
Overview of Oral Potentially Malignant Disorders: From Risk Factors to Specific Therapies

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Epidemiology and Risk Factors
2.1. Tobacco and Alcohol
2.2. HPV (Human Papilloma Virus)
2.3. Areca Nut Chewing and Microbiome Alteration
2.4. Other Risk Factors
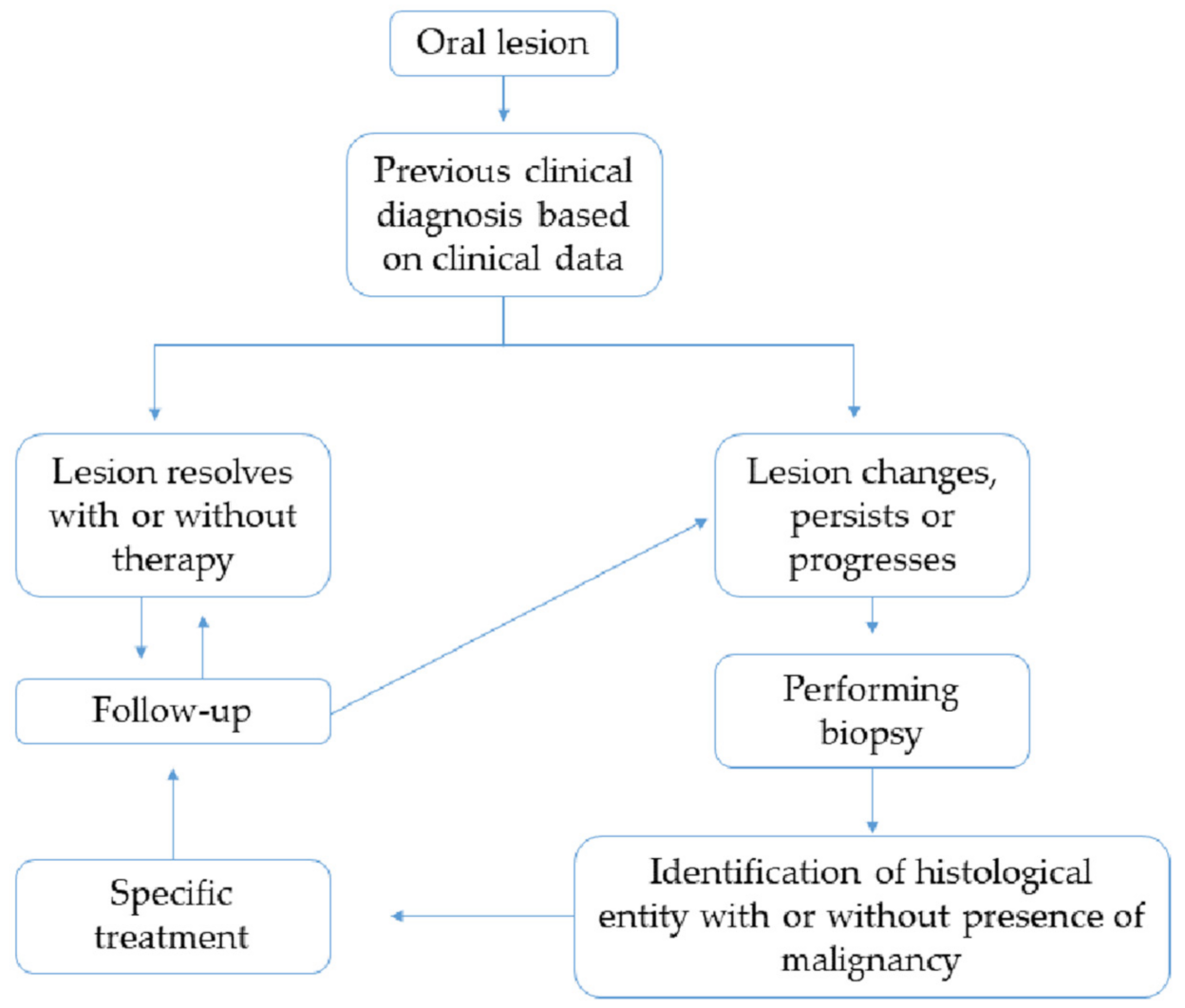
3. Early Diagnosis
4. Clinicopathological Features of OPMDs
4.1. Oral Leukoplakia (OL)
4.2. Proliferative Verrucous Leucoplakia (PVL)
4.3. Oral Erythroplakia (OE)
4.4. Oral Lichen Planus (OLP)
4.5. Oral Submucous Fibrosis (OSF)
4.6. Oral Epithelial Dysplasia (OED)
HPV-Associated Oral Epithelial Dysplasia
5. Molecular Alterations
6. Update of OPMDs Therapeutic Strategies
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Warnakulasuriya, S.; Johnson, N.W.; van der Waal, I. Nomenclature and classification of potentially malignant disorders of the oral mucosa. J. Oral Pathol. Med. 2007, 36, 575–580. [Google Scholar] [CrossRef]
- Warnakulasuriya, S. Clinical features and presentation of oral potentially malignant disorders. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 582–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aguirre-Urizar, J.M.; Lafuente-Ibáñez de Mendoza, I.; Warnakulasuriya, S. Malignant transformation of oral leukoplakia: Systematic review and meta-analysis of the last 5 years. Oral Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Abati, S.; Bramati, C.; Bondi, S.; Lissoni, A.; Trimarchi, M. Oral cancer and precancer: A narrative review on the relevance of early diagnosis. Int. J. Environ. Res. Public Health 2020, 17, 9160. [Google Scholar] [CrossRef] [PubMed]
- Porter, S.; Gueiros, L.A.; Leao, J.C.; Fedele, S. Risk factors and etiopathogenesis of potentially premalignant oral epithelial lesions. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 603–611. [Google Scholar] [CrossRef] [Green Version]
- Hernandez, B.Y.; Zhu, X.; Goodman, M.T.; Gatewood, R.; Mendiola, P.; Quinata, K.; Paulino, Y.C. Betel nut chewing, oral premalignant lesions, and the oral microbiome. PLoS ONE 2017, 12, e0172196. [Google Scholar] [CrossRef]
- Resende, R.G.; Correia-Silva Jde, F.; Galvao, C.F.; Gomes, C.C.; Carneiro, M.A.; Gomez, R.S. Oral leukoplakia in a patient with Fanconi anemia: Recurrence or a new primary lesion? J. Oral Maxillofac. Surg. 2011, 69, 1940–1943. [Google Scholar] [CrossRef]
- Kuo, C.F.; Luo, S.F.; Yu, K.H.; Chou, I.J.; Tseng, W.Y.; Chang, H.C.; Fang, Y.F.; Chiou, M.J.; See, L.C. Cancer risk among patients with systemic sclerosis: A nationwide population study in Taiwan. Scand. J. Rheumatol. 2012, 41, 44–49. [Google Scholar] [CrossRef]
- Stoopler, E.T.; Homeida, L.; Sollecito, T.P. Oral lesions associated with Fanconi anemia. Rev. Bras. Hematol. Hemoter. 2017, 39, 175–176. [Google Scholar] [CrossRef]
- Awadallah, M.; Idle, M.; Patel, K.; Kademani, D. Management update of potentially premalignant oral epithelial lesions. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 628–636. [Google Scholar] [CrossRef] [Green Version]
- Mithani, S.K.; Mydlarz, W.K.; Grumbine, F.L.; Smith, I.M.; Califano, J.A. Molecular genetics of premalignant oral lesions. Oral Dis. 2007, 13, 126–133. [Google Scholar] [CrossRef]
- Mogedas-Vegara, A.; Hueto-Madrid, J.A.; Chimenos-Kustner, E.; Bescos-Atin, C. Oral leukoplakia treatment with the carbon dioxide laser: A systematic review of the literature. J. Craniomaxillofac. Surg. 2016, 44, 331–336. [Google Scholar] [CrossRef] [Green Version]
- Mogedas-Vegara, A.; Hueto-Madrid, J.A.; Chimenos-Kustner, E.; Bescos-Atin, C. The treatment of oral leukoplakia with the CO2 laser: A retrospective study of 65 patients. J. Craniomaxillofac. Surg. 2015, 43, 677–681. [Google Scholar] [CrossRef] [Green Version]
- Vohra, F.; Al-Kheraif, A.A.; Qadri, T.; Hassan, M.I.; Ahmed, A.; Warnakulasuriya, S.; Javed, F. Efficacy of photodynamic therapy in the management of oral premalignant lesions. A systematic review. Photodiagnosis Photodyn. Ther. 2015, 12, 150–159. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wang, B.; Zheng, S.; He, Y. Photodynamic therapy in the treatment of oral leukoplakia: A systematic review. Photodiagnosis Photodyn. Ther. 2019, 25, 17–22. [Google Scholar] [CrossRef]
