
Expression of Cancer Testis Antigens in Tumor-Adjacent Normal Liver Is Associated with Post-Resection Recurrence of Hepatocellular Carcinoma

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients, Materials, and Methods
2.1. HCC Patients and Tissues
2.2. Selection of CTAs
2.3. Quantitative Real-Time PCR
2.4. Immunohistochemistry
2.5. Statistical Analysis
3. Results
3.1. A Panel of 12 CTAs Is Expressed in More Than 10% of HCC Tumors and Not in Healthy Tissues
3.2. CTAs Are Expressed in Tumor-Free Liver Tissues of HCC Patients
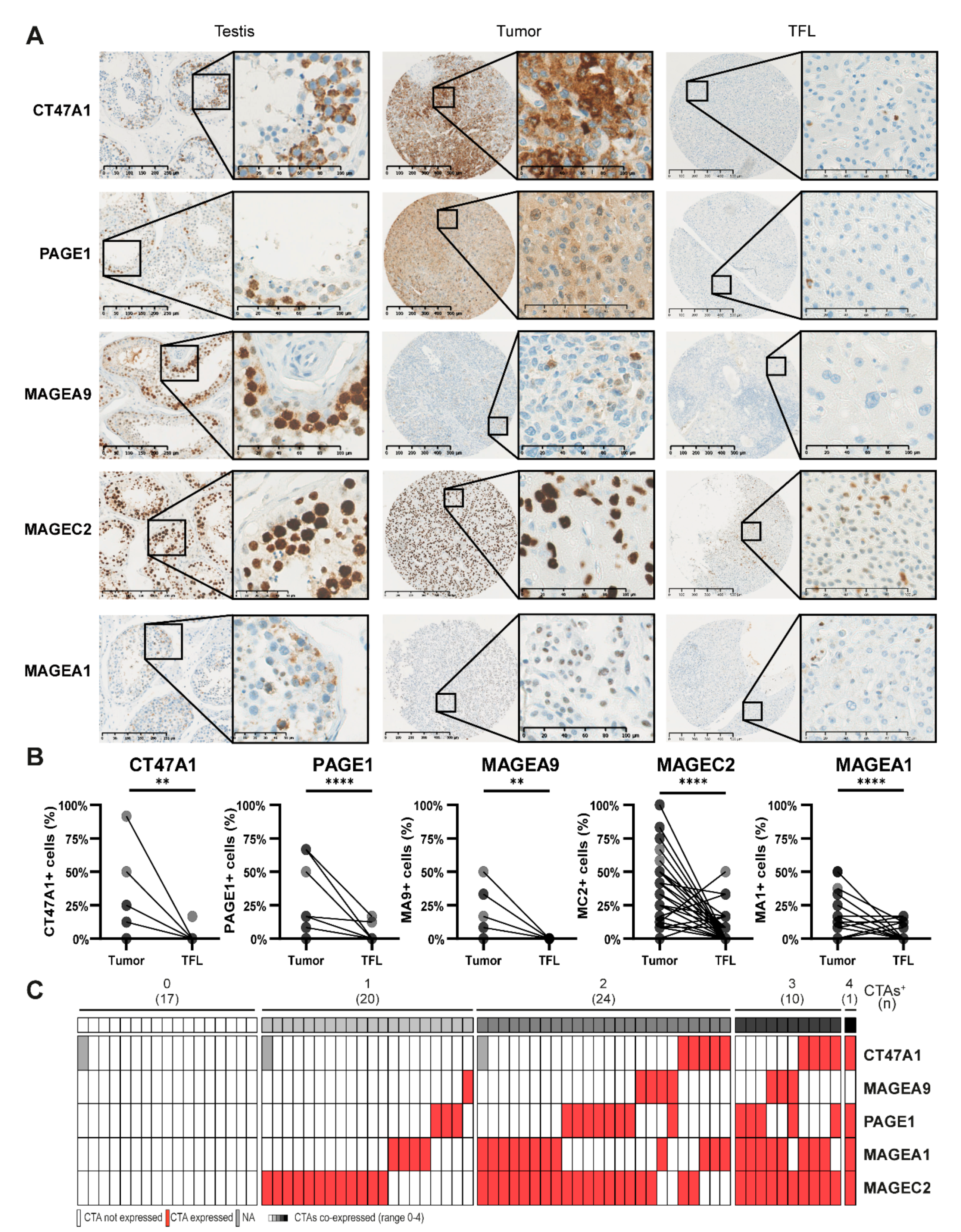
3.3. CTAs Are Expressed on Protein Level in HCC Tumors and TFL
3.4. CTA Expression in TFL Is Correlated with Early HCC Recurrence and HCC-Specific Survival after Surgical Resection
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 389, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Ulahannan, S.V.; Duffy, A.G.; McNeel, T.S.; Kish, J.K.; Dickie, L.A.; Rahma, O.E.; McGlynn, K.A.; Greten, T.F.; Altekruse, S.F. Earlier presentation and application of curative treatments in hepatocellular carcinoma. Hepatology 2014, 60, 1637–1644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poon, R.T. Differentiating early and late recurrences after resection of HCC in cirrhotic patients: Implications on surveillance, prevention, and treatment strategies. Ann. Surg. Oncol. 2009, 16, 792–794. [Google Scholar] [CrossRef] [PubMed]
- Finkelstein, S.D.; Marsh, W.; Demetris, A.J.; Swalsky, P.A.; Sasatomi, E.; Bonham, A.; Subotin, M.; Dvorchik, I. Microdissection-based allelotyping discriminates de novo tumor from intrahepatic spread in hepatocellular carcinoma. Hepatology 2003, 37, 871–879. [Google Scholar] [CrossRef]
- Hoshida, Y.; Villanueva, A.; Kobayashi, M.; Peix, J.; Chiang, D.Y.; Camargo, A.; Gupta, S.; Moore, J.; Wrobel, M.J.; Lerner, J.; et al. Gene expression in fixed tissues and outcome in hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 1995–2004. [Google Scholar] [CrossRef] [Green Version]
- Gjerstorff, M.F.; Andersen, M.H.; Ditzel, H.J. Oncogenic cancer/testis antigens: Prime candidates for immunotherapy. Oncotarget 2015, 6, 15772–15787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofmann, O.; Caballero, O.L.; Stevenson, B.J.; Chen, Y.T.; Cohen, T.; Chua, R.; Maher, C.A.; Panji, S.; Schaefer, U.; Kruger, A.; et al. Genome-wide analysis of cancer/testis gene expression. Proc. Natl. Acad. Sci USA 2008, 105, 20422–20427. [Google Scholar] [CrossRef] [Green Version]
- Whitehurst, A.W. Cause and consequence of cancer/testis antigen activation in cancer. Annu. Rev. Pharmacol. Toxicol. 2014, 54, 251–272. [Google Scholar] [CrossRef]
