
Atrial Fibrillation after Lung Cancer Surgery: Prediction, Prevention and Anticoagulation Management

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Incidence
3. Phatophysiology
4. Prognostic Implications
- Lin et al. showed how POAF increases the risk of stroke and mortality by about one and a half times, both in the short and long term. In patients undergoing non-cardiac surgery, this risk was approximately doubled [13];
- Koshy et al. showed that the risk of stroke related to POAF was 2.5 times higher than in patients who did not experience this arrhythmia during a follow-up of an average duration of 1.4 years; this risk was three times higher in patients undergoing non-thoracic surgery [14];
- AlTurki et al. showed a threefold increase in short-term stroke risk and approximately fourfold mortality risk in the long-term [15];
5. Risk Factors and Predictors
5.1. Clinical
5.1.1. Patient-Related
5.1.2. Surgery-Related
5.2. Biomarkers
5.2.1. Natriuretic Peptides
5.2.2. Troponin
5.2.3. C Reactive Protein and Inflammation Markers
5.2.4. Postoperative Noradrenalin
5.3. Echocardiograpic Parameters
5.4. Risk Scores
6. Prevention
6.1. Beta-Blockers
6.1.1. Metoprolol
6.1.2. Other Long-Acting Beta-Blockers
6.1.3. Short-Acting Beta-Blockers
6.1.4. Overall Beta-Blockers Effectiveness
6.2. Amiodarone
6.3. Calcium Channel Blockers
6.4. Renin-Angiotensin-Aldosterone System (RAAS) Inhibitors
6.5. Magnesium
6.6. Anti-Inflammatory Drugs
6.7. Other Drugs
6.8. Studies Comparing the Different Preventive Strategies
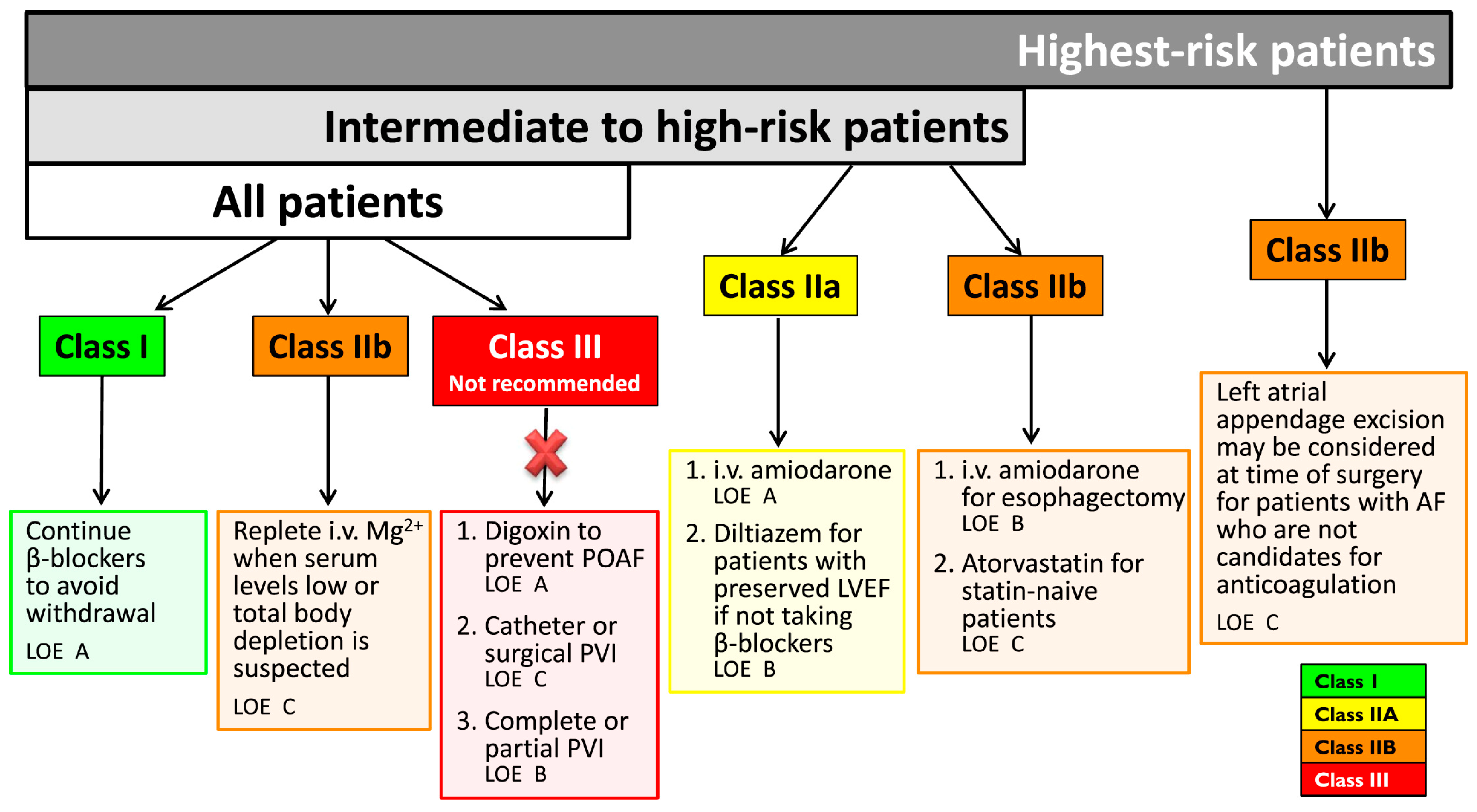
6.9. What Do Guidelines Suggest
7. Anticoagulation Management
8. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Jakobsen, C.B.; Lamberts, M.; Carlson, N.; Lock-Hansen, M.; Torp-Pedersen, C.; Gislason, G.H.; Schou, M. Incidence of atrial fibrillation in different major cancer subtypes: A Nationwide population-based 12 year follow up study. BMC Cancer 2019, 19, 1105. [Google Scholar] [CrossRef] [PubMed]
- Rahman, F.; Ko, D.; Benjamin, E.J. Association of Atrial Fibrillation and Cancer. JAMA Cardiol. 2016, 1, 384–386. [Google Scholar] [CrossRef] [Green Version]
- Cardinale, D.; Martinoni, A.; Cipolla, C.M.; Civelli, M.; Lamantia, G.; Fiorentini, C.; Mezzetti, M. Atrial fibrillation after operation for lung cancer: Clinical and prognostic significance. Ann. Thorac. Surg. 1999, 68, 1827–1831. [Google Scholar] [CrossRef]
- Dobrev, D.; Aguilar, M.; Heijman, J.; Guichard, J.B.; Nattel, S. Postoperative atrial fibrillation: Mechanisms, manifestations and management. Nat. Rev. Cardiol. 2019, 16, 417–436. [Google Scholar] [CrossRef] [PubMed]
- Roselli, E.E.; Murthy, S.C.; Rice, T.W.; Houghtaling, P.L.; Pierce, C.D.; Karchmer, D.P.; Blackstone, E.H. Atrial fibrillation complicating lung cancer resection. J. Thorac. Cardiovasc. Surg. 2005, 130, 438–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fabiani, I.; Colombo, A.; Bacchiani, G.; Cipolla, C.M.; Cardinale, D.M. Incidence, Management, Prevention and Outcome of Post-Operative Atrial Fibrillation in Thoracic Surgical Oncology. J. Clin. Med. 2019, 9, 37. [Google Scholar] [CrossRef] [Green Version]
