
Impact of Previous Irradiation on Wound Healing after Negative Pressure Wound Therapy in Head and Neck Cancer Patients—A Systematic Review

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
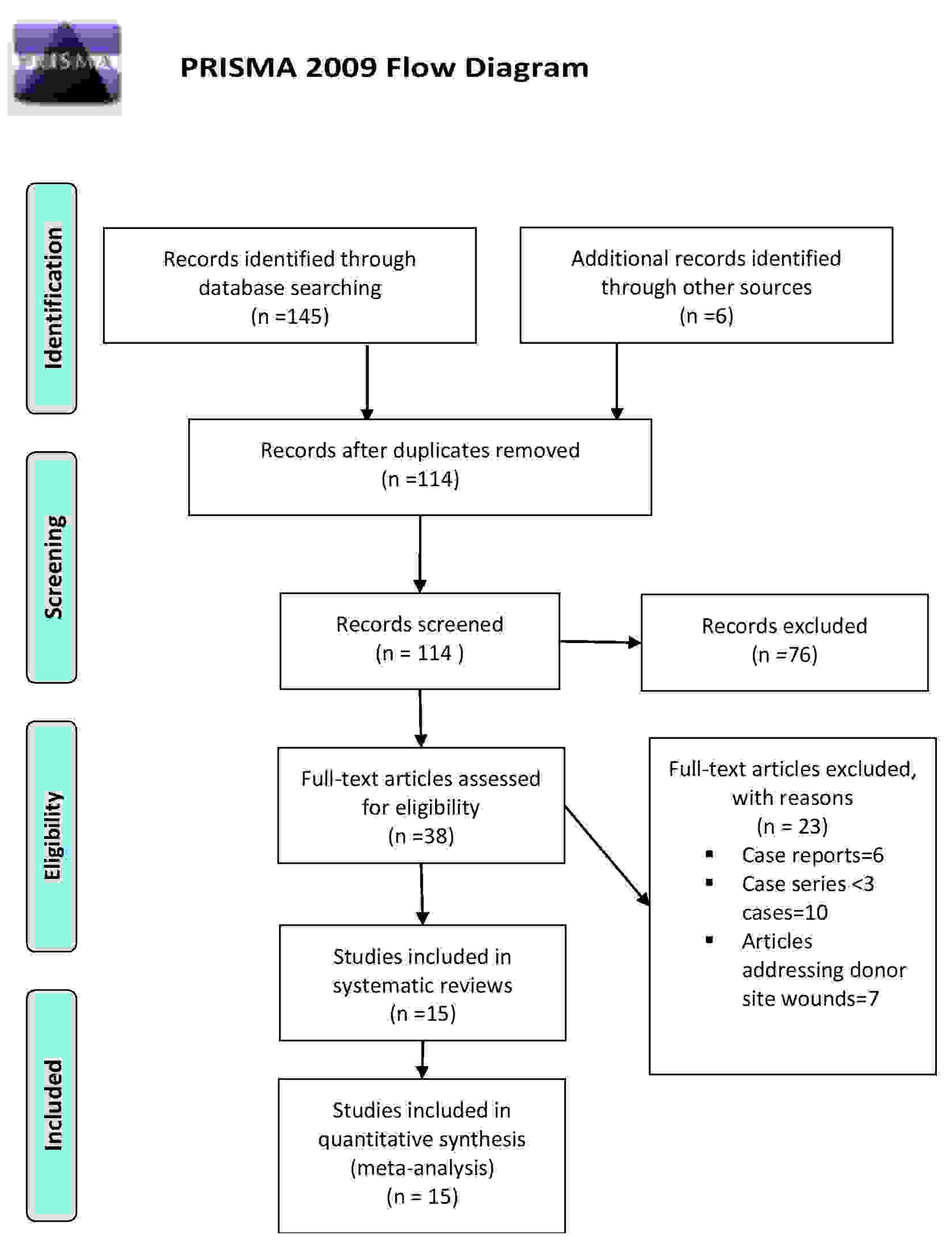
2.1. Search Findings
2.2. Study Cohort
2.3. NPWT Therapy
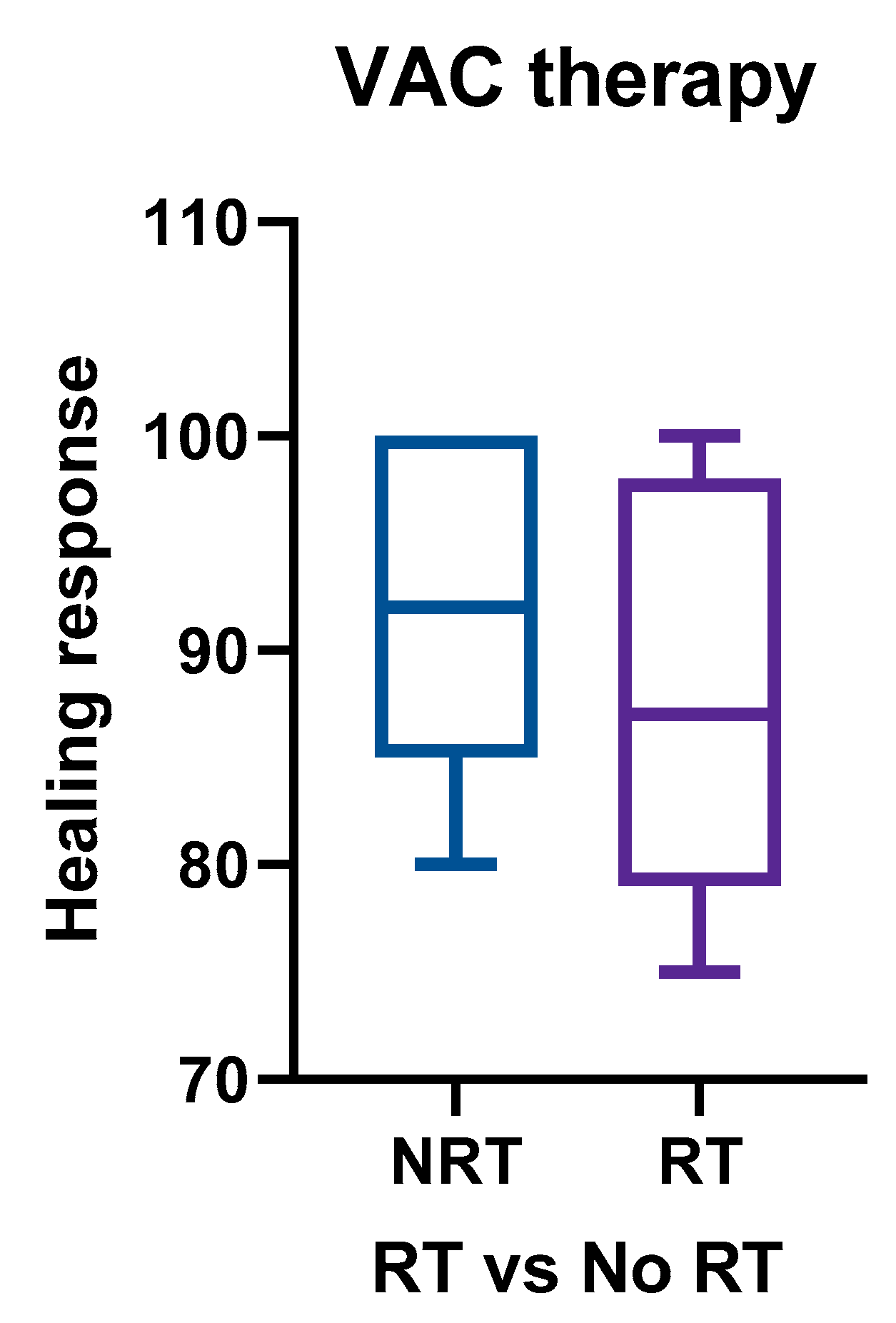
2.4. Risk Factors for Delayed Wound Healing
2.5. Quality of Studies
3. Discussion
4. Materials and Methods
4.1. Literature Search or Data Selection
4.2. Data Collection
4.3. Data Analysis and Statistical Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Armstrong, D.; Lavery, L. Negative pressure wound therapy after partial diabetic foot amputation: A multicenter, randomized controlled trial. Lancet 2005, 366, 1704–1710. [Google Scholar] [CrossRef]
- Atiyeh, B.S.; Gunn, S.W.; Hayek, S.N. State of the Art in Burn Treatment. World J. Surg. 2005, 29, 131–148. [Google Scholar] [CrossRef]
- Banwell, P. Topical negative pressure therapy in wound care. J. Wound Care 1999, 8, 79–84. [Google Scholar] [CrossRef]
- Lemmon, J.A.; Ahmad, J.; Ghavami, A.; Bidic, S.M. Vacuum-Assisted Closure over an External Fixation Device. Plast. Reconstr. Surg. 2008, 121, 234e–235e. [Google Scholar] [CrossRef]
- Argenta, L.C.; Morykwas, M.J. Vacuum-assisted closure: A new method for wound control and treatment: Clinical experience. Ann. Plast. Surg. 1997, 38, 563–577. [Google Scholar] [CrossRef] [PubMed]
