
Machine Learning Models to Predict Survival Outcomes According to the Surgical Approach of Primary Radical Hysterectomy in Patients with Early Cervical Cancer

 , , ,
, , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
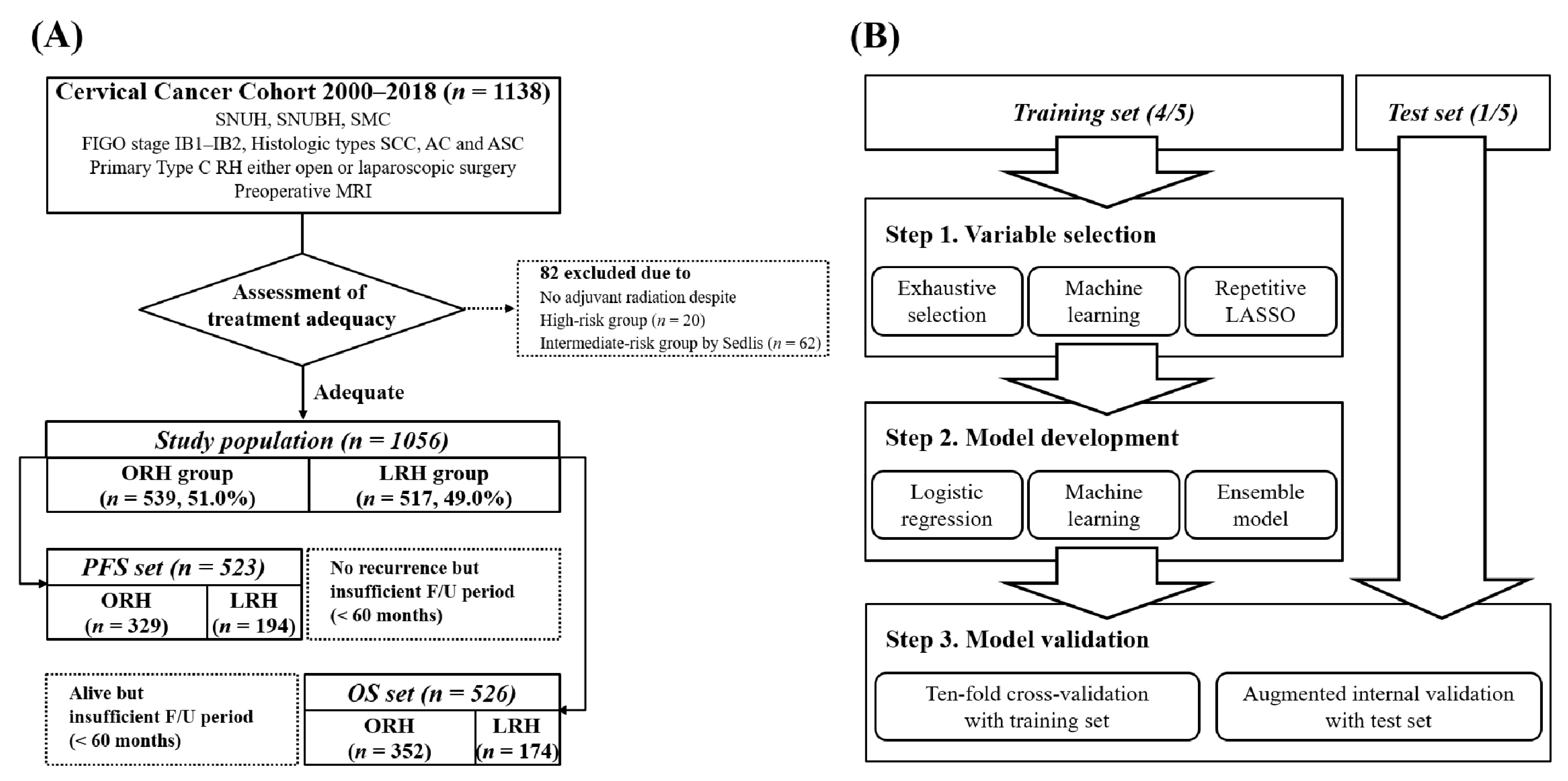
2.1. Study Population
2.2. Data Collection
2.3. Dataset Preprocessing
2.4. Variable Selection
2.5. Model Development and Validation
3. Results
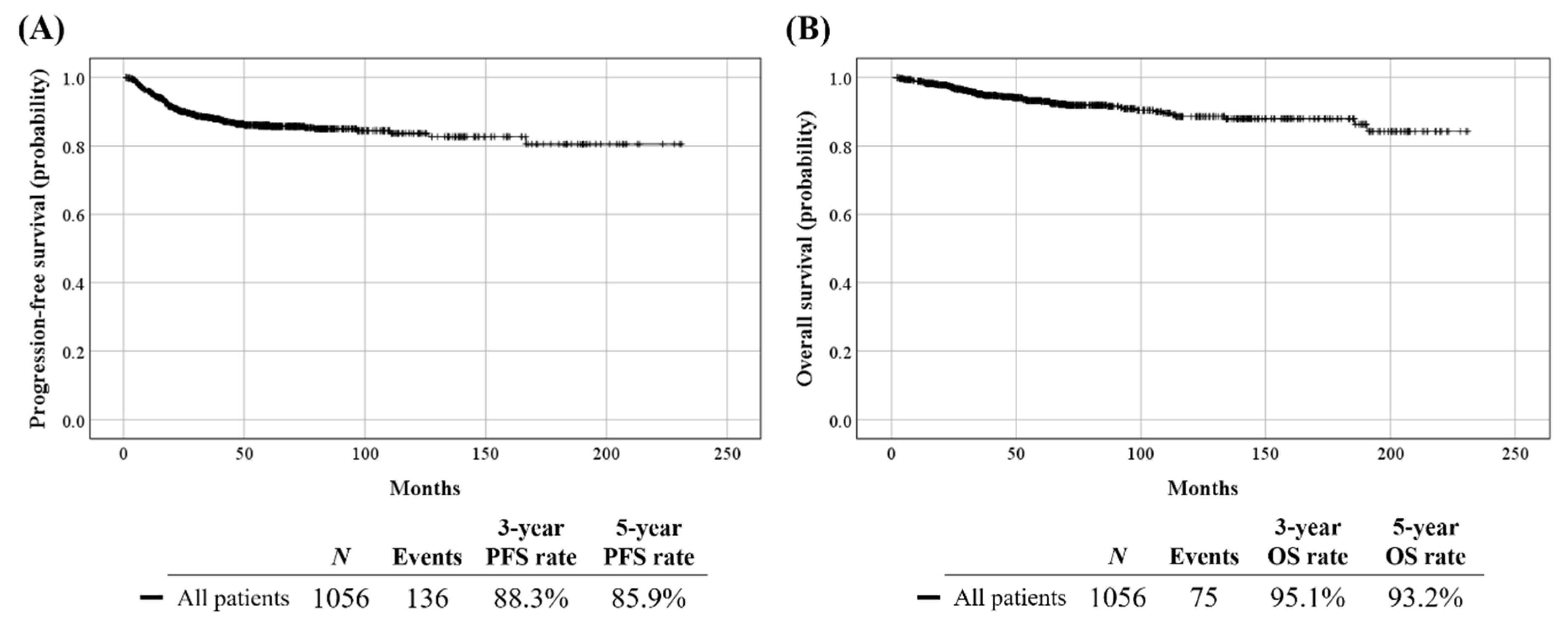
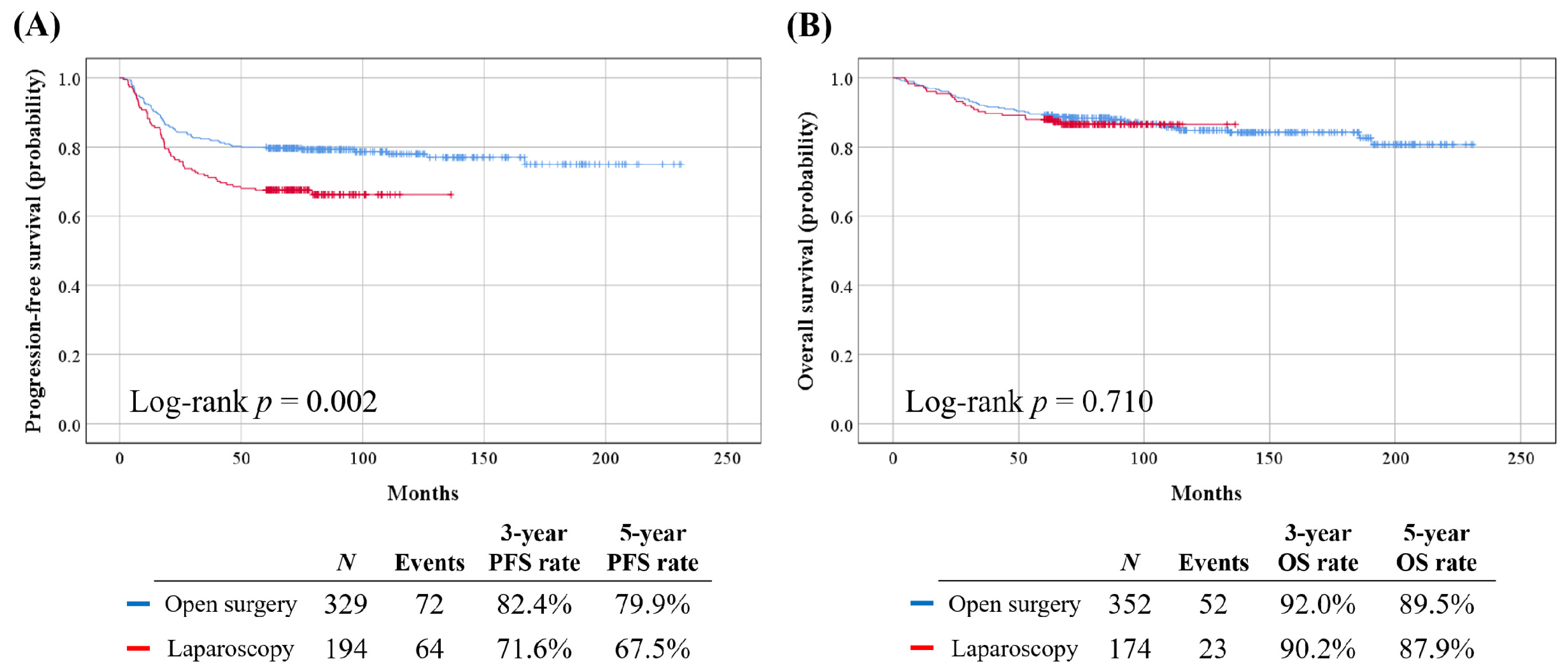
3.1. Patient Characteristics
3.2. Variable Selection
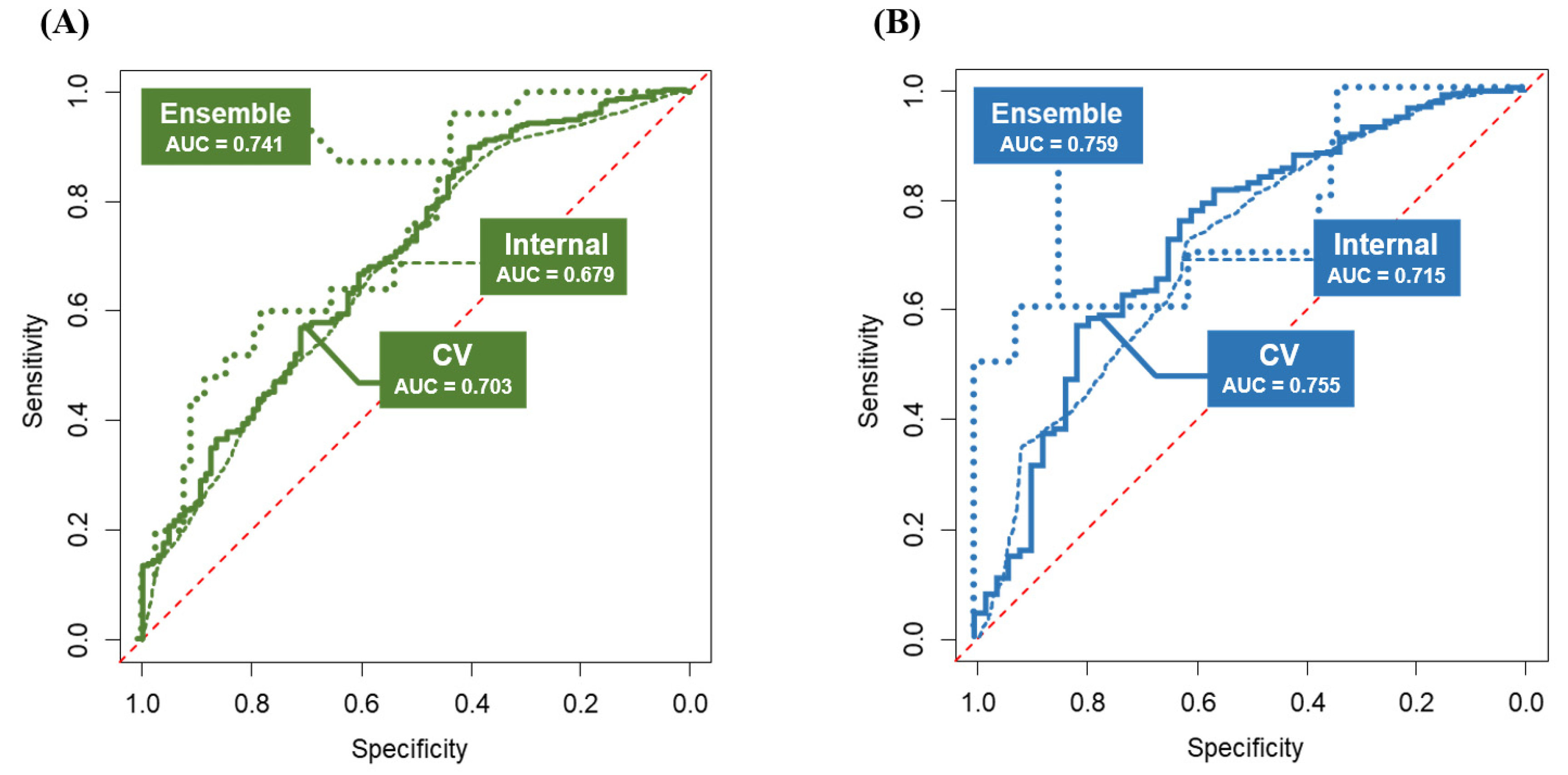
3.3. Model Development and Validation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Lim, M.C.; Won, Y.J.; Ko, M.J.; Kim, M.; Shim, S.H.; Suh, D.H.; Kim, J.W. Incidence of cervical, endometrial, and ovarian cancer in Korea during 1999–2015. J. Gynecol. Oncol. 2019, 30, e38. [Google Scholar] [CrossRef]
- Jung, K.W.; Won, Y.J.; Hong, S.; Kong, H.J.; Im, J.S.; Seo, H.G. Prediction of Cancer Incidence and Mortality in Korea, 2021. Cancer Res. Treat. 2021, 53, 316–322. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef]
- Cibula, D.; Pötter, R.; Planchamp, F.; Avall-Lundqvist, E.; Fischerova, D.; Haie Meder, C.; Köhler, C.; Landoni, F.; Lax, S.; Lindegaard, J.C.; et al. The European Society of Gynaecological Oncology/European Society for Radiotherapy and Oncology/European Society of Pathology Guidelines for the Management of Patients With Cervical Cancer. Int. J. Gynecol. Cancer 2018, 28, 641–655. [Google Scholar] [CrossRef] [PubMed]
- Lim, M.C.; Lee, M.; Shim, S.H.; Nam, E.J.; Lee, J.Y.; Kim, H.J.; Lee, Y.Y.; Lee, K.B.; Park, J.Y.; Kim, Y.H.; et al. Practice guidelines for management of cervical cancer in Korea: A Korean Society of Gynecologic Oncology Consensus Statement. J. Gynecol. Oncol. 2017, 28, e22. [Google Scholar] [CrossRef] [PubMed]