- Altman, D.G.; McShane, L.M.; Sauerbrei, W.; Taube, S.E. Reporting Recommendations for Tumor Marker Prognostic Studies (REMARK): Explanation and elaboration. PLoS Med. 2012, 9, e1001216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, A.; Bashir, M.R.; Corwin, M.T.; Cruite, I.; Dietrich, C.F.; Do, R.K.G.; Ehman, E.C.; Fowler, K.J.; Hussain, H.K.; Jha, R.C.; et al. Evidence Supporting LI-RADS Major Features for CT- and MR Imaging-based Diagnosis of Hepatocellular Carcinoma: A Systematic Review. Radiology 2018, 286, 29–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charoentong, P.; Finotello, F.; Angelova, M.; Mayer, C.; Efremova, M.; Rieder, D.; Hackl, H.; Trajanoski, Z. Pan-cancer Immunogenomic Analyses Reveal Genotype-Immunophenotype Relationships and Predictors of Response to Checkpoint Blockade. Cell Rep. 2017, 18, 248–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, N.Y.; Hallstrom, B.M.; Fagerberg, L.; Ponten, F.; Kawaji, H.; Carninci, P.; Forrest, A.R.; Fantom, C.; Hayashizaki, Y.; Uhlen, M.; et al. Complementing tissue characterization by integrating transcriptome profiling from the Human Protein Atlas and from the FANTOM5 consortium. Nucleic Acids Res. 2015, 43, 6787–6798. [Google Scholar] [CrossRef] [Green Version]
- Keen, J.C.; Moore, H.M. The Genotype-Tissue Expression (GTEx) Project: Linking Clinical Data with Molecular Analysis to Advance Personalized Medicine. J. Pers. Med. 2015, 5, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Lizio, M.; Abugessaisa, I.; Noguchi, S.; Kondo, A.; Hasegawa, A.; Hon, C.C.; de Hoon, M.; Severin, J.; Oki, S.; Hayashizaki, Y.; et al. Update of the FANTOM web resource: Expansion to provide additional transcriptome atlases. Nucleic Acids Res. 2019, 47, D752–D758. [Google Scholar] [CrossRef] [Green Version]
- Schnieders, F.; Dork, T.; Arnemann, J.; Vogel, T.; Werner, M.; Schmidtke, J. Testis-specific protein, Y-encoded (TSPY) expression in testicular tissues. Hum. Mol Genet. 1996, 5, 1801–1807. [Google Scholar] [CrossRef] [Green Version]
- Sideras, K.; Bots, S.J.; Biermann, K.; Sprengers, D.; Polak, W.G.; Jn, I.J.; de Man, R.A.; Pan, Q.; Sleijfer, S.; Bruno, M.J.; et al. Tumour antigen expression in hepatocellular carcinoma in a low-endemic western area. Br. J. Cancer 2015, 112, 1911–1920. [Google Scholar] [CrossRef] [Green Version]
- Aufhauser, D.D., Jr.; Sadot, E.; Murken, D.R.; Eddinger, K.; Hoteit, M.; Abt, P.L.; Goldberg, D.S.; DeMatteo, R.P.; Levine, M.H. Incidence of Occult Intrahepatic Metastasis in Hepatocellular Carcinoma Treated With Transplantation Corresponds to Early Recurrence Rates After Partial Hepatectomy. Ann. Surg. 2018, 267, 922–928. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.P.; Bao, Z.W.; Wu, J.B.; Chen, Y.H.; Chen, J.R.; Xie, H.Y.; Zhou, L.; Wu, J.; Zheng, S.S. Cancer-Testis Gene Expression in Hepatocellular Carcinoma: Identification of Prognostic Markers and Potential Targets for Immunotherapy. Technol. Cancer Res. Treat. 2020, 19, 1533033820944274. [Google Scholar] [CrossRef]
