
Rapid Response to the Combination of Lenvatinib and Pembrolizumab in Patients with Advanced Carcinomas (Lung Adenocarcinoma and Malignant Pleural Mesothelioma)

 ,
,  , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Isolation and Culturing of the Patients’ Peripheral CD8+ T Cells
2.3. Patient-Derived Xenograft (PDX) Generation and Propagation
2.4. Co-Culture of A549 CD8+ T Cells
2.5. Immuno-Tumor Ex Vivo Analysis (i-TEVA)
2.6. Tumor Tissue Explants Culture, Preparation of Formalin-Fixed Paraffin-Embedded (FFPE) Blocks, and Tissue Microarray
2.7. Immunohistochemistry Staining and Quantification
3. Results
3.1. Case Series
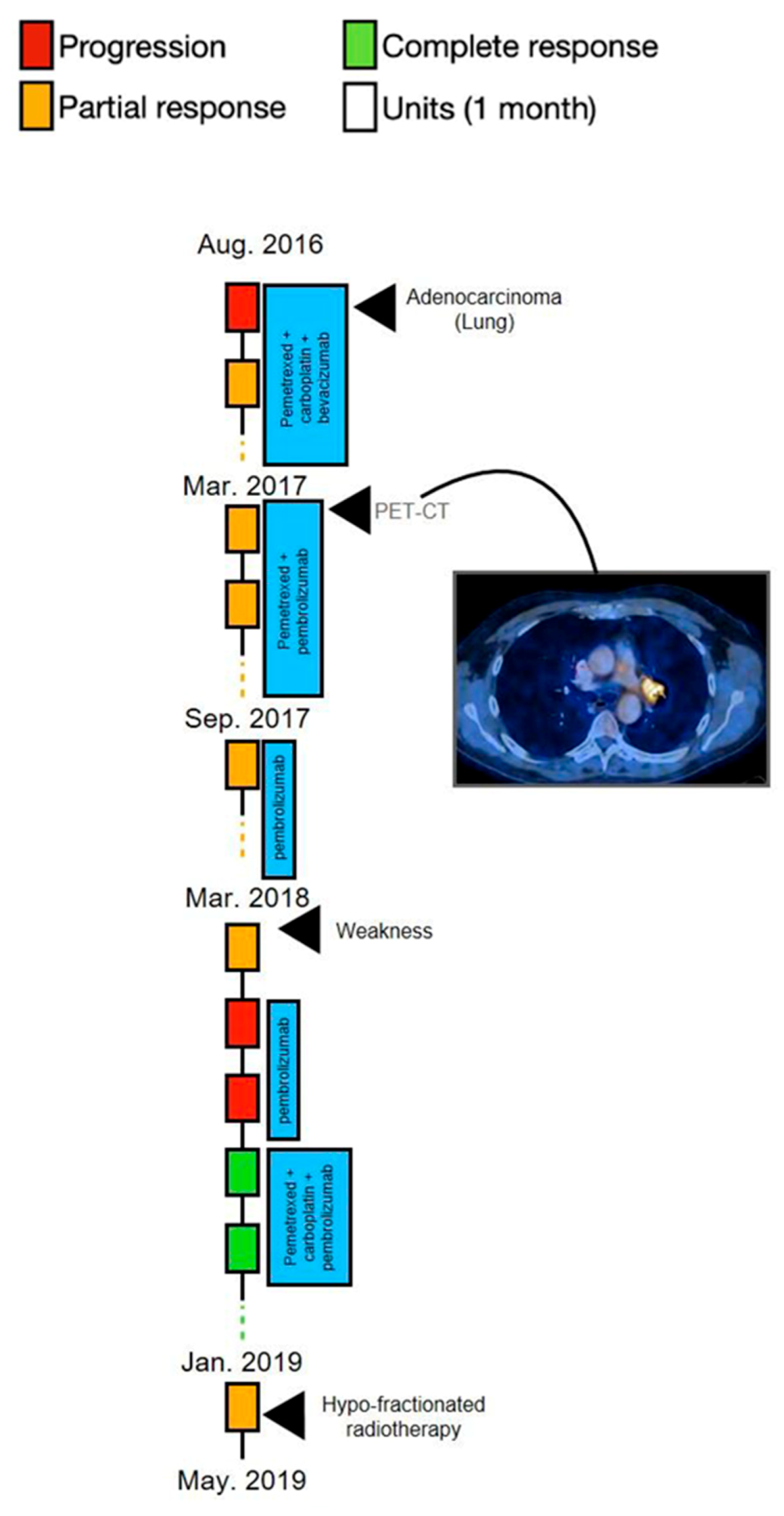
3.1.1. Case 1—Excellent Response Combined with Disappearance of the Lower Left Lung after Treatment with Lenvatinib and Pembrolizumab
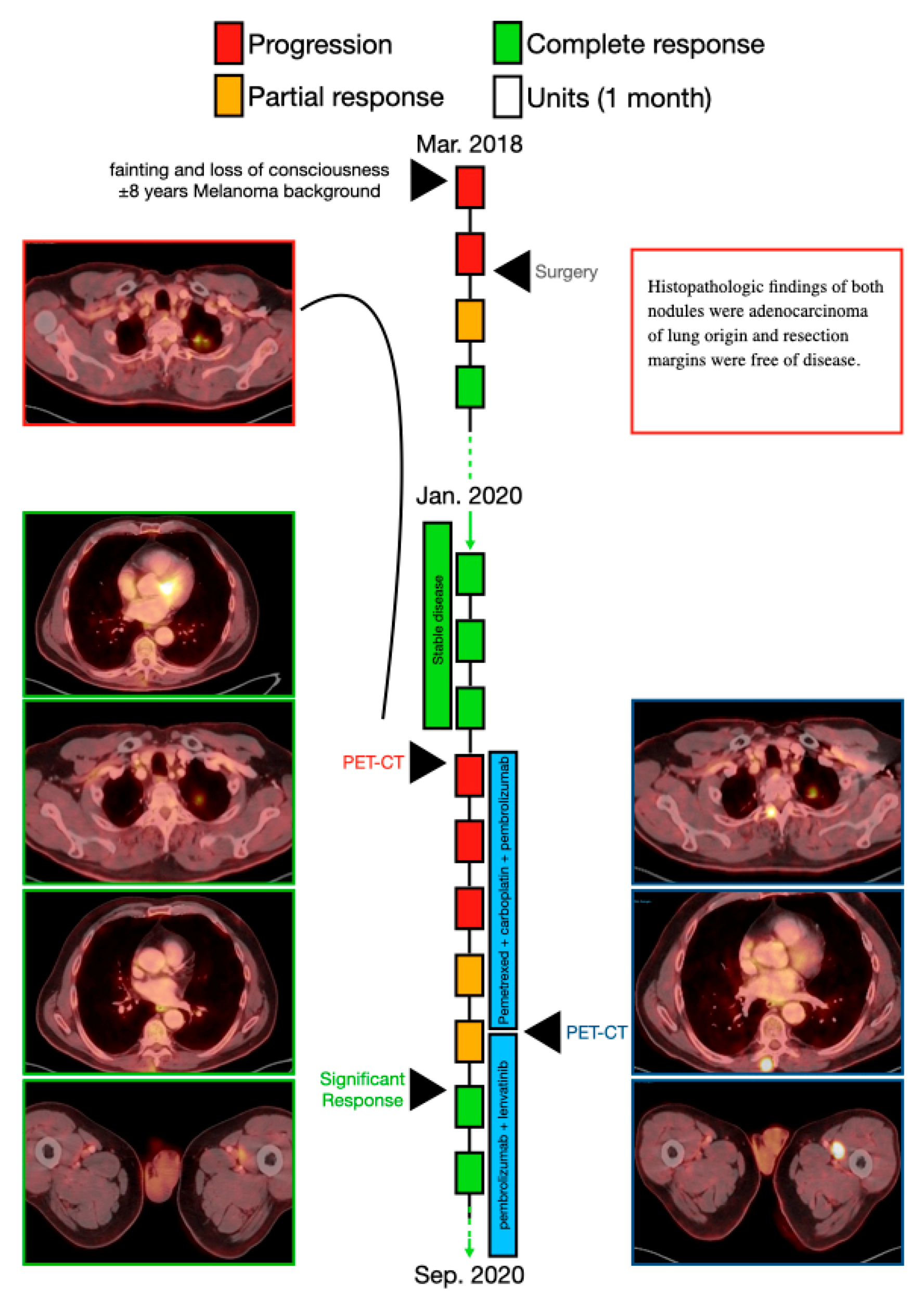
3.1.2. Case 2—A Multiple Radiological Response Followed by Less Metabolic Uptake Immediately after Combination of Lenvatinib and Pembrolizumab
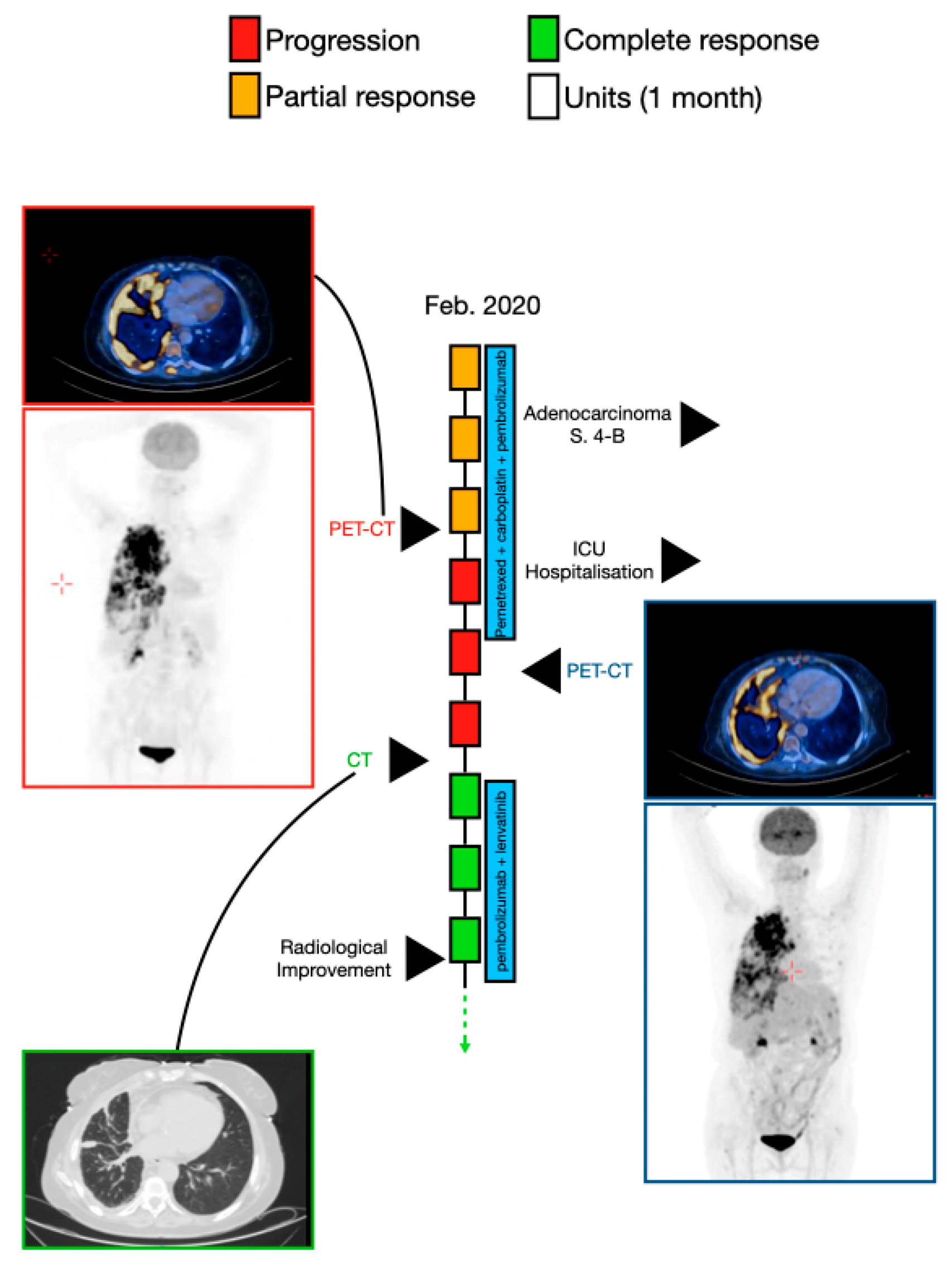
3.1.3. Case 3—Radiological Improvement Achieved after Treatment with Pembrolizumab and Lenvatinib in a Patient after Hospitalization in an Intensive Care Unit
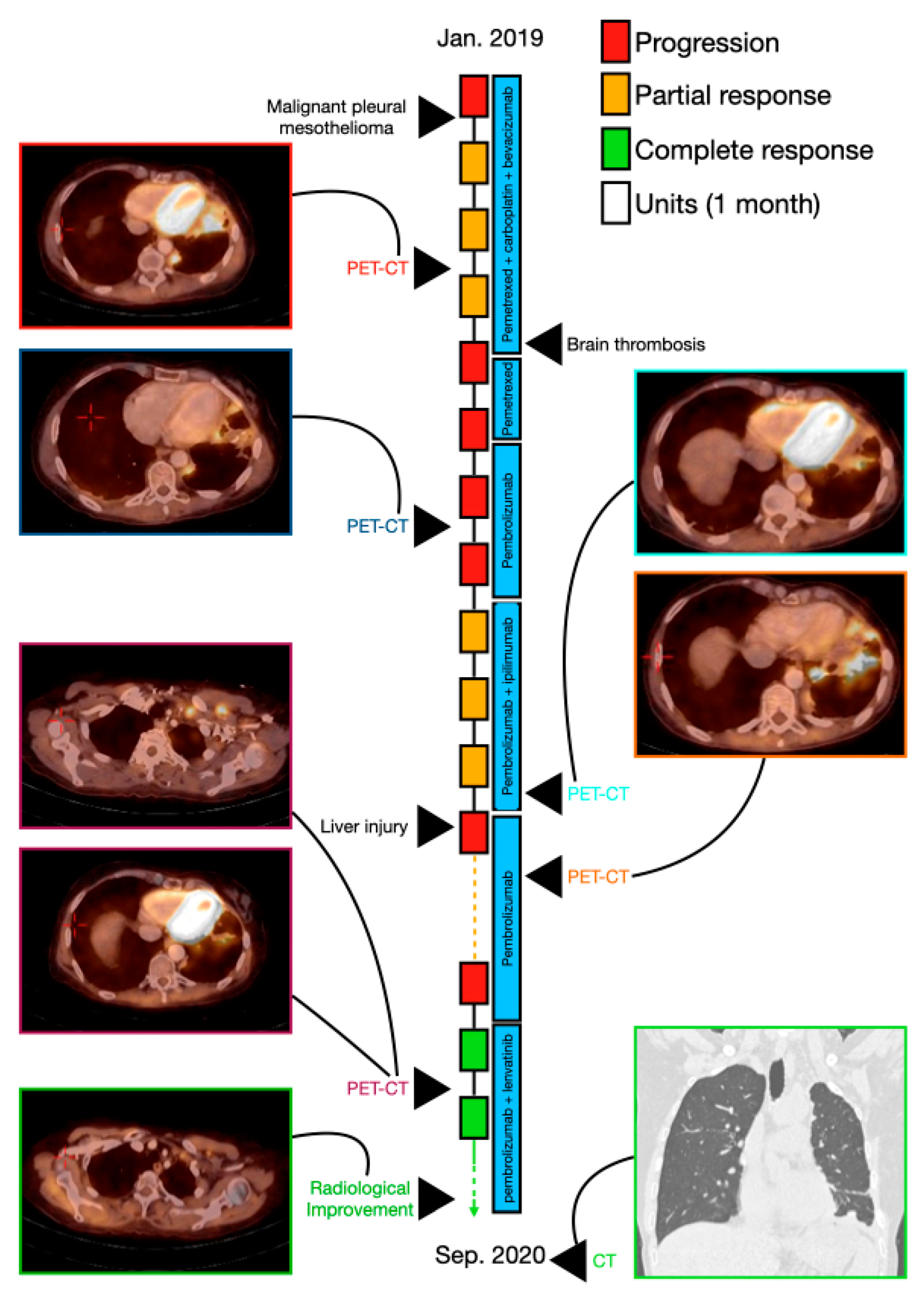
3.1.4. Case 4—A Significant Response to Pembrolizumab, Lenvatinib, and Gemcitabine in a Patient with Malignant Pleural Mesothelioma
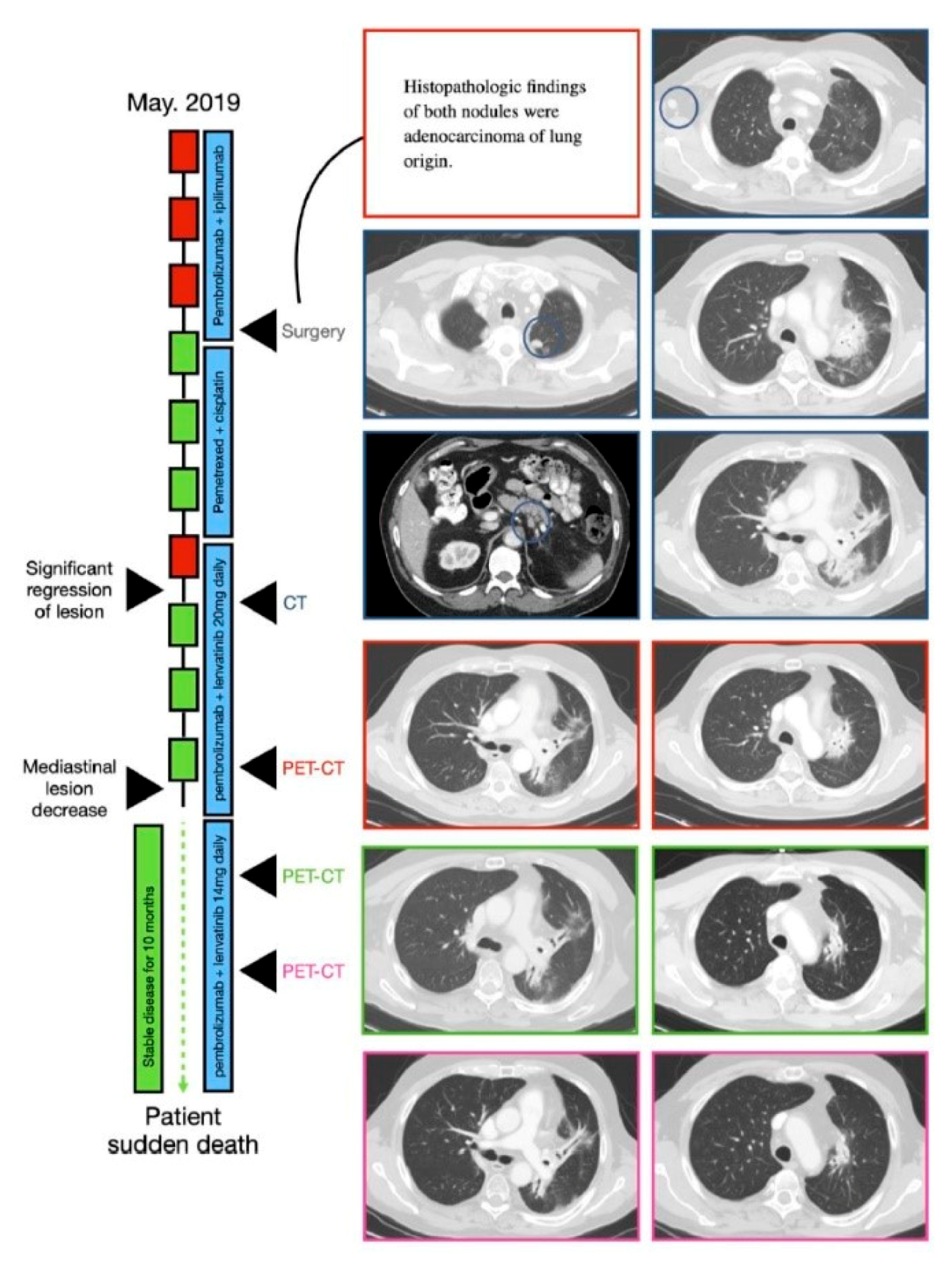
