How Should We Assign Large Infiltrative Hepatocellular Carcinomas for Staging?

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Patient Selection
2.2. Clinical Findings
2.3. Imaging Findings
2.4. Pathologic Findings
2.5. Staging System
2.6. Statistical Analysis
3. Results
3.1. Baseline Clinical and Tumor Characteristics
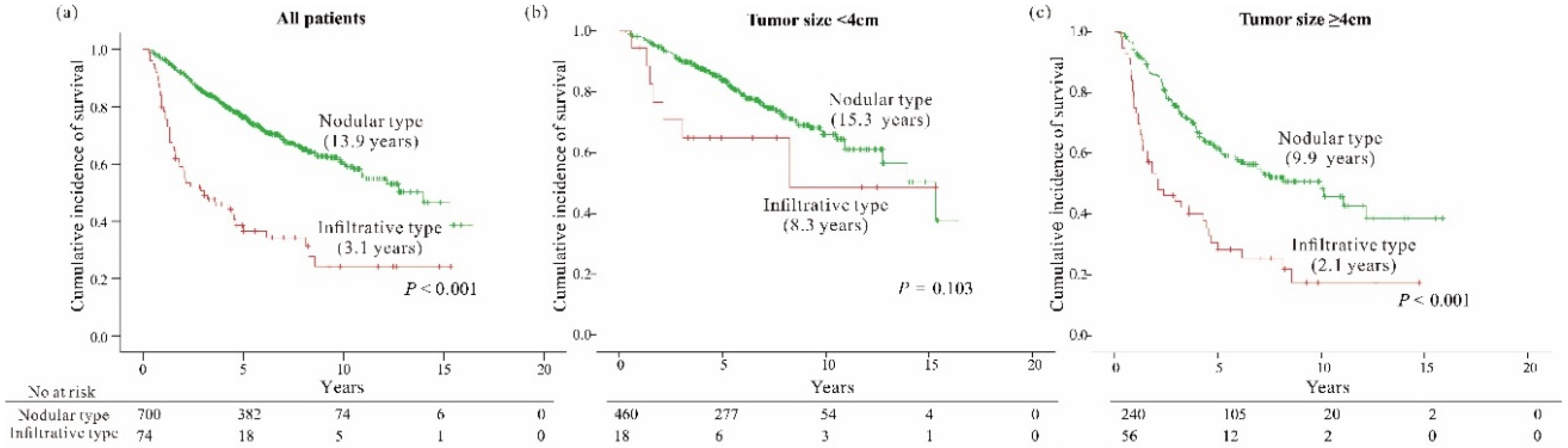
3.2. Clinical Characteristics According to the Gross Morphology of HCC: Infiltrative vs. Nodular Type
3.3. Tumor Factors Associated with OverAll Survival
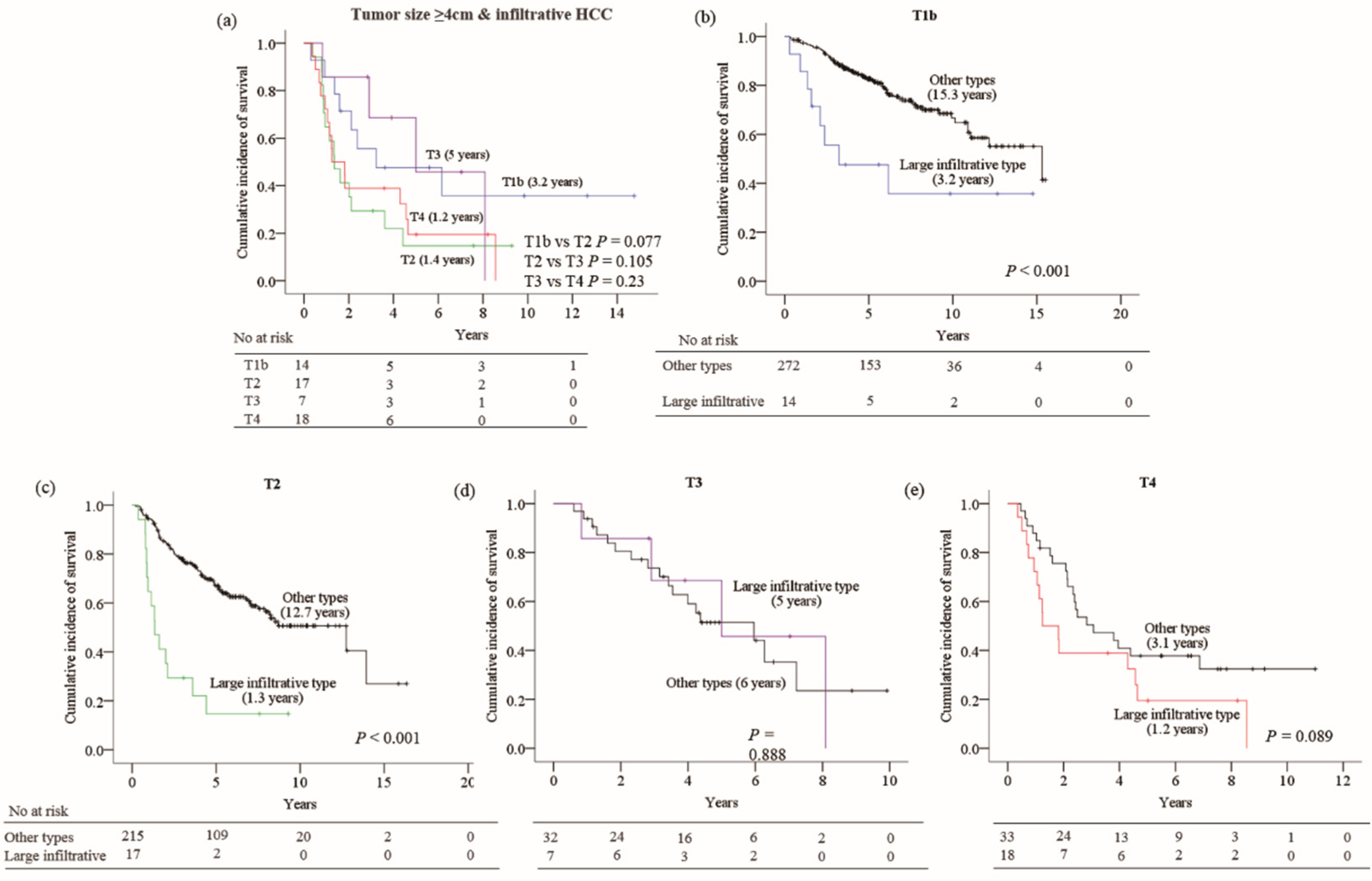
3.4. Impact of Large Infiltrative Type HCC on Current Staging Systems
3.5. The Effect of the Modification of Staging Rule for Large Infiltrative HCCs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef]
- Forner, A.; Llovet, J.M.; Bruix, J. Hepatocellular carcinoma. Lancet 2012, 379, 1245–1255. [Google Scholar] [CrossRef]
- Shindoh, J.; Andreou, A.; Aloia, T.A.; Zimmitti, G.; Lauwers, G.Y.; Laurent, A.; Nagorney, D.M.; Belghiti, J.; Cherqui, D.; Poon, R.T.; et al. Microvascular invasion does not predict long-term survival in hepatocellular carcinoma up to 2 cm: Reappraisal of the staging system for solitary tumors. Ann. Surg. Oncol. 2013, 20, 1223–1229. [Google Scholar] [CrossRef] [PubMed]
- Kamarajah, S.K.; Frankel, T.L.; Sonnenday, C.; Cho, C.S.; Nathan, H. Critical evaluation of the American Joint Commission on Cancer (AJCC) 8th edition staging system for patients with Hepatocellular Carcinoma (HCC): A Surveillance, Epidemiology, End Results (SEER) analysis. J. Surg. Oncol. 2018, 117, 644–650. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Bru, C.; Bruix, J. Prognosis of hepatocellular carcinoma: The BCLC staging classification. Semin. Liver Dis. 1999, 19, 329–338. [Google Scholar] [CrossRef]
- Nakashima, T.; Kojiro, M. Hepatocellular Carcinoma and Multiple Cancer. In Hepatocellular Carcinoma; Springer: Tokyo, Japan, 1987. [Google Scholar] [CrossRef]
- Benvegnu, L.; Noventa, F.; Bernardinello, E.; Pontisso, P.; Gatta, A.; Alberti, A. Evidence for an association between the aetiology of cirrhosis and pattern of hepatocellular carcinoma development. Gut 2001, 48, 110–115. [Google Scholar] [CrossRef] [Green Version]