- Peinemann, F.; Sauerland, S. Negative-pressure wound therapy: Systematic review of randomized controlled trials. Dtsch. Arztebl. Int. 2011, 108, 381–389. [Google Scholar] [PubMed]
- Morykwas, M.J.; Argenta, L.C.; Shelton-Brown, E.I.; McGuirt, W. Vacuum assisted closure: A new method for wound control and treatment: Animal studies and basic foundation. Ann. Plast. Surg. 1997, 38, 553–562. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.-H.; Jeng, S.-F.; Hsieh, C.-H.; Feng, G.-M.; Chen, C.C. Vacuum-assisted closure for complicated wounds in head and neck region after reconstruction. J. Plast. Reconstr. Aesthet. Surg. 2013, 66, e209–e216. [Google Scholar] [CrossRef] [PubMed]
- Andrews, B.T.; Smith, R.B.; Goldstein, D.P.; Funk, G.F. Management of complicated head and neck wounds with vacuum-assisted closure system. Head Neck 2006, 28, 974–981. [Google Scholar] [CrossRef]
- Andrews, B.T.; Smith, R.B.; Hoffman, H.T.; Funk, G.F. Orocutaneous and pharyngocutaneous fistula closure using a vacuum-assisted closure system. Ann. Otol. Rhinol. Laryngol. 2008, 117, 298–302. [Google Scholar] [CrossRef]
- Asher, S.A.; White, H.N.; Golden, J.B.; Magnuson, J.S.; Carroll, W.R.; Rosenthal, E.L. Negative Pressure Wound Therapy in Head and Neck Surgery. JAMA Facial Plast. Surg. 2014, 16, 120–126. [Google Scholar] [CrossRef] [Green Version]