- Beije, N.; Helmijr, J.C.; Weerts, M.J.A.; Beaufort, C.M.; Wiggin, M.; Marziali, A.; Verhoef, C.; Sleijfer, S.; Jansen, M.; Martens, J.W.M. Somatic mutation detection using various targeted detection assays in paired samples of circulating tumor DNA, primary tumor and metastases from patients undergoing resection of colorectal liver metastases. Mol. Oncol. 2016, 10, 1575–1584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, S.J.; Soria, J.C.; Wang, L.; Hassan, K.A.; Morice, R.C.; Walsh, G.L.; Hong, W.K.; Mao, L. Activation of melanoma antigen tumor antigens occurs early in lung carcinogenesis. Cancer Res. 2001, 61, 7959–7963. [Google Scholar] [PubMed]
- Wong, S.Y.; Hynes, R.O. Lymphatic or hematogenous dissemination: How does a metastatic tumor cell decide? Cell Cycle. 2006, 5, 812–817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, D.; Pereira, E.R.; Padera, T.P. Growth and Immune Evasion of Lymph Node Metastasis. Front. Oncol. 2018, 8, 36. [Google Scholar] [CrossRef] [Green Version]
- Nathanson, S.D. Insights into the mechanisms of lymph node metastasis. Cancer 2003, 98, 413–423. [Google Scholar] [CrossRef]
- Hollingsworth, R.E.; Jansen, K. Turning the corner on therapeutic cancer vaccines. NPJ Vaccines 2019, 4, 7. [Google Scholar] [CrossRef]
- Andersen, R.S.; Thrue, C.A.; Junker, N.; Lyngaa, R.; Donia, M.; Ellebaek, E.; Svane, I.M.; Schumacher, T.N.; Thor Straten, P.; Hadrup, S.R. Dissection of T-cell antigen specificity in human melanoma. Cancer Res. 2012, 72, 1642–1650. [Google Scholar] [CrossRef] [Green Version]
- Flecken, T.; Schmidt, N.; Hild, S.; Gostick, E.; Drognitz, O.; Zeiser, R.; Schemmer, P.; Bruns, H.; Eiermann, T.; Price, D.A.; et al. Immunodominance and functional alterations of tumor-associated antigen-specific CD8+ T-cell responses in hepatocellular carcinoma. Hepatology 2014, 59, 1415–1426. [Google Scholar] [CrossRef] [Green Version]
- Bricard, G.; Bouzourene, H.; Martinet, O.; Rimoldi, D.; Halkic, N.; Gillet, M.; Chaubert, P.; Macdonald, H.R.; Romero, P.; Cerottini, J.C.; et al. Naturally acquired MAGE-A10- and SSX-2-specific CD8+ T cell responses in patients with hepatocellular carcinoma. J. Immunol. 2005, 174, 1709–1716. [Google Scholar] [CrossRef] [Green Version]
- Zhou, G.; Sprengers, D.; Boor, P.P.C.; Doukas, M.; Schutz, H.; Mancham, S.; Pedroza-Gonzalez, A.; Polak, W.G.; de Jonge, J.; Gaspersz, M.; et al. Antibodies Against Immune Checkpoint Molecules Restore Functions of Tumor-Infiltrating T Cells in Hepatocellular Carcinomas. Gastroenterology 2017, 153, 1107–1119.e10. [Google Scholar] [CrossRef] [PubMed]
