
Liver Transplantation for Hepatocellular Carcinoma: A Real-Life Comparison of Milan Criteria and AFP Model

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
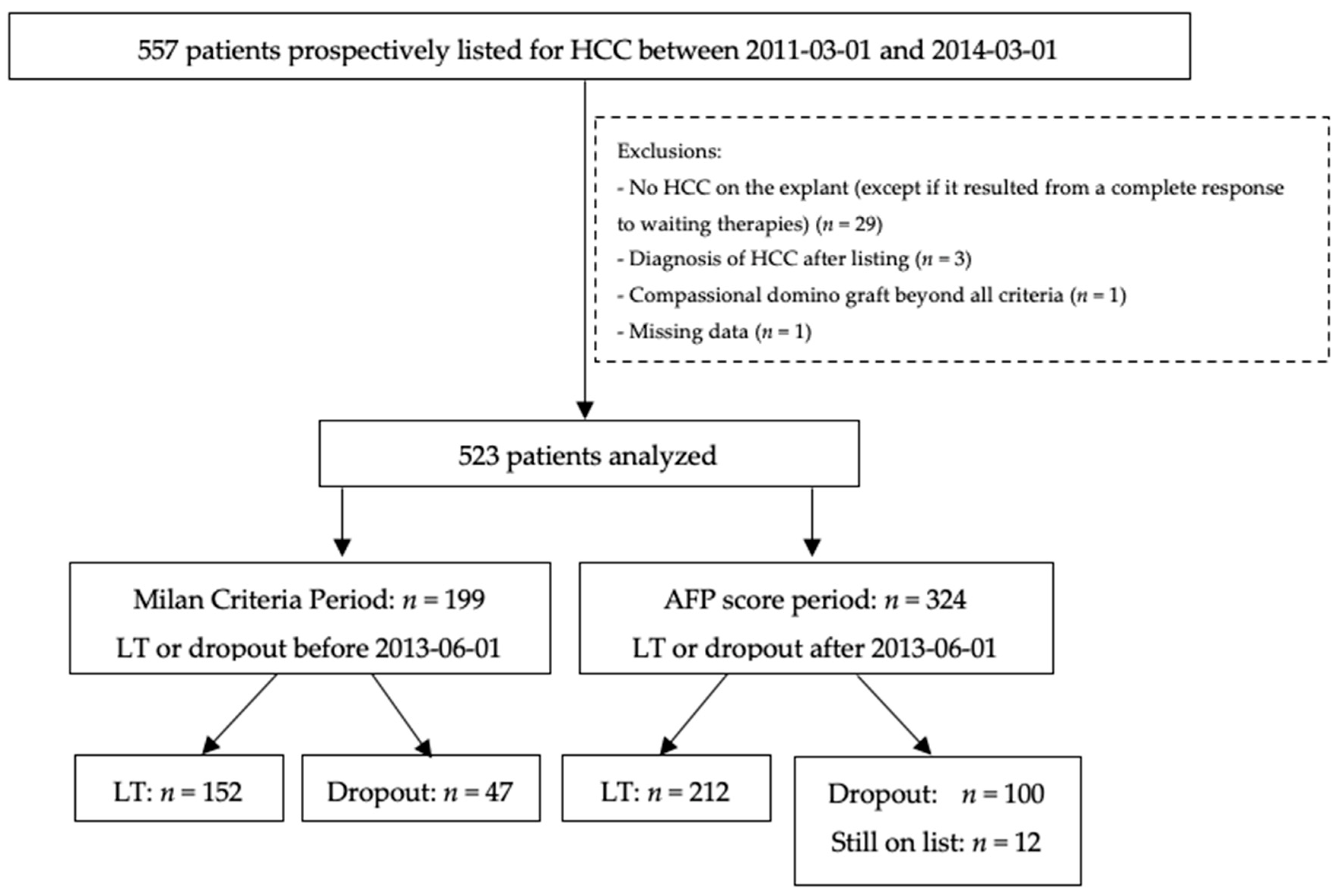
2.1. Study Design
2.2. Patients
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. Agreement for the Allocation Criteria on Explant Findings
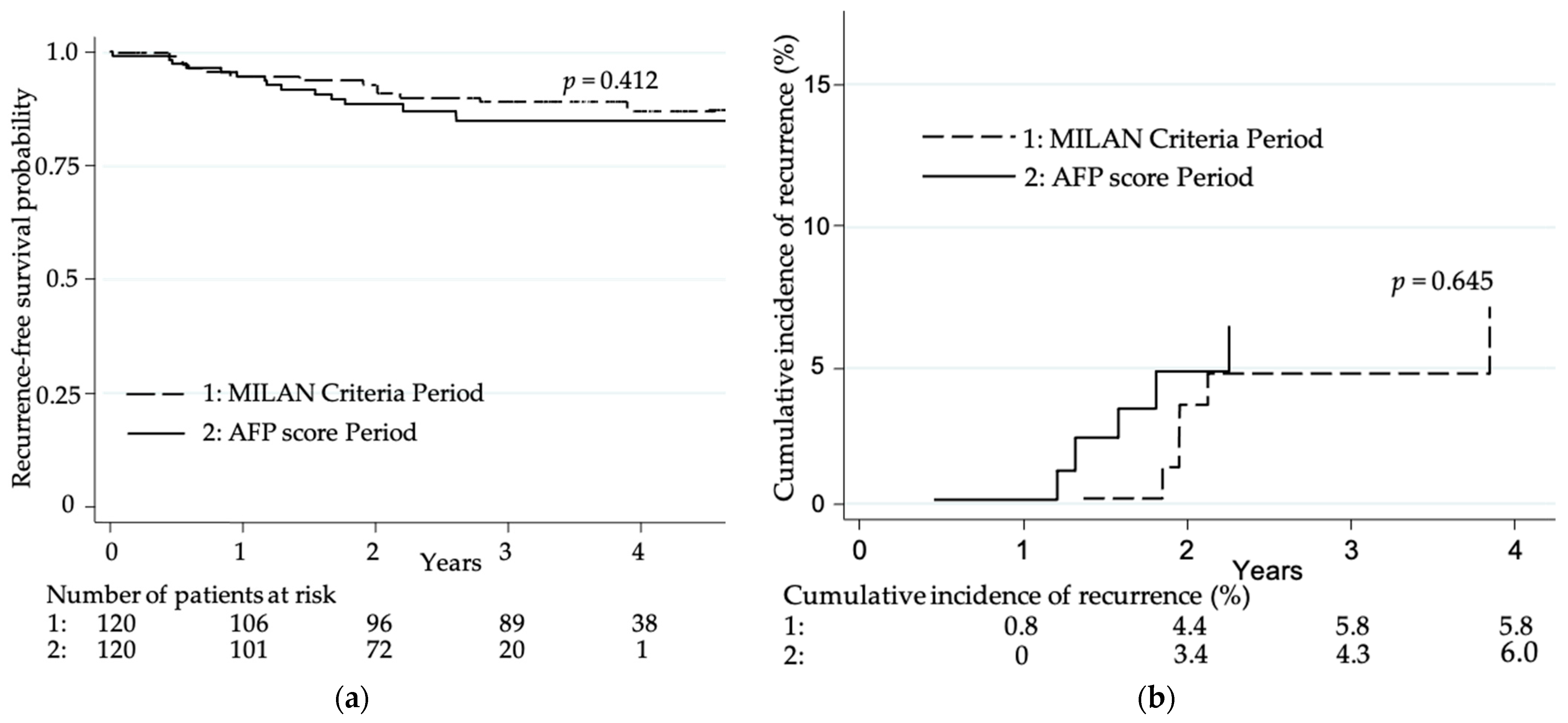
3.3. Post-LT Tumor Recurrence
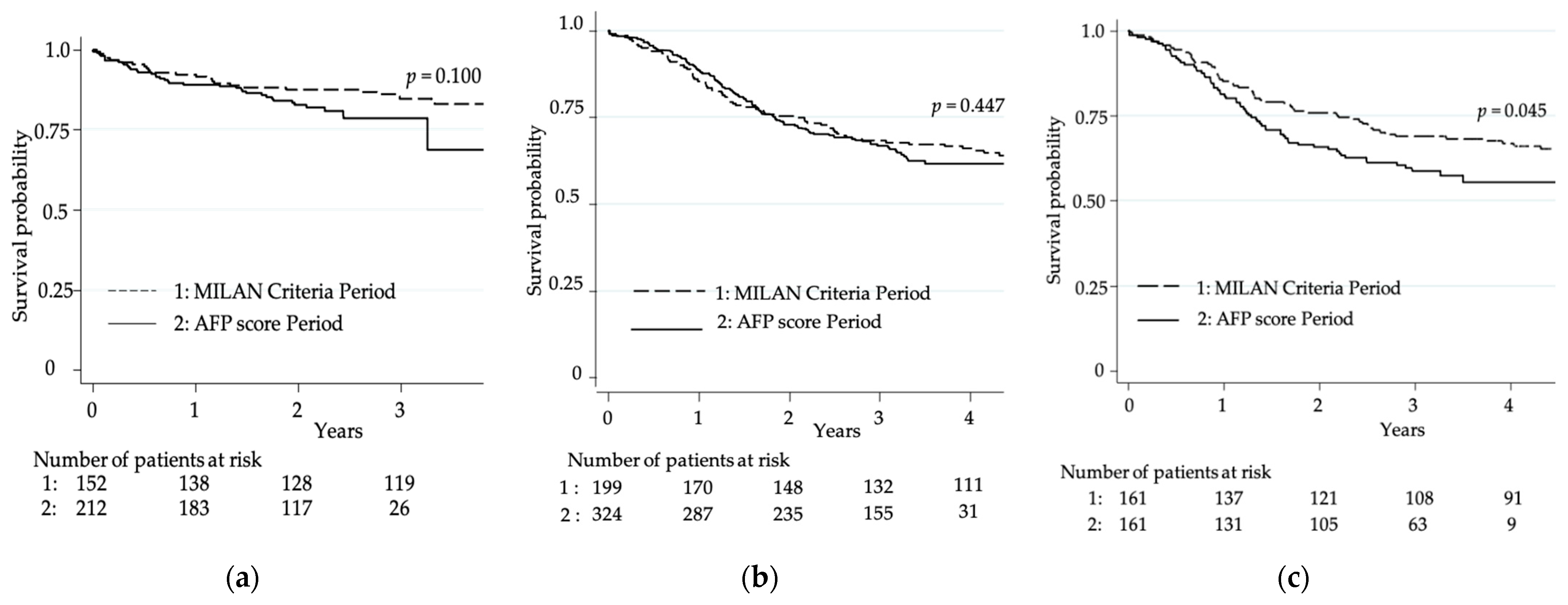
3.4. Overall Survival
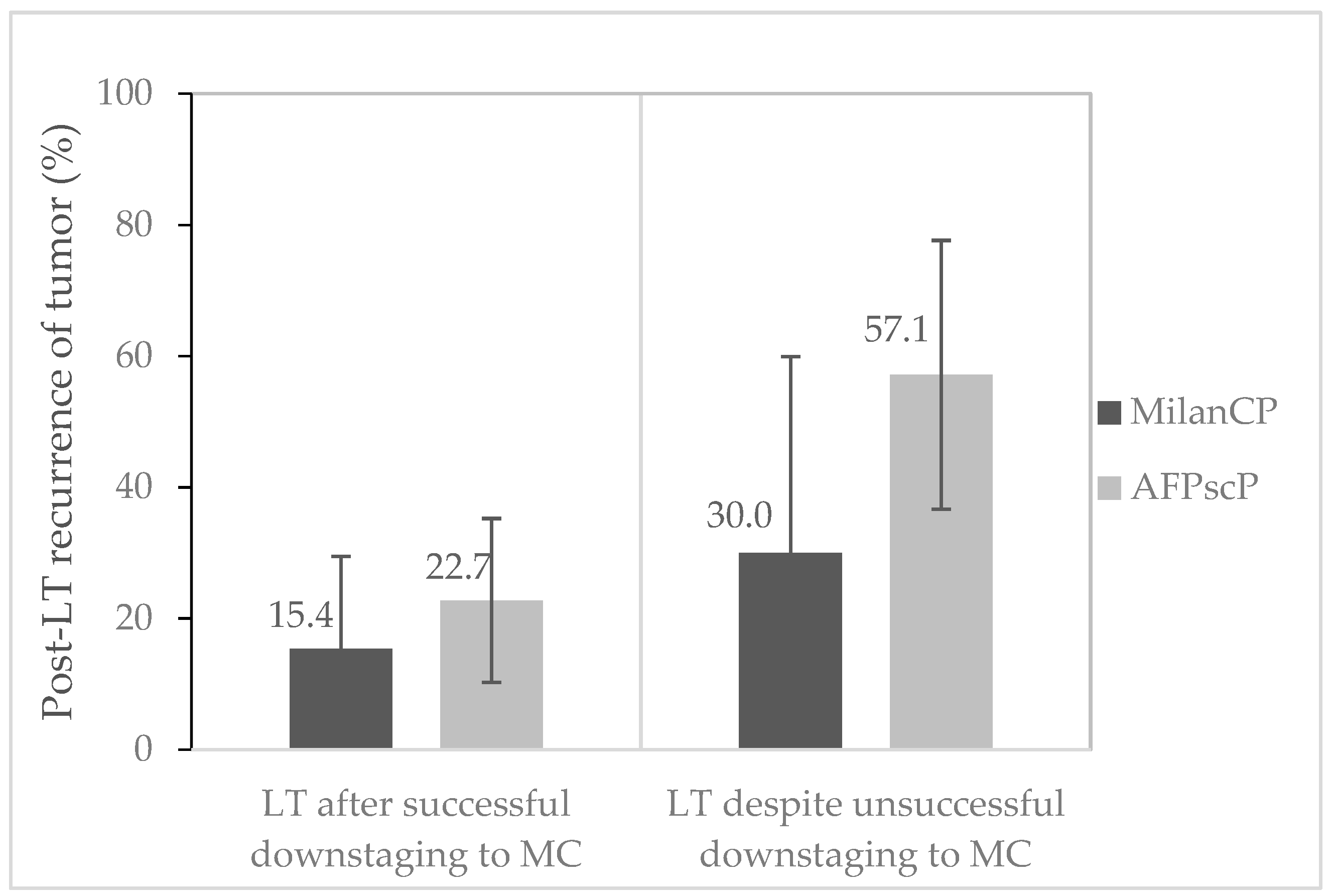
3.5. Downstaging Policy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Clavien, P.-A.; Lesurtel, M.; Bossuyt, P.M.; Gores, G.J.; Langer, B.; Perrier, A. Recommendations for liver transplantation for hepatocellular carcinoma: An international consensus conference report. Lancet Oncol. 2012, 13, e11–e22. [Google Scholar] [CrossRef] [Green Version]
- Mazzaferro, V.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A.; Bozzetti, F.; Montalto, F.; Ammatuna, M.; Morabito, A.; Gennari, L. Liver Transplantation for the Treatment of Small Hepatocellular Carcinomas in Patients with Cirrhosis. N. Engl. J. Med. 1996, 334, 693–699. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Bhoori, S.; Sposito, C.; Bongini, M.; Langer, M.; Miceli, R.; Mariani, L. Milan criteria in liver transplantation for hepatocellular carcinoma: An evidence-based analysis of 15 years of experience. Liver Transpl. 2011, 17, S44–S57. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. Electronic address eee, European Association for the Study of the L. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giard, J.-M.; Mehta, N.; Dodge, J.L.; Roberts, J.P.; Yao, F.Y. Alpha-Fetoprotein Slope >7.5 ng/mL per Month Predicts Microvascular Invasion and Tumor Recurrence after Liver Transplantation for Hepatocellular Carcinoma. Transplantation 2018, 102, 816–822. [Google Scholar] [CrossRef]
- Halazun, K.J.; Tabrizian, P.; Najjar, M.; Florman, S.; Schwartz, M.; Michelassi, F.; Samstein, B.; Brown, R.S.; Emond, J.C.; Busuttil, R.W.; et al. Is it Time to Abandon the Milan Criteria? Results of a Bicoastal US Collaboration to Redefine Hepatocellular Carcinoma Liver Transplantation Selection Policies. Ann. Surg. 2018, 268, 690–699. [Google Scholar] [CrossRef] [PubMed]
- Hameed, B.; Mehta, N.; Sapisochin, G.; Roberts, J.P.; Yao, F.Y. Alpha-fetoprotein level > 1000 ng/mL as an exclusion criterion for liver transplantation in patients with hepatocellular carcinoma meeting the Milan criteria. Liver Transpl. 2014, 20, 945–951. [Google Scholar] [CrossRef]