3.1.5. Case 5—Combined Treatment Stabilized the Patient’s Widespread Disease for a Period of 10 months
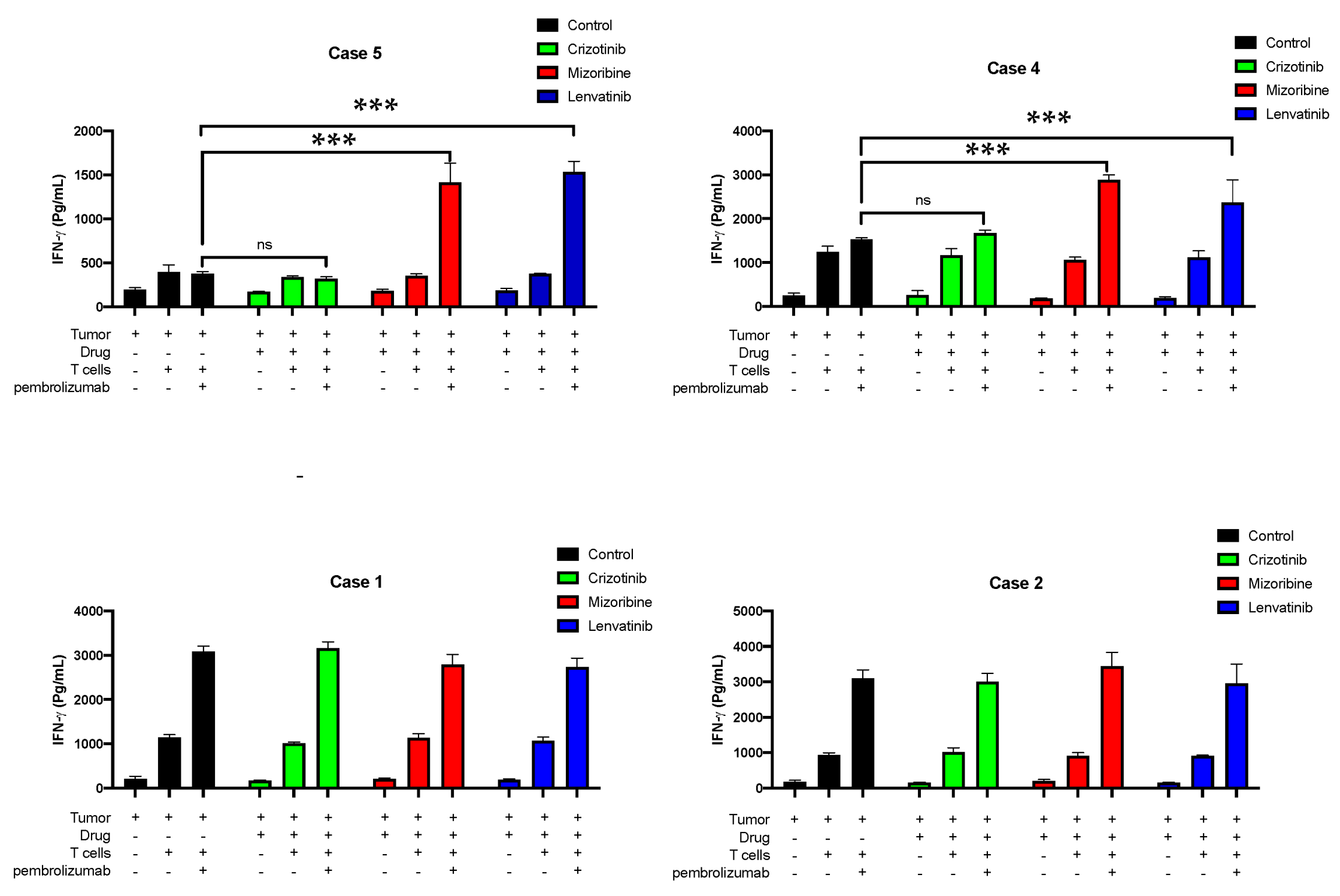
3.2. Testing CD8+ T Cell Responses of Four Patients to Lenvatinib In Vitro
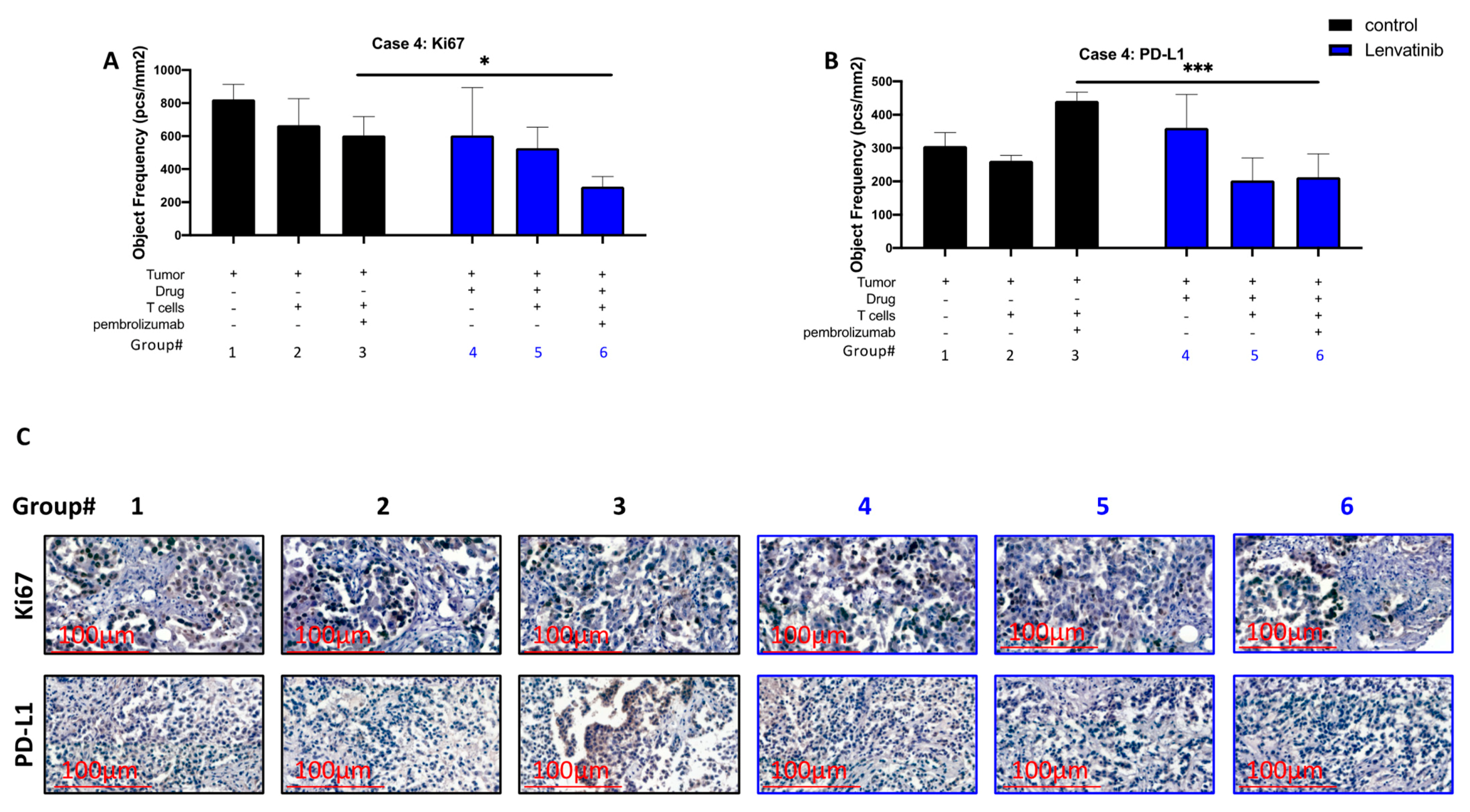
3.3. Pre-Treatment of Cancer Ex Vivo with Lenvatinib Contribute to Reduction of PD-L1 Expression and to Reduced Proliferation Levels While Using T Cells and Pembrolizumab
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Miller, K.D.; Nogueira, L.; Mariotto, A.B.; Rowland, J.H.; Yabroff, K.R.; Alfano, C.M.; Jemal, A.; Kramer, J.L.; Siegel, R.L. Cancer Treatment and Survivorship Statistics, 2019. CA Cancer J. Clin. 2019, 69, 363–385. [Google Scholar] [CrossRef] [Green Version]
- Fischer, B.M.; Mortensen, J.; Hansen, H.; Vilmann, P.; Larsen, S.S.; Loft, A.; Bertelsen, A.K.; Ravn, J.; Clementsen, P.; Høegholm, A. Multimodality Approach to Mediastinal Staging in Non-Small Cell Lung Cancer. Faults and Benefits of PET-CT: A Randomised Trial. Thorax 2011, 66, 294–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuchs, M.M.; Attenhofer Jost, C.; Babovic-Vuksanovic, D.; Connolly, H.M.; Egbe, A. Long-term Outcomes in Patients with Turner Syndrome: A 68-year Follow-up. J. Am. Heart Assoc. 2019, 8, e011501. [Google Scholar] [CrossRef] [Green Version]