- Nam, J.H.; Park, J.Y.; Kim, D.Y.; Kim, J.H.; Kim, Y.M.; Kim, Y.T. Laparoscopic versus open radical hysterectomy in early-stage cervical cancer: Long-term survival outcomes in a matched cohort study. Ann. Oncol. 2012, 23, 903–911. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Chu, H.J.; Shang, C.L.; Gong, X.; Liu, T.Y.; Zhao, Y.H.; Huang, J.M.; Yao, S.Z. Long-Term Oncological Outcomes After Laparoscopic Versus Abdominal Radical Hysterectomy in Stage IA2 to IIA2 Cervical Cancer: A Matched Cohort Study. Int. J. Gynecol. Cancer 2016, 26, 1264–1273. [Google Scholar] [CrossRef]
- Ramirez, P.T.; Frumovitz, M.; Pareja, R.; Lopez, A.; Vieira, M.; Ribeiro, R.; Buda, A.; Yan, X.; Shuzhong, Y.; Chetty, N.; et al. Minimally Invasive versus Abdominal Radical Hysterectomy for Cervical Cancer. N. Engl. J. Med. 2018, 379, 1895–1904. [Google Scholar] [CrossRef]
- Melamed, A.; Margul, D.J.; Chen, L.; Keating, N.L.; Del Carmen, M.G.; Yang, J.; Seagle, B.L.; Alexander, A.; Barber, E.L.; Rice, L.W.; et al. Survival after Minimally Invasive Radical Hysterectomy for Early-Stage Cervical Cancer. N. Engl. J. Med. 2018, 379, 1905–1914. [Google Scholar] [CrossRef]
- Chiva, L.; Zanagnolo, V.; Querleu, D.; Martin-Calvo, N.; Arévalo-Serrano, J.; Căpîlna, M.E.; Fagotti, A.; Kucukmetin, A.; Mom, C.; Chakalova, G.; et al. SUCCOR study: An international European cohort observational study comparing minimally invasive surgery versus open abdominal radical hysterectomy in patients with stage IB1 cervical cancer. Int. J. Gynecol. Cancer 2020, 30, 1269–1277. [Google Scholar] [CrossRef] [PubMed]
