Prognostic Inflammatory Index Based on Preoperative Peripheral Blood for Predicting the Prognosis of Colorectal Cancer Patients

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Identification of the PII and the Optimal Cut-Off Value
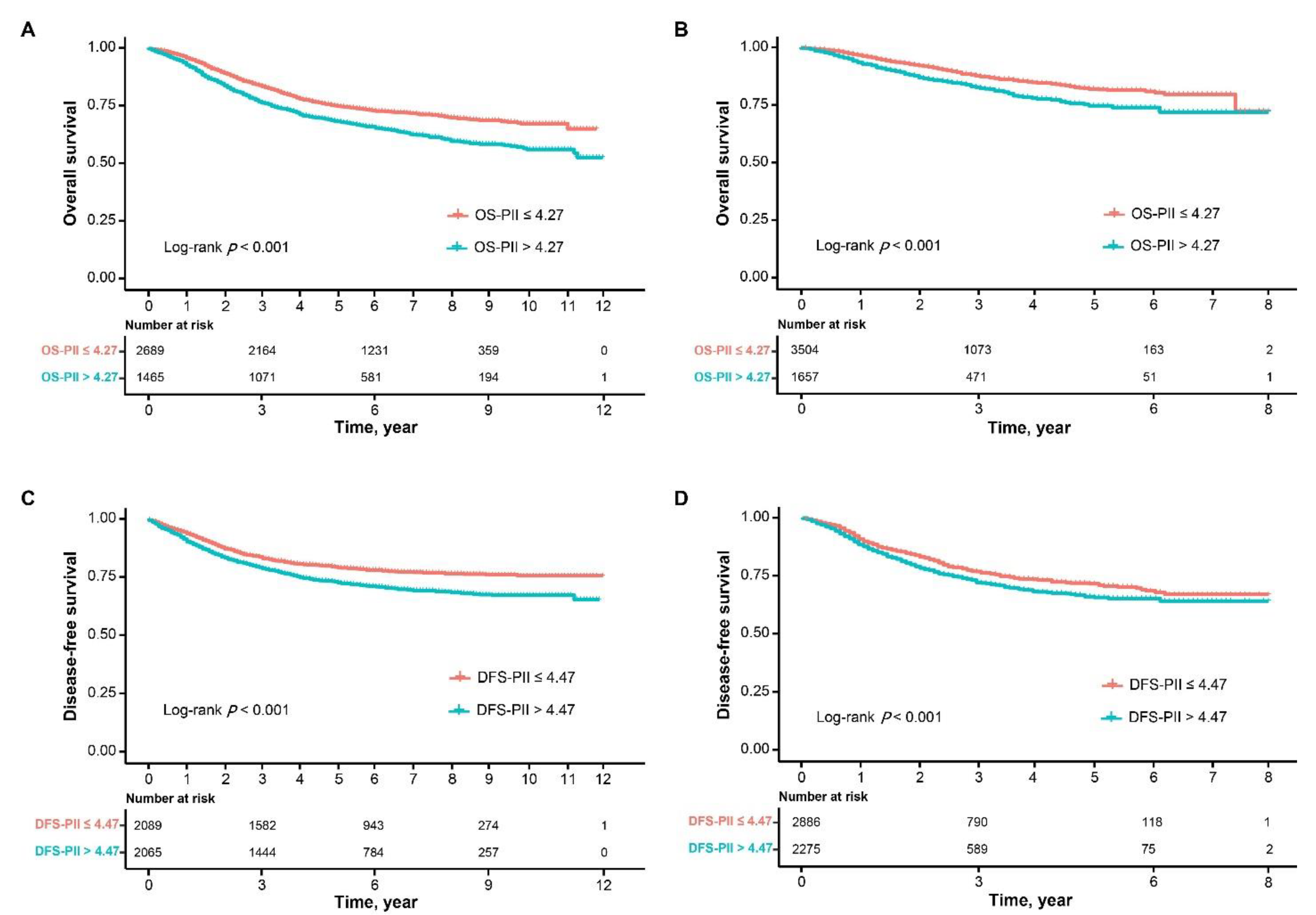
2.3. Prognostic Value of OS-PII and DFS-PII in the Training Cohort
2.4. Prognostic Value of OS-PII and DFS-PII in the Validation Cohort
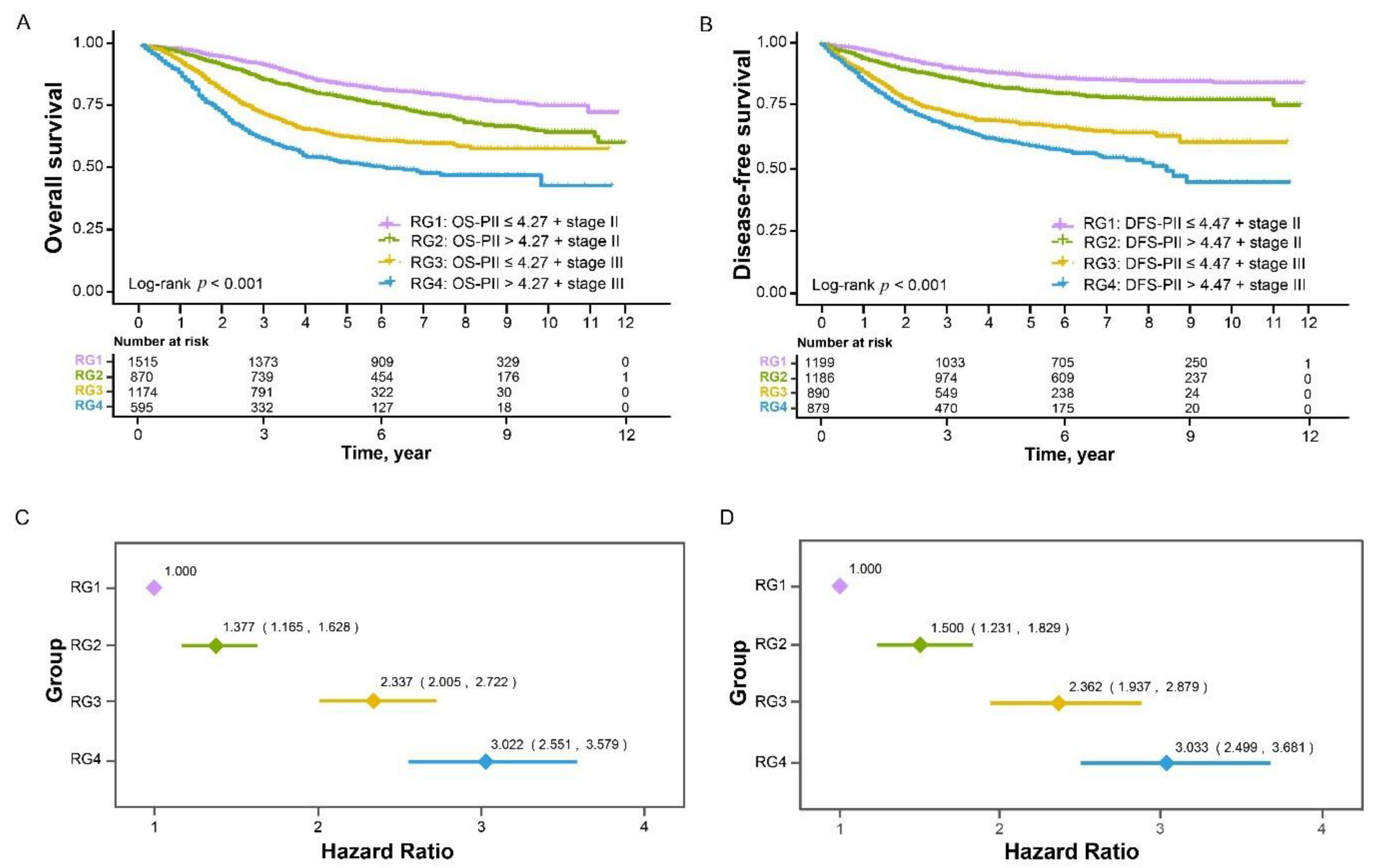
2.5. Prognostic Value of Different Combinations of PIIs and TNM Staging
2.6. Prognostic Effects of OS-PII and DFS-PII in Different Subgroups
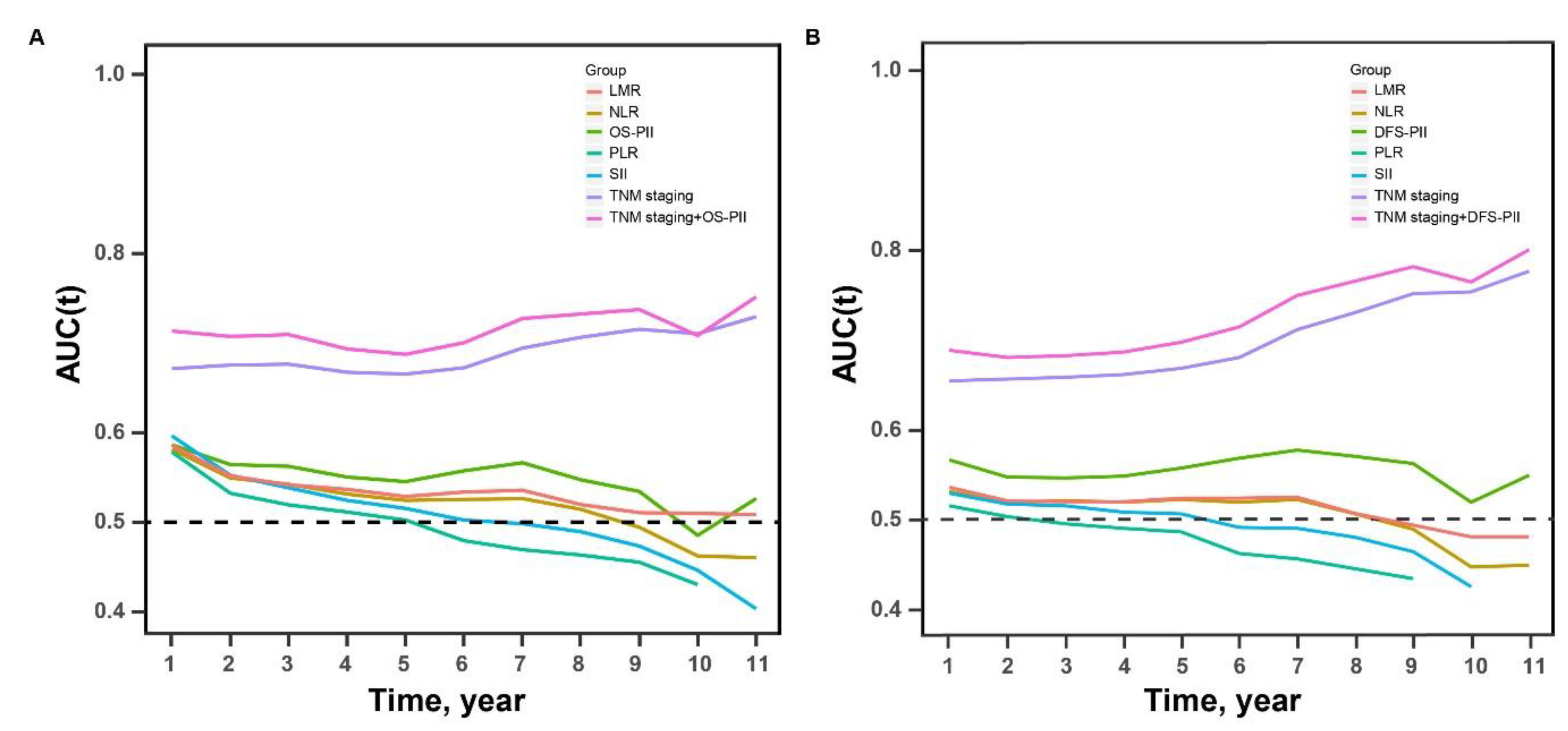
2.7. Comparison of the Prognostic Accuracy of PIIs, TNM Staging, Their Combination, and Previously Reported Biomarkers
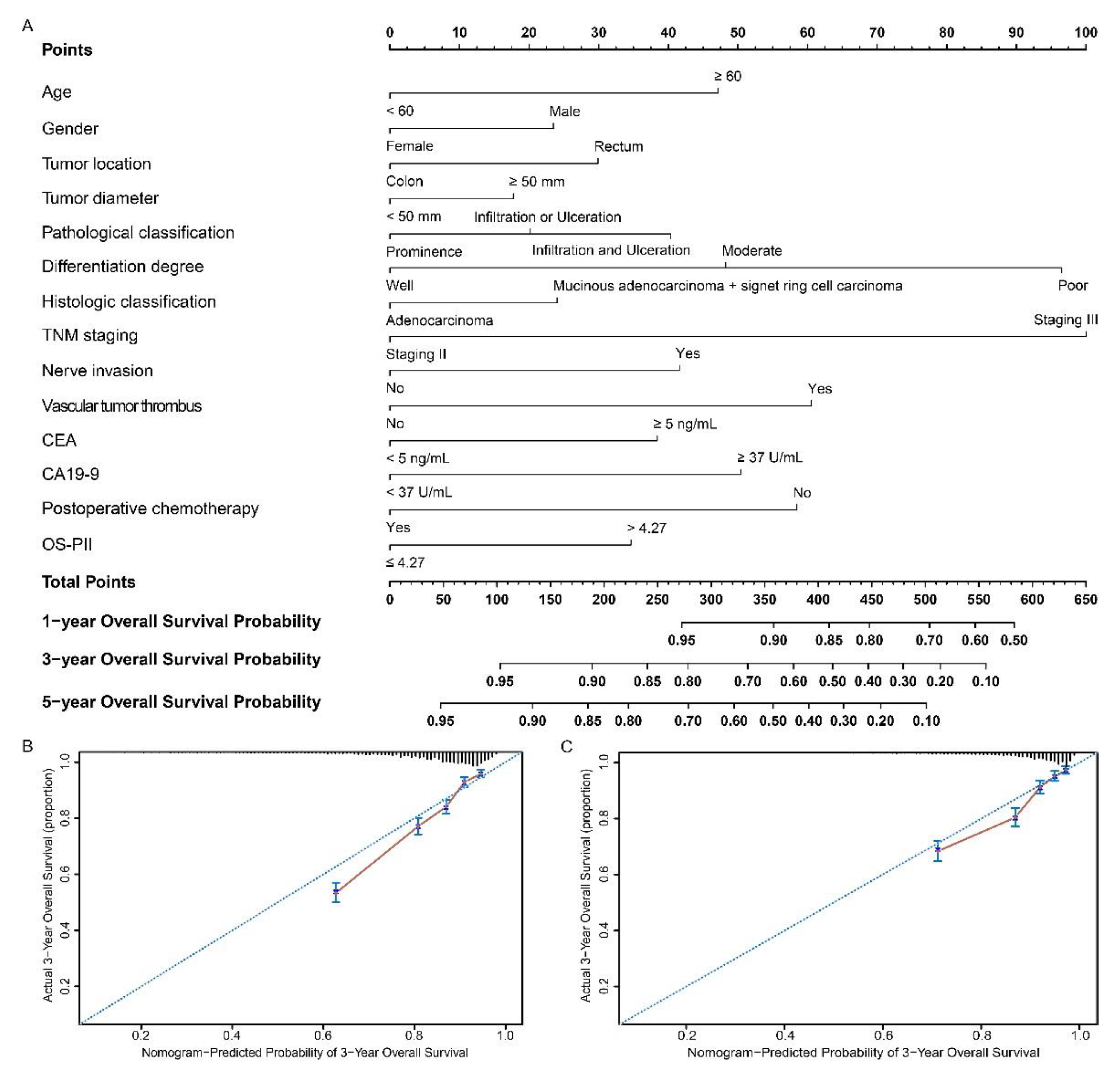
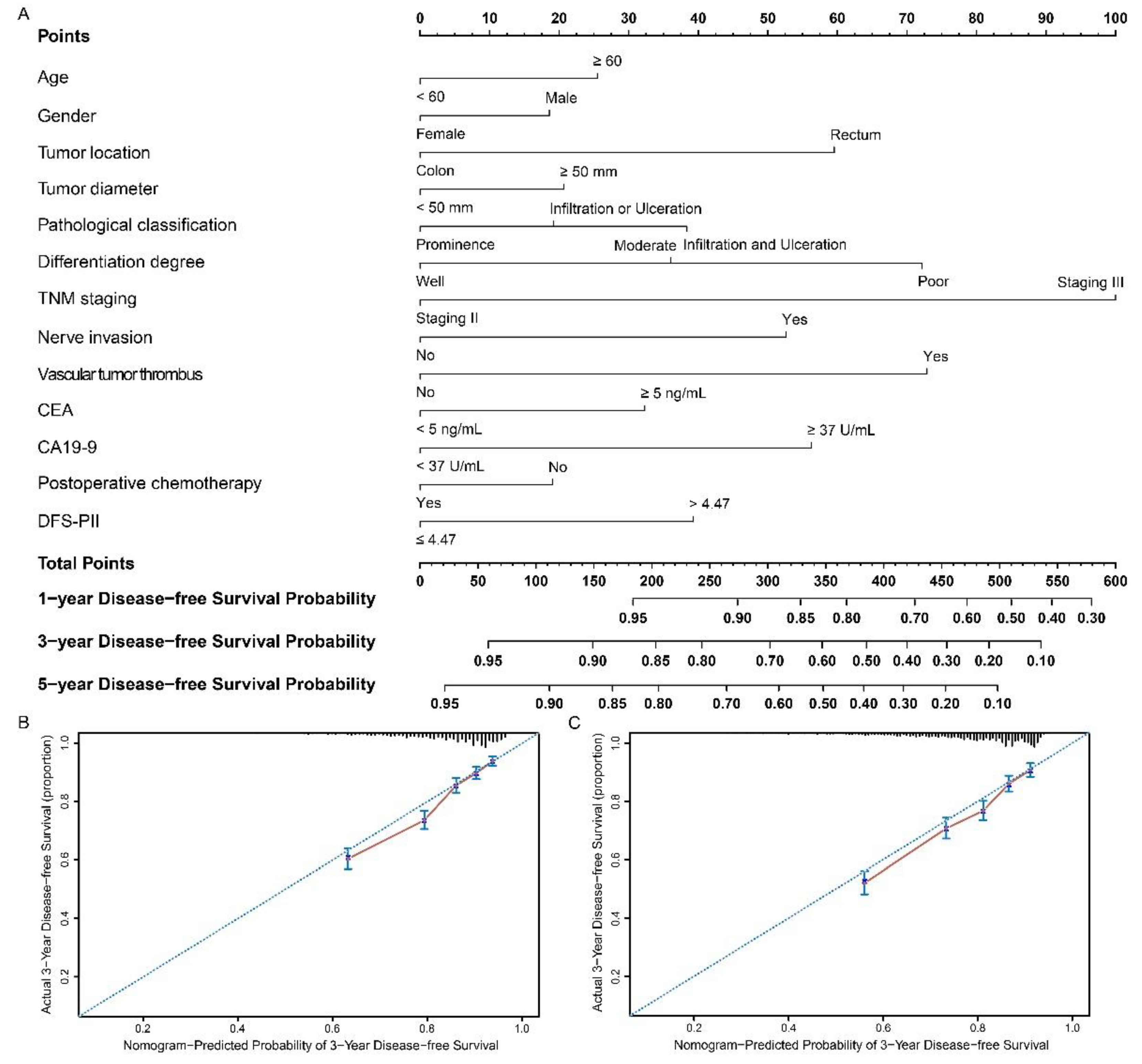
2.8. Development and Validation of Nomograms
2.9. Decision Curve Analysis
3. Discussion
4. Materials and Methods
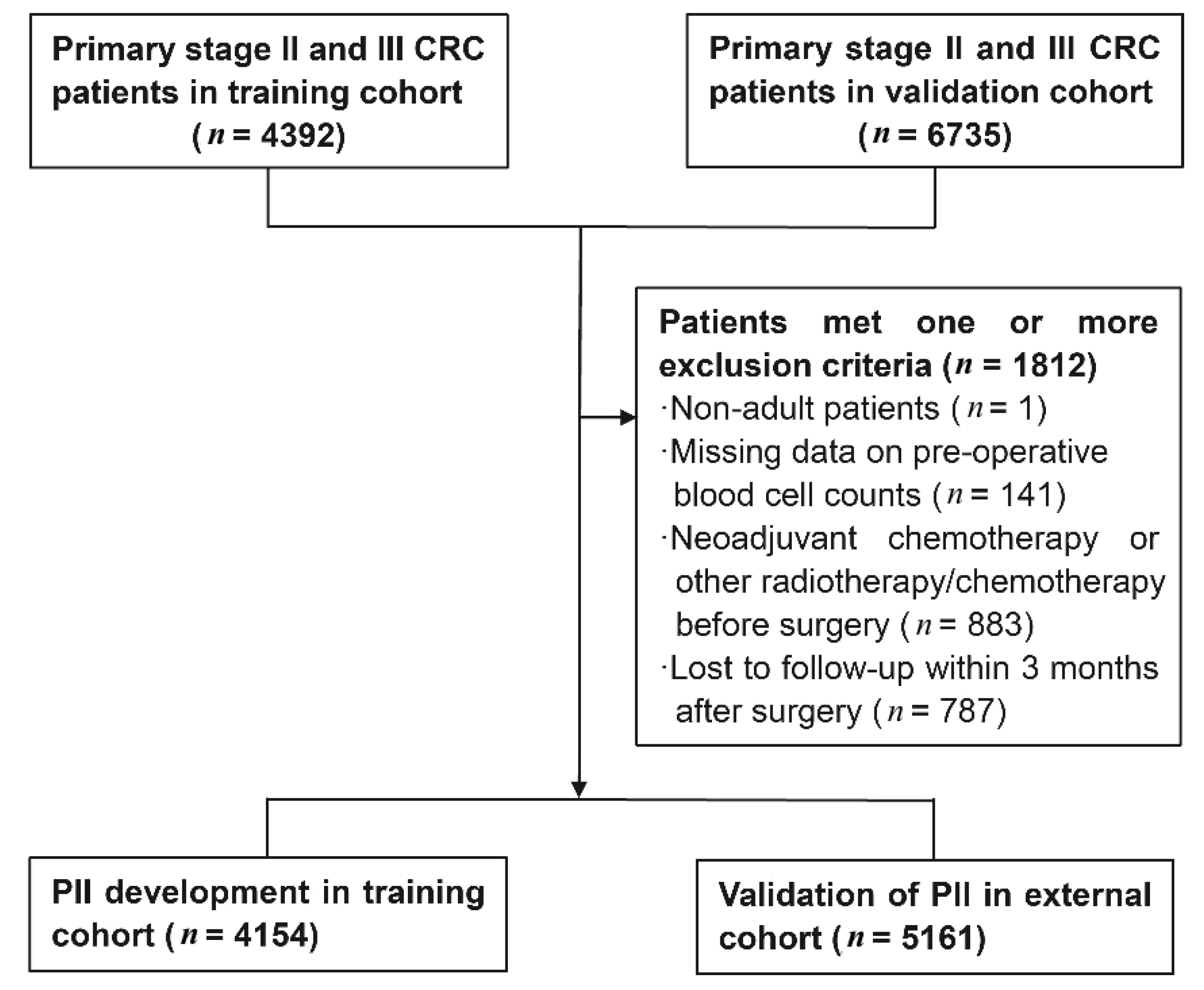
4.1. Study Population
4.2. Data Collection
4.3. Construction of the PII
4.4. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, W.; Zheng, R.; Baade, P.D.; Zhang, S.; Zeng, H.; Bray, F.; Jemal, A.; Yu, X.Q.; He, J. Cancer statistics in China, 2015. CA Cancer J. Clin. 2016, 66, 115–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnold, M.; Sierra, M.S.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017, 66, 683–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeSantis, C.E.; Lin, C.C.; Mariotto, A.B.; Siegel, R.L.; Stein, K.D.; Kramer, J.L.; Alteri, R.; Robbins, A.S.; Jemal, A. Cancer treatment and survivorship statistics, 2014. CA Cancer J. Clin. 2014, 64, 252–271. [Google Scholar] [CrossRef] [PubMed]
- Le Voyer, T.E.; Sigurdson, E.R.; Hanlon, A.L.; Mayer, R.J.; Macdonald, J.S.; Catalano, P.J.; Haller, D.G. Colon cancer survival is associated with increasing number of lymph nodes analyzed: A secondary survey of intergroup trial INT-0089. J. Clin. Oncol. 2003, 21, 2912–2919. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, J.B.; Maggard, M.A.; Ko, C.Y. Colon cancer survival rates with the new American Joint Committee on Cancer sixth edition staging. J. Natl. Cancer Inst. 2004, 96, 1420–1425. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.; Platell, C.; de Boer, B.; McCaul, K.; Iacopetta, B. Population-based study of prognostic factors in stage II colonic cancer. Br. J. Surg. 2006, 93, 866–871. [Google Scholar] [CrossRef]
- Karapetis, C.S.; Khambata-Ford, S.; Jonker, D.J.; O’Callaghan, C.J.; Tu, D.; Tebbutt, N.C.; Simes, R.J.; Chalchal, H.; Shapiro, J.D.; Robitaille, S.; et al. K-ras mutations and benefit from cetuximab in advanced colorectal cancer. N. Engl. J. Med. 2008, 359, 1757–1765. [Google Scholar] [CrossRef] [Green Version]
- Tol, J.; Nagtegaal, I.D.; Punt, C.J. BRAF mutation in metastatic colorectal cancer. N. Engl. J. Med. 2009, 361, 98–99. [Google Scholar] [CrossRef] [Green Version]
- Roth, A.D.; Tejpar, S.; Delorenzi, M.; Yan, P.; Fiocca, R.; Klingbiel, D.; Dietrich, D.; Biesmans, B.; Bodoky, G.; Barone, C.; et al. Prognostic role of KRAS and BRAF in stage II and III resected colon cancer: Results of the translational study on the PETACC-3, EORTC 40993, SAKK 60-00 trial. J. Clin. Oncol 2010, 28, 466–474. [Google Scholar] [CrossRef]
- Balkwill, F.; Mantovani, A. Inflammation and cancer: Back to Virchow? Lancet 2001, 357, 539–545. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greten, F.R.; Grivennikov, S.I. Inflammation and Cancer: Triggers, Mechanisms, and Consequences. Immunity 2019, 51, 27–41. [Google Scholar] [CrossRef] [PubMed]
