
Predictors of Invasive Adenocarcinomas among Pure Ground-Glass Nodules Less Than 2 cm in Diameter

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. CT Examination
2.3. Pure Ground-Glass Nodule Analysis
2.4. Pathological Diagnosis
2.5. Statistics
3. Results
3.1. Demographic Data and Nodule Information
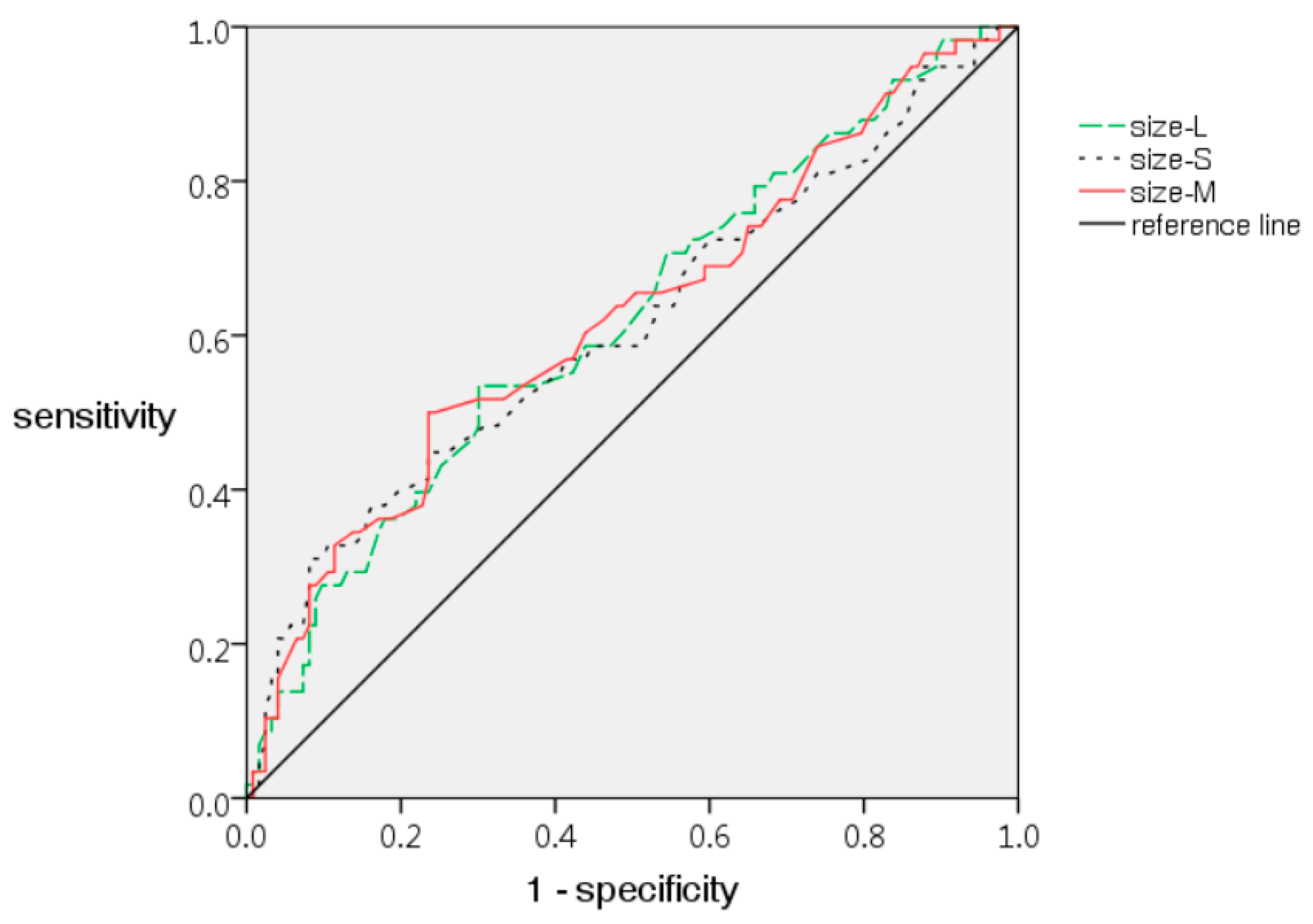
3.2. Imaging Characteristics Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN Estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Aberle, D.R.; Adams, A.M.; Berg, C.D.; Black, W.C.; Clapp, J.D.; Fagerstrom, R.M.; Gareen, I.F.; Gatsonis, C.; Marcus, P.M.; Sicks, J.D. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011, 365, 395–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Potter, A.L.; Bajaj, S.S.; Yang, C.J. The 2021 USPSTF lung cancer screening guidelines: A new frontier. Lancet. Respir. Med. 2021, 9, 689–691. [Google Scholar] [CrossRef]
- Chu, Z.G.; Li, W.J.; Fu, B.J.; Lv, F.J. CT characteristics for predicting invasiveness in pulmonary pure ground-glass nodules. AJR Am. J. Roentgenol. 2020, 215, 351–358. [Google Scholar] [CrossRef]
- Park, C.M.; Goo, J.M.; Lee, H.J.; Lee, C.H.; Chun, E.J.; Im, J.G. Nodular ground-glass opacity at thin-section CT: Histologic correlation and evaluation of change at follow-up. Radiographics 2007, 27, 391–408. [Google Scholar] [CrossRef] [Green Version]
- Travis, W.D.; Brambilla, E.; Noguchi, M.; Nicholson, A.G.; Geisinger, K.R.; Yatabe, Y.; Beer, D.G.; Powell, C.A.; Riely, G.J.; Van Schil, P.E.; et al. International association for the study of lung cancer/American Thoracic Society/European Respiratory Society international multidisciplinary classification of lung adenocarcinoma. J. Thorac. Oncol. 2011, 6, 244–285. [Google Scholar] [CrossRef] [Green Version]
- Naidich, D.P.; Bankier, A.A.; MacMahon, H.; Schaefer-Prokop, C.M.; Pistolesi, M.; Goo, J.M.; Macchiarini, P.; Crapo, J.D.; Herold, C.J.; Austin, J.H.; et al. Recommendations for the management of subsolid pulmonary nodules detected at CT: A statement from the Fleischner Society. Radiology 2013, 266, 304–317. [Google Scholar] [CrossRef]
- Moon, Y.; Lee, K.Y.; Park, J.K. The prognosis of invasive adenocarcinoma presenting as ground-glass opacity on chest computed tomography after sublobar resection. J. Thorac. Dis. 2017, 9, 3782–3792. [Google Scholar] [CrossRef] [Green Version]
- Ito, M.; Miyata, Y.; Kushitani, K.; Yoshiya, T.; Mimae, T.; Ibuki, Y.; Misumi, K.; Takeshima, Y.; Okada, M. Prediction for prognosis of resected pT1a-1bN0M0 adenocarcinoma based on tumor size and histological status: Relationship of TNM and IASLC/ATS/ERS classifications. Lung Cancer 2014, 85, 270–275. [Google Scholar] [CrossRef]