- Lee, D.D.; Samoylova, M.; Mehta, N.; Musto, K.R.; Roberts, J.P.; Yao, F.Y.; Harnois, D.M. The mRECIST Classification Provides Insight into Tumor Biology for Patients with Hepatocellular Carcinoma Awaiting Liver Transplantation. Liver Transpl. 2019, 25, 228–241. [Google Scholar] [CrossRef] [Green Version]
- Duvoux, C.; Roudot–Thoraval, F.; Decaens, T.; Pessione, F.; Badran, H.; Piardi, T.; Francoz, C.; Compagnon, P.; Vanlemmens, C.; Dumortier, J.; et al. Liver Transplantation for Hepatocellular Carcinoma: A Model Including α-Fetoprotein Improves the Performance of Milan Criteria. Gastroenterology 2012, 143, 986–994.e3. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferro, V.; Sposito, C.; Zhou, J.; Pinna, A.D.; De Carlis, L.; Fan, J.; Cescon, M.; Di Sandro, S.; Yi-Feng, H.; Lauterio, A.; et al. Metroticket 2.0 Model for Analysis of Competing Risks of Death After Liver Transplantation for Hepatocellular Carcinoma. Gastroenterology 2018, 154, 128–139. [Google Scholar] [CrossRef] [Green Version]
- Mazzaferro, V.; Llovet, J.M.; Miceli, R.; Bhoori, S.; Schiavo, M.; Mariani, L.; Camerini, T.; Roayaie, S.; Schwartz, M.E.; Grazi, G.L.; et al. Metroticket Investigator Study Group. Predicting survival after LT in patients with HCC beyond the MC: A retrospective, exploratory analysis. Lancet Oncol. 2009, 10, 35–43. [Google Scholar] [CrossRef]
- Costentin, C.E.; Amaddeo, G.; Decaens, T.; Boudjema, K.; Bachellier, P.; Muscari, F.; Salamé, E.; Bernard, P.; Francoz, C.; Dharancy, S.; et al. Prediction of hepatocellular carcinoma recurrence after liver transplantation: Comparison of four explant-based prognostic models. Liver Int. 2017, 37, 717–726. [Google Scholar] [CrossRef]
- Piñero, F.; Baña, M.T.; De Ataide, E.C.; Duque, S.H.; Marciano, S.; Varón, A.; Anders, M.; Zerega, A.; Menéndez, J.; Zapata, R.; et al. Liver transplantation for hepatocellular carcinoma: Evaluation of the alpha-fetoprotein model in a multicenter cohort from Latin America. Liver Int. 2016, 36, 1657–1667. [Google Scholar] [CrossRef] [PubMed]
- Adler, M.; De Pauw, F.; Vereerstraeten, P.; Fancello, A.; Lerut, J.; Starkel, P.; Van Vlierberghe, H.; Troisi, R.; Donckier, V.; Detry, O.; et al. Outcome of patients with hepatocellular carcinoma listed for liver transplantation within the Eurotransplant allocation system. Liver Transpl. 2008, 14, 526–533. [Google Scholar] [CrossRef] [PubMed]
