
Targeted Next-Generation Sequencing Analysis Predicts the Recurrence in Resected Lung Adenocarcinoma Harboring EGFR Mutations

 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. The Patients and Specimen Collection
2.2. NGS Processing
2.3. NGS Data Analysis
2.4. Patient Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
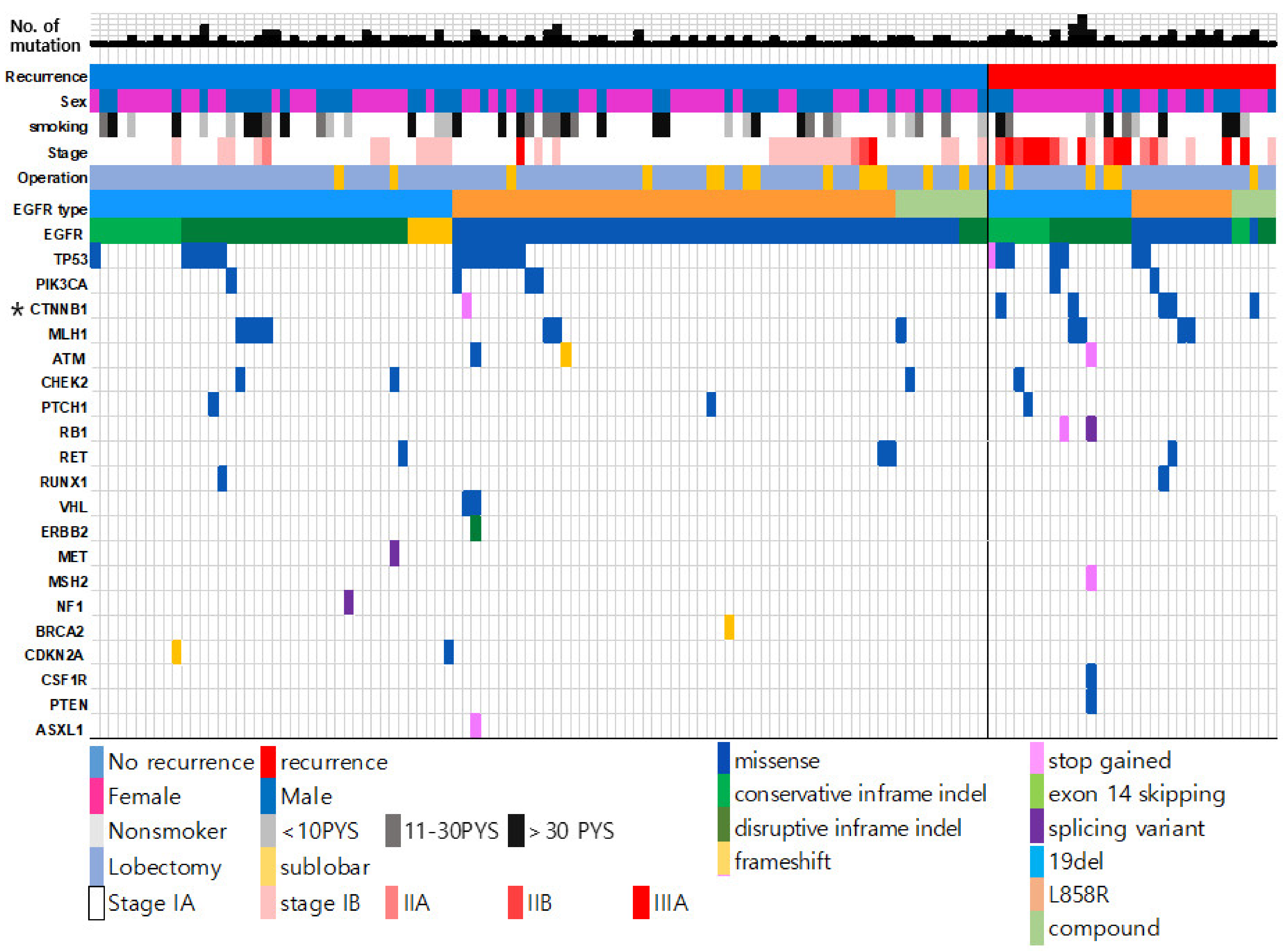
3.2. Genetic Landscape of Resected EGFR-Mutated Adenocarcinoma According to Recurrence Status
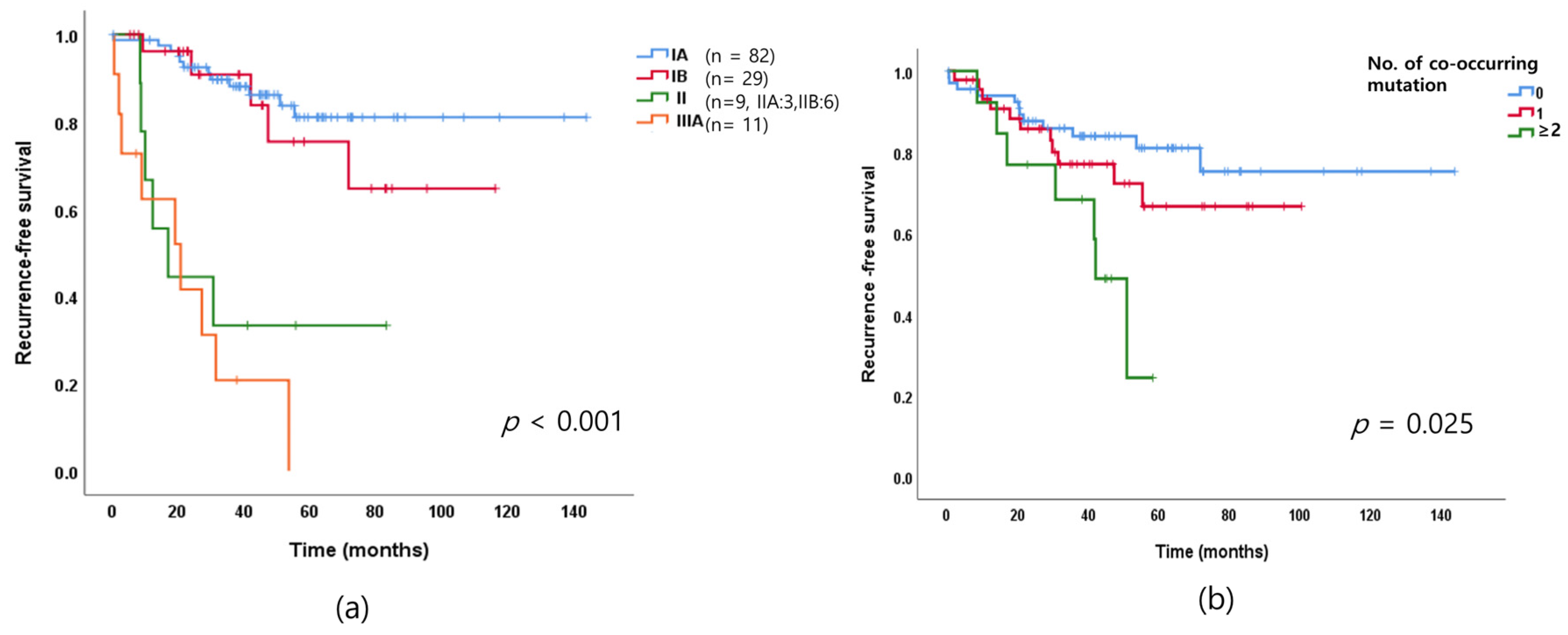
3.3. Cancer Stage Distribution of Resected EGFR-Mutated Lung Adenocarcinoma and Recurrence
3.4. Association between the Number of Genetic Alterations and Recurrence
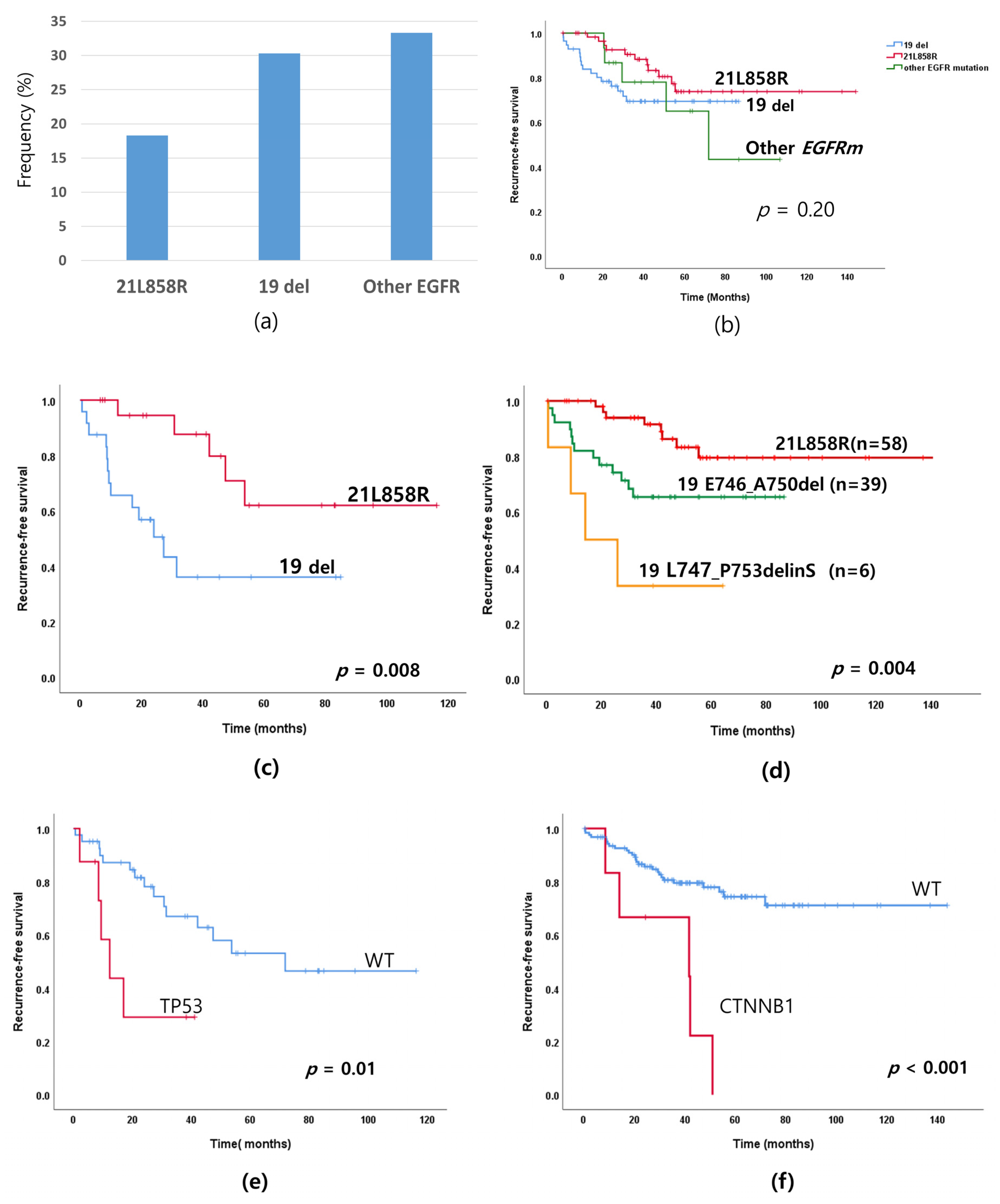
3.5. Recurrence Rate According to EGFR Mutation Subtypes and Co-Mutations
3.6. Prognostic Factors for Recurrence Based on Multivariate Analysis of Resected EGFR-Mutated Lung Adenocarcinomas
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Takamochi, K.; Oh, S.; Matsunaga, T.; Suzuki, K. Prognostic impacts of EGFR mutation status and subtype in patients with surgically resected lung adenocarcinoma. J. Thorac. Cardiovasc. Surg. 2017, 154, 1768–1774.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Angelo, S.P.; Janjigian, Y.Y.; Ahye, N.; Riely, G.J.; Chaft, J.E.; Sima, C.S.; Shen, R.; Zheng, J.; Dycoco, J.; Kris, M.G.; et al. Distinct Clinical Course of EGFR-Mutant Resected Lung Cancers: Results of Testing of 1118 Surgical Specimens and Effects of Adjuvant Gefitinib and Erlotinib. J. Thorac. Oncol. 2012, 7, 1815–1822. [Google Scholar] [CrossRef] [Green Version]
- Nishii, T.; Yokose, T.; Miyagi, Y.; Daigo, Y.; Isaka, T.; Furumoto, H.; Ito, H.; Murakami, S.; Kondo, T.; Saito, H.; et al. Prognostic value of EGFR mutations in surgically resected pathological stage I lung ade-nocarcinoma. Asia-Pac. J. Clin. Oncol. 2017, 13, e204–e211. [Google Scholar] [CrossRef]
- Zhong, W.-Z.; Wang, Q.; Mao, W.-M.; Xu, S.-T.; Wu, L.; Shen, Y.; Liu, Y.-Y.; Chen, C.; Cheng, Y.; Xu, L.; et al. Gefitinib versus vinorelbine plus cisplatin as adjuvant treatment for stage II–IIIA (N1–N2) EGFR-mutant NSCLC (ADJUVANT/CTONG1104): A randomised, open-label, phase 3 study. Lancet Oncol. 2018, 19, 139–148. [Google Scholar] [CrossRef]