- Boland, J.M.; Froemming, A.T.; Wampfler, J.A.; Maldonado, F.; Peikert, T.; Hyland, C.; de Andrade, M.; Aubry, M.C.; Yang, P.; Yi, E.S. Adenocarcinoma in situ, minimally invasive adenocarcinoma, and invasive pulmonary adenocarcinoma—Analysis of interobserver agreement, survival, radiographic characteristics, and gross pathology in 296 nodules. Hum. Pathol. 2016, 51, 41–50. [Google Scholar] [CrossRef]
- Van Schil, P.E.; Asamura, H.; Rusch, V.W.; Mitsudomi, T.; Tsuboi, M.; Brambilla, E.; Travis, W.D. Surgical implications of the new IASLC/ATS/ERS adenocarcinoma classification. Eur. Respir. J. 2012, 39, 478–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, R.; Sabanathan, S.; Richardson, J.; Mearns, A.J.; Goulden, C. Results of surgical treatment of stage I and II lung cancer. J. Cardiovasc. Surg. 1996, 37, 169–172. [Google Scholar]
- Goldstraw, P.; Chansky, K.; Crowley, J.; Rami-Porta, R.; Asamura, H.; Eberhardt, W.E.; Nicholson, A.G.; Groome, P.; Mitchell, A.; Bolejack, V. The IASLC lung cancer staging project: Proposals for revision of the TNM stage groupings in the forthcoming (Eighth) edition of the TNM classification for lung cancer. J. Thorac. Oncol. 2016, 11, 39–51. [Google Scholar] [CrossRef] [Green Version]
- Raz, D.J.; Zell, J.A.; Ou, S.H.; Gandara, D.R.; Anton-Culver, H.; Jablons, D.M. Natural history of stage I non-small cell lung cancer: Implications for early detection. Chest 2007, 132, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Andrade, J.R.; Rocha, R.D.; Falsarella, P.M.; Rahal Junior, A.; Santos, R.S.D.; Franceschini, J.P.; Fernando, H.C.; Garcia, R.G. CT-guided percutaneous core needle biopsy of pulmonary nodules smaller than 2 cm: Technical aspects and factors influencing accuracy. J. Bras. Pneumol. 2018, 44, 307–314. [Google Scholar] [CrossRef]
- Ohno, Y.; Hatabu, H.; Takenaka, D.; Higashino, T.; Watanabe, H.; Ohbayashi, C.; Sugimura, K. CT-guided transthoracic needle aspiration biopsy of small (< or =20 mm) solitary pulmonary nodules. Am. J. Roentgenol. 2003, 180, 1665–1669. [Google Scholar] [CrossRef]
- Xiang, W.; Xing, Y.; Jiang, S.; Chen, G.; Mao, H.; Labh, K.; Jia, X.; Sun, X. Morphological factors differentiating between early lung adenocarcinomas appearing as pure ground-glass nodules measuring ≤10 mm on thin-section computed tomography. Cancer Imaging 2014, 14, 33. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.M.; Park, C.M.; Goo, J.M.; Lee, H.J.; Wi, J.Y.; Kang, C.H. Invasive pulmonary adenocarcinomas versus preinvasive lesions appearing as ground-glass nodules: Differentiation by using CT features. Radiology 2013, 268, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.; Tian, S.P.; Jin, X.; Jing, R.; Yang, Y.Q.; Jin, M.; Zhao, S.H. CT and histopathologic characteristics of lung adenocarcinoma with pure ground-glass nodules 10 mm or less in diameter. Eur. Radiol. 2017, 27, 4037–4043. [Google Scholar] [CrossRef]