- Vibert, E.; Azoulay, D.; Hoti, E.; Iacopinelli, S.; Samuel, D.; Salloum, C.; Lemoine, A.; Bismuth, H.; Castaing, D.; Adam, R. Progression of Alphafetoprotein Before Liver Transplantation for Hepatocellular Carcinoma in Cirrhotic Patients: A Critical Factor. Am. J. Transpl. 2009, 10, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Decaens, T.; Roudot-Thoraval, F.; Hadni-Bresson, S.; Meyer, C.; Gugenheim, J.; Durand, F.; Bernard, P.-H.; Boillot, O.; Sulpice, L.; Calmus, Y.; et al. Impact of UCSF criteria according to pre- and post-OLT tumor features: Analysis of 479 patients listed for HCC with a short waiting time. Liver Transpl. 2006, 12, 1761–1769. [Google Scholar] [CrossRef]
- Otto, G.; Schuchmann, M.; Hoppe-Lotichius, M.; Heise, M.; Weinmann, A.; Hansen, T.; Pitton, M.P. How to decide about liver transplantation in patients with hepatocellular carcinoma: Size and number of lesions or response to TACE? J. Hepatol. 2013, 59, 279–284. [Google Scholar] [CrossRef]
- Yao, F.Y.; Mehta, N.; Flemming, J.; Dodge, J.; Hameed, B.; Fix, O.; Hirose, R.; Fidelman, N.; Kerlin, R.K., Jr.; Roberts, J.P. Downstaging of hepatocellular cancer before liver transplant: Long-term outcome compared to tumors within Milan criteria. Hepatology 2015, 61, 1968–1977. [Google Scholar] [CrossRef] [Green Version]
- Agopian, V.G.; Harlander-Locke, M.P.; Ruiz, R.M.; Klintmalm, G.B.; Senguttuvan, S.; Florman, S.S.; Haydel, B.; Hoteit, M.; Levine, M.H.; Lee, D.D.; et al. Impact of Pretransplant Bridging Locoregional Therapy for Patients with Hepatocellular Carcinoma Within Milan Criteria Undergoing Liver Transplantation: Analysis of 3601 Patients from the US Multicenter HCC Transplant Consortium. Ann. Surg. 2017, 266, 525–535. [Google Scholar] [CrossRef]
- Duffy, J.P.; Vardanian, A.; Benjamin, E.; Watson, M.; Farmer, D.G.; Ghobrial, R.M.; Lipshutz, G.; Yersiz, H.; Lu, D.S.K.; Lassman, C.; et al. Liver Transplantation Criteria for Hepatocellular Carcinoma Should Be Expanded: A 22-year experience with 467 patients at UCLA. Ann. Surg. 2007, 246, 502–511. [Google Scholar] [CrossRef] [PubMed]
- Kardashian, A.; Florman, S.S.; Haydel, B.; Ruiz, R.M.; Klintmalm, G.B.; Lee, D.D.; Taner, C.B.; Aucejo, F.; Tevar, A.D.; Humar, A.; et al. Liver Transplantation Outcomes in a U.S. Multicenter Cohort of 789 Patients with Hepatocellular Carcinoma Presenting Beyond Milan Criteria. Hepatology 2020, 72, 2014–2028. [Google Scholar] [CrossRef]
- Mehta, N.; Guy, J.; Frenette, C.T.; Dodge, J.L.; Osorio, R.W.; Minteer, W.B.; Roberts, J.P.; Yao, F.Y. Excellent Outcomes of Liver Transplantation Following Down-Staging of Hepatocellular Carcinoma to Within Milan Criteria: A Multicenter Study. Clin. Gastroenterol. Hepatol. 2018, 16, 955–964. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.; Wang, L.; Chen, J.; Bai, M.; Zhou, C.; Liu, S.; Lin, Q. Regulation of COX-2 expression and epithelial-to-mesenchymal transition by hypoxia-inducible factor-1α is associated with poor prognosis in hepatocellular carcinoma patients post TACE surgery. Int. J. Oncol. 2016, 48, 2144–2154. [Google Scholar] [CrossRef] [PubMed]