- Asher, S.A.; White, H.N.; Illing, E.A.; Carroll, W.R.; Magnuson, J.S.; Rosenthal, E.L. Intraluminal Negative Pressure Wound Therapy for Optimizing Pharyngeal Reconstruction. JAMA Otolaryngol. Neck Surg. 2014, 140, 143. [Google Scholar] [CrossRef] [Green Version]
- Dhir, K.; Reino, A.J.; Lipana, J. Vacuum-assisted closure therapy in the management of head and neck wounds. Laryngoscope 2009, 119, 54–61. [Google Scholar] [CrossRef]
- Dorneden, A.; Olson, G.; Boyd, N. Negative Pressure Wound Therapy (Wound VAC) in the Treatment of Chylous Fistula After Neck Dissection. Ann. Otol. Rhinol. Laryngol. 2019, 128, 569–574. [Google Scholar] [CrossRef]
- Inatomi, Y.; Kadota, H.; Yoshida, S.; Kamizono, K.; Shimamoto, R.; Fukushima, S.; Miyashita, K.; Matsuo, M.; Yasumatsu, R.; Tanaka, S.; et al. Utility of negative-pressure wound therapy for orocutaneous and pharyngocutaneous fistula following head and neck surgery. Head Neck 2020, 42, 103–110. [Google Scholar] [CrossRef]
- Lin, P.-Y.; Liou, T.-L.; Lin, K.-C.; Hsieh, M.-H.; Chien, C.-Y.; Hsieh, C.-H. Immediate Negative Pressure Wound Therapy after Free Flap Transfer for Head and Neck Cancer Surgery. Laryngoscope 2018, 128, 2478–2482. [Google Scholar] [CrossRef]
- Reiter, M.; Harreus, U. Vacuum assisted closure in the management of wound healing disorders in the head and neck: A retro-spective analysis of 23 cases. Am. J. Otolaryngol. 2013, 34, 411–415. [Google Scholar] [CrossRef]