- Lee, G.D.; Park, C.H.; Park, H.S.; Byun, M.K.; Lee, I.J.; Kim, T.H.; Lee, S. Lung adenocarcinoma invasiveness risk in pure ground-glass opacity lung nodules smaller than 2 cm. Thorac. Cardiovasc. Surg. 2019, 67, 321–328. [Google Scholar] [CrossRef]
- Lim, H.J.; Ahn, S.; Lee, K.S.; Han, J.; Shim, Y.M.; Woo, S.; Kim, J.H.; Yie, M.; Lee, H.Y.; Yi, C.A. Persistent pure ground-glass opacity lung nodules ≥10 mm in diameter at CT scan: Histopathologic comparisons and prognostic implications. Chest 2013, 144, 1291–1299. [Google Scholar] [CrossRef] [PubMed]
- Liang, J.; Xu, X.Q.; Xu, H.; Yuan, M.; Zhang, W.; Shi, Z.F.; Yu, T.F. Using the CT features to differentiate invasive pulmonary adenocarcinoma from pre-invasive lesion appearing as pure or mixed ground-glass nodules. Br. J. Radiol. 2015, 88, 20140811. [Google Scholar] [CrossRef] [Green Version]
- Jin, X.; Zhao, S.H.; Gao, J.; Wang, D.J.; Wu, J.; Wu, C.C.; Chang, R.P.; Ju, H.Y. CT characteristics and pathological implications of early stage (T1N0M0) lung adenocarcinoma with pure ground-glass opacity. Eur. Radiol. 2015, 25, 2532–2540. [Google Scholar] [CrossRef] [PubMed]
- Han, L.; Zhang, P.; Wang, Y.; Gao, Z.; Wang, H.; Li, X.; Ye, Z. CT quantitative parameters to predict the invasiveness of lung pure ground-glass nodules (pGGNs). Clin. Radiol. 2018, 73, 504.e501–504.e507. [Google Scholar] [CrossRef]
- Gao, F.; Sun, Y.; Zhang, G.; Zheng, X.; Li, M.; Hua, Y. CT characterization of different pathological types of subcentimeter pulmonary ground-glass nodular lesions. Br. J. Radiol. 2019, 92, 20180204. [Google Scholar] [CrossRef]
- Aoki, T.; Tomoda, Y.; Watanabe, H.; Nakata, H.; Kasai, T.; Hashimoto, H.; Kodate, M.; Osaki, T.; Yasumoto, K. Peripheral lung adenocarcinoma: Correlation of thin-section CT findings with histologic prognostic factors and survival. Radiology 2001, 220, 803–809. [Google Scholar] [CrossRef]
- Hansell, D.M.; Bankier, A.A.; MacMahon, H.; McLoud, T.C.; MΓjller, N.L.; Remy, J. Fleischner Society: Glossary of terms for thoracic imaging. Radiology 2008, 246, 697–722. [Google Scholar] [CrossRef] [Green Version]
- Kakinuma, R.; Noguchi, M.; Ashizawa, K.; Kuriyama, K.; Maeshima, A.M.; Koizumi, N.; Kondo, T.; Matsuguma, H.; Nitta, N.; Ohmatsu, H.; et al. Natural history of pulmonary subsolid nodules: A prospective multicenter study. J. Thorac. Oncol. 2016, 11, 1012–1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, F.; Li, M.; Ge, X.; Zheng, X.; Ren, Q.; Chen, Y.; Lv, F.; Hua, Y. Multi-detector spiral CT study of the relationships between pulmonary ground-glass nodules and blood vessels. Eur. Radiol. 2013, 23, 3271–3277. [Google Scholar] [CrossRef]