- Di Sandro, S.; Bagnardi, V.; Cucchetti, A.; Lauterio, A.; De Carlis, R.; Benuzzi, L.; Danieli, M.; Botta, F.; Centonze, L.; Najjar, M.; et al. From a Philosophical Framework to a Valid Prognostic Staging System of the New “Comprehensive Assessment” for Transplantable Hepatocellular Carcinoma. Cancers 2019, 11, 741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazzaferro, V. Squaring the circle of selection and allocation in liver transplantation for HCC: An adaptive approach. Hepatology 2016, 63, 1707–1717. [Google Scholar] [CrossRef] [Green Version]
- Mehta, N.; Dodge, J.L.; Roberts, J.P.; Yao, F.Y. A novel waitlist dropout score for hepatocellular carcinoma—Identifying a threshold that predicts worse post-transplant survival. J. Hepatol. 2021, 74, 829–837. [Google Scholar] [CrossRef]
- Notarpaolo, A.; Layese, R.; Magistri, P.; Gambato, M.; Colledan, M.; Magini, G.; Miglioresi, L.; Vitale, A.; Vennarecci, G.; Ambrosio, C.D.; et al. Validation of the AFP model as a predictor of HCC recurrence in patients with viral hepatitis-related cirrhosis who had received a liver transplant for HCC. J. Hepatol. 2017, 66, 552–559. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | β Coefficient | Hazard Ratio | Points |
|---|---|---|---|
| Largest diameter, cm | |||
| ≤3 | 0 | 1 | 0 |
| 3–6 | 0.272 | 1.31 | 1 |
| >6 | 1.347 | 3.84 | 4 |
| Number of nodules | |||
| 1–3 | 0 | 1 | 0 |
| ≥4 | 0.696 | 2.01 | 2 |
| AFP level, ng/mL | |||
| ≤100 | 0 | 1 | 0 |
| 100–1000 | 0.668 | 1.95 | 2 |
| >1000 | 0.945 | 2.57 | 3 |
| MilanCP (n = 199) | AFPscP (n = 324) | p Value | |
|---|---|---|---|
| Males (n, %) | 179 (89.9%) | 280 (86.4%) | 0.232 |
| Age at listing (years, median, (IQR)) | 58.7 (53.7–62.9) | 59.4 (52.9–63.2) | 0.639 |
| Cirrhosis (n, %) | 191 (96.0%) | 309 (95.4%) | 0.741 |
| Causes of cirrhosis (n, %) | |||
| Alcohol | 78 (40.8%) | 113 (36.6%) | 0.340 |
| Viral | 50 (26.2%) | 90 (29.1%) | 0.476 |
| Viral + Alcohol | 23 (12%) | 47 (15.2%) | 0.321 |
| NASH | 8 (4.2%) | 12 (3.9%) | 0.866 |
| BASH | 20 (10.5%) | 31 (10%) | 0.875 |
| Others | 12 (6.3%) | 16 (5.2%) | 0.602 |
| Data at diagnosis | |||
| Pretreatment biopsy (n, %) | 48 (24.1%) | 80 (24.7%) | 0.883 |
| Number of tumors (median, (IQR)) | 1 (1–2) | 1 (1–2) | 0.985 |
| Max diameter (mm, median, (IQR)) | 25 (20–35) | 26 (20–38) | 0.367 |