- Trinchieri, G. Cancer and inflammation: An old intuition with rapidly evolving new concepts. Annu. Rev. Immunol. 2012, 30, 677–706. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Portale, G.; Cavallin, F.; Valdegamberi, A.; Frigo, F.; Fiscon, V. Platelet-to-Lymphocyte Ratio and Neutrophil-to-Lymphocyte Ratio Are Not Prognostic Biomarkers in Rectal Cancer Patients with Curative Resection. J. Gastrointest. Surg. 2018, 22, 1611–1618. [Google Scholar] [CrossRef]
- Li, Z.; Zhao, R.; Cui, Y.; Zhou, Y.; Wu, X. The dynamic change of neutrophil to lymphocyte ratio can predict clinical outcome in stage I-III colon cancer. Sci. Rep. 2018, 8, 9453. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.H.; Lee, J.Y.; Kim, H.K.; Lee, J.W.; Jung, S.G.; Jung, K.; Kim, S.E.; Moon, W.; Park, M.I.; Park, S.J. Prognostic significance of the neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in patients with stage III and IV colorectal cancer. World J. Gastroenterol. 2017, 23, 505–515. [Google Scholar] [CrossRef]
- Wu, Q.B.; Wang, M.; Hu, T.; He, W.B.; Wang, Z.Q. Prognostic role of the lymphocyte-to-monocyte ratio in patients undergoing resection for nonmetastatic rectal cancer. Medicine (Baltimore) 2016, 95, e4945. [Google Scholar] [CrossRef]
- Mahsuni Sevinc, M.; Riza Gunduz, U.; Kinaci, E.; Armagan Aydin, A.; Bayrak, S.; Umar Gursu, R.; Gunduz, S. Preoperative neutrophil-to-lymphocyte ratio and plateletto- lymphocyte ratio as new prognostic factors for patients with colorectal cancer. J. Buon 2016, 21, 1153–1157. [Google Scholar]
- Ozawa, T.; Ishihara, S.; Nishikawa, T.; Tanaka, T.; Tanaka, J.; Kiyomatsu, T.; Hata, K.; Kawai, K.; Nozawa, H.; Kazama, S.; et al. The preoperative platelet to lymphocyte ratio is a prognostic marker in patients with stage II colorectal cancer. Int. J. Colorectal Dis. 2015, 30, 1165–1171. [Google Scholar] [CrossRef] [PubMed]
- Szkandera, J.; Pichler, M.; Absenger, G.; Stotz, M.; Arminger, F.; Weissmueller, M.; Schaberl-Moser, R.; Samonigg, H.; Kornprat, P.; Stojakovic, T.; et al. The elevated preoperative platelet to lymphocyte ratio predicts decreased time to recurrence in colon cancer patients. Am. J. Surg. 2014, 208, 210–214. [Google Scholar] [CrossRef] [PubMed]
- Malietzis, G.; Giacometti, M.; Askari, A.; Nachiappan, S.; Kennedy, R.H.; Faiz, O.D.; Aziz, O.; Jenkins, J.T. A preoperative neutrophil to lymphocyte ratio of 3 predicts disease-free survival after curative elective colorectal cancer surgery. Ann. Surg. 2014, 260, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.; Zhang, X.; Wang, G.; Zhou, Y.; Luo, M.; Wang, S.; Hong, C. The impacts of pretreatment circulating eosinophils and basophils on prognosis of stage-colorectal cancer. Asia Pac. J. Clin. Oncol. 2018, 14, e243–e251. [Google Scholar] [CrossRef]
- Sertoglu, E.; Uyanik, M.; Kayadibi, H. Value of neutrophil to lymphocyte ratio as a biomarker in colorectal adenocarcinoma. Eur. J. Cancer Prev. 2016, 25, 1–2. [Google Scholar] [CrossRef] [Green Version]
- Marx, J. Cancer research. Inflammation and cancer: The link grows stronger. Science 2004, 306, 966–968. [Google Scholar] [CrossRef]
- Kuraishy, A.; Karin, M.; Grivennikov, S.I. Tumor promotion via injury- and death-induced inflammation. Immunity 2011, 35, 467–477. [Google Scholar] [CrossRef] [Green Version]
- Grivennikov, S.I.; Greten, F.R.; Karin, M. Immunity, inflammation, and cancer. Cell 2010, 140, 883–899. [Google Scholar] [CrossRef] [Green Version]