- Doo, D.W.; Kirkland, C.T.; Griswold, L.H.; McGwin, G.; Huh, W.K.; Leath, C.A., 3rd; Kim, K.H. Comparative outcomes between robotic and abdominal radical hysterectomy for IB1 cervical cancer: Results from a single high volume institution. Gynecol. Oncol. 2019, 153, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.I.; Cho, J.H.; Seol, A.; Kim, Y.I.; Lee, M.; Kim, H.S.; Chung, H.H.; Kim, J.W.; Park, N.H.; Song, Y.S. Comparison of survival outcomes between minimally invasive surgery and conventional open surgery for radical hysterectomy as primary treatment in patients with stage IB1-IIA2 cervical cancer. Gynecol. Oncol. 2019, 153, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.I.; Lee, M.; Lee, S.; Suh, D.H.; Kim, H.S.; Kim, K.; Chung, H.H.; No, J.H.; Kim, J.W.; Park, N.H.; et al. Impact of laparoscopic radical hysterectomy on survival outcome in patients with FIGO stage IB cervical cancer: A matching study of two institutional hospitals in Korea. Gynecol. Oncol. 2019, 155, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Chen, L.; Ni, Y.; Liu, J.; Li, D.; Guo, J.; Liu, Z.; Jin, S.; Xu, Y.; Li, Z.; et al. Comparison between laparoscopic and abdominal radical hysterectomy for stage IB1 and tumor size <2 cm cervical cancer with visible or invisible tumors: A multicentre retrospective study. J. Gynecol. Oncol. 2021, 32, e17. [Google Scholar] [CrossRef]
- Uppal, S.; Gehrig, P.A.; Peng, K.; Bixel, K.L.; Matsuo, K.; Vetter, M.H.; Davidson, B.A.; Cisa, M.P.; Lees, B.F.; Brunette, L.L.; et al. Recurrence Rates in Patients With Cervical Cancer Treated With Abdominal Versus Minimally Invasive Radical Hysterectomy: A Multi-Institutional Retrospective Review Study. J. Clin. Oncol. 2020, 38, 1030–1040. [Google Scholar] [CrossRef]
- Paik, E.S.; Lim, M.C.; Kim, M.H.; Kim, Y.H.; Song, E.S.; Seong, S.J.; Suh, D.H.; Lee, J.M.; Lee, C.; Choi, C.H. Comparison of laparoscopic and abdominal radical hysterectomy in early stage cervical cancer patients without adjuvant treatment: Ancillary analysis of a Korean Gynecologic Oncology Group Study (KGOG 1028). Gynecol. Oncol. 2019, 154, 547–553. [Google Scholar] [CrossRef]