- Ivanovic, J.; Maziak, D.E.; Ramzan, S.; McGuire, A.L.; Villeneuve, P.J.; Gilbert, S.; Sundaresan, R.S.; Shamji, F.M.; Seely, A.J. Incidence, severity and perioperative risk factors for atrial fibrillation following pulmonary resection. Interact. Cardiovasc. Thorac Surg. 2014, 18, 340–346. [Google Scholar] [CrossRef] [Green Version]
- Higuchi, S.; Kabeya, Y.; Matsushita, K.; Arai, N.; Tachibana, K.; Tanaka, R.; Kawachi, R.; Takei, H.; Suzuki, Y.; Kogure, M.; et al. Incidence and complications of perioperative atrial fibrillation after non-cardiac surgery for malignancy. PLoS ONE 2019, 14, e0216239. [Google Scholar] [CrossRef] [Green Version]
- Vretzakis, G.; Simeoforidou, M.; Stamoulis, K.; Bareka, M. Supraventricular arrhythmias after thoracotomy: Is there a role for autonomic imbalance? Anesthesiol. Res. Pract. 2013, 2013, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Bessissow, A.; Khan, J.; Devereaux, P.J.; Alvarez-Garcia, J.; Alonso-Coello, P. Postoperative atrial fibrillation in non-cardiac and cardiac surgery: An overview. J. Thromb. Haemost. 2015, 13, 2134. [Google Scholar] [CrossRef]
- Wang, H.; Wang, Z.; Zhou, M.; Chen, J.; Yao, F.; Zhao, L.; He, B. Postoperative atrial fibrillation in pneumonectomy for primary lung cancer. J. Thorac. Dis. 2021, 13, 789–802. [Google Scholar] [CrossRef]
- Joshi, K.K.; Tiru, M.; Chin, T.; Fox, M.T.; Stefan, M.S. Postoperative atrial fibrillation in patients undergoing non-cardiac non-thoracic surgery: A practical approach for the hospitalist. Hosp. Pract. 2015, 43, 235–244. [Google Scholar] [CrossRef] [Green Version]
- Lin, M.H.; Kamel, H.; Singer, D.E.; Wu, Y.L.; Lee, M.; Ovbiagele, B. Perioperative/Postoperative Atrial Fibrillation and Risk of Subsequent Stroke and/or Mortality. Stroke 2019, 50, 1364–1371. [Google Scholar] [CrossRef]
- Koshy, A.N.; Hamilton, G.; Theuerle, J.; The, A.W.; Han, H.C.; Gow, P.J.; Lim, H.S.; Thijs, V.; Farouque, O. Postoperative Atrial Fibrillation Following Noncardiac Surgery Increases Risk of Stroke. Am. J. Med. 2020, 133, 311–322. [Google Scholar] [CrossRef] [Green Version]
- AlTurki, A.; Marafi, M.; Proietti, R.; Cardinale, D.; Blackwell, R.; Dorian, P.; Bessissow, A.; Vieira, L.; Greiss, I.; Essebag, V.; et al. Major Adverse Cardiovascular Events Associated with Postoperative Atrial Fibrillation After Noncardiac Surgery: A Systematic Review and Meta-Analysis. Circ. Arrhythm. Electrophysiol. 2020, 13, e007437. [Google Scholar] [CrossRef]
