
Pathologic Characteristics of Pregnancy-Related Meningiomas

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Study Design
2.3. Study Population
2.4. Exposure
2.5. Outcome
2.6. Pathology
2.7. Immunohistochemistry
2.8. Assessment of Tumor Labeling Index
2.9. Statistical Analysis
2.10. Ethics Statement
3. Results
3.1. Characteristics
3.2. Pathology
3.2.1. WHO Grades (I–III), Ki-67 Labeling Index and Histopathological Subtypes
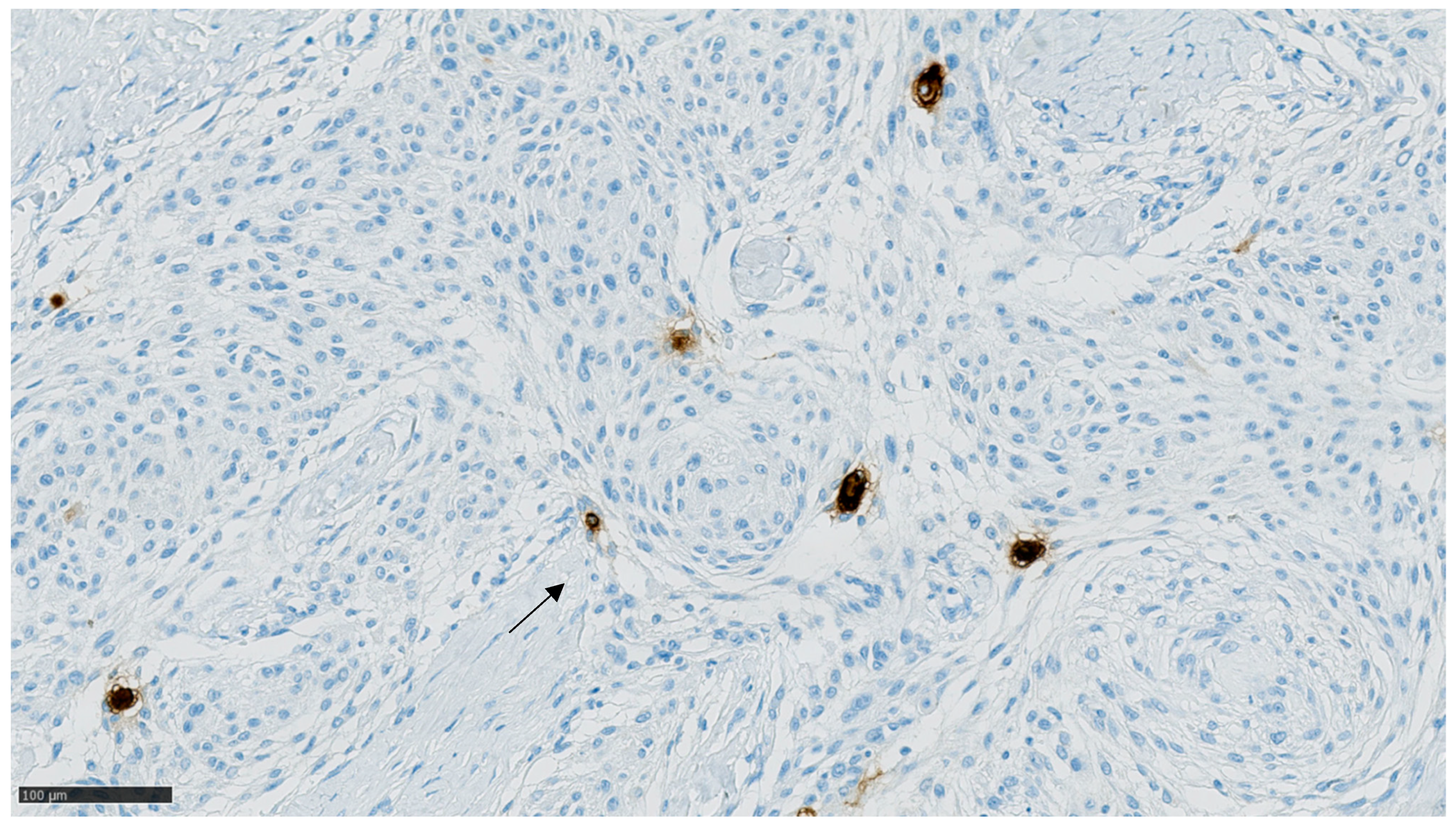
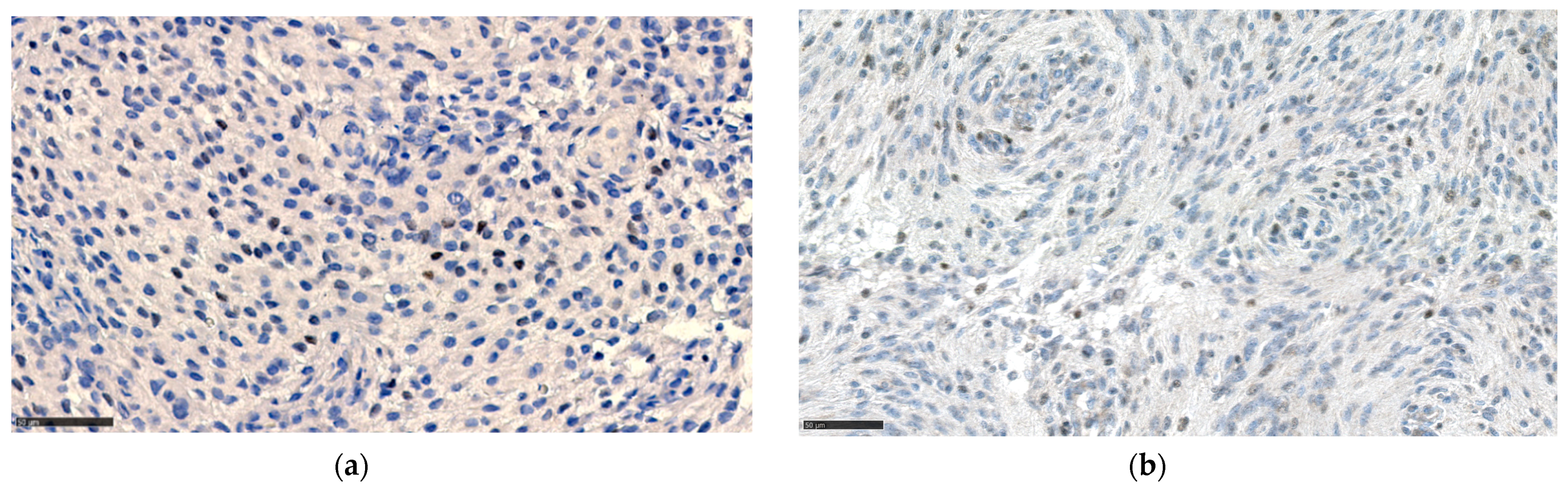
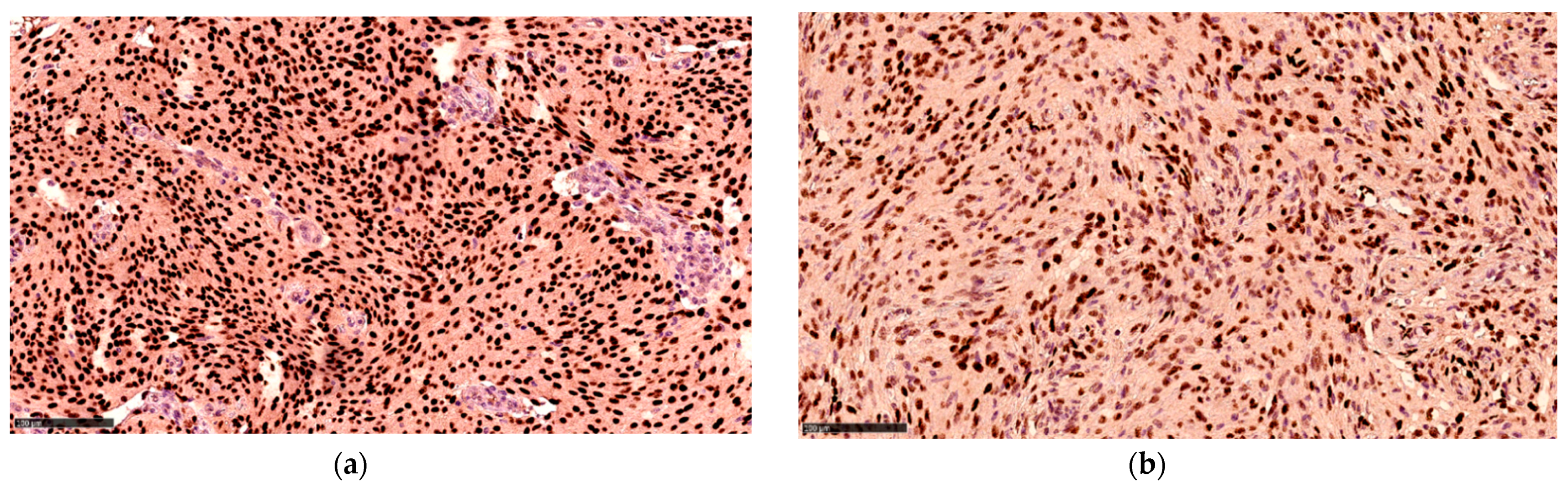
3.2.2. Hormone Receptor Status
3.3. Meningioma Location
4. Discussion
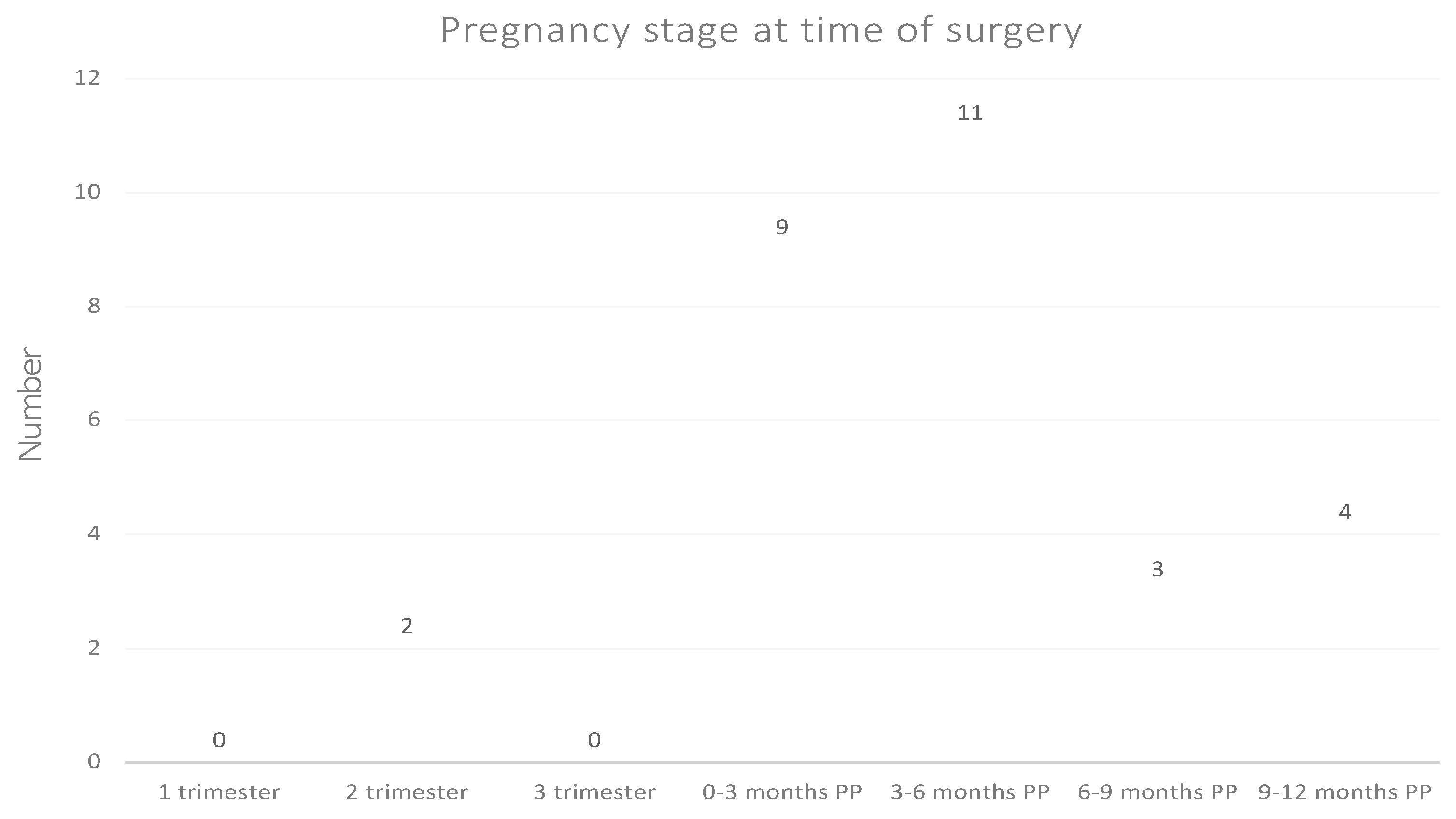
4.1. Pregnancy Stage and Replication History
4.2. Pathology and Ki-67 Labeling Index
4.3. Hormone Receptor Status
4.4. Meningioma Location
4.5. Limitations and Strengths of Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Christine, M.; Marco, H.; Karl, R.; Michele, R.; Milena, S.; Elena, M.; Charles, V. Meningioma. Crit. Rev. Oncol. Hematol. 2008, 67, 153–171. [Google Scholar] [CrossRef]
- Wiemels, J.; Wrensch, M.; Claus, E.B. Epidemiology and etiology of meningioma. J. Neuro-Oncol. 2010, 99, 307–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Claus, E.B.; Black, P.M.; Bondy, M.L.; Calvocoressi, L.; Schildkraut, J.M.; Wiemels, J.L.; Wrensch, M. Exogenous hormone use and meningioma risk. Cancer 2007, 110, 471–476. [Google Scholar] [CrossRef]
- Preston, D.L.; Ron, E.; Yonehara, S.; Kobuke, T.; Fujii, H.; Kishikawa, M.; Tokunaga, M.; Tokuoka, S.; Mabuchi, K. Tumors of the nervous system and pituitary gland associated with atomic bomb radiation exposure. J. Natl. Cancer Inst. 2002, 94, 1555–1563. [Google Scholar] [CrossRef] [Green Version]