- Rosenthal, E.L.; Blackwell, K.E.; McGrew, B.; Carroll, W.R.; Peters, G.E. Use of negative pressure dressings in head and neck recon-struction. Head Neck 2005, 27, 970–975. [Google Scholar] [CrossRef]
- Satteson, E.S.; Crantford, J.C.; Wood, J.; David, L.R. Outcomes of Vacuum-Assisted Therapy in the Treatment of Head and Neck Wounds. J. Craniofacial Surg. 2015, 26, e599–e602. [Google Scholar] [CrossRef]
- Tian, B.; Iyer, N.G.; Tan, H.K.; Tay, A.C.; Soo, K.C.; Tan, N.C. Novel technique of creating a seal for the vacuum-assisted closure system application in complex head and neck wounds. Head Neck 2016, 38, E2523–E2526. [Google Scholar] [CrossRef]
- Thierauf, J.; Wiggenhauser, P.S.; Hoffmann, T.K.; Greve, J.; Scheithauer, M.; Veit, J.A. Anwendung von Vakuum-Wundtherapie bei Spalthaut-Transplantaten im Kopf-Hals-Bereich [Application of vacuum wound therapy with split thickness skin grafts in the head and neck area]. Laryngorhinootologie 2018, 97, 474–479. [Google Scholar] [PubMed]
- Umezawa, H.; Matsutani, T.; Yokoshima, K.; Nakamizo, M.; Ogawa, R. A Novel Tube-Drainage Technique of Negative Pressure Wound Therapy for Fistulae after Reconstructive Surgery. Plast. Reconstr. Surg. Glob. Open 2018, 6, e1885. [Google Scholar] [CrossRef] [PubMed]
- National Heart, Lung and Blood Institute; National Institutes of Health; US Department of Health and Human Services. Study Quality Assessment Tools. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 20 January 2020).