- Goodson, M.L.; Sugden, K.; Kometa, S.; Thomson, P.J. Complications following interventional laser surgery for oral cancer and precancerous lesions. Br. J. Oral Maxillofac. Surg. 2012, 50, 597–600. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Armayones, S.; Chimenos-Kustner, E.; Mari, A.; Tous, S.; Penin, R.; Clavero, O.; Quiros, B.; Pavon, M.A.; Taberna, M.; Alemany, L.; et al. Human papillomavirus in premalignant oral lesions: No evidence of association in a Spanish cohort. PLoS ONE 2019, 14, e0210070. [Google Scholar] [CrossRef] [PubMed]
- Ostwald, C.; Rutsatz, K.; Schweder, J.; Schmidt, W.; Gundlach, K.; Barten, M. Human papillomavirus 6/11, 16 and 18 in oral carcinomas and benign oral lesions. Med. Microbiol. Immunol. 2003, 192, 145–148. [Google Scholar] [CrossRef]
- Upile, T.; Jerjes, W.; Al-Khawalde, M.; Radhi, H.; Sudhoff, H. Oral sex, cancer and death: Sexually transmitted cancers. Head Neck Oncol. 2012, 4, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jerjes, W.; Upile, T.; Radhi, H.; Petrie, A.; Abiola, J.; Adams, A.; Kafas, P.; Callear, J.; Carbiner, R.; Rajaram, K.; et al. The effect of tobacco and alcohol and their reduction/cessation on mortality in oral cancer patients: Short communication. Head Neck Oncol. 2012, 4, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melis, M.; Zhang, T.; Scognamiglio, T.; Gudas, L.J. Mutations in long-lived epithelial stem cells and their clonal progeny in pre-malignant lesions and in oral squamous cell carcinoma. Carcinogenesis 2020, 41, 1553–1564. [Google Scholar] [CrossRef] [PubMed]
- Izumchenko, E.; Sun, K.; Jones, S.; Brait, M.; Agrawal, N.; Koch, W.; McCord, C.L.; Riley, D.R.; Angiuoli, S.V.; Velculescu, V.E.; et al. Notch1 mutations are drivers of oral tumorigenesis. Cancer Prev. Res. 2015, 8, 277–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, S.D.; De Costa, A.M.; Young, M.R. Effect of the premalignant and tumor microenvironment on immune cell cytokine production in head and neck cancer. Cancers 2014, 6, 756–770. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Zhao, Y. Human papillomavirus infection in oral potentially malignant disorders and cancer. Arch. Oral Biol. 2017, 83, 334–339. [Google Scholar] [CrossRef]
- Yete, S.; D’Souza, W.; Saranath, D. High-risk human Papillomavirus in oral cancer: Clinical implications. Oncology 2018, 94, 133–141. [Google Scholar] [CrossRef]
- Zendeli-Bedjeti, L.; Popovska, M.; Atanasovska-Stojanovska, A.; Duvlis, S. Human papillomavirus as a potential risk factor for oral premalignant lesions. Acta Clin. Croat. 2017, 56, 369–374. [Google Scholar] [CrossRef] [Green Version]
- Gupta, P.C.; Warnakulasuriya, S. Global epidemiology of areca nut usage. Addict. Biol. 2002, 7, 77–83. [Google Scholar] [CrossRef]
- Arora, S.; Squier, C. Areca nut trade, globalisation and its health impact: Perspectives from India and South-east Asia. Perspect. Public Health 2019, 139, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Warnakulasuriya, S.; Trivedy, C.; Peters, T.J. Areca nut use: An independent risk factor for oral cancer. BMJ 2002, 324, 799–800. [Google Scholar] [CrossRef]
- Raja, K.B.; Hazarey, V.K.; Peters, T.J.; Warnakulasuriya, S. Effect of areca nut on salivary copper concentration in chronic chewers. Biometals 2007, 20, 43–47. [Google Scholar] [CrossRef]
- Lord, G.A.; Lim, C.K.; Warnakulasuriya, S.; Peters, T.J. Chemical and analytical aspects of areca nut. Addict. Biol. 2002, 7, 99–102. [Google Scholar] [CrossRef]
- Trivedy, C.; Baldwin, D.; Warnakulasuriya, S.; Johnson, N.; Peters, T. Copper content in Areca catechu (betel nut) products and oral submucous fibrosis. Lancet 1997, 349, 1447. [Google Scholar] [CrossRef]
- Reichart, P.A.; Warnakulasuriya, S. Oral lichenoid contact lesions induced by areca nut and betel quid chewing: A mini review. J. Investig. Clin. Dent. 2012, 3, 163–166. [Google Scholar] [CrossRef] [PubMed]
- Angadi, P.V.; Rao, S.S. Areca nut in pathogenesis of oral submucous fibrosis: Revisited. Oral Maxillofac. Surg. 2011, 15, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Stoopler, E.T.; Parisi, E.; Sollecito, T.P. Betel quid-induced oral lichen planus: A case report. Cutis 2003, 71, 307–311. [Google Scholar] [PubMed]