- Goldstraw, P.; Chansky, K.; Crowley, J.; Rami-Porta, R.; Asamura, H.; Eberhardt, W.E.; Nicholson, A.G.; Groome, P.; Mitchell, A.; Bolejack, V.; et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J. Thorac. Oncol. 2016, 11, 39–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gradishar, W.J.; Anderson, B.O.; Abraham, J.; Aft, R.; Agnese, D.; Allison, K.H.; Blair, S.L.; Burstein, H.J.; Dang, C.; Elias, A.D.; et al. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). J. Natl. Compr. Cancer Netw. 2020, 18, 452–478. [Google Scholar] [CrossRef] [Green Version]
- Takenaka, T.; Takenoyama, M.; Yamaguchi, M.; Toyozawa, R.; Inamasu, E.; Kojo, M.; Toyokawa, G.; Yoshida, T.; Shiraishi, Y.; Morodomi, Y.; et al. Impact of the epidermal growth factor receptor mutation status on the post-recurrence survival of patients with surgically resected non-small-cell lung cancer †. Eur. J. Cardio-Thorac. Surg. 2014, 47, 550–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lv, C.; An, C.; Feng, Q.; Ma, Y.; Li, S.; Wang, J.; Zhang, J.; Wang, X.; Yan, S.; Fang, J.; et al. A Retrospective Study of Stage I to IIIa Lung Adenocarcinoma after Resection: What Is the Optimal Adjuvant Modality for Patients with an EGFR Mutation? Clin. Lung Cancer 2015, 16, e173–e181. [Google Scholar] [CrossRef] [Green Version]
- Cheng, H.; Li, X.-J.; Wang, X.-J.; Chen, Z.-W.; Wang, R.-Q.; Zhong, H.-C.; Wu, T.-C.; Cao, Q.-D. A meta-analysis of adjuvant EGFR-TKIs for patients with resected non-small cell lung cancer. Lung Cancer 2019, 137, 7–13. [Google Scholar] [CrossRef]
- Wu, Y.-L.; Tsuboi, M.; He, J.; John, T.; Grohe, C.; Majem, M.; Goldman, J.W.; Laktionov, K.; Kim, S.-W.; Kato, T.; et al. Osimertinib in Resected EGFR-Mutated Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2020, 383, 1711–1723. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.-L.; Zhong, W.; Wang, Q.; Mao, W.; Xu, S.-T.; Wu, L.; Chen, C.; Cheng, Y.; Xu, L.; Wang, J.; et al. CTONG1104: Adjuvant gefitinib versus chemotherapy for resected N1-N2 NSCLC with EGFR mutation—Final overall survival analysis of the randomized phase III trial 1 analysis of the randomized phase III trial. J. Clin. Oncol. 2020, 38, 9005. [Google Scholar] [CrossRef]