- Albini, A.; Malavasi, V.L.; Vitolo, M.; Imberti, J.F.; Marietta, M.; Lip, G.Y.H.; Boriani, G. Long-term outcomes of postoperative atrial fibrillation following non cardiac surgery: A systematic review and metanalysis. Eur. J. Intern. Med. 2021, 85, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Lowres, N.; Mulcahy, G.; Jin, K.; Gallagher, R.; Neubeck, L.; Freedman, B. Incidence of postoperative atrial fibrillation recurrence in patients discharged in sinus rhythm after cardiac surgery: A systematic review and meta-analysis. Interact. Cardiovasc. Thorac. Surg. 2018, 26, 504–511. [Google Scholar] [CrossRef]
- Yamashita, K.; Hu, N.; Ranjan, R.; Selzman, C.H.; Dosdall, D.J. Clinical Risk Factors for Postoperative Atrial Fibrillation among Patients after Cardiac Surgery. Thorac. Cardiovasc. Surg. 2019, 67, 107–116. [Google Scholar] [CrossRef]
- Ishibashi, H.; Wakejima, R.; Asakawa, A.; Baba, S.; Nakashima, Y.; Seto, K.; Kobayashi, M.; Okubo, K. Postoperative Atrial Fibrillation in Lung Cancer Lobectomy-Analysis of Risk Factors and Prognosis. World J. Surg. 2020, 44, 3952–3959. [Google Scholar] [CrossRef] [PubMed]
- Frendl, G.; Sodickson, A.C.; Chung, M.K.; Waldo, A.L.; Gersh, B.J.; Tisdale, J.E.; Calkins, H.; Aranki, S.; Kaneko, T.; Cassivi, S.; et al. 2014 AATS guidelines for the prevention and management of perioperative atrial fibrillation and flutter for thoracic surgical procedures. J. Thorac. Cardiovasc. Surg. 2014, 148, e153–e193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwata, T.; Nagato, K.; Nakajima, T.; Suzuki, H.; Yoshida, S.; Yoshino, I. Risk factors predictive of atrial fibrillation after lung cancer surgery. Surg. Today. 2016, 46, 877–886. [Google Scholar] [CrossRef] [PubMed]
- Seitlinger, J.; Olland, A.; Guinard, S.; Massard, G.; Falcoz, P.E. Conversion from video-assisted thoracic surgery (VATS) to thoracotomy during major lung resection: How does it affect perioperative outcomes? Interact. Cardiovasc. Thorac. Surg. 2021, 32, 55–63. [Google Scholar] [CrossRef]
- Cardinale, D.; Colombo, A.; Sandri, M.T.; Lamantia, G.; Colombo, N.; Civelli, M.; Salvatici, M.; Veronesi, G.; Veglia, F.; Fiorentini, C.; et al. Increased perioperative N-terminal pro-B-type natriuretic peptide levels predict atrial fibrillation after thoracic surgery for lung cancer. Circulation 2007, 115, 1339–1344. [Google Scholar] [CrossRef] [Green Version]
- Cardinale, D.; Sandri, M.T.; Colombo, A.; Salvatici, M.; Tedeschi, I.; Bacchiani, G.; Beggiato, M.; Meroni, C.A.; Civelli, M.; Lamantia, G.; et al. Prevention of Atrial Fibrillation in High-risk Patients Undergoing Lung Cancer Surgery: The PRESAGE Trial. Ann. Surg. 2016, 264, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Nojiri, T.; Maeda, H.; Takeuchi, Y.; Funakoshi, Y.; Kimura, T.; Maekura, R.; Yamamoto, K.; Okumura, M. Predictive value of B-type natriuretic peptide for postoperative atrial fibrillation following pulmonary resection for lung cancer. Eur. J. Cardiothorac. Surg. 2010, 37, 787–791. [Google Scholar] [CrossRef]