- Kim, M.; Kong, T.W.; Kim, S.; Kim, S.C.; Kim, Y.B.; Kim, J.W.; Park, J.Y.; Suh, D.H.; Shim, S.H.; Lee, K.H.; et al. Minimally invasive surgery for radical hysterectomy in women with cervical cancer: Korean Society of Gynecologic Oncology, Korean Society of Obstetrics and Gynecology, and Korean Society of Gynecologic Endoscopy and Minimally Invasive Surgery position statement. J. Gynecol. Oncol. 2019, 30, e104. [Google Scholar] [CrossRef]
- Huang, S.; Yang, J.; Fong, S.; Zhao, Q. Artificial intelligence in cancer diagnosis and prognosis: Opportunities and challenges. Cancer Lett. 2020, 471, 61–71. [Google Scholar] [CrossRef]
- Christodoulou, E.; Ma, J.; Collins, G.S.; Steyerberg, E.W.; Verbakel, J.Y.; Van Calster, B. A systematic review shows no performance benefit of machine learning over logistic regression for clinical prediction models. J. Clin. Epidemiol. 2019, 110, 12–22. [Google Scholar] [CrossRef]
- Lynam, A.L.; Dennis, J.M.; Owen, K.R.; Oram, R.A.; Jones, A.G.; Shields, B.M.; Ferrat, L.A. Logistic regression has similar performance to optimised machine learning algorithms in a clinical setting: Application to the discrimination between type 1 and type 2 diabetes in young adults. Diagn. Progn. Res. 2020, 4, 6. [Google Scholar] [CrossRef] [PubMed]
- Querleu, D.; Morrow, C.P. Classification of radical hysterectomy. Lancet Oncol. 2008, 9, 297–303. [Google Scholar] [CrossRef]
- Sedlis, A.; Bundy, B.N.; Rotman, M.Z.; Lentz, S.S.; Muderspach, L.I.; Zaino, R.J. A randomized trial of pelvic radiation therapy versus no further therapy in selected patients with stage IB carcinoma of the cervix after radical hysterectomy and pelvic lymphadenectomy: A Gynecologic Oncology Group Study. Gynecol. Oncol. 