- Chen, M.; Xu, Y.; Zhao, J.; Zhong, W.; Zhang, L.; Bi, Y.; Wang, M. Concurrent Driver Gene Mutations as Negative Predictive Factors in Epidermal Growth Factor Receptor-Positive Non-Small Cell Lung Cancer. EBioMedicine 2019, 42, 304–310. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Lee, B.; Shim, J.H.; Lee, S.-H.; Park, W.-Y.; Choi, Y.-L.; Sun, J.-M.; Ahn, J.S.; Ahn, M.-J.; Park, K. Concurrent Genetic Alterations Predict the Progression to Target Therapy in EGFR-Mutated Advanced NSCLC. J. Thorac. Oncol. 2019, 14, 193–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helena, A.Y.; Suzawa, K.; Jordan, E.J.; Zehir, A.; Ni, A.; Kim, H.R.; Kris, M.G.; Hellmann, M.D.; Li, B.T.; Somwar, R.; et al. Concurrent Alterations in EGFR-Mutant Lung Cancers Associated with Resistance to EGFR Kinase Inhibitors and Characterization of MTOR as a Mediator of Resistance. Clin. Cancer Res. 2018, 24, 3108–3118. [Google Scholar] [CrossRef] [Green Version]
- Cho, W.C.; Tan, K.T.; Ma, V.W.; Li, J.Y.; Ngan, R.K.; Cheuk, W.; Yip, T.T.; Yang, Y.-T.; Chen, S.-J. Targeted next-generation sequencing reveals recurrence-associated genomic alterations in early-stage non-small cell lung cancer. Oncotarget 2018, 9, 36344–36357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, S.; Nagahashi, M.; Koike, T.; Ichikawa, H.; Shimada, Y.; Watanabe, S.; Kikuchi, T.; Takada, K.; Nakanishi, R.; Oki, E.; et al. Impact of Concurrent Genomic Alterations Detected by Comprehensive Genomic Sequencing on Clinical Outcomes in East-Asian Patients with EGFR-Mutated Lung Adenocarcinoma. Sci. Rep. 2018, 8, 1005. [Google Scholar] [CrossRef]
- Zhou, J.; Sanchez-Vega, F.; Caso, R.; Tan, K.S.; Brandt, W.S.; Jones, G.; Yan, S.; Adusumilli, P.S.; Bott, M.J.; Huang, J.; et al. Analysis of Tumor Genomic Pathway Alterations Using Broad-Panel Next-Generation Sequencing in Surgically Resected Lung Adenocarcinoma. Clin. Cancer Res. 2019, 25, 7475–7484. [Google Scholar] [CrossRef] [Green Version]