- Ata, Y.; Turk, T.; Ay, D.; Eris, C.; Demir, M.; Ari, H.; Ata, F.; Yavuz, S.; Ozyazicioglu, A. Ability of B-type natriuretic peptide in predicting postoperative atrial fibrillation in patients undergoing coronary artery bypass grafting. Heart Surg. Forum. 2009, 12, E211–E216. [Google Scholar] [CrossRef]
- Masson, S.; Wu, J.H.; Simon, C.; Barlera, S.; Marchioli, R.; Mariani, J.; Macchia, A.; Lombardi, F.; Vago, T.; Aleksova, A.; et al. Investigators. Circulating cardiac biomarkers and postoperative atrial fibrillation in the OPERA trial. Eur. J. Clin. Investig. 2015, 45, 170–178. [Google Scholar] [CrossRef]
- Hernández-Romero, D.; Vílchez, J.A.; Lahoz, Á.; Romero-Aniorte, A.I.; Orenes-Piñero, E.; Caballero, L.; Jara-Rubio, R.; Arribas, J.M.; García-Alberola, A.; Valdés, M.; et al. High-sensitivity troponin T as a biomarker for the development of atrial fibrillation after cardiac surgery. Eur. J. Cardiothorac. Surg. 2014, 45, 733–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, G.L.; Chen, J.; Hu, C.B.; Yan, M.L.; Xu, Q.H.; Yan, J. Value of plasma brain natriuretic peptide levels for predicting postoperative atrial fibrillation: A systemic review and meta-analysis. World J. Surg. 2014, 38, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Simmers, D.; Potgieter, D.; Ryan, L.; Fahrner, R.; Rodseth, R.N. The use of preoperative B-type natriuretic peptide as a predictor of atrial fibrillation after thoracic surgery: Systematic review and meta-analysis. J. Cardiothorac. Vasc. Anesth. 2015, 29, 389–395. [Google Scholar] [CrossRef] [Green Version]
- Knayzer, B.; Abramov, D.; Natalia, B.; Tovbin, D.; Ganiel, A.; Katz, A. Atrial fibrillation and plasma troponin I elevation after cardiac surgery: Relation to inflammation-associated parameters. J. Card. Surg. 2007, 22, 117–123. [Google Scholar] [CrossRef]
- Leal, J.C.; Petrucci, O.; Godoy, M.F.; Braile, D.M. Perioperative serum troponin I levels are associated with higher risk for atrial fibrillation in patients undergoing coronary artery bypass graft surgery. Interact. Cardiovasc. Thorac. Surg. 2012, 14, 22–25. [Google Scholar] [CrossRef] [Green Version]
- Lahoz-Tornos, Á.; Vilchez-Aguilera, J.A.; Hernandez-Romero, D.; Romero-Aniorte, A.I.; Orenes-Piñero, E.; Jara-Rubio, R.; Del Saz-Ortiz, A.; Arribas-Leal, J.M.; García-Alberola, A.; Valdés-Chávarri, M.; et al. Colesterol HDL y troponina T ultrasensible como biomarcadores predictivos de fibrilación auricular postoperatoria [HDL cholesterol and high-sensitive troponin T as predictive biomarkers of atrial fibrillation after heart surgery]. Arch. Cardiol. Mex. 2015, 85, 111–117. [Google Scholar] [PubMed]
- Li, T.; Sun, Z.L.; Xie, Q.Y. Meta-analysis Identifies Serum C-Reactive Protein as an Indicator of Atrial Fibrillation Risk After Coronary Artery Bypass Graft. Am. J. Ther. 2016, 23. [Google Scholar] [CrossRef]