- Kneuertz, P.J.; Demirjian, A.; Firoozmand, A.; Corona-Villalobos, C.; Bhagat, N.; Herman, J.; Cameron, A.; Gurakar, A.; Cosgrove, D.; Choti, M.A.; et al. Diffuse infiltrative hepatocellular carcinoma: Assessment of presentation, treatment, and outcomes. Ann. Surg. Oncol. 2012, 19, 2897–2907. [Google Scholar] [CrossRef] [Green Version]
- Eggel, H. Uber das primare Carcinom der Leber. Beitr. Pathol. Anat. Allg. Pathol. 1901, 30, 506–604. [Google Scholar]
- Liver Cancer Study Group of Japan. The general rules for the clinical and pathological study of primary liver cancer. Jpn. J. Surg. 1989, 19, 98–129. [Google Scholar] [CrossRef]
- Mehta, N.; Fidelman, N.; Sarkar, M.; Yao, F.Y. Factors associated with outcomes and response to therapy in patients with infiltrative hepatocellular carcinoma. Clin. Gastroenterol. Hepatol. 2013, 11, 572–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruix, J.; Sherman, M.; Llovet, J.M.; Beaugrand, M.; Lencioni, R.; Burroughs, A.K.; Christensen, E.; Pagliaro, L.; Colombo, M.; Rodes, J.; et al. Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL conference. European Association for the Study of the Liver. J. Hepatol. 2001, 35, 421–430. [Google Scholar] [CrossRef]
- Bruix, J.; Sherman, M.; Practice Guidelines Committee; American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma. Hepatology (Baltimore, Md.) 2005, 42, 1208–1236. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Sherman, M.; American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma: An update. Hepatology (Baltimore, Md.) 2011, 53, 1020–1022. [Google Scholar] [CrossRef] [PubMed]
- Jang, J.Y.; Lee, J.S.; Kim, H.-J.; Shim, J.-J.; Kim, J.H.; Kim, B.H.; Kwon, C.H.; Lee, S.D.; Lee, H.W.; Kim, J.H.; et al. The general rules for the study of primary liver cancer. J. Liver Cancer 2017, 17, 19–44. [Google Scholar] [CrossRef] [Green Version]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Stone, M.; Criteria, A.; Armitage, P.; Colton, T. (Eds.) Encyclopedia of Biostatistics; Wiley: Chichester, UK, 1998; pp. 123–124. [Google Scholar]
- Frank, E.H.J. Harrell Miscellaneous. R Package Version 3.9-2. Available online: https://CRAN.R-project.org/package=Hmisc (accessed on 10 February 2012).