- Travis, W.D.; Brambilla, E.; Nicholson, A.G.; Yatabe, Y.; Austin, J.H.M.; Beasley, M.B.; Chirieac, L.R.; Dacic, S.; Duhig, E.; Flieder, D.B.; et al. The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J. Thorac. Oncol. 2015, 10, 1243–1260. [Google Scholar] [CrossRef] [Green Version]
- Martini, N.; Bains, M.S.; Burt, M.E.; Zakowski, M.F.; McCormack, P.; Rusch, V.W.; Ginsberg, R.J. Incidence of local recurrence and second primary tumors in resected stage I lung cancer. J. Thorac. Cardiovasc. Surg. 1995, 109, 120–129. [Google Scholar] [CrossRef] [Green Version]
- Maeda, R.; Yoshida, J.; Ishii, G.; Hishida, T.; Nishimura, M.; Nagai, K. Risk Facotrs for tumor recurrence in patients with early-stage (stage I and II) non-small cell lung cancer. Chest 2011, 140, 1494–1502. [Google Scholar] [CrossRef]
- Kobayashi, N.; Toyooka, S.; Soh, J.; Ichimura, K.; Yanai, H.; Suehisa, H.; Ichihara, S.; Yamane, M.; Aoe, M.; Sano, Y.; et al. Risk Factors for Recurrence and Unfavorable Prognosis in Patients with Stage I NSCLC and a Tumor Diameter of 20 mm or Less. J. Thorac. Oncol. 2007, 2, 808–812. [Google Scholar] [CrossRef] [Green Version]
- Dziedzic, D.A.; Rudzinski, P.; Langfort, R.; Orlowski, T. Risk Factors for Local and Distant Recurrence after Surgical Treatment in Patients with Non–Small-Cell Lung Cancer. Clin. Lung Cancer 2016, 17, e157–e167. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, E.L.; Meier, P. Nonparametric Estimation from Incomplete Observations. J. Am. Stat. Assoc. 1958, 53, 457. [Google Scholar] [CrossRef]
- Improta, G.; Zupa, A.; Natalicchio, M.I.; Sisinni, L.; Marinaccio, A.; Bozza, G.; Vita, G.; Aieta, M.; Landriscina, M. Uncommon frame-shift exon 19 EGFR mutations are sensitive to EGFR tyrosine kinase inhibitors in non-small cell lung carcinoma. Med. Oncol. 2018, 35, 28. [Google Scholar] [CrossRef] [PubMed]
- Tokudome, N.; Koh, Y.; Akamatsu, H.; Fujimoto, D.; Okamoto, I.; Nakagawa, K.; Hida, T.; Imamura, F.; Morita, S.; Yamamoto, N. Differential significance of molecular subtypes which were classified into EGFR exon 19 deletion on the first line afatinib monotherapy. BMC Cancer 2020, 20, 103. [Google Scholar] [CrossRef]