| Sum of diameter (mm, median, (IQR)) | 34 (23–48) | 34 (25–53) | 0.750 |
| AFP value, ng/mL (median, (IQR)) | 10 (5–24.8) | 8.2 (5–21.3) | 0.507 |
| AFPsc diag: ≤2 vs. >2 | 176/23 (88.4% vs. 11.6%) | 279/45 (86.1% vs. 13.9%) | 0.441 |
| Data at listing | |||
| Pre-existing tumor treatment to avoid LT | 52 (26.1%) | 88 (27.2%) | 0.796 |
| Length between diagnosis and listing (days, median, (IQR)) | 270 (132–521) | 238 (130–530) | 0.402 |
| Child–Pugh (n, %) | |||
| A | 91 (45.7%) | 184 (56.8%) | 0.017 |
| B | 60 (30.2%) | 88 (27.2%) | 0.591 |
| C | 48 (24.1%) | 52 (16.1%) | 0.016 |
| MELD score (median, (IQR)) | 10.6 (8.2–15.7) | 9.7 (7.6–14) | 0.063 |
| MELD > 20 (%, n) | 26 (13.6) | 25 (7.7) | 0.045 |
| Number of tumors (median, (IQR)) | 2 (1–3) | 2 (1–3) | 0.147 |
| Largest diameter (median, (IQR)) | 24 (20–33) | 26 (19–36) | 0.428 |
| Sum of diameter (mm, median, (IQR)) | 37 (24–54) | 40 (26–61.5) | 0.139 |
| AFP value, ng/mL (median, (IQR)) | 8 (4.1–20.7) | 7.4 (4–20) | 0.583 |
| Milan criteria: within vs. beyond | 175/24 (87.9 vs. 12.1%) | 278/46 (85.8 vs. 14.2%) | 0.486 |
| AFPsc-listing: ≤2 vs. >2 | 194/5 (97.5% vs. 2.5%) | 307/17 (94.8% vs. 5.2%) | 0.130 |
| Waiting time | |||
| Bridging treatments (n, %) | 150 (75.4%) | 273 (84.3%) | 0.012 |
| Number of treatments (median, (IQR)) | 2 (1–2) (1–5) | 2 (1–3) (1–8) | ≤0.001 |
| Downstaging policy (n, %) | 54 (34.8%) | 92 (33.4%) | 0.771 |
| Unsuccessful downstaging (n, %) | 28/54 (52%) | 48/92 (50%) | 0.971 |
| Dropout of list (n, %, (IQR)) | 47 (23.6%) (17.9–30.1) | 100 (30.9%) (25.9–36.2) | 0.073 |
| Dropout for HCC progression (n, %, (IQR)) | 35 (17.6%) (12.3–22.9) | 67 (18.4%) (14.2–22.6) | 0.926 |
| Number of patients in ‘TCI’ (n, %) | 68 (34%) | 186 (57%) | 0.022 |
| Median ‘TCI’ time/patient (d, median, (IQR)) | 66 (41–153) | 120 (54–374) | ≤0.001 |
| Number of patients still waiting | 0 | 12 | |
| Last imaging before LT | N = 152 | N = 212 | |
| Median time last imaging–LT (days, (IQR)) | 42 (18–74) | 43.5 (21.5–67.5) | 0.999 |
| Number of tumors (median, (IQR)) | 2 (1–3) | 2 (1–3) | 0.340 |
| Largest diameter (median, (IQR)) | 23.5 (18–31) | 27 (20–35) | 0.064 |
| Sum of diameter (mm, median, (IQR)) | 40 (24–60) | 45 (29–76) | 0.085 |
| AFP value, ng/mL (median, (IQR)) | 6 (3.6–19.9) | 6 (3–13) | 0.306 |
| Last Milan criteria: within vs. beyond | 130/21 (86.1% vs. 13.9%) | 186/26 (87.7% vs. 12.3%) | 0.646 |
| Last-AFPsc: ≤2 vs. >2 | 142/9 (94% vs. 6%) | 208/8 (96.2% vs. 3.8%) | 0.331 |
| Transplantation data (n = 364) | N = 152 | N = 212 | |
| Rate of liver transplantation | 76.4% | 69.1% * | 0.008 |