- Shang, X.Y.; Chen, H.S.; Zhang, H.G.; Pang, X.W.; Qiao, H.; Peng, J.R.; Qin, L.L.; Fei, R.; Mei, M.H.; Leng, X.S.; et al. The spontaneous CD8+ T-cell response to HLA-A2-restricted NY-ESO-1b peptide in hepatocellular carcinoma patients. Clin. Cancer Res. 2004, 10, 6946–6955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inada, Y.; Mizukoshi, E.; Seike, T.; Tamai, T.; Iida, N.; Kitahara, M.; Yamashita, T.; Arai, K.; Terashima, T.; Fushimi, K.; et al. Characteristics of Immune Response to Tumor-Associated Antigens and Immune Cell Profile in Patients With Hepatocellular Carcinoma. Hepatology 2019, 69, 653–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, Y.H.; Li, Y.Y.; Qiao, H.; Wang, H.C.; Yang, X.A.; Zhang, H.G.; Pang, X.W.; Zhang, Y.; Chen, W.F. TSPY is a cancer testis antigen expressed in human hepatocellular carcinoma. Br. J. Cancer 2005, 93, 458–463. [Google Scholar] [CrossRef] [Green Version]
- Korangy, F.; Ormandy, L.A.; Bleck, J.S.; Klempnauer, J.; Wilkens, L.; Manns, M.P.; Greten, T.F. Spontaneous tumor-specific humoral and cellular immune responses to NY-ESO-1 in hepatocellular carcinoma. Clin. Cancer Res. 2004, 10, 4332–4341. [Google Scholar] [CrossRef] [Green Version]
- Djureinovic, D.; Dodig-Crnkovic, T.; Hellstrom, C.; Holgersson, G.; Bergqvist, M.; Mattsson, J.S.M.; Ponten, F.; Stahle, E.; Schwenk, J.M.; Micke, P. Detection of autoantibodies against cancer-testis antigens in non-small cell lung cancer. Lung Cancer 2018, 125, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Deng, Q.; Li, K.Y.; Chen, H.; Dai, J.H.; Zhai, Y.Y.; Wang, Q.; Li, N.; Wang, Y.P.; Han, Z.G. RNA interference against cancer/testis genes identifies dual specificity phosphatase 21 as a potential therapeutic target in human hepatocellular carcinoma. Hepatology 2014, 59, 518–530. [Google Scholar] [CrossRef] [PubMed]
- Maxfield, K.E.; Taus, P.J.; Corcoran, K.; Wooten, J.; Macion, J.; Zhou, Y.; Borromeo, M.; Kollipara, R.K.; Yan, J.; Xie, Y.; et al. Comprehensive functional characterization of cancer-testis antigens defines obligate participation in multiple hallmarks of cancer. Nat. Commun. 2015, 6, 8840. [Google Scholar] [CrossRef] [Green Version]
- Tu, W.; Yang, B.; Leng, X.; Pei, X.; Xu, J.; Liu, M.; Dong, Q.; Tao, D.; Lu, Y.; Liu, Y.; et al. Testis-specific protein, Y-linked 1 activates PI3K/AKT and RAS signaling pathways through suppressing IGFBP3 expression during tumor progression. Cancer Sci. 2019, 110, 1573–1586. [Google Scholar] [CrossRef] [Green Version]
- Velazquez, E.F.; Jungbluth, A.A.; Yancovitz, M.; Gnjatic, S.; Adams, S.; O’Neill, D.; Zavilevich, K.; Albukh, T.; Christos, P.; Mazumdar, M.; et al. Expression of the cancer/testis antigen NY-ESO-1 in primary and metastatic malignant melanoma (MM)--correlation with prognostic factors. Cancer Immun. 2007, 7, 11. [Google Scholar]