- VanderLaan, P.; Rangachari, D.; Mockus, S.M.; Spotlow, V.; Reddi, H.V.; Malcolm, J.; Huberman, M.S.; Joseph, L.J.; Kobayashi, S.S.; Costa, D.B. Mutations in TP53, PIK3CA, PTEN and other genes in EGFR mutated lung cancers: Correlation with clinical outcomes. Lung Cancer 2017, 106, 17–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aisner, D.L.; Sholl, L.M.; Berry, L.D.; Rossi, M.R.; Chen, H.; Fujimoto, J.; Moreira, A.L.; Ramalingam, S.S.; Villaruz, L.C.; Otterson, G.A.; et al. The Impact of Smoking and TP53 Mutations in Lung Adenocarcinoma Patients with Targetable Mutations—The Lung Cancer Mutation Consortium (LCMC2). Clin. Cancer Res. 2018, 24, 1038–1047. [Google Scholar] [CrossRef] [Green Version]
- Stewart, D.J. Wnt Signaling Pathway in Non-Small Cell Lung Cancer. J. Natl. Cancer Inst. 2014, 106, djt356. [Google Scholar] [CrossRef]
- Rapp, J.; Jaromi, L.; Kvell, K.; Miskei, G.; Pongracz, J.E. WNT signaling—Lung cancer is no exception. Respir. Res. 2017, 18, 167. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, M.; Akiri, G.; Chin, C.; Wisnivesky, J.P.; Beasley, M.B.; Weiser, T.S.; Swanson, S.J.; Aaronson, S.A. Wnt Pathway Activation Predicts Increased Risk of Tumor Recurrence in Patients with Stage I Nonsmall Cell Lung Cancer. Ann. Surg. 2013, 257, 548–554. [Google Scholar] [CrossRef] [Green Version]
- Chun, Y.J.; Choi, J.W.; Kim, S.; Kim, H.R.; Cho, B.C.; Hong, M.H.; Jung, D.; Son, H.; Cho, E.K.; Korean Lung Cancer Consortium (KLCC); et al. Molecular characterization of lung adenocarcinoma from Korean patients using next generation sequencing. PLoS ONE 2019, 14, e0224379. [Google Scholar] [CrossRef]
- Kim, S.; Jeong, S. Mutation Hotspots in the β-Catenin Gene: Lessons from the Human Cancer Genome Databases. Mol. Cells 2019, 42, 8–16. [Google Scholar] [CrossRef]
- Kurnit, K.; Kim, G.N.; Fellman, B.M.; Urbauer, D.L.; Mills, G.; Zhang, W.; Broaddus, R.R. CTNNB1 (beta-catenin) mutation identifies low grade, early stage endometrial cancer patients at increased risk of recurrence. Mod. Pathol. 2017, 30, 1032–1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collisson, E.A.; Campbell, J.; Brooks, A.; Berger, A.; Lee, W.; Chmielecki, J.; Beer, D.; Cope, L.; Creighton, C.; Danilova, L.; et al. The Cancer Genome Atlas Research Network Comprehensive molecular profiling of lung adenocarcinoma. Nat. Cell Biol. 2014, 511, 543–550. [Google Scholar] [CrossRef]