| Median waiting time (months) (IQR) | 7.7 (3.7–12) | 12.3 (8.2–16.1) | <0.001 |
| LT consecutive to downstaging policy | 36/152 (23.7%) | 51/212 (24.1%) | 0.949 |
| Number of tumors (median, (IQR)) | 2 (1–4) (0–20) | 2 (1–4) (0–50) | 0.775 |
| Largest diameter (mm, median, (IQR)) | 25 (15.5–35) | 27.5 (17–37) | 0.320 |
| Sum of diameter (median, (IQR)) | 42 (27–67.5) | 45 (29–77.5) | 0.171 |
| Milan criteria explant: within vs. beyond | 100/52 (65.8% vs. 34.2%) | 150/62 (70.8% vs. 29.2%) | 0.314 |
| AFPsc explant: ≤2 vs. >2 | 133/19 (87.5% vs. 12.5%) | 187/25 (88.2% vs. 11.8%) | 0.838 |
| Cholangiocarcinoma component | 8 (5.3%) | 12 (5.7%) | 0.802 |
| Macrovascular invasion | 13 (8.5%) | 15 (7.1%) | 0.527 |
| Microvascular invasion | 35 (23.0%) | 50 (23.6%) | 0.901 |
| Satellites nodules | 33 (21.7%) | 43 (20.3%) | 0.741 |
| Major differentiation grade | |||
| Not assessable | 58 (38.2%) | 79 (37.3%) | 0.741 |
| Well | 44 (28.9%) | 56 (26.4%) | 0.593 |
| Moderate | 48 (31.6%) | 72 (34%) | 0.633 |
| Poor | 2 (1.3%) | 5 (2.4%) | 0.475 |
| Percentage of tumor necrosis (median) Complete pathological response after bridging treatments | 30.5 (0–82.5) 20/119 (16.8%) | 36 (0–75) 25/179 (14.0%) | 0.965 0.504 |
| Post-transplantation data (n = 364) | N = 152 | N = 212 | |
| Follow-up (years, median, (IQR)) | 4.13 (1.81–4.81) | 2.07 (1.49–2.65) | <0.001 |
| Death (n, %) | 26 (17.1%) | 39 (18.4%) | 0.751 |
| Postoperative related death (n, %) | 12 (8.5%) | 18 (7.2%) | 0.663 |
| Tumor recurrence (n, % (IQR)) | 14 (9.2% (5.1; 15)) | 28 (13.2% (9; 18.5)) | 0.239 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| Risk Factors | OR | 95% CI | p | OR | 95% CI | p |
| AFPscP/MilanCP | 0.94 | 0.50–1.77 | 0.838 | 1.07 | 0.51–2.23 | 0.865 |
| AFPsc diag > 2 | 1.99 | 0.92–4.34 | 0.082 | NS | ||
| Treatment to avoid transplantation | 0.83 | 0.40–1.70 | 0.605 | |||
| Child–Pugh B | 1.58 | 0.79–3.15 | 0.192 | |||
| MELD score > 20 | 0.46 | 0.11–2.00 | 0.300 | |||
| AFPsc listing ‘viable’ > 2 | 1.86 | 0.38–9.04 | 0.443 | |||
| Pre-LT bridging treatments | 2.55 | 0.88–9.04 | 0.085 | NS | ||
| Number of bridging treatments | 1.43 | 1.09–1.86 | 0.009 | NS | ||
| Downstaging policy | 4.38 | 2.28–8.41 | <0.001 | 5.13 | 2.45–10.8 | <0.001 |
| Waiting time > 14.5 months | 1.69 | 0.86–3.32 | 0.128 | |||
| Beyond Milan on last imaging | 5.31 | 2.59–10.9 | <0.001 | NS | ||
| Last AFPsc ‘viable’ > 2 | 33.0 | 10.2–108 | <0.001 | 40.4 | 11.5–142 | <0.001 |
| Milan CP (n = 152) | AFPscP (n = 212) | |||
|---|---|---|---|---|
| Last imaging assessment | Within AFP score | Within Milan criteria | 10/129 (7.8%) | 22/186 (11.8%) |