- Ovington, L.G. The evolution of wound management: Ancient origins and advances of the past 20 years. Home Health Nurse 2002, 20, 652–656. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, W.; Strecker, W.; Bombelli, M.; Kinzl, L. Vacuum sealing as treatment of soft tissue damage in open fractures. Unfallchirurg 1993, 96, 488–492. (In German) [Google Scholar]
- Fleischmann, W.; Lang, E.; Klinzl, L. Vacuum assisted wound closure after dermatofasciotomy of the lower extremity. Unfallchirurg 1996, 99, 283–287. (In German) [Google Scholar]
- Fleischmann, W.; Russ, M.; Marquardt, C. Closure of defect wounds by vacuum sealing with instrumental skin expansion. Unfallchirurg 1996, 99, 970–974. (In German) [Google Scholar] [CrossRef]
- Fleischmann, W.; Lang, E.; Russ, M. Treatment of infection by vacuum sealing. Unfallchirurg 1997, 100, 301–304. (In German) [Google Scholar] [CrossRef]
- Palm, H.G.; Hauer, T.; Simon, C.; Willy, C. Vacuum-assisted closure of head and neck wounds. HNO 2011, 59, 819–830. (In German) [Google Scholar] [CrossRef]
- Parsons, J.T.; Mendenhall, W.M.; Stringer, S.P.; Cassisi, N.J.; Million, R.R. An analysis of factors influencing the outcome of postoper-ative irradiation for squamous cell carcinoma of the oral cavity. Int. J. Radiat. Oncol. Biol. Phys. 1997, 39, 137–148. [Google Scholar] [CrossRef]
- Johnston, J.; Mariano, F.; Vokes, D. Negative pressure dressing around the airway. N. Z. Med. J. 2013, 126, 74–78. [Google Scholar]
- Poglio, G.; Grivetto, F.; Nicolotti, M.; Arcuri, F.; Benech, A. Management of an Exposed Mandibular Plate After Fibula Free Flap With Vacuum-Assisted Closure System. J. Craniofacial Surg. 2011, 22, 905–908. [Google Scholar] [CrossRef] [PubMed]
- Benech, A.; Arcuri, F.; Poglio, G.; Brucoli, M.; Guglielmetti, R.; Crespi, M.; Pia, F. Vacuum-assisted closure therapy in reconstructive surgery. Acta Otorhinolaryngol. Ital. 2012, 32, 192–197. [Google Scholar] [PubMed]
- Mouës, C.; Heule, F.; Hovius, S. A review of topical negative pressure therapy in wound healing: Sufficient evidence? Am. J. Surg. 2011, 201, 544–556. [Google Scholar] [CrossRef]
- Borgquist, O.; Ingemansson, R.; Malmsjö, M. Wound Edge Microvascular Blood Flow during Negative-Pressure Wound Therapy: Examining the Effects of Pressures from −10 to −175 mmHg. Plast. Reconstr. Surg. 2010, 125, 502–509. [Google Scholar] [CrossRef]
- Mir, A.; Guys, N.; Bs, K.A.; Svider, P.F.; Rayess, H.; Zuliani, G.; Raza, S.N.; Lin, H. Negative Pressure Wound Therapy in the Head and Neck: An Evidence-Based Approach. Laryngoscope 2019, 129, 671–683. [Google Scholar] [CrossRef] [PubMed]
- Loaec, E.; Vaillant, P.-Y.; Bonne, L.; Marianowski, R. Negative-pressure wound therapy for the treatment of pharyngocutaneous fistula. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2014, 131, 351–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz, S.R.; Yueh, B.; Maynard, C.; Daley, J.; Henderson, W.; Khuri, S.F. Predictors of wound complications after laryngectomy: A study of over 2000 patients. Otolaryngol. Head Neck Surg. 2004, 131, 61–68. [Google Scholar] [CrossRef]