- Li, Y.C.; Chang, J.T.; Chiu, C.; Lu, Y.C.; Li, Y.L.; Chiang, C.H.; You, G.R.; Lee, L.Y.; Cheng, A.J. Areca nut contributes to oral malignancy through facilitating the conversion of cancer stem cells. Mol. Carcinog. 2016, 55, 1012–1023. [Google Scholar] [CrossRef]
- Li, Y.C.; Cheng, A.J.; Lee, L.Y.; Huang, Y.C.; Chang, J.T. Multifaceted mechanisms of areca nuts in oral carcinogenesis: The molecular pathology from precancerous condition to malignant transformation. J. Cancer 2019, 10, 4054–4062. [Google Scholar] [CrossRef] [Green Version]
- Zhong, X.; Lu, Q.; Zhang, Q.; He, Y.; Wei, W.; Wang, Y. Oral microbiota alteration associated with oral cancer and areca chewing. Oral Dis. 2021, 27, 226–239. [Google Scholar] [CrossRef]
- Chattopadhyay, I.; Verma, M.; Panda, M. Role of oral microbiome signatures in diagnosis and prognosis of oral cancer. Technol. Cancer Res. Treat. 2019, 18, 1533033819867354. [Google Scholar] [CrossRef] [Green Version]
- Geng, F.; Zhang, Y.; Lu, Z.; Zhang, S.; Pan, Y. Fusobacterium nucleatum caused DNA damage and promoted cell proliferation by the Ku70/p53 pathway in oral cancer cells. DNA Cell Biol. 2020, 39, 144–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grimm, M.; Cetindis, M.; Biegner, T.; Lehman, M.; Munz, A.; Teriete, P.; Reinert, S. Serum vitamin D levels of patients with oral squamous cell carcinoma (OSCC) and expression of vitamin D receptor in oral precancerous lesions and OSCC. Med. Oral Patol. Oral Cir. Bucal. 2015, 20, e188–e195. [Google Scholar] [CrossRef]
- Olesen, A.B.; Svaerke, C.; Farkas, D.K.; Sorensen, H.T. Systemic sclerosis and the risk of cancer: A nationwide population-based cohort study. Br. J. Dermatol. 2010, 163, 800–806. [Google Scholar] [CrossRef]
- Onishi, A.; Sugiyama, D.; Kumagai, S.; Morinobu, A. Cancer incidence in systemic sclerosis: Meta-analysis of population-based cohort studies. Arthritis Rheum. 2013, 65, 1913–1921. [Google Scholar] [CrossRef]
- Fernandez Garcia, M.S.; Teruya-Feldstein, J. The diagnosis and treatment of dyskeratosis congenita: A review. J. Blood Med. 2014, 5, 157–167. [Google Scholar]
- Seoane, J.; Alvarez-Novoa, P.; Gomez, I.; Takkouche, B.; Diz, P.; Warnakulasiruya, S.; Seoane-Romero, J.M.; Varela-Centelles, P. Early oral cancer diagnosis: The Aarhus statement perspective. A systematic review and meta-analysis. Head Neck 2016, 38, E2182–E2189. [Google Scholar] [CrossRef] [PubMed]
- Papadiochou, S.; Papadiochos, I.; Perisanidis, C.; Papadogeorgakis, N. Medical practitioners’ educational competence about oral and oropharyngeal carcinoma: A systematic review and meta-analysis. Br. J. Oral Maxillofac. Surg. 2020, 58, 3–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varela-Centelles, P.; Seoane, J.; Lopez-Cedrun, J.L.; Fernandez-Sanroman, J.; Garcia-Martin, J.M.; Takkouche, B.; Alvarez-Novoa, P.; Seoane-Romero, J.M. The length of patient and primary care time interval in the pathways to treatment in symptomatic oral cancer. A quantitative systematic review. Clin. Otolaryngol. 2018, 43, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Fuller, C.; Camilon, R.; Nguyen, S.; Jennings, J.; Day, T.; Gillespie, M.B. Adjunctive diagnostic techniques for oral lesions of unknown malignant potential: Systematic review with meta-analysis. Head Neck 2015, 37, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Macey, R.; Walsh, T.; Brocklehurst, P.; Kerr, A.R.; Liu, J.L.; Lingen, M.W.; Ogden, G.R.; Warnakulasuriya, S.; Scully, C. Diagnostic tests for oral cancer and potentially malignant disorders in patients presenting with clinically evident lesions. Cochrane Database Syst. Rev. 2015, 5, CD010276. [Google Scholar] [CrossRef] [Green Version]
- Brocklehurst, P.; Kujan, O.; O’Malley, L.A.; Ogden, G.; Shepherd, S.; Glenny, A.M. Screening programmes for the early detection and prevention of oral cancer. Cochrane Database Syst. Rev. 2013, 11, CD004150. [Google Scholar] [CrossRef] [Green Version]
- Walsh, T.; Liu, J.L.; Brocklehurst, P.; Glenny, A.M.; Lingen, M.; Kerr, A.R.; Ogden, G.; Warnakulasuriya, S.; Scully, C. Clinical assessment to screen for the detection of oral cavity cancer and potentially malignant disorders in apparently healthy adults. Cochrane Database Syst. Rev. 2013, 2013, CD010173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warnakulasuriya, S.; Fennell, N.; Diz, P.; Seoane, J.; Rapidis, A. An appraisal of oral cancer and pre-cancer screening programmes in Europe: A systematic review. J. Oral Pathol. Med. 2015, 44, 559–570. [Google Scholar] [CrossRef] [PubMed]
