Episodic Breathlessness with and without Background Dyspnea in Advanced Cancer Patients Admitted to an Acute Supportive Care Unit


 and
and
Abstract
:1. Introduction
2. Patients and Methods (Ethical Code: n.1/2014)
2.1. Data Collection
2.2. Measurements
2.3. Statistical Analysis
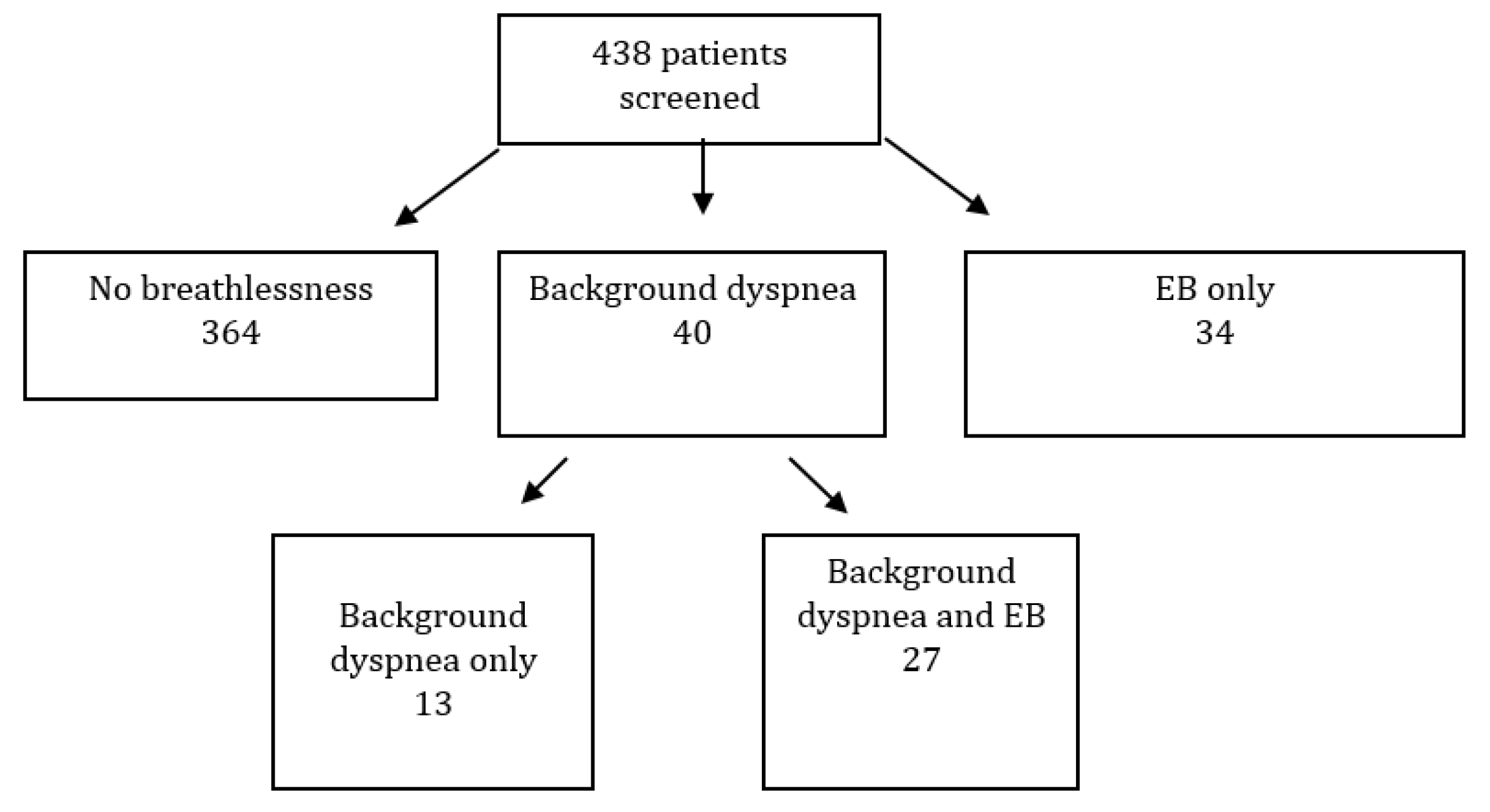
3. Results
3.1. Background Dyspnea
3.2. Episodic Breathlessness
4. Discussion
4.1. Background Dyspnea
4.2. Episodic Breathlessness
4.3. Triggers for Episodic Breathlessness
4.4. Episodic Breathlessness Intensity
4.5. Episodic Breathlessness Duration
4.6. Factors Associated with Continuous Dyspnea and Episodic Breathlessness
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Dudgeon, D.J.; Kristjanson, L.; Sloan, J.A.; Lertzman, M.; Clement, K. Dyspnea in cancer patients: Prevalence and associated factors. J. Pain Symptom Manag. 2001, 21, 92–95. [Google Scholar] [CrossRef]
- Bruera, E.; Schmitz, B.; Pither, J.; Neumann, C.M.; Hanson, J. The frequency and correlates of dyspnea in patients with advanced cancer. J. Pain Symptom Manag. 2000, 19, 357–362. [Google Scholar] [CrossRef]
- Mercadante, S. Episodic breathlessness in patients with advanced cancer: Characteristics and management. Drugs 2018, 78, 543–547. [Google Scholar] [CrossRef] [PubMed]
- Mercadante, S.; Portenoy, R.K. Breakthrough cancer pain: Twenty-five years of study. Pain 2016, 157, 2657–2663. [Google Scholar] [CrossRef] [PubMed]
- Simon, S.T.; Higginson, I.J.; Benalia, H.; Gysels, M.; Murtagh, F.E.; Spicer, J.; Bausewein, C. Episodic and continuous breathlessness: A new categorization of breathlessness. J. Pain Symptom Manag. 2013, 45, 1019–1029. [Google Scholar] [CrossRef] [PubMed]
- Simon, S.T.; Higginson, I.J.; Benalia, H.; Gysels, M.; Murtagh, F.E.; Spicer, J.; Bausewein, C. Episodes of breathlessness: Types and patterns—A qualitative study exploring experiences of patients with advanced diseases. Palliat. Med. 2013, 27, 524–532. [Google Scholar] [CrossRef] [Green Version]
- Simon, S.T.; Weingartner, V.; Higginson, I.J.; Voltz, R.; Bausewein, C. Definition, categorization, and terminology of episodic breathlessness: Consensus by an international Delphi survey. Pain Symptom Manag. 2014, 47, 828–838. [Google Scholar] [CrossRef]
- Mercadante, S.; Aielli, F.; Adile, C.; Valle, A.; Fusco, F.; Ferrera, P.; Caruselli, A.; Cartoni, C.; Marchetti, P.; Bellavia, G. Epidemiology and characteristics of episodic breathlessness in advanced cancer patients: An observational study. J. Pain Symptom Manag. 2016, 51, 17–24. [Google Scholar] [CrossRef] [Green Version]