- Barrow, C.; Browning, J.; MacGregor, D.; Davis, I.D.; Sturrock, S.; Jungbluth, A.A.; Cebon, J. Tumor antigen expression in melanoma varies according to antigen and stage. Clin. Cancer Res. 2006, 12, 764–771. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CTA | mRNA-Positive HCC (%) 1 | Mean in mRNA-+ HCC (Range) 2 | Relative Expression HCC (Compared to Testis) 3 | mRNA-Positive TFL (%) 4 | Mean in mRNA-+ TFL (Range) 5 | Relative Expression TFL(Compared to Testis) 6 | mRNA-Positive Cirrhotic Tissue 7 |
|---|---|---|---|---|---|---|---|
| CAGE1 | 14.4 | 0.082 (0.003–0.711) | 0.188 | 2.0 | 0.009 (0.003–0.015) | 0.020 | 0 |
| CT47A1 | 26.8 | 1.311 (0.001–20.565) | 0.632 | 6.1 | 0.255 (0.01–0.769) | 0.123 | 0 |
| MAGEA1 | 58.6 | 0.403 (0.003–1.926) | 4.170 | 13.0 | 0.055 (0.005–0.188) | 0.567 | 0 |
| MAGEA9 | 14.1 | 0.41 (0.001–4.953) | 2.848 | 1.0 | 0.035 (0.035–0.035) | 0.243 | 0 |
| MAGEA10 | 12.4 | 0.123 (0.002–0.518) | 1.080 | 4.1 | 0.028 (0.004–0.088) | 0.249 | 0 |
| MAGEB2 | 24.2 | 0.395 (0.002–2.4) | 0.761 | 6.0 | 0.053 (0.018–0.127) | 0.102 | 0 |
| MAGEC1 | 47.5 | 0.109 (0.001–0.841) | 0.407 | 32.0 | 0.047 (0.002–0.466) | 0.174 | 28.6 |
| MAGEC2 | 55.6 | 0.692 (0.001–9.305) | 1.542 | 19.0 | 0.041 (0.003–0.28) | 0.091 | 25.7 |
| NYESO1 | 10.1 | 0.13 (0.007–1.04) | 0.525 | 1.0 | 0.018 (0.018–0.018) | 0.071 | 0 |
| PAGE1 | 18.2 | 0.37 (0.002–2.225) | 1.001 | 5.0 | 0.059 (0.009–0.179) | 0.159 | 2.9 |
| SLCO6A1 | 25.8 | 0.095 (0.002–0.411) | 0.053 | 4.1 | 0.011 (0.004–0.017) | 0.006 | 2.9 |
| TSPY * | 21.0 | 0.827 (0.004–7.401) | 34.135 | 4.8 | 0.218 (0.001–0.641) | 9.012 | 4.2 |
| Discovery Cohort | ||||||||
|---|---|---|---|---|---|---|---|---|
| Early Recurrence (<2 yr) | HCC-Specific Survival | |||||||
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||
| Variable | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value |
| ≥1 CTA in TFL | 2.3 (1.3–4.0) | 0.0034 | 2.5 (1.47–4.5) | 0.003 | 2.4 (1.1–5.4) | 0.03 | 2.3 (1.0–5.3) | 0.044 |
| ≥2 CTAs in TFL | 2.1 (1.2–3.7) | 0.013 | 1.7 (0.7–3.9) | 0.22 | ||||
| ≥3 CTAs in TFL | 4.2 (1.9–9.4) | 0.00053 | 5.1 (1.9–14) | 0.0015 | ||||
| Number of CTAs in TFL (numeric) | 1.3 (1.2–1.5) | 2.0 × 10−5 | 1.3 (1.1–1.5) | 0.0011 | ||||
| >1 tumor | 1.2 (0.7–2.0) | 0.56 | 1.1 (0.5–2.4) | 0.83 | ||||
| >2 tumors | 2.6 (1.3–4.9) | 0.0042 | 2.4 (1.2–4.7) | 0.02 | 1.8 (0.7–4.9) | 0.22 | ||
| Cirrhosis | 1.6 (0.9–2.8) | 0.12 | 1.5 (0.7–3.4) | 0.33 | ||||
| Chronic viral hepatitis | 2.3 (1.3–4.0) | 0.0031 | 2.7 (1.5–5.0) | 0.001 | 3.3 (1.5–7.2) | 0.0032 | 4.63 (2.0–10.8) | 0.0004 |
| Vascular invasion | 1.3 (0.7–2.3) | 0.41 | 2.2 (0.96–4.9) | 0.063 | ||||