- van der Waal, I. Potentially malignant disorders of the oral and oropharyngeal mucosa; terminology, classification and present concepts of management. Oral Oncol. 2009, 45, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Gorsky, M.; Epstein, J.B. The effect of retinoids on premalignant oral lesions: Focus on topical therapy. Cancer 2002, 95, 1258–1264. [Google Scholar] [CrossRef] [PubMed]
- Capella, D.L.; Goncalves, J.M.; Abrantes, A.A.A.; Grando, L.J.; Daniel, F.I. Proliferative verrucous leukoplakia: Diagnosis, management and current advances. Braz. J. Otorhinolaryngol. 2017, 83, 585–593. [Google Scholar] [CrossRef] [PubMed]
- van der Waal, I. Potentially malignant disorders of the oral and oropharyngeal mucosa; present concepts of management. Oral Oncol. 2010, 46, 423–425. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, R.; Thayalan, D.K.; Padmanaban, R.; Ramadas, R.; Annasamy, R.K.; Anandan, N. Association of serum and salivary tumor necrosis factor-alpha with histological grading in oral cancer and its role in differentiating premalignant and malignant oral disease. Asian Pac. J. Cancer Prev. 2014, 15, 7141–7148. [Google Scholar] [CrossRef] [Green Version]
- Yang, S.W.; Lee, Y.S.; Chang, L.C.; Hsieh, T.Y.; Chen, T.A. Outcome of excision of oral erythroplakia. Br. J. Oral Maxillofac. Surg. 2015, 53, 142–147. [Google Scholar] [CrossRef]
- Kurago, Z.B. Etiology and pathogenesis of oral lichen planus: An overview. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 122, 72–80. [Google Scholar] [CrossRef]
- Alrashdan, M.S.; Cirillo, N.; McCullough, M. Oral lichen planus: A literature review and update. Arch. Dermatol. Res. 2016, 308, 539–551. [Google Scholar] [CrossRef]
- Al-Hashimi, I.; Schifter, M.; Lockhart, P.B.; Wray, D.; Brennan, M.; Migliorati, C.A.; Axell, T.; Bruce, A.J.; Carpenter, W.; Eisenberg, E.; et al. Oral lichen planus and oral lichenoid lesions: Diagnostic and therapeutic considerations. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 103, S25.e1–S25.e12. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Pola, M.J.; Gonzalez-Alvarez, L.; Garcia-Martin, J.M. Treatment of oral lichen planus. Systematic review and therapeutic guide. Med. Clin. 2017, 149, 351–362. [Google Scholar] [CrossRef]
- Arakeri, G.; Brennan, P.A. Oral submucous fibrosis: An overview of the aetiology, pathogenesis, classification, and principles of management. Br. J. Oral Maxillofac. Surg. 2013, 51, 587–593. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, P.; Manjunath, M.; Khakhla, D.; Gubrellay, P.; Bhargava, R.; Guruprasad, L. Assessment and correlation between functional and histological staging of oral submucous fibrosis: A clinicohistopathologic study. Natl. J. Maxillofac. Surg. 2019, 10, 27–32. [Google Scholar] [PubMed]
- Shakunthala, G.K.; Annigeri, R.G.; Arunkumar, S. Role of oxidative stress in the pathogenesis of oral submucous fibrosis: A preliminary prospective study. Contemp. Clin. Dent. 2015, 6, S172–S174. [Google Scholar] [CrossRef]
- Shen, Y.W.; Shih, Y.H.; Fuh, L.J.; Shieh, T.M. Oral Submucous Fibrosis: A Review on Biomarkers, Pathogenic Mechanisms, and Treatments. Int. J. Mol. Sci. 2020, 21, 7231. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Jawanda, M.K.; Madhushankari, G.S. Current challenges and the diagnostic pitfalls in the grading of epithelial dysplasia in oral potentially malignant disorders: A review. J. Oral Biol. Craniofac. Res. 2020, 10, 788–799. [Google Scholar] [CrossRef] [PubMed]
- Muller, S. Oral epithelial dysplasia, atypical verrucous lesions and oral potentially malignant disorders: Focus on histopathology. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 591–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kujan, O.; Oliver, R.J.; Khattab, A.; Roberts, S.A.; Thakker, N.; Sloan, P. Evaluation of a new binary system of grading oral epithelial dysplasia for prediction of malignant transformation. Oral Oncol. 2006, 42, 987–993. [Google Scholar] [CrossRef]