- Mercadante, S.; Fusco, F.; Caruselli, A.; Cartoni, C.; Masedu, F.; Valenti, M.; Aielli, F. Background and episodic breathlessness in advanced cancer patients followed at home. Curr. Med. Res. Opin. 2017, 33, 155–160. [Google Scholar] [CrossRef]
- Mercadante, S.; Adile, C.; Caruselli, A.; Ferrera, P.; Costanzi, A.; Marchetti, P.; Casuccio, A. The palliative-supportive care unit in a comprehensive cancer center as crossroad for patients’ oncological pathway. PLoS ONE 2016, 11, e0157300. [Google Scholar] [CrossRef] [Green Version]
- Pirovano, M.; Maltoni, M.; Nanni, O.; Marinari, M.; Indelli, M.; Zaninetta, G.; Petrella, V.; Barni, S.; Zecca, E.; Scarpi, E.; et al. A new palliative prognostic score: A first step for the staging of terminally ill cancer patients. Italian multicenter and study group on palliative care. J. Pain Symptom Manag. 1999, 17, 231–239. [Google Scholar] [CrossRef]
- Hui, D.; Bruera, E. The Edmonton symptom assessment system 25 years later: Past, present, and future developments. J. Pain Symptom Manag. 2017, 53, 630–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banzett, R.B.; O’Donnell, C.R.; Guilfoyle, T.E.; Parshall, M.B.; Schwartzstein, R.M.; Meek, P.M.; Gracely, R.H.; Lansing, R.W. Multidimensional dyspnea profile: An instrument for clinical and laboratory research. Eur. Respir. J. 2015, 45, 1681–1691. [Google Scholar] [CrossRef]
- Ekström, M.; Bornefalk, H.; Sköld, M.; Janson, C.; Blomberg, A.; Sandberg, J.; Bornefalk-Hermansson, A.; Igelström, H.; Sundh, J. Validation of the Swedish multidimensional dyspnea profile (MDP) in outpatients with cardiorespiratory disease. BMJ Open Resp. Res. 2019, 6, e000381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, K.; Akechi, T.; Okuyama, Y.; Nishiwaki, Y. Impact of dyspnea, pain, and fatigue on daily life activities in ambulatory patients with advanced lung cancer. J. Pain Symptom Manag. 2002, 23, 417–423. [Google Scholar] [CrossRef]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. Athens insomnia scale: Validation of an instrument based on ICD-10 criteria. J. Psychosom. Res. 2000, 48, 555–560. [Google Scholar] [CrossRef]
- Snaith, R.P. The hospital anxiety and depression scale. Health Qual. Life Outcomes 2003, 1, 29. [Google Scholar] [CrossRef] [Green Version]