- Ron, E.; Modan, B.; Boice, J.D.; Alfandary, E.; Stovall, M.; Chetrit, A.; Katz, L. Tumors of the Brain and Nervous System after Radiotherapy in Childhood. N. Engl. J. Med. 1988, 319, 1033–1039. [Google Scholar] [CrossRef]
- Anic, G.M.; Madden, M.H.; Nabors, L.B.; Olson, J.J.; LaRocca, R.V.; Thompson, Z.J.; Pamnani, S.J.; Forsyth, P.A.; Thompson, R.C.; Egan, K.M. Reproductive factors and risk of primary brain tumors in women. J. Neuro-Oncol. 2014, 118, 297–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Claus, E.B.; Calvocoressi, L.; Bondy, M.L.; Wrensch, M.; Wiemels, J.L.; Schildkraut, J.M. Exogenous hormone use, reproductive factors, and risk of intracraniel meningioma in females. J. Neurosurg. 2014, 118, 649–656. [Google Scholar] [CrossRef] [PubMed]
- Custer, B.; Longstreth, W.T.; Phillips, L.E.; Koepsell, T.D.; Van Belle, G. Hormonal exposures and the risk of intracranial meningioma in women: A population-based case-control study. BMC Cancer 2006, 6, 152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatch, E.E.; Linet, M.S.; Zhang, J.; Fine, H.A.; Shapiro, W.R.; Selker, R.G.; Black, P.M.; Inskip, P.D. Reproductive and hormonal factors and risk of brain tumors in adult females. Int. J. Cancer 2004, 114, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Korhonen, K.; Raitanen, J.; Isola, J.; Haapasalo, H.; Salminen, T.; Auvinen, A. Exogenous sex hormone use and risk of meningioma: A population-based case–control study in Finland. Cancer Causes Control 2010, 21, 2149–2156. [Google Scholar] [CrossRef]
- Lee, E.; Grutsch, J.; Persky, V.; Glick, R.; Mendes, J.; Davis, F. Association of meningioma with reproductive factors. Int. J. Cancer 2006, 119, 1152–1157. [Google Scholar] [CrossRef] [PubMed]
- Preston-Martin, S.; Monroe, K.; Lee, P.J.; Bernstein, L.; Kelsey, J.; Henderson, S.; Forrester, D.; Henderson, B. Spinal meningiomas in women in Los Angeles County: Investigation of an etiological hypothesis. Cancer Epidemiol. Biomark. Prev. 1995, 4, 333–339. [Google Scholar]