1999, 73, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, D.G.; Snyder, B.; Coakley, F.; Reinhold, C.; Thomas, G.; Amendola, M.; Schwartz, L.H.; Woodward, P.; Pannu, H.; Hricak, H. Early invasive cervical cancer: Tumor delineation by magnetic resonance imaging, computed tomography, and clinical examination, verified by pathologic results, in the ACRIN 6651/GOG 183 Intergroup Study. J. Clin. Oncol. 2006, 24, 5687–5694. [Google Scholar] [CrossRef]
- Hricak, H.; Gatsonis, C.; Coakley, F.V.; Snyder, B.; Reinhold, C.; Schwartz, L.H.; Woodward, P.J.; Pannu, H.K.; Amendola, M.; Mitchell, D.G. Early invasive cervical cancer: CT and MR imaging in preoperative evaluation—ACRIN/GOG comparative study of diagnostic performance and interobserver variability. Radiology 2007, 245, 491–498. [Google Scholar] [CrossRef]
- Dappa, E.; Elger, T.; Hasenburg, A.; Düber, C.; Battista, M.J.; Hötker, A.M. The value of advanced MRI techniques in the assessment of cervical cancer: A review. Insights Imaging 2017, 8, 471–481. [Google Scholar] [CrossRef]
- Sala, E.; Rockall, A.G.; Freeman, S.J.; Mitchell, D.G.; Reinhold, C. The added role of MR imaging in treatment stratification of patients with gynecologic malignancies: What the radiologist needs to know. Radiology 2013, 266, 717–740. [Google Scholar] [CrossRef] [PubMed]
- Woo, S.; Atun, R.; Ward, Z.J.; Scott, A.M.; Hricak, H.; Vargas, H.A. Diagnostic performance of conventional and advanced imaging modalities for assessing newly diagnosed cervical cancer: Systematic review and meta-analysis. Eur. Radiol. 2020, 30, 5560–5577. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Nitecki, R.; Ramirez, P.T.; Frumovitz, M.; Krause, K.J.; Tergas, A.I.; Wright, J.D.; Rauh-Hain, J.A.; Melamed, A. Survival After Minimally Invasive vs Open Radical Hysterectomy for Early-Stage Cervical Cancer: A Systematic Review and Meta-analysis. JAMA Oncol. 2020, 6, 1019–1027. [Google Scholar] [CrossRef]