- Nankivell, P.; Williams, H.; Matthews, P.; Suortamo, S.; Snead, D.; McConkey, C.; Mehanna, H. The binary oral dysplasia grading system: Validity testing and suggested improvement. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 87–94. [Google Scholar] [CrossRef]
- Lerman, M.A.; Almazrooa, S.; Lindeman, N.; Hall, D.; Villa, A.; Woo, S.B. HPV-16 in a distinct subset of oral epithelial dysplasia. Mod. Pathol. 2017, 30, 1646–1654. [Google Scholar] [CrossRef]
- McCord, C.; Xu, J.; Xu, W.; Qiu, X.; McComb, R.J.; Perez-Ordonez, B.; Bradley, G. Association of high-risk human papillomavirus infection with oral epithelial dysplasia. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Khanal, S.; Trainor, P.J.; Zahin, M.; Ghim, S.J.; Joh, J.; Rai, S.N.; Jenson, A.B.; Shumway, B.S. Histologic variation in high grade oral epithelial dysplasia when associated with high-risk human papillomavirus. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2017, 123, 566–585. [Google Scholar] [CrossRef] [PubMed]
- Hendawi, N.; Niklander, S.; Allsobrook, O.; Khurram, S.A.; Bolt, R.; Doorbar, J.; Speight, P.M.; Hunter, K.D. HPV can establish productive infection in dysplastic oral mucosa, but HPV status is poorly predicted by histological features and p16 expression. Histopathology 2019, 76, 592–602. [Google Scholar] [CrossRef] [PubMed]
- de la Cour, C.D.; Sperling, C.D.; Belmonte, F.; Syrjanen, S.; Kjaer, S.K. Human papillomavirus prevalence in oral potentially malignant disorders: Systematic review and meta-analysis. Oral Dis. 2021, 27, 431–438. [Google Scholar] [CrossRef]
- Odell, E.; Thavaraj, S.; Gale, N.; Nadal, A.; Zidar, N.; Gnepp, D. Precursor Lesions for Squamous Carcinoma of the Upper Aerodigestive Tract. In Gnepp's Diagnostic Surgical Pathology of the Head and Neck, 3rd ed.; Gnepp, D., Bishop, J., Eds.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 1–62. [Google Scholar]
- Mao, L.; Lee, J.S.; Fan, Y.H.; Ro, J.Y.; Batsakis, J.G.; Lippman, S.; Hittelman, W.; Hong, W.K. Frequent microsatellite alterations at chromosomes 9p21 and 3p14 in oral premalignant lesions and their value in cancer risk assessment. Nat. Med. 1996, 2, 682–685. [Google Scholar] [CrossRef]
- Mao, L.; El-Naggar, A.K.; Papadimitrakopoulou, V.; Shin, D.M.; Shin, H.C.; Fan, Y.; Zhou, X.; Clayman, G.; Lee, J.J.; Lee, J.S.; et al. Phenotype and genotype of advanced premalignant head and neck lesions after chemopreventive therapy. J. Natl. Cancer Inst. 1998, 90, 1545–1551. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.J.; Hong, W.K.; Hittelman, W.N.; Mao, L.; Lotan, R.; Shin, D.M.; Benner, S.E.; Xu, X.C.; Lee, J.S.; Papadimitrakopoulou, V.M.; et al. Predicting cancer development in oral leukoplakia: Ten years of translational research. Clin. Cancer Res. 2000, 6, 1702–1710. [Google Scholar]
- Zhang, L.; Poh, C.F.; Williams, M.; Laronde, D.M.; Berean, K.; Gardner, P.J.; Jiang, H.; Wu, L.; Lee, J.J.; Rosin, M.P. Loss of heterozygosity (LOH) profiles--validated risk predictors for progression to oral cancer. Cancer Prev. Res. 2012, 5, 1081–1089. [Google Scholar] [CrossRef] [Green Version]
- William, W.N., Jr.; Papadimitrakopoulou, V.; Lee, J.J.; Mao, L.; Cohen, E.E.; Lin, H.Y.; Gillenwater, A.M.; Martin, J.W.; Lingen, M.W.; Boyle, J.O.; et al. Erlotinib and the Risk of Oral Cancer: The Erlotinib Prevention of Oral Cancer (EPOC) Randomized Clinical Trial. JAMA Oncol. 2016, 2, 209–216. [Google Scholar] [CrossRef] [Green Version]
- Alaizari, N.A.; Sperandio, M.; Odell, E.W.; Peruzzo, D.; Al-Maweri, S.A. Meta-analysis of the predictive value of DNA aneuploidy in malignant transformation of oral potentially malignant disorders. J. Oral Pathol. Med. 2018, 47, 97–103. [Google Scholar] [CrossRef]
- Guimaraes, L.M.; Diniz, M.G.; Rogatto, S.R.; Gomez, R.S.; Gomes, C.C. The genetic basis of oral leukoplakia and its key role in understanding oral carcinogenesis. J. Oral Pathol. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Foy, J.P.; Bertolus, C.; William, W.N., Jr.; Saintigny, P. Oral premalignancy: The roles of early detection and chemoprevention. Otolaryngol. Clin. N. Am. 2013, 46, 579–597. [Google Scholar] [CrossRef] [Green Version]