- Kastner, J.; Hossain, R.; Jeudy, J.; Dako, F.; Mehta, V.; Dalal, S.; Dharaiya, E.; White, C. Lung-RADS version 1.0 versus lung-RADS version 1.1: Comparison of categories using nodules from the national lung screening trial. Radiology 2021. [Google Scholar] [CrossRef]
- Hammer, M.M.; Palazzo, L.L.; Kong, C.Y.; Hunsaker, A.R. Cancer risk in subsolid nodules in the national lung screening trial. Radiology 2019, 293, 441–448. [Google Scholar] [CrossRef]
- Horeweg, N.; van Rosmalen, J.; Heuvelmans, M.A.; van der Aalst, C.M.; Vliegenthart, R.; Scholten, E.T.; ten Haaf, K.; Nackaerts, K.; Lammers, J.W.; Weenink, C.; et al. Lung cancer probability in patients with CT-detected pulmonary nodules: A prespecified analysis of data from the NELSON trial of low-dose CT screening. Lancet. Oncol. 2014, 15, 1332–1341. [Google Scholar] [CrossRef]
- Qi, L.; Xue, K.; Li, C.; He, W.; Mao, D.; Xiao, L.; Hua, Y.; Li, M. Analysis of CT morphologic features and attenuation for differentiating among transient lesions, atypical adenomatous hyperplasia, adenocarcinoma in situ, minimally invasive and invasive adenocarcinoma presenting as pure ground-glass nodules. Sci. Rep. 2019, 9, 14586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bankier, A.A.; MacMahon, H.; Goo, J.M.; Rubin, G.D.; Schaefer-Prokop, C.M.; Naidich, D.P. Recommendations for measuring pulmonary nodules at CT: A statement from the fleischner society. Radiology 2017, 285, 584–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gurney, J.W. Determining the likelihood of malignancy in solitary pulmonary nodules with Bayesian analysis. Part I. Theory. Radiology 1993, 186, 405–413. [Google Scholar] [CrossRef]
- Winer-Muram, H.T. The solitary pulmonary nodule. Radiology 2006, 239, 34–49. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Goo, J.M.; Lee, C.H.; Park, C.M.; Kim, K.G.; Park, E.A.; Lee, H.Y. Predictive CT findings of malignancy in ground-glass nodules on thin-section chest CT: The effects on radiologist performance. Eur. Radiol. 2009, 19, 552–560. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.N.; Wu, P.W.; Huang, P.C.; Pan, K.T.; Juan, Y.H.; Chuang, W.Y.; Wu, Y.C.; Lin, G.; Wan, Y.L. Correlation between CT imaging features and pathological diagnosis of ground-glass nodules proven by surgical pathology. J. Radiol. Sci. 2021, 46, 21–29. [Google Scholar] [CrossRef]
- Furuya, K.; Murayama, S.; Soeda, H.; Murakami, J.; Ichinose, Y.; Yabuuchi, H.; Katsuda, Y.; Koga, M.; Masuda, K. New classification of small pulmonary nodules by margin characteristics on high-resolution CT. Acta. Radiol. 1999, 40, 496–504. [Google Scholar] [CrossRef]