- Bhatla, N.; Berek, J.S.; Cuello Fredes, M.; Denny, L.A.; Grenman, S.; Karunaratne, K.; Kehoe, S.T.; Konishi, I.; Olawaiye, A.B.; Prat, J.; et al. Revised FIGO staging for carcinoma of the cervix uteri. Int. J. Gynaecol. Obstet. 2019, 145, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Cibula, D.; Dostalek, L.; Hillemanns, P.; Scambia, G.; Jarkovsky, J.; Persson, J.; Raspagliesi, F.; Novak, Z.; Jaeger, A.; Capilna, M.E.; et al. Completion of radical hysterectomy does not improve survival of patients with cervical cancer and intraoperatively detected lymph node involvement: ABRAX international retrospective cohort study. Eur. J. Cancer 2021, 143, 88–100. [Google Scholar] [CrossRef] [PubMed]
- Cruz, J.A.; Wishart, D.S. Applications of machine learning in cancer prediction and prognosis. Cancer Inform. 2007, 2, 59–77. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Schwarz, J.K.; Lewis, J.S., Jr.; Huettner, P.C.; Rader, J.S.; Deasy, J.O.; Grigsby, P.W.; Wang, X. A microRNA expression signature for cervical cancer prognosis. Cancer Res. 2010, 70, 1441–1448. [Google Scholar] [CrossRef] [Green Version]
- Tewari, K.S. Minimally Invasive Surgery for Early-Stage Cervical Carcinoma: Interpreting the Laparoscopic Approach to Cervical Cancer Trial Results. J. Clin. Oncol. 2019, 37, 3075–3080. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | PFS Set (n = 523, %) | OS Set (n = 526, %) |
|---|---|---|
| Age, years | 47.6 (24.6–78.1) | 48.0 (24.6–78.1) |
| Surgical approach | ||
| Open surgery | 329 (62.9) | 352 (66.9) |
| Laparoscopy | 194 (37.1) | 174 (33.1) |
| 2009 FIGO stage | ||
| IB1 | 442 (84.5) | 452 (85.9) |