- Weymann, A.; Popov, A.F.; Sabashnikov, A.; Ali-Hasan-Al-Saegh, S.; Ryazanov, M.; Tse, G.; Mirhosseini, S.J.; Liu, T.; Lotfaliani, M.; Sedaghat, M.; et al. Baseline and postoperative levels of C-reactive protein and interleukins as inflammatory predictors of atrial fibrillation following cardiac surgery: A systematic review and meta-analysis. Kardiol. Pol. 2018, 76, 440–451. [Google Scholar] [CrossRef] [Green Version]
- Olesen, O.J.; Vinding, N.E.; Østergaard, L.; Butt, J.H.; Gislason, G.H.; Torp-Pedersen, C.; Køber, L.; Fosbøl, E.L. C-reactive protein after coronary artery bypass graft surgery and its relationship with postoperative atrial fibrillation. Europace 2020, 22, 1182–1188. [Google Scholar] [CrossRef]
- Liu, Z.; Nguyen Khuong, J.; Borg Caruana, C.; Jackson, S.M.; Campbell, R.; Ramson, D.M.; Penny-Dimri, J.C.; Kluger, M.; Segal, R.; Perry, L.A. The Prognostic Value of Elevated Perioperative Neutrophil-Lymphocyte Ratio in Predicting Postoperative Atrial Fibrillation After Cardiac Surgery: A Systematic Review and Meta-Analysis. Heart Lung Circ. 2020, 29, 1015–1024. [Google Scholar] [CrossRef]
- Kalman, J.M.; Munawar, M.; Howes, L.G.; Louis, W.J.; Buxton, B.F.; Gutteridge, G.; Tonkin, A.M. Atrial fibrillation after coronary artery bypass grafting is associated with sympathetic activation. Ann. Thorac. Surg. 1995, 60, 1709–1715. [Google Scholar] [CrossRef]
- Nojiri, T.; Maeda, H.; Takeuchi, Y.; Funakoshi, Y.; Maekura, R.; Yamamoto, K.; Okumura, M. Predictive value of preoperative tissue Doppler echocardiographic analysis for postoperative atrial fibrillation after pulmonary resection for lung cancer. J. Thorac. Cardiovasc. Surg. 2010, 140, 764–768. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.; Sun, J.; Yuan, X.; Liu, H. Risk factors and prediction model construction of post-operative atrial fibrillation after thoracic surgery in Chinese patients. Arch. Med. Sci. 2021. [Google Scholar] [CrossRef]
- Hidayet, Ş.; Yağmur, J.; Bayramoğlu, A.; Taşolar, M.H.; Kurtoğlu, E.; Özyalın, F. Prediction of postoperative atrial fibrillation with left atrial mechanical functions and NT-pro ANP levels after coronary artery bypass surgery: A three-dimensional echocardiography study. Echocardiography 2018, 35, 661–666. [Google Scholar] [CrossRef]
- Pernigo, M.; Benfari, G.; Geremia, G.; Noni, M.; Borio, G.; Mazzali, G.; Zamboni, M.; Onorati, F.; Faggian, G.; Vassanelli, C.; et al. Atrial Function as an Independent Predictor of Postoperative Atrial Fibrillation in Patients Undergoing Aortic Valve Surgery for Severe Aortic Stenosis. J. Am. Soc. Echocardiogr. 2017, 30, 956–965. [Google Scholar] [CrossRef]