- Bohannon, I.A.; Carroll, W.R.; Magnuson, J.S.; Rosenthal, E.L. Closure of post-laryngectomy pharyngocutaneous fistulae. Head Neck Oncol. 2011, 3, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Clare, M.P.; Fitzgibbons, T.C.; McMullen, S.T.; Stice, R.C.; Hayes, D.F.; Henkel, L. Experience with the Vacuum Assisted Closure Negative Pressure Technique in the Treatment of Non-healing Diabetic and Dysvascular Wounds. Foot Ankle Int. 2002, 23, 896–901. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Lavery, A.L.; Abu-Rumman, P.; Espensen, E.H.; Vazquez, J.R.; Nixon, B.P.; Boulton, A.J. Outcomes of sub atmospheric pressure wound dressing therapy on wound of the diabetic foot. Ostomy Wound Manag. 2002, 48, 64–68. [Google Scholar]
- Kwon, D.; Genden, E.M.; De Bree, R.; Rodrigo, J.P.; Rinaldo, A.; Sanabria, A.; Rapidis, A.D.; Takes, R.P.; Ferlito, A. Overcoming wound complications in head and neck salvage surgery. Auris Nasus Larynx 2018, 45, 1135–1142. [Google Scholar] [CrossRef] [PubMed]
- Herle, P.; Shukla, L.; Morrison, W.A.; Shayan, R. Preoperative radiation and free flap outcomes for head and neck reconstruction: A systematic review and meta-analysis. ANZ J. Surg. 2015, 85, 121–127. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Study Type | Year of Publication | N | Age (in Years) | M:F | Pressure Mode | Negative Pressure | Comorbidity | Previous Irradiation (N) | Healing Response | Complication |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Andrew [9] | 2006 | Retrospective case series | 12 | 67 | 8:4 | - | 125 | DM *-2 CAD *-2 HTN *-7 Pulmonary disease-7 | 1 | 100 | - |
| Andrew [10] | 2008 | Case series | 3 | 67 | 2:1 | - | 150 | 2 | 66 | ||
| Asher [11] | 2014 | Retrospective cohort | 108 | 64 | 87:28 | Continuous | 125 | - | 47 | 75 | Bleeding Retained sponge |
| Asher [12] | 2014 | Retrospective cohort | 12 | 63 | 6:7 | Continuous | 125 | DM *-4 Hypothyroidism-6 Malnutrition-6 | 9 | 92 | - |
| Dhir [13] | 2009 | Retrospective cohort | 19 | 63 | 17:2 | Continuous | 110 | DM *-8 HTN *-16 Malnutrition-9 CAD *-6 PVD *-7 | 10 | 84 | - |
| Dorneden [14] | 2019 | Case series | 3 | 66 | 1:2 | Continuous | 125 | - | 0 | 100 | Electrolyte loss |
| Inatomi [15] | 2019 | Retrospective cohort | 32 | 63 | 28:6 | - | 125 | - | 14 | 82 | None |
| Lin [16] | 2018 | Retrospective series | 31 | 52 | 29:2 | - | 100 | DM *-5 HTN *-6 | 0 | 90 | - |
| Reiter [17] | 2013 | Retrospective cohort | 23 | 58 | 12:0 | Continuous | 125 | HTN *-3 | 11 | 78 | None |
| Rosenthal [18] | 2005 | Retrospective series | 14 | 59 | 14:5 | Continuous | 125 | - | 0 | 86 | None |
| Satteson [19] | 2015 | Retrospective cohort | 69 | 66 | 45:25 | Continuous | - | Smoking-30 HTN *-35 DM *-17 | 36 | 90 | Infection Hematoma Seroma |
| Tian [20] | 2016 | Case series | 4 | 55 | 3:1 | - | - | - | 0 | - | None |
| Thierauf [21] | 2018 | Retrospective case series | 20 | 8:5 | 70 | DM *-3 PVD *-1 HIV *-1 RA *-1 | 7 | 110 | None | ||
| Umezawa [22] | 2018 | Case series | 17 | 67 | 10:1 | - | 6 | 100 | Contact dermatitis | ||
| Yang [8] | 2013 | Case series | 13 | 50 | 13:0 | Continuous | 125 | DM *-4 HTN *-2 CVA *-1 | 0 | 92 | None |
| Variable | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| OR | p | 95% CI | OR | p | 95% CI | |