- Ma, X.; Le Teuff, G.; Lacas, B.; Tsao, M.; Graziano, S.; Pignon, J.-P.; Douillard, J.-Y.; Le Chevalier, T.; Seymour, L.; Filipits, M.; et al. Prognostic and Predictive Effect of TP53 Mutations in Patients with Non–Small Cell Lung Cancer from Adjuvant Cisplatin—Based Therapy Randomized Trials: A LACE-Bio Pooled Analysis. J. Thorac. Oncol. 2016, 11, 850–861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, J.J.; Cardarella, S.; Lydon, C.A.; Dahlberg, S.; Jackman, D.M.; Jänne, P.A.; Johnson, B.E. Five-Year Survival in EGFR-Mutant Metastatic Lung Adenocarcinoma Treated with EGFR-TKIs. J. Thorac. Oncol. 2016, 11, 556–565. [Google Scholar] [CrossRef] [Green Version]
- Isaka, T.; Yokose, T.; Ito, H.; Nagata, M.; Furumoto, H.; Nishii, T.; Katayama, K.; Yamada, K.; Nakayama, H.; Masuda, M. Correlations Between the EGFR Mutation Status and Clinicopathological Features of Clinical Stage I Lung Adenocarcinoma. Medicine 2015, 94, e1784. [Google Scholar] [CrossRef]
- Li, W.-Q.; Cui, J.-W. Non-small cell lung cancer patients with ex19del or exon 21 L858R mutation: Distinct mechanisms, different efficacies to treatments. J. Cancer Res. Clin. Oncol. 2020, 146, 2329–2338. [Google Scholar] [CrossRef]
- Demicheli, R.; Fornili, M.; Ambrogi, F.; Higgins, K.; Boyd, J.A.; Biganzoli, E.; Kelsey, C. Recurrence Dynamics for Non–Small-Cell Lung Cancer: Effect of Surgery on the Development of Metastases. J. Thorac. Oncol. 2012, 7, 723–730. [Google Scholar] [CrossRef] [Green Version]
- Jung, Y.-S.; Park, J.-I. Wnt signaling in cancer: Therapeutic targeting of Wnt signaling beyond β-catenin and the destruction complex. Exp. Mol. Med. 2020, 52, 183–191. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Patients | No Recurrence (%) | Recurrence (%) | p-Value |
|---|---|---|---|---|
| The number of patients | 131 | 98 (74.8) | 33 (25.2) | p < 0.001 |
| Age | 64.0 ± 11.2 | 65.5 ± 10.9 | 58.8 ± 11.2 | 0.01 |