- Wigertz, A.; Lönn, S.; Hall, P.; Auvinen, A.; Christensen, H.C.; Johansen, C.; Klaeboe, L.; Salminen, T.; Schoemaker, M.; Swerdlow, A.; et al. Reproductive Factors and Risk of Meningioma and Glioma. Cancer Epidemiol. Biomarkers Prev. 2008, 17, 2663–2670. [Google Scholar] [CrossRef] [Green Version]
- Lambe, M.; Coogan, P.; Baron, J. Reproductive factors and the risk of brain tumors: A population-based study in Sweden. Int. J. Cancer 1997, 72, 389–393. [Google Scholar] [CrossRef]
- Benson, V.S.; Pirie, K.; Green, J.; Bull, D.; Casabonne, D.; Reeves, G.K.; Beral, V.; for the Million Women Study Collaborators. Hormone replacement therapy and incidence of central nervous system tumours in the Million Women Study. Int. J. Cancer 2010, 127, 1692–1698. [Google Scholar] [CrossRef]
- Wigertz, A.; Lönn, S.; Mathiesen, T.; Ahlbom, A.; Hall, P.; Feychting, M. Risk of Brain Tumors Associated with Exposure to Exogenous Female Sex Hormones. Am. J. Epidemiol. 2006, 164, 629–636. [Google Scholar] [CrossRef] [Green Version]
- Benson, V.S.; for the Million Women Study Collaborators; Pirie, K.; Green, J.; Casabonne, D.; Beral, V. Lifestyle factors and primary glioma and meningioma tumours in the Million Women Study cohort. Br. J. Cancer 2008, 99, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Blitshteyn, S.; Crook, J.E.; Jaeckle, K.A. Is There an Association Between Meningioma and Hormone Replacement Therapy? J. Clin. Oncol. 2008, 26, 279–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korhonen, K.; Salminen, T.; Raitanen, J.; Auvinen, A.; Isola, J.; Haapasalo, H. Female predominance in meningiomas can not be explained by differences in progesterone, estrogen, or androgen receptor expression. J. Neuro-Oncol. 