| IB2 | 81 (15.5) | 74 (14.1) |
| Histologic type | ||
| Squamous cell carcinoma | 377 (72.1) | 393 (74.7) |
| Adenocarcinoma | 116 (22.2) | 105 (20.0) |
| Adenosquamous carcinoma | 30 (5.7) | 28 (5.3) |
| Preoperative conization | ||
| No | 364 (69.6) | 355 (67.5) |
| Yes | 159 (30.4) | 171 (32.5) |
| Preoperative tumor markers | ||
| CEA, ng/mL | 1.3 (0.1–210.0) a | 1.3 (0.1–210.0) d |
| SCC, ng/mL | 1.0 (0.1–118.7) b | 1.0 (0.1–118.7) e |
| CA-125, IU/mL | 12.1 (0.9–271.5) c | 12.0 (0.9–273.0) f |
| Cervical mass size by MRI, mm | 22.0 (0–82.0) | 20.5 (0–82.0) |
| No residual tumor | 134 (25.6) | 148 (28.1) |
| <20 | 83 (15.9) | 86 (16.3) |
| ≥20 and <40 | 200 (38.2) | 195 (37.1) |
| ≥40 | 106 (20.3) | 97 (18.4) |
| PM invasion on imaging * | ||
| No | 438 (83.7) | 449 (85.4) |
| Suspicious | 85 (16.3) | 77 (14.6) |
| LN metastasis on imaging † | ||
| No | 387 (74.0) | 393 (74.7) |
| Suspicious | 136 (26.0) | 133 (25.3) |
| Pelvic lymphadenectomy | ||
| No | 1 (0.2) § | 1 (0.2) § |
| Yes | 522 (99.8) | 525 (99.8) |
| Para-aortic lymphadenectomy | ||
| No | 405 (77.4) | 414 (78.7) |
| Sampling/Dissection | 118 (22.6) | 112 (21.3) |
| Pathologic cervical mass size, mm ‡ | 28.0 (0–110.0) | 26.0 (0–110.0) |
| No residual tumor | 64 (12.2) | 73 (13.9) |
| <20 | 114 (21.8) | 120 (22.8) |
| ≥20 and <40 | 206 (39.4) | 200 (38.0) |
| ≥40 | 139 (26.6) | 133 (25.3) |
| Pathologic risk factors | ||
| PM invasion | 89 (17.0) | 83 (15.8) |
| LN metastasis | 137 (26.2) | 123 (23.4) |
| Resection margin involvement | 16 (3.1) | 12 (2.3) |
| LVSI | 227 (43.4) | 209 (39.7) |
| Invasion depth ≥ 1/2 | 300 (57.4) | 289 (54.9) |
| Adjuvant treatment | ||
| No | 229 (43.8) | 247 (47.0) |
| Radiation only | 86 (16.4) | 83 (15.8) |
| CCRT | 208 (39.8) | 196 (37.3) |
| Variables | PFS Set (n = 523) | OS Set (n = 526) | ||