- Hu, J.; Peng, L.; Qian, H.; Li, Y.J.; Meng, W.; Xiao, Z.H.; Zhao, J.J.; Hu, J.Z.; Zhang, E.Y. Transoesophageal echocardiography for prediction of postoperative atrial fibrillation after isolated aortic valve replacement: Two-dimensional speckle tracking for intraoperative assessment of left ventricular longitudinal strain. Eur. J. Cardiothorac. Surg. 2015, 47, 833–839. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.L.; Zeng, M.; Liu, Y.; Xu, Y.; Bai, Y.; Cao, L.; Ling, Z.; Fan, J.; Yin, Y. CHA2DS2-VASc Score for Identifying Patients at High Risk of Postoperative Atrial Fibrillation After Cardiac Surgery: A Meta-analysis. Ann. Thorac. Surg. 2020, 109, 1210–1216. [Google Scholar] [CrossRef]
- Lee, C.T.; Strauss, D.M.; Stone, L.E.; Stoltzfus, J.C.; Puc, M.M.; Burfeind, W.R. Preoperative CHA2DS2-VASc Score Predicts Postoperative Atrial Fibrillation after Lobectomy. Thorac. Cardiovasc. Surg. 2019, 67, 125–130. [Google Scholar] [CrossRef]
- Geçmen, Ç.; Babür, G.G.; Erdoğan, E.; Hatipoğlu, S.; Güler, E.; Yılmaz, F.; Unkun, T.; Cap, M.; Bengi, B.R.; Bayram, T.; et al. SYNTAX score predicts postoperative atrial fibrillation in patients undergoing on-pump isolated coronary artery bypass grafting surgery. Anatol. J. Cardiol. 2016, 16, 655–661. [Google Scholar]
- Erdolu, B.; As, A.K.; Engin, M. The Relationship between the HATCH Score, Neutrophil to Lymphocyte Ratio and Postoperative Atrial Fibrillation After Off-Pump Coronary Artery Bypass Graft Surgery. Heart Surg. Forum. 2020, 23, E088–E092. [Google Scholar] [CrossRef]
- Mariscalco, G.; Biancari, F.; Zanobini, M.; Cottini, M.; Piffaretti, G.; Saccocci, M.; Banach, M.; Beghi, C.; Angelini, G.D. Bedside tool for predicting the risk of postoperative atrial fibrillation after cardiac surgery: The POAF score. J. Am. Heart Assoc. 2014, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burgos, L.M.; Seoane, L.; Parodi, J.B.; Espinoza, J.; Galizia, B.V.; Benzadón, M.; Navia, D. Postoperative atrial fibrillation is associated with higher scores on predictive indices. J. Thorac. Cardiovasc. Surg. 2019, 157, 2279–2286. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, C.J.; Bille, S.; Ahlburg, P.; Rybro, L.; Hjortholm, K.; Andresen, E.B. Perioperative metoprolol reduces the frequency of atrial fibrillation after thoracotomy for lung resection. J. Cardiothorac. Vasc. Anesth. 1997, 11, 746–751. [Google Scholar] [CrossRef]
- Skiba, M.A.; Pick, A.W.; Chaudhuri, K.; Bailey, M.; Krum, H.; Kwa, L.J.; Rosenfeldt, F.L. Prophylaxis against atrial fibrillation after cardiac surgery: Beneficial effect of perioperative metoprolol. Heart Lung Circ. 2013, 22, 627–633. [Google Scholar] [CrossRef]
- Norhayati, M.N.; Shaiful, B.I.; Zaharah, S.; Nik, H.N.H.; Mohammad, A.Z.; Irfan, M. Metoprolol for prophylaxis of postoperative atrial fibrillation in cardiac surgery patients: Systematic review and meta-analysis. BMJ Open. 2020, 10, e038364. [Google Scholar] [CrossRef]
- Wang, H.S.; Wang, Z.W.; Yin, Z.T. Carvedilol for prevention of atrial fibrillation after cardiac surgery: A meta-analysis. PLoS ONE 2014, 9, e94005. [Google Scholar] [CrossRef] [Green Version]