- Trevisani, F.; Caraceni, P.; Bernardi, M.; D’Intino, P.E.; Arienti, V.; Amorati, P.; Stefanini, G.F.; Grazi, G.; Mazziotti, A.; Fornalè, L. Gross pathologic types of hepatocellular carcinoma in Italian patients. Relationship with demographic, environmental, and clinical factors. Cancer 1993, 72, 1557–1563. [Google Scholar] [CrossRef]
- Kanematsu, M.; Semelka, R.C.; Leonardou, P.; Mastropasqua, M.; Lee, J.K.T. Hepatocellular carcinoma of diffuse type: MR imaging findings and clinical manifestations. J. Magn. Reson. Imaging 2003, 18, 189–195. [Google Scholar] [CrossRef]
- Reynolds, A.R.; Furlan, A.; Fetzer, D.T.; Sasatomi, E.; Borhani, A.A.; Heller, M.T.; Tublin, M.E. Infiltrative hepatocellular carcinoma: What radiologists need to know. Radiographics 2015, 35, 371–386. [Google Scholar] [CrossRef]
- Demirjian, A.; Peng, P.; Geschwind, J.F.; Cosgrove, D.; Schutz, J.; Kamel, I.R.; Pawlik, T.M. Infiltrating hepatocellular carcinoma: Seeing the tree through the forest. J. Gastrointest Surg. 2011, 15, 2089–2097. [Google Scholar] [CrossRef] [Green Version]
- Yan, X.; Fu, X.; Deng, M.; Chen, J.; He, J.; Shi, J.; Qiu, Y. Infiltrative Hepatocellular Carcinoma: Assessment of Factors Associated with Outcomes in Patients Undergoing Hepatectomy. Medicine 2016, 95, e3589. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total | Infiltrative Type | Nodular Types | p-Value | |
|---|---|---|---|---|---|
| Number of patients | 774 | 74 (9.6) | 700 (90.4) | ||
| Clinical factors | |||||
| Age >60 years, n (%) | 312 (40.3) | 28 (37.8) | 284 (40.6) | 0.648 | |
| Male, n (%) | 607 (78.4) | 57 (77) | 550 (78.6) | 0.759 | |
| Etiologies | |||||
| HBV | 601 (77.6) | 58 (78.4) | 543 (77.6) | 0.138 | |
| HCV | 48 (6.2) | 1 (1.4) | 47 (6.7) | ||
| Alcoholic | 67 (8.7) | 6 (8.1) | 61 (8.7) | ||
| Cryptogenic | 58 (7.5) | 9 (12.2) | 49 (7) | ||
| Laboratory findings | |||||
| ALT, IU/L | 33 (6–413) | 38 (6–166) | 33 (6–413) | 0.244 | |
| AST, IU/L | 36 (9–374) | 38 (16–318) | 35 (9–374) | 0.34 | |
| Albumin, g/dL | 4.2 (2.8–5.1) | 4.1 (3.1–5.1) | 4.2 (2.8–5.0) | 0.069 | |
| Total bilirubin, mg/dL | 0.69 (0.1–9.8) | 0.80 (0.3–9.78) | 0.68 (0.1–3.69) | 0.01 | |
| PT INR | 1.04 (0.71–1.78) | 1.04 (0.76–1.4) | 1.04 (0.71–1.78) | 0.76 | |
| AFP >20 ng/mL (n = 752) | 367 (48.7) | 52 (71.2) | 315 (46.3) | <0.001 | |
| PIVKA-II >50 mAU/mL (n = 606) | 322 (53.1) | 46 (80.7) | 276 (50.3) | <0.001 | |