- Vogelzang, N.J.; Rusthoven, J.J.; Symanowski, J.; Denham, C.; Kaukel, E.; Ruffie, P.; Gatzemeier, U.; Boyer, M.; Emri, S.; Manegold, C. Phase III Study of Pemetrexed in Combination with Cisplatin versus Cisplatin Alone in Patients with Malignant Pleural Mesothelioma. J. Clin. Oncol. 2003, 21, 2636–2644. [Google Scholar] [CrossRef]
- Hysi, I.; Pimpec-Barthes, L.; Alifano, M.; Venissac, N.; Mouroux, J.; Regnard, J.-F.; Riquet, M.; Porte, H. Lymph Node Involvement and Metastatic Lymph Node Ratio Influence the Survival of Malignant Pleural Mesothelioma: A French Multicenter Retrospective Study. Oncol. Rep. 2014, 31, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Pardoll, D.M. The Blockade of Immune Checkpoints in Cancer Immunotherapy. Nat. Rev. Cancer 2012, 12, 252–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tohyama, O.; Matsui, J.; Kodama, K.; Hata-Sugi, N.; Kimura, T.; Okamoto, K.; Minoshima, Y.; Iwata, M.; Funahashi, Y. Antitumor Activity of Lenvatinib (E7080): An Angiogenesis Inhibitor That Targets Multiple Receptor Tyrosine Kinases in Preclinical Human Thyroid Cancer Models. J. Thyroid Res. 2014, 2014, 638747. [Google Scholar] [CrossRef]
- Taylor, M.H.; Lee, C.-H.; Makker, V.; Rasco, D.; Dutcus, C.E.; Wu, J.; Stepan, D.E.; Shumaker, R.C.; Motzer, R.J. Phase IB/II Trial of Lenvatinib plus Pembrolizumab in Patients with Advanced Renal Cell Carcinoma, Endometrial Cancer, and Other Selected Advanced Solid Tumors. J. Clin. Oncol. 2020, 38, 1154. [Google Scholar] [CrossRef]