| Tumor > 5 cm | 1.3 (0.7–2.3) | 0.37 | 2.3 (0.9–5.7) | 0.081 | ||||
| AFP > 200 ug/L | 1.9 (1.0–3.4) | 0.034 | 2.7 (1.2–6) | 0.013 | ||||
| AFP > 400 ug/L | 2.4 (1.3–4.5) | 0.0051 | 3.0 (1.5–5.8) | 0.001 | 3.3 (1.5–7.3) | 0.0038 | 4.0 (1.7–9.4) | 0.002 |
| Validation Cohort | ||||||||
| Early Recurrence (<2 yr) | HCC-Specific Survival | |||||||
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||
| Variable | HR (95% CI) | p-value | HR (95% CI) | p-value | HR (95% CI) | p-value | HR (95% CI) | p-value |
| ≥1 CTA in TFL | 2.2 (1.1–4.2) | 0.022 | 2.1 (1.1–4.1) | 0.03 | 3.3 (1.4–7.7) | 0.0074 | 3.6 (1.5–8.8) | 0.004 |
| ≥2 CTAs in TFL | 1.5 (0.58–3.8) | 0.41 | 2.3 (0.83–6.3) | 0.11 | ||||
| ≥3 CTAs in TFL | 1.1 × 10−7 (0-Inf) | 1 | 3.9 × 10−8 (0-Inf) | 1 | ||||
| Number of CTAs in TFL (numeric) | 1.2 (0.89–1.7) | 0.21 | 1.4 (0.95–2) | 0.095 | ||||
| >1 tumor | 2.1 (1–4.2) | 0.043 | 2.2 (1.1–4.5) | 0.03 | 0.9 (0.27–3.1) | 0.87 | ||
| >2 tumors | 1.7 (0.67–4.4) | 0.26 | 0.96 (0.22–4.1) | 0.96 | ||||
| Cirrhosis | 0.77 (0.39–1.5) | 0.45 | 2.3 (0.97–5.5) | 0.059 | 2.6 (1.1–6.3) | 0.03 | ||
| Chronic viral hepatitis | 0.91 (0.42–2) | 0.82 | 0.98 (0.36–2.7) | 0.97 | ||||
| Vascular invasion | 2.1 (0.98–4.4) | 0.055 | 1.5 (0.59–3.9) | 0.38 | ||||
| Tumor > 5 cm | 2.5 (1.2–5) | 0.011 | 2.6 (1.3–5.3) | 0.007 | 1.5 (0.61–3.6) | 0.38 | ||
| AFP > 200 ug/L | 1.6 (0.8–3.3) | 0.18 | 0.83 (0.28–2.5) | 0.74 | ||||
| AFP > 400 ug/L | 1.3 (0.61–2.9) | 0.46 | 0.65 (0.19–2.2) | 0.5 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noordam, L.; Ge, Z.; Özturk, H.; Doukas, M.; Mancham, S.; Boor, P.P.C.; Campos Carrascosa, L.; Zhou, G.; van den Bosch, T.P.P.; Pan, Q.; et al. Expression of Cancer Testis Antigens in Tumor-Adjacent Normal Liver Is Associated with Post-Resection Recurrence of Hepatocellular Carcinoma. Cancers 2021, 13, 2499. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13102499
Noordam L, Ge Z, Özturk H, Doukas M, Mancham S, Boor PPC, Campos Carrascosa L, Zhou G, van den Bosch TPP, Pan Q, et al. Expression of Cancer Testis Antigens in Tumor-Adjacent Normal Liver Is Associated with Post-Resection Recurrence of Hepatocellular Carcinoma. Cancers. 2021; 13(10):2499. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13102499
Chicago/Turabian StyleNoordam, Lisanne, Zhouhong Ge, Hadiye Özturk, Michail Doukas, Shanta Mancham, Patrick P. C. Boor, Lucia Campos Carrascosa, Guoying Zhou, Thierry P. P. van den Bosch, Qiuwei Pan, and et al. 2021. "Expression of Cancer Testis Antigens in Tumor-Adjacent Normal Liver Is Associated with Post-Resection Recurrence of Hepatocellular Carcinoma" Cancers 13, no. 10: 2499. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13102499