- Parikka, H.; Toivonen, L.; Heikkilä, L.; Virtanen, K.; Järvinen, A. Comparison of sotalol and metoprolol in the prevention of atrial fibrillation after coronary artery bypass surgery. J. Cardiovasc. Pharmacol. 1998, 31, 67–73. [Google Scholar] [CrossRef]
- Kerin, N.Z.; Jacob, S. The efficacy of sotalol in preventing postoperative atrial fibrillation: A meta-analysis. Am. J. Med. 2011, 124, 875.e1–875.e9. [Google Scholar] [CrossRef]
- Sasaki, K.; Kumagai, K.; Maeda, K.; Akiyama, M.; Ito, K.; Matsuo, S.; Katahira, S.; Suzuki, T.; Suzuki, Y.; Kaiho, Y.; et al. Preventive effect of low-dose landiolol on postoperative atrial fibrillation study (PELTA study). Gen. Thorac. Cardiovasc. Surg. 2020, 68, 1240–1251. [Google Scholar] [CrossRef] [PubMed]
- Aoyama, H.; Otsuka, Y.; Aoyama, Y. Landiolol infusion during general anesthesia does not prevent postoperative atrial fibrillation in patients undergoing lung resection. Gen. Thorac. Cardiovasc. Surg. 2016, 64, 735–741. [Google Scholar] [CrossRef]
- Sakamoto, A.; Hamasaki, T.; Kitakaze, M. Perioperative landiolol administration reduces atrial fibrillation after cardiac surgery: A meta-analysis of randomized controlled trials. Adv. Ther. 2014, 31, 440–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walter, E.; Heringlake, M. Cost-Effectiveness Analysis of Landiolol, an Ultrashort-Acting Beta-Blocker, for Prevention of Postoperative Atrial Fibrillation for the Germany Health Care System. J. Cardiothorac. Vasc. Anesth. 2020, 34, 888–897. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.H.; Jang, M.J.; Hwang, H.Y. Perioperative Beta-Blocker for Atrial Fibrillation after Cardiac Surgery: A Meta-Analysis. Thorac. Cardiovasc. Surg. 2021, 69, 133–140. [Google Scholar]
- Oesterle, A.; Weber, B.; Tung, R.; Choudhry, N.K.; Singh, J.P.; Upadhyay, G.A. Preventing Postoperative Atrial Fibrillation After Noncardiac Surgery: A Meta-analysis. Am. J. Med. 2018, 131, 795–804. [Google Scholar] [CrossRef]
- Riber, L.P.; Christensen, T.D.; Jensen, H.K.; Hoejsgaard, A.; Pilegaard, H.K. Amiodarone significantly decreases atrial fibrillation in patients undergoing surgery for lung cancer. Ann. Thorac. Surg. 2012, 94, 339–346. [Google Scholar] [CrossRef]
- Riber, L.P.; Christensen, T.D.; Pilegaard, H.K. Amiodarone is a cost-neutral way of preventing atrial fibrillation after surgery for lung cancer. Eur. J. Cardiothorac. Surg. 2014, 45, 120–125. [Google Scholar] [CrossRef]
- Giri, S.; White, C.M.; Dunn, A.B.; Felton, K.; Freeman-Bosco, L.; Reddy, P.; Tsikouris, J.P.; Wilcox, H.A.; Kluger, J. Oral amiodarone for prevention of atrial fibrillation after open heart surgery, the Atrial Fibrillation Suppression Trial (AFIST): A randomised placebo-controlled trial. Lancet 2001, 357, 830–836. [Google Scholar] [CrossRef]
- Zhu, J.; Wang, C.; Gao, D.; Zhang, C.; Zhang, Y.; Lu, Y.; Gao, Y. Meta-analysis of amiodarone versus β-blocker as a prophylactic therapy against atrial fibrillation following cardiac surgery. Intern. Med. J. 2012, 42, 1078–1087. [Google Scholar] [CrossRef]