- Nie, Y.; Liu, H.; Tan, X.; Wang, H.; Li, F.; Li, C.; Han, P.; Lyv, X.; Xu, X.; Guo, M. Correlation between high-resolution computed tomography lung nodule characteristics and EGFR mutation in lung adenocarcinomas. Onco. Targets. 2019, 12, 519–526. [Google Scholar] [CrossRef] [Green Version]
- Hu, H.; Wang, Q.; Tang, H.; Xiong, L.; Lin, Q. Multi-slice computed tomography characteristics of solitary pulmonary ground-glass nodules: Differences between malignant and benign. Thorac. Cancer 2016, 7, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Yanagawa, M.; Johkoh, T.; Noguchi, M.; Morii, E.; Shintani, Y.; Okumura, M.; Hata, A.; Fujiwara, M.; Honda, O.; Tomiyama, N. Radiological prediction of tumor invasiveness of lung adenocarcinoma on thin-section CT. Medicine 2017, 96, e6331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.; Park, C.M.; Song, Y.S.; Sunwoo, L.; Choi, Y.R.; Kim, J.I.; Kim, J.H.; Bae, J.S.; Lee, J.H.; Goo, J.M. Measurement variability of persistent pulmonary subsolid nodules on same-day repeat CT: What is the threshold to determine true nodule growth during follow-up? PLoS ONE 2016, 11, e0148853. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Ma, H.; Ni, C.J.; He, J.K.; Ma, H.T.; Ge, J.F. Clinical characteristics and prognosis of ground-glass opacity nodules in young patients. J. Thorac. Dis. 2019, 11, 557–563. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Benign | AAH | AIS | MIA | IA | All | p-Value |
|---|---|---|---|---|---|---|---|
| Nodule Numbers | 29 | 14 | 25 | 55 | 58 | 181 | |
| Age | 55.8 ± 10.3 | 55.4 ± 12.2 | 55.1 ± 10.9 | 53.9 ± 11.6 | 55.4 ± 10.7 | 55.0 ± 11.0 | 0.956 |
| Sex (Female) | 21 (72.4) | 10 (71.4) | 16 (64.0) | 37 (67.3) | 45 (77.6) | 129 (71.3) | 0.695 |
| Smoking history | 2 (6.9) | 1 (7.1) | 2 (8.0) | 8 (14.5) | 2 (3.4) | 15 (8.3) | 0.318 |
| Drinking history | 2 (6.9) | 1 (7.1) | 1 (4.0) | 2 (3.6) | 2 (3.4) | 8 (4.4) | 0.833 |
| Cancer history | 5 (17.2) | 1 (7.1) | 3 (12.0) | 18 (32.7) | 14 (24.1) | 41 (22.7) | 0.122 |
| Nodule Location | 0.698 | ||||||
| In upper lobe | 15 (51.7) | 9 (64.3) | 16 (64.0) | 27 (49.1) | 31 (53.4) | 98 (54.1) | |
| Not in upper lobe | 14 (48.3) | 5 (35.7) | 9 (36.0) | 28 (50.9) | 27 (46.6) | 83 (45.9) |
| Imaging Features | Benign | AAH | AIS | MIA | IA | p-Value |
|---|---|---|---|---|---|---|
| Size-L | 7.4 ± 3.0 | 6.3 ± 2.5 | 6.0 ± 1.9 | 7.1 ± 2.7 | 8.2 ± 3.4 | 0.029 * |
| Size-S | 5.6 ± 1.9 | 4.6 ± 1.7 | 5.0 ± 1.3 | 5.3 ± 2.5 | 6.2 ± 2.6 | 0.043 * |
| Size-M | 6.5 ± 2.4 | 5.4 ± 2.0 | 5.5 ± 1.5 | 6.2 ± 2.5 | 7.2 ± 2.9 | 0.025 * |
| Content | 0.643 | |||||
| Homogenous GGN | 17 (58.6) | 10 (71.4) | 16 (64.0) | 30 (54.5) | 30 (51.7) | |
| Heterogeneous GGN | 12 (41.4) | 4 (28.6) | 9 (36.0) | 25 (45.5) | 28 (48.3) | |