| Beyond Milan criteria | 1/14 (7.1%) | 2/18 (11.1%) | ||
| Beyond AFP score | Within Milan criteria | 1/2 (50%) | 0 | |
| Beyond Milan criteria | 2/6 (33%) | 4/8 (50%) | ||
| Explant assessment | Within AFP score | Within Milan criteria | 4/100 (4%) | 8/150 (5.3%) |
| Beyond Milan criteria | 4/34 (11.8%) | 8/37 (22%) | ||
| Beyond AFP score | Within Milan criteria | 0 | 0 | |
| Beyond Milan criteria | 6/18 (33%) | 12/25 (48%) |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| Risk Factors | SHR | 95% CI | p | SHR | 95% CI | p |
| AFPscP/MilanCP | 1.82 | 0.96–3.48 | 0.067 | 2.34 | 1.16–4.73 | 0.017 |
| AFPsc diag > 2 | 2.56 | 1.32–4.95 | 0.005 | NS | ||
| αFP value diag > 100 ng/mL | 1.74 | 0.74–4.09 | 0.202 | |||
| Treatment to avoid transplantation | 2.01 | 1.09–3.71 | 0.025 | 2.24 | 1.20–4.17 | 0.011 |
| Number of preemptive treatments | 1.3 | 2.11 | 0.222 | |||
| Child B | 0.90 | 0.45–1.80 | 0.760 | |||
| MELD > 20 | 0.69 | 0.22–2.15 | 0.520 | |||
| AFPsc listing > 2 | 1.87 | 0.50–7.00 | 0.354 | |||
| αFP value listing > 100 ng/mL | 0.68 | 0.10–4.56 | 0.689 | |||
| Pre-LT bridging treatments | 3.43 | 1.08–10.87 | 0.036 | NS | ||
| Number of bridging treatments | 1.37 | 1.13–1.65 | 0.001 | |||
| Downstaging policy | 3.54 | 1.94–6.48 | <0.001 | 2.50 | 1.30–4.81 | 0.006 |
| Waiting time | 1.02 | 0.99–1.05 | 0.274 | |||
| Waiting time > 14.5 months | 2.02 | 1.06–3.84 | 0.032 | NS | ||
| Last AFPsc > 2 | 5.97 | 2.74–13.02 | <0.001 | 2.58 | 1.06–6.30 | 0.038 |
| Last αFP value > 100 ng/mL | 5.26 | 2.59–10.68 | <0.001 | |||
| Macrovascular invasion | 5.98 | 3.07–11.67 | <0.001 | |||
| Microvascular invasion | 5.58 | 3.02–10.33 | <0.001 | 2.61 | 1.17–5.81 | 0.018 |
| Satellites nodules | 2.59 | 1.38–4.84 | 0.003 | |||
| Presence of intermediate differentiation | 3.13 | 1.10–8.94 | 0.033 | |||
| Presence of poor differentiation | 7.55 | 2.28–25.0 | 0.001 | |||
| Necrosis (for 10%) | 0.97 | 0.91–1.05 | 0.472 | |||
| AFPsc explant > 2 | 6.85 | 3.69–12.71 | <0.001 | 2.82 | 1.14–6.99 | 0.025 |
| Cholangiocarcinoma component | 6.98 | 3.46–14.10 | <0.001 | 5.22 | 2.65–10.30 | ≤0.001 |
| Univariate Analysis | Multivariate Analysis | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| If No Recurrence | If Recurrence | ||||||||
| Risk Factors | OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p |
| AFPscP/MilanCP | 1.55 | 0.92–2.63 | 0.103 | NS | 1.95 | 1.00–8.17 | 0.051 | ||
| AFPsc diag > 2 | 1.54 | 0.84–2.83 | 0.165 | ||||||
| αFP value diag > 100 ng/mL | 1.44 | 0.69–3.02 | 0.336 | ||||||
| Treatment to avoid transplantation | 2.02 | 1.24–3.31 | 0.005 | 1.93 | 0.99–3.64 | 0.054 | NS | ||