2006, 80, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Bickerstaff, E.R.; Small, J.M.; Guest, I.A. The relapsing course of certain meningiomas in relation to pregnancy and menstruation. J. Neurol. Neurosurg. Psychiatry 1958, 21, 89–91. [Google Scholar] [CrossRef] [Green Version]
- Michelsen, J.J.; New, P.F. Brain tumour and pregnancy. J. Neurol. Neurosurg. Psychiatry 1969, 32, 305–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wahab, M.; Al-Azzawi, F. Meningioma and hormonal influences. Climacteric 2003, 6, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Laviv, Y.; Ohla, V.; Kasper, E.M. Unique features of pregnancy-related meningiomas: Lessons learned from 148 reported cases and theoretical implications of a prolactin modulated pathogenesis. Neurosurg. Rev. 2016, 41, 95–108. [Google Scholar] [CrossRef]
- Kanaan, I.; Jallu, A.; Kanaan, H. Management Strategy for Meningioma in Pregnancy: A Clinical Study. Semin. Neurol. 2003, 13, 197–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moscovici, S.; Fraifeld, S.; Cohen, J.E.; Dotan, S.; Elchalal, U.; Shoshan, Y.; Spektor, S. Parasellar Meningiomas in Pregnancy: Surgical Results and Visual Outcomes. World Neurosurg. 2014, 82, e503–e512. [Google Scholar] [CrossRef]
- Roelvink, N.C.A.; Kamphorst, W.; Van Alphen, H.A.M.; Rao, B.R. Pregnancy-Related Primary Brain and Spinal Tumors. Arch. Neurol. 1987, 44, 209–215. [Google Scholar] [CrossRef]
- Couce, M.E.; Aker, F.V.; Scheithauer, B.W. Chordoid Meningioma: A clinicopathologic study of 42 cases. Am. J. Surg. Pathol. 2000, 24, 899–905. [Google Scholar] [CrossRef]
- Jain, D.; Sharma, M.C.; Sarkar, C.; Suri, V.; Garg, A.; Singh, M.; Sharma, B.S.; Mahapatra, A.K. Clear cell Meningioma, an uncommon variant of meningioma: A clinicopathologic study of nine cases. J. Neuro-Oncol. 2006, 81, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Gregerson, K. ProlactinStructure, Function, and Regulation of Secretion. Knobil Neill’s Physiol. Reprod. 2006, 1, 1703–1726. [Google Scholar] [CrossRef]