- Monteiro, L.; Mello, F.W.; Warnakulasuriya, S. Tissue biomarkers for predicting the risk of oral cancer in patients diagnosed with oral leukoplakia: A systematic review. Oral Dis. 2020. [Google Scholar] [CrossRef]
- Taoudi Benchekroun, M.; Saintigny, P.; Thomas, S.M.; El-Naggar, A.K.; Papadimitrakopoulou, V.; Ren, H.; Lang, W.; Fan, Y.H.; Huang, J.; Feng, L.; et al. Epidermal growth factor receptor expression and gene copy number in the risk of oral cancer. Cancer Prev. Res. 2010, 3, 800–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amornphimoltham, P.; Sriuranpong, V.; Patel, V.; Benavides, F.; Conti, C.J.; Sauk, J.; Sausville, E.A.; Molinolo, A.A.; Gutkind, J.S. Persistent activation of the Akt pathway in head and neck squamous cell carcinoma: A potential target for UCN-01. Clin. Cancer Res. 2004, 10, 4029–4037. [Google Scholar] [CrossRef] [Green Version]
- Brito, J.A.; Gomes, C.C.; Guimaraes, A.L.; Campos, K.; Gomez, R.S. Relationship between microRNA expression levels and histopathological features of dysplasia in oral leukoplakia. J. Oral Pathol. Med. 2014, 43, 211–216. [Google Scholar] [CrossRef]
- Cervigne, N.K.; Reis, P.P.; Machado, J.; Sadikovic, B.; Bradley, G.; Galloni, N.N.; Pintilie, M.; Jurisica, I.; Perez-Ordonez, B.; Gilbert, R.; et al. Identification of a microRNA signature associated with progression of leukoplakia to oral carcinoma. Hum. Mol. Genet. 2009, 18, 4818–4829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foy, J.P.; Bertolus, C.; Ortiz-Cuaran, S.; Albaret, M.A.; Williams, W.N.; Lang, W.; Destandau, S.; Souza, G.; Sohier, E.; Kielbassa, J.; et al. Immunological and classical subtypes of oral premalignant lesions. Oncoimmunology 2018, 7, e1496880. [Google Scholar] [CrossRef] [Green Version]
- Romani, C.; Salviato, E.; Paderno, A.; Zanotti, L.; Ravaggi, A.; Deganello, A.; Berretti, G.; Gualtieri, T.; Marchini, S.; D’Incalci, M.; et al. Genome-wide study of salivary miRNAs identifies miR-423-5p as promising diagnostic and prognostic biomarker in oral squamous cell carcinoma. Theranostics 2021, 11, 2987–2999. [Google Scholar] [CrossRef]
- Ganci, F.; Sacconi, A.; Manciocco, V.; Covello, R.; Benevolo, M.; Rollo, F.; Strano, S.; Valsoni, S.; Bicciato, S.; Spriano, G.; et al. Altered peritumoral microRNA expression predicts head and neck cancer patients with a high risk of recurrence. Mod. Pathol. 2017, 30, 1387–1401. [Google Scholar] [CrossRef] [Green Version]
- Vahabi, M.; Pulito, C.; Sacconi, A.; Donzelli, S.; D’Andrea, M.; Manciocco, V.; Pellini, R.; Paci, P.; Sanguineti, G.; Strigari, L.; et al. miR-96-5p targets PTEN expression affecting radio-chemosensitivity of HNSCC cells. J. Exp. Clin. Cancer Res. 2019, 38, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kresty, L.A.; Mallery, S.R.; Knobloch, T.J.; Song, H.; Lloyd, M.; Casto, B.C.; Weghorst, C.M. Alterations of p16(INK4a) and p14(ARF) in patients with severe oral epithelial dysplasia. Cancer Res. 2002, 62, 5295–5300. [Google Scholar]
- Diez-Perez, R.; Campo-Trapero, J.; Cano-Sanchez, J.; Lopez-Duran, M.; Gonzalez-Moles, M.A.; Bascones-Ilundain, J.; Bascones-Martinez, A. Methylation in oral cancer and pre-cancerous lesions (Review). Oncol. Rep. 2011, 25, 1203–1209. [Google Scholar] [PubMed] [Green Version]
- Rabello Piva, M.; Batista De Souza, L.; Saquete Martins-Filho, P.R.; Calazans Soares, R.; De Santana Santos, T.; Sávio De Souza Andrade, E. Role of inflammation in oral carcinogenesis (Part I): Histological grading of malignancy using a binary system. Oncol. Lett. 2011, 2, 1225–1231. [Google Scholar] [CrossRef] [PubMed]
- Chaves, A.L.F.; Silva, A.G.; Maia, F.M.; Lopes, G.F.M.; de Paulo, L.F.B.; Muniz, L.V.; Dos Santos, H.B.; Soares, J.M.A.; Souza, A.A.; de Oliveira Barbosa, L.A.; et al. Reduced CD8(+) T cells infiltration can be associated to a malignant transformation in potentially malignant oral epithelial lesions. Clin. Oral Investig. 2019, 23, 1913–1919. [Google Scholar] [CrossRef] [PubMed]
- Dave, K.; Ali, A.; Magalhaes, M. Increased expression of PD-1 and PD-L1 in oral lesions progressing to oral squamous cell carcinoma: A pilot study. Sci. Rep. 2020, 10, 9705. [Google Scholar] [CrossRef]
- Carenzo, A.; Serafini, M.S.; Roca, E.; Paderno, A.; Mattavelli, D.; Romani, C.; Saintigny, P.; Koljenovic, S.; Licitra, L.; De Cecco, L.; et al. Gene expression clustering and selected head and neck cancer gene signatures highlight risk probability differences in oral premalignant lesions. Cells 2020, 9, 1828. [Google Scholar] [CrossRef]