- Zhan, X.; Sun, X.; Hong, Y.; Wang, Y.; Ding, K. Combined Detection of Preoperative Neutrophil-to-Lymphocyte Ratio and CEA as an Independent Prognostic Factor in Nonmetastatic Patients Undergoing Colorectal Cancer Resection Is Superior to NLR or CEA Alone. Biomed. Res. Int. 2017, 2017, 3809464. [Google Scholar] [CrossRef]
- Guthrie, G.J.; Roxburgh, C.S.; Farhan-Alanie, O.M.; Horgan, P.G.; McMillan, D.C. Comparison of the prognostic value of longitudinal measurements of systemic inflammation in patients undergoing curative resection of colorectal cancer. Br. J. Cancer 2013, 109, 24–28. [Google Scholar] [CrossRef] [Green Version]
- Shibutani, M.; Maeda, K.; Nagahara, H.; Noda, E.; Ohtani, H.; Nishiguchi, Y.; Hirakawa, K. A high preoperative neutrophil-to-lymphocyte ratio is associated with poor survival in patients with colorectal cancer. Anticancer Res. 2013, 33, 3291–3294. [Google Scholar] [PubMed]
- Kubo, T.; Ono, S.; Ueno, H.; Shinto, E.; Yamamoto, J.; Hase, K. Impact of the perioperative neutrophil-to-lymphocyte ratio on the long-term survival following an elective resection of colorectal carcinoma. Int. J. Colorectal Dis. 2014, 29, 1091–1099. [Google Scholar] [CrossRef] [PubMed]
- He, W.; Yin, C.; Guo, G.; Jiang, C.; Wang, F.; Qiu, H.; Chen, X.; Rong, R.; Zhang, B.; Xia, L. Initial neutrophil lymphocyte ratio is superior to platelet lymphocyte ratio as an adverse prognostic and predictive factor in metastatic colorectal cancer. Med. Oncol. 2013, 30, 439. [Google Scholar] [CrossRef] [PubMed]
- Galizia, G.; Lieto, E.; Zamboli, A.; De Vita, F.; Castellano, P.; Romano, C.; Auricchio, A.; Cardella, F.; De Stefano, L.; Orditura, M. Neutrophil to lymphocyte ratio is a strong predictor of tumor recurrence in early colon cancers: A propensity score-matched analysis. Surgery 2015, 158, 112–120. [Google Scholar] [CrossRef]
- Walsh, S.R.; Cook, E.J.; Goulder, F.; Justin, T.A.; Keeling, N.J. Neutrophil-lymphocyte ratio as a prognostic factor in colorectal cancer. J. Surg. Oncol. 2005, 91, 181–184. [Google Scholar] [CrossRef]
- Absenger, G.; Szkandera, J.; Stotz, M.; Postlmayr, U.; Pichler, M.; Ress, A.L.; Schaberl-Moser, R.; Loibner, H.; Samonigg, H.; Gerger, A. Preoperative neutrophil-to-lymphocyte ratio predicts clinical outcome in patients with stage II and III colon cancer. Anticancer Res. 2013, 33, 4591–4594. [Google Scholar]
- Ying, H.Q.; Deng, Q.W.; He, B.S.; Pan, Y.Q.; Wang, F.; Sun, H.L.; Chen, J.; Liu, X.; Wang, S.K. The prognostic value of preoperative NLR, d-NLR, PLR and LMR for predicting clinical outcome in surgical colorectal cancer patients. Med. Oncol. 2014, 31, 305. [Google Scholar] [CrossRef]
- Gijsbers, K.; Gouwy, M.; Struyf, S.; Wuyts, A.; Proost, P.; Opdenakker, G.; Penninckx, F.; Ectors, N.; Geboes, K.; Van Damme, J. GCP-2/CXCL6 synergizes with other endothelial cell-derived chemokines in neutrophil mobilization and is associated with angiogenesis in gastrointestinal tumors. Exp. Cell Res. 2005, 303, 331–342. [Google Scholar] [CrossRef]
- Mantovani, A.; Cassatella, M.A.; Costantini, C.; Jaillon, S. Neutrophils in the activation and regulation of innate and adaptive immunity. Nat. Rev. Immunol. 2011, 11, 519–531. [Google Scholar] [CrossRef]
- Mizuno, R.; Kawada, K.; Itatani, Y.; Ogawa, R.; Kiyasu, Y.; Sakai, Y. The Role of Tumor-Associated Neutrophils in Colorectal Cancer. Int. J. Mol. Sci. 2019, 20, 529. [Google Scholar] [CrossRef] [Green Version]