| Shape | 0.203 | |||||
| Oval or polygonal | 24 (82.8) | 12 (85.7) | 25 (100.0) | 48 (87.3) | 53 (91.4) | |
| Irregular | 5 (17.2) | 2 (14.3) | 0 (0) | 7 (12.7) | 5 (8.6) | |
| Interface | 0.100 | |||||
| Well-defined | 23 (79.3) | 13 (92.9) | 24 (96.0) | 53 (96.4) | 51 (87.9) | |
| Ill-defined | 6 (20.7) | 1 (7.1) | 1 (4.0) | 2 (3.6) | 7 (12.1) | |
| Margin | 0.708 | |||||
| Smooth | 25 (86.2) | 12 (85.7) | 20 (80.0) | 43 (78.2) | 43 (74.1) | |
| Coarse | 4 (13.8) | 2 (14.3) | 5 (20.0) | 12 (21.8) | 15 (25.9) | |
| Lobulation | 1 (3.4) | 1 (7.1) | 1 (4.0) | 0 (0) | 6 (10.3) | 0.083 |
| Spiculation | 0 (0) | 0 (0) | 0 (0) | 3 (5.5) | 1 (1.7) | 0.635 |
| Air cavity | 8 (27.6) | 2 (14.3) | 5 (20.0) | 11 (20.0) | 24 (41.4) | 0.060 |
| Vessel relationship | 0.532 | |||||
| Type I | 26 (89.7) | 14 (100.0) | 24 (96.0) | 47 (85.5) | 52 (89.7) | |
| Type II | 3 (10.3) | 0 (0) | 1 (4.0) | 8 (14.5) | 6 (10.3) | |
| Pleural retraction | 2 (6.9) | 2 (14.3) | 4 (16.0) | 6 (10.9) | 11 (19.0) | 0.590 |
| Imaging Features | NIA | IA | Univariate p-Value | Multivariate p-Value |
|---|---|---|---|---|
| Size-L | 6.8 ± 2.7 | 8.2 ± 3.4 | 0.009 * | |
| Size-S | 5.2 ± 2.1 | 6.2 ± 2.6 | 0.016 * | |
| Size-M | 6.0 ± 2.3 | 7.2 ± 2.9 | 0.008 * | 0.051 |
| Heterogeneous content | 50 (40.7) | 28 (48.3) | 0.334 | |
| Irregular shape | 14 (11.4) | 5 (8.6) | 0.572 | |
| Ill-defined interface | 10 (8.1) | 7 (12.1) | 0.397 | |
| Coarse margin | 23 (18.7) | 15 (25.9) | 0.270 | |
| Lobulation | 3 (2.4) | 6 (10.3) | 0.031 * | 0.053 |
| Spiculation | 3 (2.4) | 1 (1.7) | 1.000 | |
| Air cavity | 26 (21.1) | 24 (41.4) | 0.004 * | 0.042 * |
| Type II vessel relationship | 12 (9.8) | 6 (10.3) | 0.117 | |
| Pleural retraction | 14 (11.4) | 11 (19.0) | 0.168 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, W.-C.; Huang, P.-C.; Pan, K.-T.; Chuang, W.-Y.; Wu, C.-Y.; Wong, H.-F.; Yang, C.-T.; Wan, Y.-L. Predictors of Invasive Adenocarcinomas among Pure Ground-Glass Nodules Less Than 2 cm in Diameter. Cancers 2021, 13, 3945. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13163945
Hsu W-C, Huang P-C, Pan K-T, Chuang W-Y, Wu C-Y, Wong H-F, Yang C-T, Wan Y-L. Predictors of Invasive Adenocarcinomas among Pure Ground-Glass Nodules Less Than 2 cm in Diameter. Cancers. 2021; 13(16):3945. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13163945
Chicago/Turabian StyleHsu, Wen-Chi, Pei-Ching Huang, Kuang-Tse Pan, Wen-Yu Chuang, Ching-Yang Wu, Ho-Fai Wong, Cheng-Ta Yang, and Yung-Liang Wan. 2021. "Predictors of Invasive Adenocarcinomas among Pure Ground-Glass Nodules Less Than 2 cm in Diameter" Cancers 13, no. 16: 3945. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13163945