- Capozzi, M.; de Divitiis, C.; Ottaiano, A.; von Arx, C.; Scala, S.; Tatangelo, F.; Delrio, P.; Tafuto, S. Lenvatinib, a Molecule with Versatile Application: From Preclinical Evidence to Future Development in Anti-Cancer Treatment. Cancer Manag. Res. 2019, 11, 3847. [Google Scholar] [CrossRef] [Green Version]
- Keshet, R.; Lee, J.S.; Adler, L.; Iraqi, M.; Ariav, Y.; Lim, L.Q.J.; Lerner, S.; Rabinovich, S.; Oren, R.; Katzir, R. Targeting Purine Synthesis in ASS1-Expressing Tumors Enhances the Response to Immune Checkpoint Inhibitors. Nat. Cancer 2020, 1, 894–908. [Google Scholar] [CrossRef]
- Ghosh, S.; Prasad, M.; Kundu, K.; Cohen, L.; Yegodayev, K.M.; Zorea, J.; Joshua, B.-Z.; Lasry, B.; Dimitstein, O.; Bahat-Dinur, A. Tumor Tissue Explant Culture of Patient-Derived Xenograft as Potential Prioritization Tool for Targeted Therapy. Front. Oncol. 2019, 9, 17. [Google Scholar] [CrossRef] [Green Version]
- Ottolenghi, A.; Bolel, P.; Sarkar, R.; Greenshpan, Y.; Iraqi, M.; Ghosh, S.; Bhattacharya, B.; Taylor, Z.V.; Kundu, K.; Radinsky, O. Life-Extended Glycosylated IL-2 Promotes Treg Induction and Suppression of Autoimmunity. Sci. Rep. 2021, 11, 1–15. [Google Scholar] [CrossRef]
- Kundu, K.; Ghosh, S.; Sarkar, R.; Edri, A.; Brusilovsky, M.; Gershoni-Yahalom, O.; Yossef, R.; Shemesh, A.; Soria, J.-C.; Lazar, V. Inhibition of the NKp44-PCNA Immune Checkpoint Using a MAb to PCNA. Cancer Immunol. Res. 2019, 7, 1120–1134. [Google Scholar] [CrossRef]