- Augier, S.; Ciucci, T.; Luci, C.; Carle, G.F.; Blin-Wakkach, C.; Wakkach, A. Inflammatory blood monocytes contribute to tumor development and represent a privileged target to improve host immunosurveillance. J. Immunol. 2010, 185, 7165–7173. [Google Scholar] [CrossRef] [PubMed]
- Condeelis, J.; Pollard, J.W. Macrophages: Obligate partners for tumor cell migration, invasion, and metastasis. Cell 2006, 124, 263–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diakos, C.I.; Charles, K.A.; McMillan, D.C.; Clarke, S.J. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014, 15, e493–e503. [Google Scholar] [CrossRef]
- Gaertner, F.; Massberg, S. Patrolling the vascular borders: Platelets in immunity to infection and cancer. Nat. Rev. Immunol. 2019, 19, 747–760. [Google Scholar] [CrossRef]
- Michael, J.V.; Wurtzel, J.G.T.; Mao, G.F.; Rao, A.K.; Kolpakov, M.A.; Sabri, A.; Hoffman, N.E.; Rajan, S.; Tomar, D.; Madesh, M.; et al. Platelet microparticles infiltrating solid tumors transfer miRNAs that suppress tumor growth. Blood 2017, 130, 567–580. [Google Scholar] [CrossRef] [Green Version]
- Prizment, A.E.; Vierkant, R.A.; Smyrk, T.C.; Tillmans, L.S.; Lee, J.J.; Sriramarao, P.; Nelson, H.H.; Lynch, C.F.; Thibodeau, S.N.; Church, T.R.; et al. Tumor eosinophil infiltration and improved survival of colorectal cancer patients: Iowa Women’s Health Study. Mod. Pathol. 2016, 29, 516–527. [Google Scholar] [CrossRef]
- Xie, F.; Liu, L.B.; Shang, W.Q.; Chang, K.K.; Meng, Y.H.; Mei, J.; Yu, J.J.; Li, D.J.; Li, M.Q. The infiltration and functional regulation of eosinophils induced by TSLP promote the proliferation of cervical cancer cell. Cancer Lett. 2015, 364, 106–117. [Google Scholar] [CrossRef]
- Kozak, M.M.; von Eyben, R.; Pai, J.S.; Anderson, E.M.; Welton, M.L.; Shelton, A.A.; Kin, C.; Koong, A.C.; Chang, D.T. The Prognostic Significance of Pretreatment Hematologic Parameters in Patients Undergoing Resection for Colorectal Cancer. Am. J. Clin. Oncol. 2017, 40, 405–412. [Google Scholar] [CrossRef]
- Brenner, H.; Kloor, M.; Pox, C.P. Colorectal cancer. Lancet 2014, 383, 1490–1502. [Google Scholar] [CrossRef]
- Balachandran, V.P.; Gonen, M.; Smith, J.J.; DeMatteo, R.P. Nomograms in oncology: More than meets the eye. Lancet Oncol. 2015, 16, e173–e180. [Google Scholar] [CrossRef] [Green Version]
- Sternberg, C.N. Are nomograms better than currently available stage groupings for bladder cancer? J. Clin. Oncol. 2006, 24, 3819–3820. [Google Scholar] [CrossRef] [PubMed]
- Touijer, K.; Scardino, P.T. Nomograms for staging, prognosis, and predicting treatment outcomes. Cancer 2009, 115, 3107–3111. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef] [PubMed]
- McShane, L.M.; Altman, D.G.; Sauerbrei, W.; Taube, S.E.; Gion, M.; Clark, G.M. Reporting recommendations for tumor marker prognostic studies (REMARK). J. Natl. Cancer Inst. 2005, 97, 1180–1184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camp, R.L.; Dolled-Filhart, M.; Rimm, D.L. X-tile: A new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin. Cancer Res. 2004, 10, 7252–7259. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; White, I.R.; Carlin, J.B.; Spratt, M.; Royston, P.; Kenward, M.G.; Wood, A.M.; Carpenter, J.R. Multiple imputation for missing data in epidemiological and clinical research: Potential and pitfalls. BMJ 2009, 338, b2393. [Google Scholar] [CrossRef]
- Iasonos, A.; Schrag, D.; Raj, G.V.; Panageas, K.S. How to build and interpret a nomogram for cancer prognosis. J. Clin. Oncol. 2008, 26, 1364–1370. [Google Scholar] [CrossRef]