- Abbassi-Ghanavati, M.; Greer, L.; Cunningham, F. A Reference Table for Clinicians. Obstet. Gynecol. 2009, 114, 1326–1331. [Google Scholar] [CrossRef]
- Boyle-Walsh, E.; Shenkin, A.; White, M.C.; Fraser, W.D. Effect of glycoprotein and protein hormones on human meningioma cell proliferation in vitro. J. Endocrinol. 1995, 145, 155–161. [Google Scholar] [CrossRef]
- Jimenez-Hakim, E.; El-Azouzi, M.; Black, P.M. The effect of prolactin and bombesin on the growth of meningioma-derived cells in monolayer culture. J. Neuro-Oncol. 1993, 16, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Muccioli, G.; Ghè, C.; Faccani, G.; Lanotte, M.; Forni, M.; Ciccarelli, E. Prolactin receptors in human meningiomas: Characterization and biological role. J. Endocrinol. 1997, 153, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Corbacho, A.M.; De La Escalera, G.M.; Clapp, C. Roles of prolactin and related members of the prolactin/growth hormone/placental lactogen family in angiogenesis. J. Endocrinol. 2002, 173, 219–238. [Google Scholar] [CrossRef] [Green Version]
- Barresi, V. Angiogenesis in meningiomas. Brain Tumor Pathol. 2011, 28, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Breves, J.P.; McCormick, S.D.; Karlstrom, R.O. Prolactin and teleost ionocytes: New insights into cellular and molecular targets of prolactin in vertebrate epithelia. Gen. Comp. Endocrinol. 2014, 203, 21–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loretz, C.A.; Bern, H.A. Prolactin and Osmoregulation in Vertebrates. An update. Neuroendocrinology 1982, 35, 292–304. [Google Scholar] [CrossRef] [PubMed]