| Sex (Female) | 2.26 | 0.103 | 0.85–6.0 | 2.01 | 0.223 | 0.66–6.15 |
| RT (Yes) | 4.34 | 0.005 | 1.54–11.6 | 4.07 | 0.010 | 1.39–11.9 |
| DM (Yes) | 5.65 | <0.001 | 2.14–14.9 | 5.62 | 0.001 | 2.01–15.6 |
| RT and DM (Yes) * | 10.6 | <0.001 | 3.38–33.3 | |||
| Malnutrition (Yes) | 1.34 | 0.671 | 0.35–5.21 | |||
| PVD (Yes) | 1.17 | 0.889 | 0.13–10.2 | |||
| Hypothyroidism (Yes) | 0.86 | 0.889 | 0.10–7.52 | |||
| Authors | Study Design | Clear Study Objective | Sample Size Justification | Association/Assessed Levels of Exposure on Outcome | Exposure Defined/Exposure Assessed Repeatedly | Clearly Define Outcome | Clearly Statistic Defined | Follow Up > 80% | Confounding Variables Measured | Rating |
|---|---|---|---|---|---|---|---|---|---|---|
| Andrew [9] | Retrospective case series | +/+ | + | +/+/+ | +/+ | + | + | + | NR * | Good |
| Andrew [10] | Case series | +/+ | NR * | + | +/+ | CD * | + | + | NR * | Fair |
| Asher [11] | Retrospective cohort | +/+ | + | +/+/+ | +/+ | + | + | + | + | Good |
| Asher [12] | Retrospective cohort | +/+ | + | +/+/+ | +/+ | + | + | + | + | Good |
| Dhir [13] | Retrospective cohort | +/+ | + | +/+/+ | +/+ | + | + | + | + | Good |
| Dorneden [14] | Case series | + | CD * | +/+/+ | +/+ | CD * | + | + | NR * | Fair |
| Inatomi [15] | Retrospective cohort | +/+ | + | +/+/+ | +/+ | + | + | + | + | Good |
| Lin [16] | Retrospective series | +/+ | + | +/+/+ | + | + | + | + | CD * | Good |
| Reiter [17] | Retrospective cohort | +/+ | + | +/+/+ | + | + | + | + | + | Good |
| Rosenthal [18] | Retrospective series | +/+ | + | +/+/+ | + | + | + | + | + | Good |
| Satteson [19] | Retrospective cohort | +/+ | + | +/+/+ | + | + | + | + | + | Good |
| Tian [20] | Case series | + | CD * | + | + | + | + | + | NR * | Fair |
| Thierauf [21] | Retrospective case series | + | + | + | + | + | + | + | + | Good |
| Umezawa [22] | Case series | + | + | +/+ | + | + | + | + | CD * | Good |
| Yang [8] | Case series | + | + | +/+/+ | + | + | + | + | + | Good |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faisal, M.; Berend, P.D.; Seemann, R.; Janik, S.; Grasl, S.; Ritzengruber, A.; Mendel, H.; Jamshed, A.; Hussain, R.; Erovic, B.M. Impact of Previous Irradiation on Wound Healing after Negative Pressure Wound Therapy in Head and Neck Cancer Patients—A Systematic Review. Cancers 2021, 13, 2482. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13102482
Faisal M, Berend PD, Seemann R, Janik S, Grasl S, Ritzengruber A, Mendel H, Jamshed A, Hussain R, Erovic BM. Impact of Previous Irradiation on Wound Healing after Negative Pressure Wound Therapy in Head and Neck Cancer Patients—A Systematic Review. Cancers. 2021; 13(10):2482. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13102482
Chicago/Turabian StyleFaisal, Muhammad, Peter D. Berend, Rudolf Seemann, Stefan Janik, Stefan Grasl, Andrea Ritzengruber, Herbert Mendel, Arif Jamshed, Raza Hussain, and Boban M. Erovic. 2021. "Impact of Previous Irradiation on Wound Healing after Negative Pressure Wound Therapy in Head and Neck Cancer Patients—A Systematic Review" Cancers 13, no. 10: 2482. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13102482