- Kamarudin, A.N.; Cox, T.; Kolamunnage-Dona, R. Time-dependent ROC curve analysis in medical research: Current methods and applications. BMC Med. Res. Methodol. 2017, 17, 53. [Google Scholar] [CrossRef] [Green Version]
- Heagerty, P.J.; Lumley, T.; Pepe, M.S. Time-dependent ROC curves for censored survival data and a diagnostic marker. Biometrics 2000, 56, 337–344. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic or Characteristic | Training Cohort (N = 4154) | Validation Cohort (N = 5161) | p Value |
|---|---|---|---|
| Age (year) a | 59.3 ± 11.65 | 58.5 ± 11.95 | 0.850 |
| <60 | 2103 (50.6) | 2645 (51.2) | 0.549 |
| ≥60 | 2051 (49.4) | 2516 (48.8) | |
| Gender b | 0.804 | ||
| Male | 2454 (59.1) | 3062 (59.3) | |
| Female | 1700 (40.9) | 2099 (40.7) | |
| BMI (kg/m2) b | - | ||
| <24 | 1828 (44.0) | - | |
| ≥24 | 1383 (33.3) | - | |
| Hypertension b | - | ||
| No | 3554 (85.6) | - | |
| Yes | 600 (14.4) | - | |
| Diabetes mellitus b | - | ||
| No | 3842 (92.5) | - | |
| Yes | 312 (7.5) | - | |
| Tumor location b | 0.005 | ||
| Right colon | 899 (21.6) | 1220 (23.7) | |
| Transverse colon | 85 (2.0) | 110 (2.1) | |
| Left colon | 256 (6.2) | 362 (7.0) | |
| Sigmoid colon | 721 (17.4) | 773 (15.0) | |
| Rectum | 2193 (52.8) | 2696 (52.2) | |
| Tumor diameter b | <0.001 | ||
| <50 mm | 1640 (39.5) | 3446 (66.8) | |
| ≥50 mm | 2359 (56.8) | 1710 (33.1) | |
| Pathological classification b | <0.001 | ||
| Prominence | 2740 (66.0) | 1277 (24.7) | |
| Infiltration | 268 (6.4) | 238 (4.6) | |
| Ulceration | 160 (3.9) | 3436 (66.6) | |
| Infiltration and ulceration | 986 (23.7) | 210 (4.1) | |
| Differentiation degree b | <0.001 | ||
| Well | 331 (8.0) | 48 (0.9) | |
| Moderate | 3225 (77.6) | 3755 (72.8) | |
| Poor | 598 (14.4) | 1358 (26.3) | |
| Histologic classification b | <0.001 | ||
| Adenocarcinoma | 3136 (75.5) | 4342 (84.1) | |
| Mucinous adenocarcinoma + signet ring cell carcinoma | 1018 (24.5) | 819 (15.9) | |
| TNM staging b | <0.001 | ||
| II | 2385 (57.4) | 2086 (40.4) | |
| III | 1769 (42.6) | 3075 (59.6) | |
| AJCC staging II b | <0.001 | ||
| IIA | 974 (40.8) | 1175 (56.3) | |
| IIB | 180 (7.6) | 882 (42.3) | |
| IIC | 1231 (51.6) | 29 (1.4) | |
| AJCC staging III b | <0.001 | ||
| IIIA | 122 (6.9) | 271 (8.8) | |
| IIIB | 752 (42.5) | 1727 (56.2) | |
| IIIC | 895 (50.6) | 1077 (35.0) | |
| Tumor invasion b | <0.001 | ||
| T1–T3 | 1847 (44.5) | 2588 (50.1) | |
| T4 | 2307 (55.5) | 2573 (49.9) | |
| Lymph nodes involved b | <0.001 | ||
| N0 | 2385 (57.4) | 2086 (40.4) | |
| N1–N2 | 1769 (42.6) | 3075 (59.6) | |
| Cancer nodules b | <0.001 | ||
| No | 3863 (93.0) | 4249 (82.3) | |
| Yes | 291 (7.0) | 912 (17.7) | |
| Nerve invasion b | <0.001 | ||
| No | 3836 (92.3) | 3898 (75.5) | |
| Yes | 318 (7.7) | 1263 (24.5) | |
| Vascular tumor thrombus b | <0.001 | ||
| No | 4009 (96.5) | 3622 (70.2) | |
| Yes | 145 (3.5) | 1539 (29.8) | |
| CEA b | 0.971 | ||
| <5 ng/mL | 2203 (53.0) | 2832 (54.9) | |
| ≥5 ng/mL | 1626 (39.1) | 2087 (40.4) | |
| CA19-9 b | <0.001 | ||
| <37 U/mL | 3026 (72.8) | 3932 (76.2) | |
| ≥37 U/mL | 621 (14.9) | 991 (19.2) | |
| Postoperative chemotherapy b | <0.001 | ||
| No | 2413 (58.1) | 940 (18.2) | |
| Yes | 1741 (41.9) | 4221 (81.8) | |
| Postoperative radiotherapy b | <0.001 | ||
| No | 3969 (95.5) | 4752 (92.1) | |
| Yes | 185 (4.5) | 409 (7.9) | |
| Platelet counts (109/L) c | 247 (204–305) | 232 (189–283) | <0.001 |
| Neutrophil counts (109/L) c | 3.77 (2.95–4.83) | 3.50 (2.80–4.50) | <0.001 |
