple myeloma and lymphoma. Leuk. Lymphoma 2018, 59, 2546–2556. [Google Scholar] [CrossRef] [PubMed]
- Horger, M.; Weisel, K.; Horger, W.; Mroue, A.; Fenchel, M.; Lichy, M. Whole-Body Diffusion-Weighted MRI with Apparent Diffusion Coefficient Mapping for Early Response Monitoring in Multiple Myeloma: Preliminary Results. Am. J. Roentgenol. 2011, 196, W790–W795. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Huang, J.; Xu, W.-B.; Guan, Y.-J.; Ling, H.-W.; Mi, J.-Q.; Yan, H. Discriminating Depth of Response to Therapy in Multiple Myeloma Using Whole-body Diffusion-weighted MRI with Apparent Diffusion Coefficient. Acad. Radiol. 2018, 25, 904–914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giles, S.; Messiou, C.; Collins, D.; Morgan, V.A.; Simpkin, C.J.; West, S.; Davies, F.E.; Morgan, G.J.; DeSouza, N.M. Whole-Body Diffusion-weighted MR Imaging for Assessment of Treatment Response in Myeloma. Radiology 2014, 271, 785–794. [Google Scholar] [CrossRef] [Green Version]
- Morvan, L.; Carlier, T.; Jamet, B.; Bailly, C.; Bodet-Milin, C.; Moreau, P.; Kraeber-Bodéré, F.; Mateus, D. Leveraging RSF and PET images for prognosis of multiple myeloma at diagnosis. Int. J. Comput. Assist. Radiol. Surg. 2019, 15, 129–139. [Google Scholar] [CrossRef]







© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ekert, K.; Hinterleitner, C.; Baumgartner, K.; Fritz, J.; Horger, M. Extended Texture Analysis of Non-Enhanced Whole-Body MRI Image Data for Response Assessment in Multiple Myeloma Patients Undergoing Systemic Therapy. Cancers 2020, 12, 761. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12030761
Ekert K, Hinterleitner C, Baumgartner K, Fritz J, Horger M. Extended Texture Analysis of Non-Enhanced Whole-Body MRI Image Data for Response Assessment in Multiple Myeloma Patients Undergoing Systemic Therapy. Cancers. 2020; 12(3):761. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12030761
Chicago/Turabian StyleEkert, Kaspar, Clemens Hinterleitner, Karolin Baumgartner, Jan Fritz, and Marius Horger. 2020. "Extended Texture Analysis of Non-Enhanced Whole-Body MRI Image Data for Response Assessment in Multiple Myeloma Patients Undergoing Systemic Therapy" Cancers 12, no. 3: 761. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12030761