- Carretero-González, A.; Lora, D.; Ghanem, I.; Zugazagoitia, J.; Castellano, D.; Sepúlveda, J.M.; López-Martin, J.A.; Paz-Ares, L.; de Velasco, G. Analysis of Response Rate with ANTI PD1/PD-L1 Monoclonal Antibodies in Advanced Solid Tumors: A Meta-Analysis of Randomized Clinical Trials. Oncotarget 2018, 9, 8706. [Google Scholar] [CrossRef] [Green Version]
- Grosso, J.; Horak, C.E.; Inzunza, D.; Cardona, D.M.; Simon, J.S.; Gupta, A.K.; Sankar, V.; Park, J.-S.; Kollia, G.; Taube, J.M. Association of Tumor PD-L1 Expression and Immune Biomarkers with Clinical Activity in Patients (Pts) with Advanced Solid Tumors Treated with Nivolumab (Anti-PD-1; BMS-936558; ONO-4538). J. Clin. Oncol. 2013, 31, 3016. [Google Scholar] [CrossRef]
- Wu, P.; Wu, D.; Li, L.; Chai, Y.; Huang, J. PD-L1 and Survival in Solid Tumors: A Meta-Analysis. PLoS ONE 2015, 10, e0131403. [Google Scholar] [CrossRef] [PubMed]
- Gentzler, R.; Hall, R.; Kunk, P.R.; Gaughan, E.; Dillon, P.; Slingluff, C.L., Jr.; Rahma, O.E. Beyond Melanoma: Inhibiting the PD-1/PD-L1 Pathway in Solid Tumors. Immunotherapy 2016, 8, 583–600. [Google Scholar] [CrossRef] [PubMed]
- Xiang, X.; Yu, P.-C.; di Long, X.-L.L.; Zhang, S.; You, X.-M.; Zhong, J.-H.; Li, L.-Q. Prognostic Value of PD–L1 Expression in Patients with Primary Solid Tumors. Oncotarget 2018, 9, 5058. [Google Scholar] [CrossRef] [Green Version]