| Child-Pugh grade | |||||
| A | 757 (97.8) | 71 (95.9) | 686 (98) | 0.252 | |
| B | 17 (2.2) | 3 (4.1) | 14 (2) | ||
| Tumor factors | |||||
| No. of tumors, n (%) | |||||
| Unifocal | 607 (78.4) | 48 (64.9) | 559 (79.9) | 0.003 | |
| Multifocal | 167 (21.6) | 26 (35.1) | 141 (20.1) | ||
| Tumor size, n (%) | |||||
| <4 cm | 478 (61.8) | 18 (24.3) | 460 (65.7) | <0.001 | |
| ≥4 cm | 296 (38.2) | 56 (75.7) | 240 (34.3) | ||
| Vessel invasion, n (%) | |||||
| None | 515 (66.5) | 23 (31.1) | 492 (70.3) | <0.001 | |
| Micro | 219 (28.3) | 34 (45.9) | 185 (26.4) | ||
| Major | 40 (5.2) | 17 (23) | 23 (3.3) | ||
| AJCC 8th T-stage, n (%) | |||||
| 1a | 166 (21.4) | 2 (2.7) | 164 (23.4) | <0.001 | |
| 1b | 286 (37) | 17 (23) | 269 (38.4) | ||
| 2 | 232 (30) | 28 (37.8) | 204 (29.1) | ||
| 3 | 39 (5) | 7 (9.5) | 32 (4.6) | ||
| 4 | 51 (6.6) | 20 (27) | 31 (4.4) | ||
| BCLC, n (%) | |||||
| (Number of patients) | 774 | 69 (8.9) | 705 (91.1) | ||
| 0 | 166 (21.4) | 0 | 166 (23.5) | <0.001 | |
| A | 475 (61.4) | 40 (58) | 435 (61.7) | ||
| B | 86 (11.1) | 10 (14.5) | 76 (10.8) | ||
| C | 47 (6.1) | 19 (27.5) | 28 (4) | ||
| Variables | Univariate Analysis | Multivariate Analysis | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| HR (95% CI) | p | Model 1 | Model 2 | Model 3 | ||||||
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |||||
| All patients | ||||||||||
| Clinical factors | ||||||||||
| Age >60 years | 1.043 (0.812–1.339) | 0.742 | ||||||||
| Male | 1.485 (1.067–2.067) | 0.019 | 1.358 (0.973–1.896) | 0.072 | ||||||
| Etiologies | ||||||||||
| HBV | – | 0.023 | ||||||||
| HCV | 1.303 (0.792–2.142) | 0.297 | 0.507 | |||||||
| Alcoholic | 1.733 (1.184–2.536) | 0.005 | ||||||||
| Cryptogenic | 1.37 (0.888–2.113) | 0.154 | ||||||||
| Laboratory findings | ||||||||||
| Albumin >4 g/dL | 0.513 (0.402–0.655) | <0.001 | 0.588 (0.458–0.756) | <0.001 | ||||||
| Total bilirubin >1 mg/dL | 1.153 (0.85–1.563) | 0.36 | ||||||||
| INR >1 | 1.286 (0.977–1.692) | 0.073 | 1.319 (0.996–1.748) | 0.050 | ||||||
| Tumor factors | ||||||||||
| Tumor size, ≥4 cm | 2.545 (1.992–3.251) | <0.001 | 1.836 (1.405–2.399) | <0.001 | ||||||
| Infiltrative vs. nodular types | 3.28 (2.394–4.494) | <0.001 | 2.035 (1.456–2.845) | <0.001 | ||||||