- Hertrampf, K.; Kunkel, M.; S2k-Leitlinie Diagnostik und Management von Vorläuferläsionen des Oralen Plattenepithelkarzinoms in der Zahn-, Mund- und Kieferheilkunde. DZZ. 2020. Available online: https://www.awmf.org/leitlinien/detail/ll/007-092.html (accessed on 20 July 2021).
- Lauritano, D.; Lucchese, A.; Gabrione, F.; Di Stasio, D.; Silvestre Rangil, J.; Carinci, F. The effectiveness of laser-assisted surgical excision of leukoplakias and hyperkeratosis of oral mucosa: A case series in a group of patients. Int. J. Environ. Res. Public Health 2019, 16, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, S.; Shah, J.S.; Parikh, S.; Limbdiwala, P.; Goel, S. Clinical correlative study on early detection of oral cancer and precancerous lesions by modified oral brush biopsy and cytology followed by histopathology. J. Cancer Res. Ther. 2014, 10, 232–238. [Google Scholar] [CrossRef]
- Hesse, J.; Schmalfuss, A.; Kvaal, S.I. Photodynamic therapy of oral lichen planus. Photochem. Photobiol. Sci. 2020, 19, 1271–1279. [Google Scholar] [CrossRef] [PubMed]
- Sulewska, M.; Duraj, E.; Sobaniec, S.; Graczyk, A.; Milewski, R.; Wroblewska, M.; Pietruski, J.; Pietruska, M. A clinical evaluation of efficacy of photodynamic therapy in treatment of reticular oral lichen planus: A case series. Photodiagnosis Photodyn. Ther. 2019, 25, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Di Stasio, D.; Romano, A.; Gentile, C.; Maio, C.; Lucchese, A.; Serpico, R.; Paparella, R.; Minervini, G.; Candotto, V.; Laino, L. Systemic and topical photodynamic therapy (PDT) on oral mucosa lesions: An overview. J. Biol. Regul. Homeost. Agents 2018, 32, 123–126. [Google Scholar]
- Roomaney, I.A.; Holmes, H.K.; Engel, M.M. Treatment of oral fungal infections using photodynamic therapy: Systematic review and meta-analysis. Clin. Exp. Dent. Res. 2021, 3, 354–364. [Google Scholar] [CrossRef] [PubMed]
- Mylona, V.; Anagnostaki, E.; Parker, S.; Cronshaw, M.; Lynch, E.; Grootveld, M. Laser-assisted aPDT protocols in randomized controlled clinical trials in dentistry: A systematic review. Dent. J. 2020, 8, 107. [Google Scholar] [CrossRef] [PubMed]
- Saba, N.F.; Haigentz, M., Jr.; Vermorken, J.B.; Strojan, P.; Bossi, P.; Rinaldo, A.; Takes, R.P.; Ferlito, A. Prevention of head and neck squamous cell carcinoma: Removing the chemo from chemoprevention. Oral Oncol. 2015, 51, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, W.B.; Taylor, T.H.; Kennedy, A.R.; Melrose, R.J.; Messadi, D.V.; Gu, M.; Le, A.D.; Perloff, M.; Civantos, F.; Goodwin, W.J.; et al. Bowman birk inhibitor concentrate and oral leukoplakia: A randomized phase IIb trial. Cancer Prev. Res. 2013, 6, 410–418. [Google Scholar] [CrossRef] [Green Version]
- Johnson, S.D.; Young, M.R. Indomethacin treatment of mice with premalignant oral lesions sustains cytokine production and slows progression to cancer. Front. Immunol. 2016, 7, 379. [Google Scholar] [CrossRef] [Green Version]
- Rudin, C.M.; Cohen, E.E.; Papadimitrakopoulou, V.A.; Silverman, S., Jr.; Recant, W.; El-Naggar, A.K.; Stenson, K.; Lippman, S.M.; Hong, W.K.; Vokes, E.E. An attenuated adenovirus, ONYX-015, as mouthwash therapy for premalignant oral dysplasia. J. Clin. Oncol. 2003, 21, 4546–4552. [Google Scholar] [CrossRef] [Green Version]
- Ferris, R.L.; Blumenschein, G., Jr.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab for recurrent squamous-cell carcinoma of the head and neck. N. Engl. J. Med. 2016, 375, 1856–1867. [Google Scholar] [CrossRef]
- Cohen, E.E.W.; Soulieres, D.; Le Tourneau, C.; Dinis, J.; Licitra, L.; Ahn, M.J.; Soria, A.; Machiels, J.P.; Mach, N.; Mehra, R.; et al. Pembrolizumab versus methotrexate, docetaxel, or cetuximab for recurrent or metastatic head-and-neck squamous cell carcinoma (KEYNOTE-040): A randomised, open-label, phase 3 study. Lancet 2019, 393, 156–167. [Google Scholar] [CrossRef]
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulieres, D.; Tahara, M.; de Castro, G., Jr.; Psyrri, A.; Baste, N.; Neupane, P.; Bratland, A.; et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomised, open-label, phase 3 study. Lancet 2019, 394, 1915–1928. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| OPMD Entity | Common Oral Sites | Clinical Appearance | Histopathology | Prevalence | Affected Population | Malignant Potential |