| Lymphocyte counts (109/L) c | 1.89 (1.50–2.34) | 1.70 (1.30–2.10) | <0.001 |
| Monocyte counts (109/L) c | 0.43 (0.33–0.54) | 0.40 (0.30–0.50) | <0.001 |
| Eosinophil counts (109/L) c | 0.12 (0.06–0.20) | 0.13 (0.08–0.22) | <0.001 |
| Basophil counts (109/L) c | 0.04 (0.02–0.06) | 0.02 (0.01–0.04) | <0.001 |
| Demographic or Characteristic | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age | <0.001 | <0.001 | ||
| <60 | 1.000 | 1.000 | ||
| ≥60 | 1.654 (1.479–1.851) | 1.521 (1.354–1.708) | ||
| Gender | 0.013 | <0.001 | ||
| Male | 1.000 | 1.000 | ||
| Female | 0.866 (0.773–0.970) | 0.802 (0.715–0.899) | ||
| Tumor location | <0.001 | 0.001 | ||
| Colon | 1.000 | 1.000 | ||
| Rectum | 1.297 (1.160–1.449) | 1.224 (1.089–1.377) | ||
| Tumor diameter | <0.001 | 0.009 | ||
| <50 mm | 1.000 | 1.000 | ||
| ≥50 mm | 1.248 (1.113–1.400) | 1.171 (1.040–1.319) | ||
| Pathological classification | ||||
| Prominence | 1.000 | 1.000 | ||
| Infiltration or Ulceration | 1.544 (1.298–1.836) | <0.001 | 1.357 (1.138–1.619) | 0.001 |
| Infiltration and Ulceration | 1.578 (1.394–1.786) | <0.001 | 1.394 (1.228–1.581) | <0.001 |
| Differentiation degree | ||||
| Well | 1.000 | 1.000 | ||
| Moderate | 1.608 (1.243–2.079) | <0.001 | 1.480 (1.142–1.916) | 0.003 |
| Poor | 2.812 (2.132–3.708) | <0.001 | 2.269 (1.715–3.003) | <0.001 |
| Histologic classification | 0.011 | 0.002 | ||
| Adenocarcinoma | 1.000 | 1.000 | ||
| Mucinous adenocarcinoma or signet ring cell carcinoma | 1.176 (1.039–1.332) | 1.219 (1.073–1.385) | ||
| TNM staging | <0.001 | <0.001 | ||
| II | 1.000 | 1.000 | ||
| III | 2.447 (2.187–2.738) | 2.248 (1.995–2.534) | ||
| Nerve invasion | <0.001 | 0.001 | ||
| No | 1.000 | 1.000 | ||
| Yes | 1.774 (1.480–2.126) | 1.387 (1.146–1.679) | ||
| Vascular tumor thrombus | <0.001 | <0.001 | ||
| No | 1.000 | 1.000 | ||
| Yes | 2.435 (1.922–3.087) | 1.669 (1.302–2.139) | ||
| CEA | <0.001 | <0.001 | ||
| <5 ng/mL | 1.000 | 1.000 | ||
| ≥5 ng/mL | 1.709 (1.521–1.921) | 1.373 (1.217–1.550) | ||
| CA19-9 | <0.001 | <0.001 | ||
| <37 U/mL | 1.000 | 1.000 | ||
| ≥37 U/mL | 2.012 (1.761–2.298) | 1.525 (1.322–1.760) | ||
| Postoperative chemotherapy | <0.001 | <0.001 | ||
| No | 1.000 | 1.000 | ||
| Yes | 0.669 (0.596–0.751) | 0.578 (0.511–0.654) | ||
| Postoperative radiotherapy | <0.001 | <0.001 | ||
| No | 1.000 | 1.000 | ||
| Yes | 1.854 (1.496–2.298) | 1.824 (1.458–2.282) | ||
| OS-PII (Continuous) | 1.105 (1.072–1.139) | <0.001 | 1.087 (1.052–1.122) | <0.001 |
| OS-PII (Binary) | <0.001 | <0.001 | ||
| ≤4.27 | 1.000 | 1.000 | ||
| >4.27 | 1.400 (1.253–1.565) | 1.330 (1.189–1.489) | ||
| Demographic or Characteristic | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age (year) | 0.010 | <0.001 | ||
| <60 | 1.000 | 1.000 | ||
| ≥60 | 1.176 (1.040–1.331) | 1.261 (1.109–1.433) | ||
| Gender | 0.048 | 0.014 | ||
| Male | 1.000 | 1.000 | ||
| Female | 0.880 (0.776–0.999) | 0.851 (0.749–0.968) | ||
| Tumor location | <0.001 | <0.001 | ||
| Colon | 1.000 | 1.000 | ||
| Rectum | 1.633 (1.437–1.856) | 1.504 (1.314–1.721) | ||
| Tumor diameter | 0.004 | 0.008 | ||
| <50 mm | 1.000 | 1.000 | ||
| ≥50 mm | 1.211 (1.063–1.379) | 1.195 (1.047–1.362) | ||
| Pathological classification | ||||
| Prominence | 1.000 | 1.000 | ||
| Infiltration or Ulceration | 1.559 (1.288–1.888) | <0.001 | 1.395 (1.148–1.695) | 0.001 |
| Infiltration and Ulceration | 1.498 (1.302–1.724) | <0.001 | 1.316 (1.141–1.518) | <0.001 |
| Differentiation degree | ||||