| Multifocal vs unifocal | 2.164 (1.661–2.819) | <0.001 | 1.503 (1.133–1.994) | 0.005 | ||||||
| Presence of vessel invasion | ||||||||||
| None | – | <0.001 | <0.001 | |||||||
| Micro | 2.159 (1.662–2.804) | <0.001 | 1.669 (1.267–2.198) | <0.001 | ||||||
| Major | 5.686 (3.833–8.434) | <0.001 | 2.372 (1.523–3.693) | <0.001 | ||||||
| Tumor size <4 cm group | ||||||||||
| Clinical factors | ||||||||||
| Male | 1.75 (1.032–2.967) | 0.038 | 1.629 (0.955–2.778) | 0.073 | 1.652 (0.97–2.812) | 0.065 | 1.602 (0.94–2.729) | 0.083 | ||
| Laboratory findings | ||||||||||
| Albumin >4 g/dL | 0.513 (0.355–0.74) | <0.001 | 0.597 (0.409–0.872) | 0.008 | 0.597 (0.409–0.873) | 0.008 | 0.585 (0.401–0.855) | 0.006 | ||
| PT INR >1 | 1.96 (1.21–3.173) | 0.006 | 1.7 (1.04–2.779) | 0.034 | 1.752 (1.07–2.869) | 0.026 | 1.791 (1.093–2.935) | 0.021 | ||
| Tumor factors | ||||||||||
| Tumor size, >2 cm | 1.795 (1.199–2.686) | 0.004 | 1.49 (0.983–2.257) | 0.06 | ||||||
| Infiltrative type vs. others | 1.879 (0.87–4.06) | 0.109 | ||||||||
| Multifocal vs unifocal | 1.561 (0.988–2.465) | 0.056 | 0.176 | |||||||
| Presence of vessel invasion | ||||||||||
| None | - | <0.001 | 0.004 | |||||||
| Micro | 1.461 (0.956–2.231) | 0.079 | 1.399 (0.91–2.151) | 0.126 | ||||||
| Major | 7.031 (3.048–16.22) | <0.001 | 3.995 (1.688–9.458) | 0.002 | ||||||
| AJCC 8th T-stage | ||||||||||
| T1a | - | <0.001 | - | <0.001 | ||||||
| T1b | 1.425 (0.887–2.289) | 0.143 | 1.274 (0.79–2.056) | 0.321 | ||||||
| T2 | 2.036 (1.262–3.285) | 0.004 | 1.968 (1.217–3.182) | 0.006 | ||||||
| T4 | 9.17 (3.782–22.234) | <0.001 | 5.613 (2.26–13.941) | <0.001 | ||||||
| BCLC stage | ||||||||||
| 0 | – | <0.001 | - | <0.001 | ||||||
| A | 1.52 (0.985–2.344) | 0.058 | 1.39 (0.899–2.151) | 0.139 | ||||||
| B | 3.959 (2.016–7.772) | <0.001 | 4.134 (2.096–8.156) | <0.001 | ||||||
| C | 9.199 (3.794-22.304) | <0.001 | 5.597 (2.255–13.894) | <0.001 | ||||||
| Tumor size ≥4 cm group | ||||||||||
| Laboratory findings | ||||||||||
| Albumin >4 g/dL | 0.543 (0.39–0.755) | <0.001 | 0.6 (0.429–0.838) | 0.003 | 0.592 (0.423–0.828) | 0.002 | 0.581 (0.416–0.811) | 0.001 | ||
| Tumor factors | ||||||||||
| Size >5 cm | 1.598 (1.109–2.303) | 0.012 | 0.614 | |||||||