| <65 years | 71 (54.2) | 47 (66.2) | 24 (33.8) | 0.007 |
| ≥65 years | 60 (45.8) | 51 (85.0) | 9 (15.0) | |
| Sex | 0.7 | |||
| male | 57 (43.8) | 43 (75.5) | 14 (24.5) | |
| female | 74 (56.2) | 55 (74.3) | 19 (25.7) | |
| Smoking history (n = 128 a) | 0.73 | |||
| Non-smoker | 80 (62.5) | 60 (75.0) | 20 (25.0) | |
| Ever-smoker | 48 (37.5) | 36 (75.0) | 12 (25.0) | |
| Smoking dose | 9.6 ± 16.5 | 10.1 ± 16.9 | 8.1 ± 14.9 | 0.56 |
| Non-smoker | 80 (62.5) | 60 (75.0) | 20 (25.0) | 0.47 * |
| <10 PYS | 16 (12.6) | 13 (81.2) | 3 (18.8) | |
| 11–30 PYS | 12 (10.2) | 10 (83.3) | 2 (16.7) | |
| >30 PYS | 20 (15.7) | 14 (75) | 6 (25) | |
| Stage b | 0.001 * | |||
| IA | 82 (62.6) | 70 (85.4) | 12 (14.6) | |
| IB | 29 (22.1) | 23 (82.8) | 5 (17.2) | |
| II | 9 (6.9) | 3 (33.3) | 6 (66.7) | |
| IIIA | 11 (8.4) | 2 (18.2) | 9 (81.8) | |
| Surgical procedure | 0.53 | |||
| sublobar resection | 20 (15.4) | 14 (70) | 6 (30.0) | |
| lobectomy | 111 (84.6) | 85 (76.6) | 26 (23.4) | |
| Pathologic invasion | ||||
| VPI | 28 (20.0) | 13 (46.4) | 15 (53.6) | 0.001 |
| No VPI | 103 (80.0) | 87 (84.3) | 16 (15.7) | |
| LVI | 8 (5.3) | 2 (25) | 6 (75.0) | 0.003 * |
| no LVI | 123 (94.7) | 98 (78.0) | 25 (22.0) | |
| EGFR mutation subtype | ||||
| L858R/L861Q | 58/2 (45.8) | 49 (81.7) | 11 (18.3) | 0.3 * |
| Exon 19 del | 56 (42.7) | 39 (69.7) | 17 (30.3) | |
| Exon 20 ins | 5 (3.8) | 3 (60) | 2 (40) | |
| Compound mutation c | 10 (7.7) | 7 (66.7) | 3 (30) | |
| Adjuvant chemotherapy | ||||
| No treatment | 94 (71.8) | 79 (85.1) | 15 (14.9) | |
| Treatment | 37 (28.2) | 19 (51.4) | 18 (47.2) | 0.001 |
| Death | 16 (12.3) | 0 (0) | 16 (100) | <0.001 * |
| Univariate Analysis | Multivariate Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Category | Variables | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| Age | ≥65 vs. <65 | 0.37 | 0.16–0.82 | 0.009 | 0.38 | 0.15–0.97 | 0.04 |
| Sex | Male vs. female | 0.93 | 0.46–1.89 | 0.85 | 0.75 | 0.24–2.28 | 0.61 |
| Smoking history | Ever-smoker vs. non-smoker | 1.04 | 0.49–2.17 | 0.91 | 1.15 | 0.36–3.59 | 0.8 |
| Pathologic stage | II-III vs. I | 9.23 | 4.45–18.7 | <0.001 | 8.02 | 3.73–17.2 | <0.001 |