- Miriam, J.; Johnson, M.J.; Currow, D.C. Opioids for breathlessness: A narrative review. BMJ Support Palliat. Care 2020. [Google Scholar] [CrossRef]
- Mercadante, S.; Casuccio, A.; Fulfaro, F. The course of symptom frequency and intensity in advanced cancer patients followed at home. J Pain Symptom Manag. 2000, 20, 104–112. [Google Scholar] [CrossRef]
- Reddy, S.K.; Parsons, H.A.; Elsayem, A.; Palmer, J.L.; Bruera, E. Characteristics and correlates of dyspnea in patients with advanced cancer. J. Palliat. Med. 2009, 12, 29–36. [Google Scholar] [CrossRef]
- Weingärtner, V.; Bausewein, C.; Higginson, I.J.; Scheve, C.; Murtagh, F.E.; Voltz, R.; Simon, S.T. Characterizing episodic breathlessness in patients with advanced disease. J. Palliat. Med. 2013, 16, 1275–1279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weingärtner, V.; Scheve, C.; Gerdes, V.; Schwarz-Eywill, M.; Prenzel, R.; Otremba, B.; Mühlenbrock, J.; Bausewein, C.; Higginson, I.J.; Voltz, R.; et al. Characteristics of episodic breathlessness as reported by patients with advanced chronic obstructive pulmonary disease and lung cancer: Results of a descriptive cohort study. Palliat. Med. 2015, 29, 420–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charles, M.A.; Reymond, L.; Israel, F. Relief of incident dyspnea in palliative cancer patients: A pilot, randomized, controlled trial comparing nebulized hydromorphone, systemic hydromorphone, and nebulized saline. J. Pain Symptom Manag. 2008, 36, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Simon, S.T.; Kloke, M.; Alt-Epping, B.; Gärtner, J.; Hellmich, M.; Hein, R.; Piel, M.; Cornely, O.A.; Nauck, F.; Voltz, R. EffenDysd-fentanyl buccal tablet for the relief of episodic breathlessness in patients with advanced cancer: A multicenter, open-label, randomized, morphine-controlled, crossover, phase II trial. J. Pain Symptom Manag. 2016, 52, 617–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maddocks, M.; Taylor, V.; Klezlova, R. When will I get my breath back? Recovery time of exercise- induced breathlessness in patients with thoracic cancer. Lung Cancer 2012, 76, 128–129. [Google Scholar] [PubMed]
- Hui, D.; Hernandez, F.; Larsson, L.; Liu, D.; Kilgore, K.; Naberhuis, J.; Virgilio, A.; Reddy, S.; Reddy, A.; Dalal, S.; et al. Prophylactic fentanyl sublingual spray for episodic exertional dyspnea in cancer patients: A pilot double-blind randomized controlled trial. J. Pain Symptom Manag. 2019, 58, 605–613. [Google Scholar] [CrossRef]