- Abry, E.; Thomassen, I.; Salvesen, O.; Torp, S.H. The significance of Ki-67/MIB-1 labeling index in human meningiomas: A literature study. Pathol. Res. Pract. 2010, 206, 810–815. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Song, S.-Y.; Jiang, J.-B.; Wang, T.-J.; Yan, C.-X. The prognostic role of Ki-67/MIB-1 in meningioma: A systematic review with meta-analysis. Medicine 2020, 99, e18644. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, C.B. The Danish Civil Registration System. Scand. J. Public Health 2011, 39, 22–25. [Google Scholar] [CrossRef]
- Lynge, E.; Sandegaard, J.L.; Rebolj, M. The Danish National Patient Register. Scand. J. Public Health 2011, 39, 30–33. [Google Scholar] [CrossRef]
- Gjerstorff, M.L. The Danish Cancer Registry. Scand. J. Public Health 2011, 39, 42–45. [Google Scholar] [CrossRef]
- Bjerregaard, B.; Larsen, O.B. The Danish Pathology Register. Scand. J. Public Health 2011, 39, 72–74. [Google Scholar] [CrossRef] [Green Version]
- Hu, Y.; Ding, Y.; Yang, M.; Xiang, Z. Serum prolactin levels across pregnancy and the establishment of reference intervals. Clin. Chem. Lab. Med. 2017, 56, 803–807. [Google Scholar] [CrossRef]
- Hammond, M.E.H.; Hayes, D.F.; Dowsett, M.; Allred, D.C.; Hagerty, K.L.; Badve, S.; Fitzgibbons, P.; Francis, G.; Goldstein, N.S.; Hayes, M.; et al. American Society of Clinical Oncology/College of American Pathologists Guideline Recommendations for Immunohistochemical Testing of Estrogen and Progesterone Receptors in Breast Cancer. J. Clin. Oncol. 2010, 28, 2784–2795. [Google Scholar] [CrossRef] [Green Version]
- Modha, A.; Gutin, P.H. Diagnosis and Treatment of Atypical and Anaplastic Meningiomas: A Review. Neurosurgery 2005, 57, 538–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciccarelli, E.; Razzore, P.; Gaia, D.; Todaro, C.; Longo, A.; Forni, M.; Ghè, C.; Camanni, F.; Muccioli, G.; Faccani, G.; et al. Hyperprolactinaemia and prolactin binding in benign intracranial tumours. J. Neurosurg. Sci. 2001, 45, 70–74. [Google Scholar] [PubMed]