- Kulangara, K.; Hanks, D.A.; Waldroup, S.; Peltz, L.; Shah, S.; Roach, C.; Juco, J.W.; Emancipator, K.; Stanforth, D. Development of the Combined Positive Score (CPS) for the Evaluation of PD-L1 in Solid Tumors with the Immunohistochemistry Assay PD-L1 IHC 22C3 PharmDx. J. Clin. Oncol. 2017, 35. [Google Scholar] [CrossRef]
- Cha, E.; Wallin, J.; Kowanetz, M. PD-L1 Inhibition with MPDL3280A for Solid Tumors. In Proceedings of the Seminars in Oncology; Elsevier: Amsterdam, The Netherlands, 2015; Volume 42, pp. 484–487. [Google Scholar]
- Mazza, V.; Cappuzzo, F. Treating EGFR Mutation Resistance in Non-Small Cell Lung Cancer–Role of Osimertinib. Appl. Clin. Genet. 2017, 10, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, S.; Boggon, T.J.; Dayaram, T.; Jänne, P.A.; Kocher, O.; Meyerson, M.; Johnson, B.E.; Eck, M.J.; Tenen, D.G.; Halmos, B. EGFR Mutation and Resistance of Non–Small-Cell Lung Cancer to Gefitinib. N. Engl. J. Med. 2005, 352, 786–792. [Google Scholar] [CrossRef]
- Merenbakh-Lamin, K.; Ben-Baruch, N.; Yeheskel, A.; Dvir, A.; Soussan-Gutman, L.; Jeselsohn, R.; Yelensky, R.; Brown, M.; Miller, V.A.; Sarid, D. D538G Mutation in Estrogen Receptor-α: A Novel Mechanism for Acquired Endocrine Resistance in Breast Cancer. Cancer Res. 2013, 73, 6856–6864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahcall, M.; Sim, T.; Paweletz, C.P.; Patel, J.D.; Alden, R.S.; Kuang, Y.; Sacher, A.G.; Kim, N.D.; Lydon, C.A.; Awad, M.M. Acquired METD1228V Mutation and Resistance to MET Inhibition in Lung Cancer. Cancer Discov. 