| Extension of surgery | sublobar resection or lobectomy | 1.32 | 0.54–3.21 | 0.53 | 1.44 | 0.74–2.80 | 0.27 |
| Pathologic invasion | VPI vs. none | 4.52 | 2.23–9.18 | <0.001 | 8.02 | 3.73–17.2 | <0.001 |
| Adjuvant chemotherapy | Adjuvant chemothrapy | 4.78 | 2.36–9.67 | <0.001 | 2.21 | 1.14–4.24 | 0.017 |
| No. of co-mutation | 1 vs. 0 | 1.51 | 0.66–3.4 | 0.32 | 1.76 | 0.72–4.3 | 0.213 |
| No. of co-mutation | 2 vs. 0 | 3.84 | 1.47–10.1 | 0.006 | 5.57 | 1.57–19.6 | 0.008 |
| EGFR mutation | 19-del vs. 21L858R (all stage) | 1.88 | 0.87–4.07 | 0.1 | 1.82 | 0.76–4.32 | 0.17 |
| 19-del vs. 21L858R (IB-IIIA) | 4.01 | 1.41–11.3 | 0.009 | 8.31 | 1.98–34.8 | 0.004 | |
| pE746_A 750del vs. 21L858R | 2.19 | 1.04–4.60 | 0.03 | 1.7 | 0.75–3.83 | 0.2 | |
| pL747_P753delinS vs. pE746_A 750del | 2.52 | 0.71–8.88 | 0.15 | 1.69 | 0.75–3.83 | 0.2 | |
| pL747_P753delinS vs. 21L858R | 6.76 | 1.93–23.7 | 0.003 | 7.55 | 1.91–29.8 | 0.004 | |
| CTNNB1 | CTNNB1/EGFR vs. EGFR | 5.19 | 1.97–13.6 | 0.001 | 8.65 | 3.0–24.9 | <0.001 |
| TP53 mutation | TP53/EGFR vs. EGFR (All stage) | 1.89 | 0.71–5.05 | 0.2 | 2.14 | 0.84–5.43 | 0.1 |
| TP53/EGFR vs. EGFR(IB-IIIA) | 3.48 | 1.21–10.0 | 0.01 | 3.06 | 1.04–11.7 | 0.05 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, I.A.; Hur, J.Y.; Kim, H.J.; Lee, S.A.; Hwang, J.J.; Kim, W.S.; Lee, K.Y. Targeted Next-Generation Sequencing Analysis Predicts the Recurrence in Resected Lung Adenocarcinoma Harboring EGFR Mutations. Cancers 2021, 13, 3632. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13143632
Kim IA, Hur JY, Kim HJ, Lee SA, Hwang JJ, Kim WS, Lee KY. Targeted Next-Generation Sequencing Analysis Predicts the Recurrence in Resected Lung Adenocarcinoma Harboring EGFR Mutations. Cancers. 2021; 13(14):3632. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13143632
Chicago/Turabian StyleKim, In Ae, Jae Young Hur, Hee Joung Kim, Song Am Lee, Jae Joon Hwang, Wan Seop Kim, and Kye Young Lee. 2021. "Targeted Next-Generation Sequencing Analysis Predicts the Recurrence in Resected Lung Adenocarcinoma Harboring EGFR Mutations" Cancers 13, no. 14: 3632. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13143632