| Number of preemptive treatments | 1.30 | 0.84–2.01 | 0.231 | ||||||
| Child B | 1.88 | 1.10–3.18 | 0.020 | 2.50 | 1.19–4.16 | 0.012 | 1.77 | 0.85–4.47 | 0.077 |
| MELD > 20 | 1.12 | 0.51–2.46 | 0.778 | ||||||
| AFPsc listing > 2 | 0.53 | 0.07–3.85 | 0.534 | ||||||
| αFP value listing > 100 ng/mL | 1.46 | 0.46–4.66 | 0.520 | ||||||
| Pre-LT bridging treatments | 1.11 | 0.59–2.09 | 0.737 | ||||||
| Number of bridging treatments | 1.18 | 0.94–1.46 | 0.154 | ||||||
| Downstaging policy | 1.70 | 1.02–2.84 | 0.043 | NS | NS | ||||
| Waiting time | 1.02 | 0.98–1.05 | 0.337 | ||||||
| Waiting time > 14.5 months | 1.55 | 0.89–2.70 | 0.119 | ||||||
| Last AFPsc > 2 | 3.06 | 1.46–6.43 | 0.003 | NS | NS | ||||
| Last αFP value > 100 ng/mL | 1.75 | 0.84–3.67 | 0.138 | ||||||
| Macrovascular invasion | 2.75 | 1.47–5.15 | 0.002 | NS | NS | ||||
| Microvascular invasion | 1.35 | 0.79–2.30 | 0.277 | ||||||
| Satellites nodules | 1.13 | 0.649–2.02 | 0.669 | ||||||
| Presence of intermediate differentiation | 1.30 | 0.67–2.51 | 0.443 | ||||||
| Presence of poor differentiation | 3.11 | 1.34–7.21 | 0.008 | NS | NS | ||||
| Necrosis | 0.94 | 0.88–1.01 | 0.075 | ||||||
| AFPsc explant > 2 | 3.44 | 2.01–5.87 | <0.001 | NS | 2.84 | 1.52–9.74 | 0.005 | ||
| Cholangiocarcinoma component | 3.49 | 1.78–6.85 | <0.001 | NS | NS | ||||
| Recurrence | 5.51 | 3.34–9.13 | <0.001 | ||||||
| Secondary other tumors | 2.08 | 0.99–4.35 | 0.053 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brusset, B.; Dumortier, J.; Cherqui, D.; Pageaux, G.-P.; Boleslawski, E.; Chapron, L.; Quesada, J.-L.; Radenne, S.; Samuel, D.; Navarro, F.; et al. Liver Transplantation for Hepatocellular Carcinoma: A Real-Life Comparison of Milan Criteria and AFP Model. Cancers 2021, 13, 2480. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13102480
Brusset B, Dumortier J, Cherqui D, Pageaux G-P, Boleslawski E, Chapron L, Quesada J-L, Radenne S, Samuel D, Navarro F, et al. Liver Transplantation for Hepatocellular Carcinoma: A Real-Life Comparison of Milan Criteria and AFP Model. Cancers. 2021; 13(10):2480. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13102480
Chicago/Turabian StyleBrusset, Bleuenn, Jerome Dumortier, Daniel Cherqui, Georges-Philippe Pageaux, Emmanuel Boleslawski, Ludivine Chapron, Jean-Louis Quesada, Sylvie Radenne, Didier Samuel, Francis Navarro, and et al. 2021. "Liver Transplantation for Hepatocellular Carcinoma: A Real-Life Comparison of Milan Criteria and AFP Model" Cancers 13, no. 10: 2480. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13102480