|---|---|---|---|---|---|---|
| Leukoplakia | Any mucosal site | Two distinct appearances may be seen as dysplastic or non-dysplastic leukoplakia | 0.02% | Men >40 years | ||
| Homogenous type | White, flat with clearly, evident borders | Low | ||||
| Nonhomogeneous type (erythroleukoplakia) | White/red, verrucous/exophytic, or nodular presentation | High | ||||
| Proliferative verrucous leukoplakia | Gingiva, buccal mucosa, alveolar ridges, tongue | Asymptomatic, nonhomogenous white plaque often with a verrucous, keratotic surface. Multifocal presentation | Ranging from single hyperkeratosis to verrucous hyperplasia and varying degrees of dysplasia | <1% | Women >60 years | High |
| Erythroplakia | Buccal mucosa, palate, ventral tongue, floor of the mouth | Asymptomatic, erythematous oral mucosal lesion with a smooth or velvety in appearance | Epithelium is nonkeratinized, thin, and atrophic, allowing for visualization of underlying microvasculature; squamous hyperplasia may be seen without concomitant dysplasia (benign), varying degrees of dysplasia, or carcinoma in situ | 0.02% to 0.83% | Adults >45 years | Very high |
| Lichen planus | Buccal mucosa, followed by the gingiva (desquamative) and the tongue | Variable forms: reticular, papular, plaque, erythematous or atrophic, erosive, or bullous forms; a combination of characteristics of different subtypes may coexist | Band-like lymphocytic infiltration and liquefaction degeneration of the basal cell layer; other features include hyperkeratosis, the presence of civatte bodies, and hydropic degeneration of basal cells | 0.5% to 2.2% | Women between 30 and 60 years | Low |
| Oral submucous fubrosis | Any mucosal site | Initial phase: burning sensation and/or intolerance to spicy food. It gradually to juxtaepitelial fibrosis of the oral cavity | Mucosal changes such as atrophic changes, pigment incontinence, ulceration with granulation tissue, hyperplastic changes, dysplasia, and carcinoma. Submucosal changes such as fibrosis, diffuse chronic inflammatory infiltrate, atrophy of minor salivary glands, skeletal muscle atrophy, bandlike infiltrate, edema and congestion, and vesicle formation | 0.2–2.3% in males and 1.2–4.6% in females | Asians population with age range from 11 to 60 years | High |
| Architectural Changes | Cytological Changes |
|---|---|
| Irregular stratification | Abnormal variation in nuclear size |
| Loss of polarity of basal cells | Abnormal variation in nuclear shape |
| Bulbous rete ridges | Abnormal variation in cell size |
| Increased number of mitotic figures | Abnormal variation in cell shape |
| Premature keratinization in a single cell | Increased nuclear/cytoplasm ratio |
| Squamous eddies within rete ridges | Atypical mitotic figures |
| Loss of intracellular cohesion | Increased number and size of nucleoli |
| Hyperchromasia |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lorini, L.; Bescós Atín, C.; Thavaraj, S.; Müller-Richter, U.; Alberola Ferranti, M.; Pamias Romero, J.; Sáez Barba, M.; de Pablo García-Cuenca, A.; Braña García, I.; Bossi, P.; et al. Overview of Oral Potentially Malignant Disorders: From Risk Factors to Specific Therapies. Cancers 2021, 13, 3696. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13153696
Lorini L, Bescós Atín C, Thavaraj S, Müller-Richter U, Alberola Ferranti M, Pamias Romero J, Sáez Barba M, de Pablo García-Cuenca A, Braña García I, Bossi P, et al. Overview of Oral Potentially Malignant Disorders: From Risk Factors to Specific Therapies. Cancers. 2021; 13(15):3696. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13153696
Chicago/Turabian StyleLorini, Luigi, Coro Bescós Atín, Selvam Thavaraj, Urs Müller-Richter, Margarita Alberola Ferranti, Jorge Pamias Romero, Manel Sáez Barba, Alba de Pablo García-Cuenca, Irene Braña García, Paolo Bossi, and et al. 2021. "Overview of Oral Potentially Malignant Disorders: From Risk Factors to Specific Therapies" Cancers 13, no. 15: 3696. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13153696