- Leães, C.G.S.; Filho, A.P.; Lima, J.F.P.; Dallago, C.M.; Batista, R.; Barbosa-Coutinho, L.M.; Ferreira, N.P.; Oliveira, M.D.C. Hyperprolactinemia and immunohistochemical expression of intracellular prolactin and prolactin receptor in primary central nervous system tumors and their relationship with cellular replication. Brain Tumor Pathol. 2007, 24, 41–46. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pregnancy-Related Meningiomas (N = 29) N (%) | Controls (N= 68) N (%) | p-Value ** | |
|---|---|---|---|
| WHO Grade | |||
| I | 26 (89.7) | 57 (83.8) | 0.54 |
| II | 3 (10.3) | 9 (13.2) | 1.00 |
| III | 0 (0) | 2 (2.9) | 1.00 |
| Ki-67 labeling index (%) Mean value (SD) | |||
| WHO Grade I | 6.3 (6.0) | 6.5 (5.0) | 0.88 |
| WHO Grade II | 4.3 (2.9) | 11.3 (7.4) * | 0.043 |
| WHO Grade III | NA | 15.5 (13.4) | NA |
| Histopathological subtype | |||
| Meningothelial/Transitional | 18 (62.1) | 42 (61.8) | 1.00 |
| Fibrous | 5 (17.2) | 11 (16.2) | 1.00 |
| Microcystic | 3 (10.3) | 1 (1.5) | 0.079 |
| Angiomatous | 0 (0) | 1 (1.5) | 1.00 |
| Metaplastic | 0 (0) | 1 (1.5) | 1.00 |
| Secretory | 0 (0) | 1 (1.5) | 1.00 |
| Chordoid | 1 (3.4) | 1 (1.5) | 0.51 |
| Clear cell | 1 (3.4) | 0 (0) | 0.30 |
| Atypical | 1 (3.4) | 8 (11.8) | 0.27 |
| Papillary | 0 (0) | 1 (1.5) | 1.00 |
| Rhabdoid | 0 (0) | 1 (1.5) | 1.00 |
| Receptor Type | Pregnancy-Related Meningiomas (N = 29) N (%) | Controls (N= 68) N (%) | p-Value # | |
|---|---|---|---|---|
| Prolactin receptor | 2 (6.9) | 2 (2.9) | 0.58 | |
| Prolactin | 0 (0) | 0 (0) | 1.00 | |
| Estrogen * | − | 21 (72.4) | 57 (83.8) | 0.26 |