- Hui, D.; Kilgore, K.; Frisbee-Hume, S.; Park, M.; Liu, D.; Balachandran, D.D.; Bruera, E. Effect of prophylactic fentanyl buccal tablet on episodic exertional dyspnea: A pilot double-blind randomized controlled trial. J. Pain Symptom Manag. 2017, 54, 798–805. [Google Scholar] [CrossRef] [Green Version]
- Hui, D.; Kilgore, K.; Park, M.; Williamns, J.; Liu, D.; Bruera, E. Impact of prophylactic fentanyl pectin nasal spray on exercise-induced episodic dyspnea in cancer patients: A double-blind, randomized controlled trial. J. Pain Symptom Manag. 2016, 52, 459–468. [Google Scholar] [CrossRef] [Green Version]
- Hui, D.; Xu, A.; Frisbee-Hume, S.; Chisholm, G.; Morgado, M.; Reddy, S.; Bruera, E. Effects of prophylactic subcutaneous fentanyl on exercise-induced breakthrough dyspnea in cancer patients: A preliminary double-blind, randomized, controlled trial. J. Pain Symptom Manag. 2014, 47, 209–217. [Google Scholar] [CrossRef]
- Simon, S.T.; Weingärtner, V.; Higginson, I.J.; Benalia, H.; Gysels, M.; Murtagh, F.E.; Spicer, J.; Linde, P.; Voltz, R.; Bausewein, C. “I Can Breathe Again!” Patients’ self-management strategies for episodic breathlessness in advanced disease, derived from qualitative interviews. J. Pain Symptom Manag. 2016, 52, 228–234. [Google Scholar] [CrossRef]


{kind=link}
| No Dyspnea N° 398 | Dyspnea N° 40 | ||||
|---|---|---|---|---|---|
| Age | ≤65 years | 200 (93.5%) | 14 (6.5%) | p = 0.189 | |
| 66–75 years | 129 (88.4%) | 17 (11.6%) | |||
| 76–85 years | 59 (86.8%) | 9 (13.2%) | |||
| ≥85 years | 7 (100%) | 0 (0%) | |||
| Gender | Male | 207 (91.6%) | 19 (8.4%) | p = 0.621 | |
| Female | 191 (90.1%) | 21 (9.9%) | |||
| Cancer | Lung | 75 (75.8%) | 24 (24.2%) | p < 0.0005 | |
| Breast | 46 (88.5%) | 6 (11.5%) | |||
| Gastrointestinal | 101 (98.1%) | 2 (1.9%) | |||
| Liver | 15 (100%) | 0 (0%) | |||
| Gynecological | 22 (91.7%) | 2 (8.3%) | |||
| Head-Neck | 14 (87.5%) | 2 (12.5%) | |||
| Haematological | 7 (100%) | 0 (0%) | |||
| Prostate | 17 (100%) | 0 (0%) | |||
| Pancreas | 47 (100%) | 0 (0%) | |||
| Urological | 25 (92.6%) | 2(7.4%) | |||
| Other | 25 (92.6%) | 2 (7.4%) | |||
| Unknown | 4 (100%) | 0 (0%) | |||
| Comorbidity | Cardiovascular | Yes | 188 (88.7%) | 24 (11.3%) | p = 0.166 |
| No | 174 (93.0%) | 13 (7.0%) | |||
| Bronco-pulmunary | Yes | 33 (75.0%) | 11 (58.0%) | p = 0.010 | |
| No | 329 (89.9%) | 37 (10.1%) | |||
| Kidney disease | Yes | 12 (85.7%) | 2 (14.3%) | p = 0.379 | |
| No | 350 (90.9%) | 35 (9.1%) | |||