2016, 6, 1334–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, E.S. Treatment Options after First-Line Immunotherapy in Metastatic NSCLC. Expert Rev. Anticancer Ther. 2020, 20, 221–228. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case No. | Gender | Age | Smoking History | Histopathologic Diagnosis | Stage at Diagnosis | Genetic Alterations | Treatment before LEN+PEM | LEN + PEM Outcome | ||
|---|---|---|---|---|---|---|---|---|---|---|
| chemotherapy | immunotherapy | VEGF-A | ||||||||
| 1 | M | 68 | 30 PY | adenocarcinoma of lung | 4-C | MDM2, KRAS amplification, RB1 amplification, STK11 | 13 mo. | 12 mo. (combined with chemo | CR after 2 mo + | |
| 2 | M | 68 | 60 PY | adenocarcinoma of lung | 1-B | 4 mo. | 4 mo. (combined with chemo) | Significant response after 2 mo + | ||
| 3 | F | 64 | 40 PY | adenocarcinoma of lung | 4-B | 4 mo. | 4 mo (combined with chemo) | CR after 3 mo + | ||
| 4 | F | 50 | 10 PY | malignant pleural mesothelioma | 3-B | 6 mo. | 9 mo | 4 mo. (combined with chemo) | Significant response after 2 mo. + | |
| 5 | M | 61 | 35 PY | adenocarcinoma of lung | 4-C | KRAS, STK11, PDL1 < 24% | 19 mo. | 14 mo. (combined with chemo) + 11 mo. (without chemo) | 5 mo. (combined with chemo) | Stabilized disease with no adverse events for 10 mo., until patient’s sudden death. |
| Case No. | Diarrhea | Fatigue | Hypothyroidism | Hypertension | Weight Loss |