| + | 8 (27.6) | 9 (13.2) | 0.14 | |
| ++ | 0 (0) | 2 (2.9) | 1.00 | |
| Progesterone ** | 0–25% | 4 (14.3) | 14 (20.9) | 0.57 |
| 25–50% | 4 (14.3) | 6 (9.0) | 0.47 | |
| 50–75% | 3 (10.7) | 10 (14.9) | 0.75 | |
| 75–100% | 17 (60.7) | 37 (55.2) | 0.66 |
| Location by Proximity to the Pituitary Gland | Pregnancy-Related Meningiomas (N = 29) N (%) | Controls (N= 68) N (%) | p-Value # |
|---|---|---|---|
| Frontal/parasellar region * | 17 (58.6) | 24 (35.3) | 0.044 |
| Other ** | 2 (6.9) | 17 (25.0) | 0.051 |
| No information | 10 (34.5) | 27 (39.7) | 0.66 |
| Location according to the major anatomical intracranial regions | |||
| A: Frontoparietal, olfactory groove, “fossa anterior” and frontal convexity | 7 (24.1) | 16 (23.5) | 1.00 |
| B: Sphenoid wing, suprasellar, temporofrontal and tuberculum sellae | 10 (34.5) | 10 (14.7) | 0.052 |
| C: Occipital and fossa posterior | 1 (3.4) | 15 (22.1) | 0.034 |
| No information | 11 (37.9) | 27 (39.7) | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giraldi, L.; Lauridsen, E.K.; Maier, A.D.; Hansen, J.V.; Broholm, H.; Fugleholm, K.; Scheie, D.; Munch, T.N. Pathologic Characteristics of Pregnancy-Related Meningiomas. Cancers 2021, 13, 3879. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13153879
Giraldi L, Lauridsen EK, Maier AD, Hansen JV, Broholm H, Fugleholm K, Scheie D, Munch TN. Pathologic Characteristics of Pregnancy-Related Meningiomas. Cancers. 2021; 13(15):3879. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13153879
Chicago/Turabian StyleGiraldi, Laura, Emma Kofoed Lauridsen, Andrea Daniela Maier, Jørgen Vinsløv Hansen, Helle Broholm, Kåre Fugleholm, David Scheie, and Tina Nørgaard Munch. 2021. "Pathologic Characteristics of Pregnancy-Related Meningiomas" Cancers 13, no. 15: 3879. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13153879