| Liver disease | Yes | 9 (100%) | 0 (62.5%) | p = 1.0 | |
| No | 353 (90.5%) | 37 (9.5%) | |||
| None | 120/398 (30.2%) | 6/40 (15.0) | p = 0.032 | ||
| Treatment | Disease-oriented | 264 (92.6%) | 22 (7.4%) | p = 0.165 | |
| Palliative Care | 6 (22.2%) | 21 (77.8%) | p = <0.0005 |
| Mean | SD | |
|---|---|---|
| Pain | 3.83 | 3.094 |
| Weakness | 6.56 | 2.349 |
| Nausea | 1.86 | 2.754 |
| Depression | 3.78 | 3.283 |
| Anxiety | 4.33 | 3.152 |
| Drowsiness | 4.86 | 3.042 |
| Dyspnea | 4.71 | 3.126 |
| Poor sleep | 4.41 | 3.426 |
| Poor appetite | 4.41 | 3.646 |
| Poor well-being | 5.43 | 2.798 |
| Total | 43.87 | 16.996 |
| Background Dyspnea Only (13 pts) | Background and EB (27 pts) | EB Only (34 pts) | |||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||
| MDP effort | 3.83 | 3.433 | 7.16 | 1.818 | 5.29 | 2.452 | 0.0003 A vs. B 0.002 C vs. B |
| MDP unpleasantness | 4.50 | 2.876 | 7.69 | 1.463 | 5.84 | 2.541 | <0.0005 A vs. B 0.001 C vs. B |
| MDP quality-intensity | 18.17 | 14.534 | 27.40 | 8.124 | 21.53 | 12.371 | 0.014 A vs. B 0.038 C vs. B |
| MDP emotional | 15.33 | 13.255 | 22.00 | 14.547 | 18.55 | 13.994 | NS |
| BDI | 32.58 | 15.635 | 42.70 | 11.671 | 34.19 | 17.610 | 0.027 A vs. B 0.035 C vs. B |
| ASS | 9.17 | 5.006 | 9.81 | 3.962 | 8.59 | 5.200 | NS |
| HADS-A | 8.20 | 3.458 | 9.00 | 4.287 | 8.88 | 3.951 | NS |
| HADS-D | 8.20 | 2.658 | 8.91 | 3.146 | 10.12 | 4.512 | NS |
| TOTAL HADS | 16.40 | 5.680 | 17.91 | 6.886 | 19.00 | 6.468 | NS |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mercadante, S.; Adile, C.; Ferrera, P.; Bonanno, G.; Restivo, V.; Casuccio, A. Episodic Breathlessness with and without Background Dyspnea in Advanced Cancer Patients Admitted to an Acute Supportive Care Unit. Cancers 2020, 12, 2102. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12082102
Mercadante S, Adile C, Ferrera P, Bonanno G, Restivo V, Casuccio A. Episodic Breathlessness with and without Background Dyspnea in Advanced Cancer Patients Admitted to an Acute Supportive Care Unit. Cancers. 2020; 12(8):2102. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12082102
Chicago/Turabian StyleMercadante, Sebastiano, Claudio Adile, Patrizia Ferrera, Giuseppe Bonanno, Vincenzo Restivo, and Alessandra Casuccio. 2020. "Episodic Breathlessness with and without Background Dyspnea in Advanced Cancer Patients Admitted to an Acute Supportive Care Unit" Cancers 12, no. 8: 2102. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12082102