| Well | 1.000 | 1.000 | ||
| Moderate | 1.336 (1.029–1.734) | 0.030 | 1.257 (0.966–1.637) | 0.088 |
| Poor | 2.161 (1.620–2.882) | <0.001 | 1.708 (1.275–2.287) | <0.001 |
| Histologic classification | 0.164 | - | ||
| Adenocarcinoma | 1.000 | - | ||
| Mucinous adenocarcinoma or signet ring cell carcinoma | 1.105 (0.960–1.273) | - | ||
| TNM staging | <0.001 | <0.001 | ||
| II | 1.000 | 1.000 | ||
| III | 2.720 (2.396–3.088) | 2.148 (1.878–2.457) | ||
| Nerve invasion | <0.001 | <0.001 | ||
| No | 1.000 | 1.000 | ||
| Yes | 2.084 (1.728–2.513) | 1.479 (1.212–1.805) | ||
| Vascular tumor thrombus | <0.001 | <0.001 | ||
| No | 1.000 | 1.000 | ||
| Yes | 2.810 (2.203–3.584) | 1.758 (1.361–2.273) | ||
| CEA | <0.001 | 0.001 | ||
| <5 ng/mL | 1.000 | 1.000 | ||
| ≥5 ng/mL | 1.530 (1.347–1.738) | 1.259 (1.100–1.442) | ||
| CA19-9 | <0.001 | <0.001 | ||
| <37 U/mL | 1.000 | 1.000 | ||
| ≥37 U/mL | 1.914 (1.631–2.245) | 1.594 (1.353–1.878) | ||
| Postoperative chemotherapy | <0.001 | 0.277 | ||
| No | 1.000 | 1.000 | ||
| Yes | 1.272 (1.125–1.439) | 1.076 (0.943–1.229) | ||
| Postoperative radiotherapy | <0.001 | <0.001 | ||
| No | 1.000 | 1.000 | ||
| Yes | 3.212 (2.623–3.932) | 2.281 (1.839–2.828) | ||
| DFS-PII (Continuous) | 1.105 (1.069–1.143) | <0.001 | 1.089 (1.053–1.128) | <0.001 |
| DFS-PII (Binary) | <0.001 | <0.001 | ||
| ≤4.47 | 1.000 | 1.000 | ||
| >4.47 | 1.395 (1.233–1.580) | 1.366 (1.206–1.548) | ||
| Demographic or Characteristic | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age | <0.001 | <0.001 | ||
| <60 | 1.000 | 1.000 | ||
| ≥60 | 1.418 (1.197–1.679) | 1.468 (1.235–1.745) | ||
| Gender | 0.508 | 0.604 | ||
| Male | 1.000 | 1.000 | ||
| Female | 1.059 (0.893–1.256) | 1.047 (0.881–1.244) | ||
| Tumor location | 0.397 | 0.653 | ||
| Colon | 1.000 | 1.000 | ||
| Rectum | 0.930 (0.786–1.100) | 0.958 (0.793–1.156) | ||
| Tumor diameter | 0.603 | 0.288 | ||
| <50 mm | 1.000 | 1.000 | ||
| ≥50 mm | 1.048 (0.878–1.252) | 1.106 (0.919–1.331) | ||
| Pathological classification | ||||
| Prominence | 1.000 | 1.000 | ||
| Infiltration or Ulceration | 1.488 (1.189–1.861) | 0.001 | 1.223 (0.972–1.539) | 0.086 |
| Infiltration and Ulceration | 1.616 (1.081–2.415) | 0.019 | 1.424 (0.948–2.139) | 0.088 |
| Differentiation degree | ||||
| Well | 1.000 | 1.000 | ||
| Moderate | 2.289 (0.570–9.196) | 0.243 | 1.350 (0.334–5.452) | 0.673 |
| Poor | 4.904 (1.218–19.745) | 0.025 | 2.096 (0.516–8.513) | 0.301 |
| Histologic classification | 0.001 | 0.634 | ||
| Adenocarcinoma | 1.000 | 1.000 | ||
| Mucinous adenocarcinoma or signet ring cell carcinoma | 1.413 (1.145–1.743) | 1.059 (0.838–1.338) | ||
| TNM staging | <0.001 | <0.001 | ||
| II | 1.000 | 1.000 | ||
| III | 2.985 (2.414–3.691) | 2.083 (1.648–2.634) | ||
| Nerve invasion | <0.001 | 0.010 | ||
| No | 1.000 | 1.000 | ||
| Yes | 1.950 (1.635–2.325) | 1.284 (1.062–1.551) | ||
| Vascular tumor thrombus | <0.001 | <0.001 | ||
| No | 1.000 | 1.000 | ||
| Yes | 2.774 (2.342–3.285) | 1.721 (1.427–2.076) | ||
| CEA | <0.001 | <0.001 | ||
| <5 ng/mL | 1.000 | 1.000 | ||
| ≥5 ng/mL | 2.375 (1.994–2.830) | 1.661 (1.376–2.006) | ||
| CA19-9 | <0.001 | <0.001 | ||
| <37 U/mL | 1.000 | 1.000 | ||
| ≥37 U/mL | 3.073 (2.583–3.654) | 1.917 (1.581–2.323) | ||
| Postoperative chemotherapy | 0.014 | <0.001 | ||
| No | 1.000 | 1.000 | ||
| Yes | 0.774 (0.631–0.949) | 0.618 (0.499–0.766) | ||
| Postoperative radiotherapy | 0.016 | 0.089 | ||
| No | 1.000 | 1.000 | ||
| Yes | 1.329 (1.055–1.675) | 1.257 (0.965–1.637) | ||