|---|---|---|---|---|
| OR | 90% CI | OR | 90% CI | |
| Surgical approach: Laparosocpy vs. Open | 0.856 | 0.805–0.911 | ||
| CEA, ng/mL | 0.994 | 0.991–0.997 | 0.997 | 0.995–0.999 |
| SCC, ng/mL | 0.995 | 0.992–0.997 | 0.995 | 0.993–0.997 |
| Preoperative conization: Yes vs. No | 1.091 | 1.022–1.166 | ||
| 2009 FIGO stage, IB2 vs. IB1 | 0.908 | 0.832–0.991 | ||
| LN metastasis on imaging *: Suspicious vs. No | 0.924 | 0.862–0.991 | 0.919 | 0.872–0.969 |
| CA-125, IU/mL | 0.999 | 0.998–1.000 | ||
| Cervical mass size by MRI: ≥20 mm vs. <20 mm | 0.942 | 0.899–0.986 | ||
| Histologic type: Squamous vs. Non-squamous | 1.073 | 1.021–1.127 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.I.; Lee, S.; Choi, C.H.; Lee, M.; Suh, D.H.; Kim, H.S.; Kim, K.; Chung, H.H.; No, J.H.; Kim, J.-W.; et al. Machine Learning Models to Predict Survival Outcomes According to the Surgical Approach of Primary Radical Hysterectomy in Patients with Early Cervical Cancer. Cancers 2021, 13, 3709. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13153709
Kim SI, Lee S, Choi CH, Lee M, Suh DH, Kim HS, Kim K, Chung HH, No JH, Kim J-W, et al. Machine Learning Models to Predict Survival Outcomes According to the Surgical Approach of Primary Radical Hysterectomy in Patients with Early Cervical Cancer. Cancers. 2021; 13(15):3709. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13153709
Chicago/Turabian StyleKim, Se Ik, Sungyoung Lee, Chel Hun Choi, Maria Lee, Dong Hoon Suh, Hee Seung Kim, Kidong Kim, Hyun Hoon Chung, Jae Hong No, Jae-Weon Kim, and et al. 2021. "Machine Learning Models to Predict Survival Outcomes According to the Surgical Approach of Primary Radical Hysterectomy in Patients with Early Cervical Cancer" Cancers 13, no. 15: 3709. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13153709