| Infiltrative type vs. others | 2.581 (1.793–3.715) | <0.001 | 2.181 (1.496–3.181) | <0.001 | 2.318 (1.585–3.39) | <0.001 | 2.301 (1.578–3.357) | <0.001 | ||
| Multifocal vs unifocal | 1.978 (1.408–2.779) | <0.001 | 1.517 (1.063–2.165) | 0.022 | ||||||
| Presence of vessel invasion | ||||||||||
| None | <0.001 | 0.001 | ||||||||
| Micro | 2.098 (1.448–3.038) | <0.001 | 1.838 (1.258–2.686) | 0.002 | ||||||
| Major | 3.655 (2.245–5.951) | <0.001 | 2.271 (1.345–3.834) | 0.002 | ||||||
| AJCC 8th T-stage | ||||||||||
| T1b | – | <0.001 | <0.001 | |||||||
| T2 | 2.43 (1.58-3.738) | <0.001 | 2.442 (1.588–3.756) | <0.001 | ||||||
| T3 | 2.348 (1.35–4.084) | 0.003 | 2.014 (1.155–3.512) | 0.014 | ||||||
| T4 | 3.153 (2.13–5.796) | <0.001 | 2.476 (1.473–4.16) | 0.001 | ||||||
| BCLC stage | ||||||||||
| A | – | <0.001 | <0.001 | |||||||
| B | 1.913 (1.288–2.842) | 0.001 | 2.115 (1.415–3.161) | <0.001 | ||||||
| C | 3.571 (2.341–5.448) | <0.001 | 2.753 (1.786–4.242) | <0.001 | ||||||
| Staging System | AIC | C-Index | LHRχ2 |
|---|---|---|---|
| Original AJCC 8th T-stage | 3108.946 | 0.673 (0.642–0.704) | 87.73 (<0.001) |
| T3 modified T-stage | 3090.167 | 0.692 (0.661–0.724) * | 106.52 (<0.001) |
| T4 modified T-stage | 3088.784 | 0.693 (0.662–0.725) * | 107.89 (<0.001) |
| Original BCLC stage | 3088.764 | 0.667 (0.637–0.696) | 105.82 (<0.001) |
| Modified BCLC stage | 3069.662 | 0.686 (0.656–0.716) * | 125.02 (<0.001) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.J.; Lee, Y.R.; Seo, C.G.; Goh, H.G.; Kim, T.H.; Yim, S.Y.; Han, N.Y.; Lee, J.M.; Choi, H.S.; Kim, E.S.; et al. How Should We Assign Large Infiltrative Hepatocellular Carcinomas for Staging? Cancers 2020, 12, 2589. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12092589
Lee YJ, Lee YR, Seo CG, Goh HG, Kim TH, Yim SY, Han NY, Lee JM, Choi HS, Kim ES, et al. How Should We Assign Large Infiltrative Hepatocellular Carcinomas for Staging? Cancers. 2020; 12(9):2589. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12092589
Chicago/Turabian StyleLee, Yoo Jin, Yoo Ra Lee, Chung Gyo Seo, Hyun Gil Goh, Tae Hyung Kim, Sun Young Yim, Na Yeon Han, Jae Min Lee, Hyuk Soon Choi, Eun Sun Kim, and et al. 2020. "How Should We Assign Large Infiltrative Hepatocellular Carcinomas for Staging?" Cancers 12, no. 9: 2589. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12092589