| OS-PII (Continuous) | 1.164 (1.107–1.224) | <0.001 | 1.133 (1.076–1.194) | <0.001 |
| OS-PII (Binary) | <0.001 | <0.001 | ||
| ≤4.27 | 1.000 | 1.000 | ||
| >4.27 | 1.561 (1.316–1.852) | 1.407 (1.182–1.674) | ||
| Demographic or Characteristic | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age (year) | 0.291 | 0.108 | ||
| <60 | 1.000 | 1.000 | ||
| ≥60 | 1.070 (0.944–1.212) | 1.110 (0.978–1.261) | ||
| Gender | 0.623 | 0.328 | ||
| Male | 1.000 | 1.000 | ||
| Female | 0.969 (0.853–1.100) | 0.938 (0.825–1.067) | ||
| Tumor location | 0.946 | 0.891 | ||
| Colon | 1.000 | 1.000 | ||
| Rectum | 1.004 (0.888–1.138) | 0.990 (0.863–1.136) | ||
| Tumor diameter | 0.266 | 0.951 | ||
| <50 mm | 1.000 | 1.000 | ||
| ≥50 mm | 0.927 (0.810–1.060) | 0.996 (0.866–1.144) | ||
| Pathological classification | ||||
| Prominence | 1.000 | 1.000 | ||
| Infiltration or Ulceration | 1.420 (1.208–1.668) | <0.001 | 1.193 (1.013–1.405) | 0.035 |
| Infiltration and Ulceration | 1.414 (1.040–1.923) | 0.027 | 1.232 (0.904–1.680) | 0.187 |
| Differentiation degree | ||||
| Well | 1.000 | 1.000 | ||
| Moderate | 1.796 (0.744–4.332) | 0.192 | 1.149 (0.475–2.780) | 0.758 |
| Poor | 2.965 (1.225–7.178) | 0.016 | 1.435 (0.590–3.491) | 0.426 |
| Histologic classification | 0.056 | - | ||
| Adenocarcinoma | 1.000 | - | ||
| Mucinous adenocarcinoma or signet ring cell carcinoma | 1.174 (0.996–1.384) | - | ||
| TNM staging | <0.001 | <0.001 | ||
| II | 1.000 | 1.000 | ||
| III | 2.448 (2.112–2.837) | 1.684 (1.429–1.984) | ||
| Nerve invasion | <0.001 | <0.001 | ||
| No | 1.000 | 1.000 | ||
| Yes | 1.999 (1.755–2.277) | 1.389 (1.207–1.597) | ||
| Vascular tumor thrombus | <0.001 | <0.001 | ||
| No | 1.000 | 1.000 | ||
| Yes | 2.249 (1.983–2.551) | 1.528 (1.327–1.758) | ||
| CEA | <0.001 | <0.001 | ||
| <5 ng/mL | 1.000 | 1.000 | ||
| ≥5 ng/mL | 2.004 (1.763–2.279) | 1.589 (1.384–1.824) | ||
| CA19-9 | <0.001 | <0.001 | ||
| <37 U/mL | 1.000 | 1.000 | ||
| ≥37 U/mL | 2.306 (2.015–2.639) | 1.584 (1.364–1.841) | ||
| Postoperative chemotherapy | 0.004 | 0.317 | ||
| No | 1.000 | 1.000 | ||
| Yes | 1.291 (1.087–1.534) | 1.096 (0.916–1.312) | ||
| Postoperative radiotherapy | 0.001 | 0.257 | ||
| No | 1.000 | 1.000 | ||
| Yes | 1.353 (1.133–1.615) | 1.121 (0.920–1.366) | ||
| DFS-PII (Continuous) | 1.054 (1.036–1.073) | 0.003 | 1.037 (1.002–1.075) | 0.040 |
| DFS-PII (Binary) | 0.001 | 0.019 | ||
| ≤4.47 | 1.000 | 1.000 | ||
| >4.47 | 1.248 (1.101–1.414) | 1.162 (1.025–1.318) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, J.; Zhu, J.; Du, F.; Zhang, L.; Li, D.; Huang, H.; Tian, T.; Liu, Y.; Zhang, L.; Liu, Y.; et al. Prognostic Inflammatory Index Based on Preoperative Peripheral Blood for Predicting the Prognosis of Colorectal Cancer Patients. Cancers 2021, 13, 3. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13010003
Fu J, Zhu J, Du F, Zhang L, Li D, Huang H, Tian T, Liu Y, Zhang L, Liu Y, et al. Prognostic Inflammatory Index Based on Preoperative Peripheral Blood for Predicting the Prognosis of Colorectal Cancer Patients. Cancers. 2021; 13(1):3. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13010003
Chicago/Turabian StyleFu, Jinming, Ji Zhu, Fenqi Du, Lijie Zhang, Dapeng Li, Hao Huang, Tian Tian, Yupeng Liu, Lei Zhang, Ying Liu, and et al. 2021. "Prognostic Inflammatory Index Based on Preoperative Peripheral Blood for Predicting the Prognosis of Colorectal Cancer Patients" Cancers 13, no. 1: 3. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13010003