|---|---|---|---|---|---|
| 1 | 2 | 1 | 1 | 0 | 0 |
| 2 | 2 | 1 | 0 | 1 | 1 |
| 3 | 0 | 2 | 0 | 1 | 1 |
| 4 | 0 | 1 | 0 | 0 | 1 |
| 5 | 0 | 1 | 1 | 1 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shalata, W.; Iraqi, M.; Bhattacharya, B.; Fuchs, V.; Roisman, L.C.; Cohen, A.Y.; Massalha, I.; Yakobson, A.; Prasad, M.; Elkabets, M.; et al. Rapid Response to the Combination of Lenvatinib and Pembrolizumab in Patients with Advanced Carcinomas (Lung Adenocarcinoma and Malignant Pleural Mesothelioma). Cancers 2021, 13, 3630. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13143630
Shalata W, Iraqi M, Bhattacharya B, Fuchs V, Roisman LC, Cohen AY, Massalha I, Yakobson A, Prasad M, Elkabets M, et al. Rapid Response to the Combination of Lenvatinib and Pembrolizumab in Patients with Advanced Carcinomas (Lung Adenocarcinoma and Malignant Pleural Mesothelioma). Cancers. 2021; 13(14):3630. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13143630
Chicago/Turabian StyleShalata, Walid, Muhammed Iraqi, Baisali Bhattacharya, Vered Fuchs, Laila C. Roisman, Ahron Yehonatan Cohen, Ismaell Massalha, Alexander Yakobson, Manu Prasad, Moshe Elkabets, and et al. 2021. "Rapid Response to the Combination of Lenvatinib and Pembrolizumab in Patients with Advanced Carcinomas (Lung Adenocarcinoma and Malignant Pleural Mesothelioma)" Cancers 13, no. 14: 3630. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13143630