- Van, M.W.; Tits, G.; Demuynck, K.; Lacquet, L.; Deneffe, G.; Tjandra-Maga, T.; Demedts, M. Verapamil as prophylactic treatment for atrial fibrillation after lung operations. Ann. Thorac. Surg. 1996, 61, 1083–1086. [Google Scholar] [CrossRef] [Green Version]
- Hochreiter, M.; Schmidt, T.; Siegler, B.H.; Sisic, L.; Schmidt, K.; Bruckner, T.; Müller-Stich, B.P.; Diener, M.K.; Weigand, M.A.; Büchler, M.W.; et al. Diltiazem Prophylaxis for the Prevention of Atrial Fibrillation in Patients Undergoing Thoracoabdominal Esophagectomy: A Retrospective Cohort Study. World J. Surg. 2020, 44, 2295–2304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lederer, M.R.; Deemer, A.; Liongson, F.A.; Roma, N.; Lee, C.T.; Stoltzfus, J.C.; Burfeind, W.R. Diltiazem Does Not Prevent Postoperative Atrial Fibrillation After Thoracoscopic Lobectomy. Innovations 2021, 16, 249–253. [Google Scholar] [CrossRef]
- Ozaydin, M.; Dede, O.; Varol, E.; Kapan, S.; Turker, Y.; Peker, O.; Duver, H.; Ibrisim, E. Effect of renin-angiotensin aldosteron system blockers on postoperative atrial fibrillation. Int. J. Cardiol. 2008, 127, 362–367. [Google Scholar] [CrossRef]
- Chen, S.; Acou, W.J.; Kiuchi, M.G.; Meyer, C.; Sommer, P.; Martinek, M.; Schratter, A.; Andrea, B.R.; Ling, Z.; Liu, S.; et al. Association of Preoperative Renin-Angiotensin System Inhibitors with Prevention of Postoperative Atrial Fibrillation and Adverse Events: A Systematic Review and Meta-analysis. JAMA Netw. Open 2019, 2, e194934. [Google Scholar] [CrossRef] [Green Version]
- Milne, B.; Gilbey, T.; Ostermann, M.; Kunst, G. Pro: We Should Stop ACE Inhibitors Early Before Cardiac Surgery to Prevent Postoperative Acute Kidney Injury. J. Cardiothorac. Vasc. Anesth. 2020, 34, 2832–2835. [Google Scholar] [CrossRef]
- Osawa, E.A.; Cutuli, S.L.; Cioccari, L.; Bitker, L.; Peck, L.; Young, H.; Hessels, L.; Yanase, F.; Fukushima, J.T.; Hajjar, L.A.; et al. Continuous Magnesium Infusion to Prevent Atrial Fibrillation After Cardiac Surgery: A Sequential Matched Case-Controlled Pilot Study. J. Cardiothorac. Vasc. Anesth. 2020, 34, 2940–2947. [Google Scholar] [CrossRef]
- Solomon, A.J.; Berger, A.K.; Trivedi, K.K.; Hannan, R.L.; Katz, N.M. The combination of propranolol and magnesium does not prevent postoperative atrial fibrillation. Ann. Thorac. Surg. 2000, 69, 126–129. [Google Scholar] [CrossRef]
- Chaudhary, R.; Garg, J.; Turagam, M.; Chaudhary, R.; Gupta, R.; Nazir, T.; Bozorgnia, B.; Albert, C.; Lakkireddy, D. Role of Prophylactic Magnesium Supplementation in Prevention of Postoperative Atrial Fibrillation in Patients Undergoing Coronary Artery Bypass Grafting: A Systematic Review and Meta-Analysis of 20 Randomized Controlled Trials. J. Atr. Fibrillation 2019, 12, 2154. [Google Scholar] [CrossRef]
- Miller, S.; Crystal, E.; Garfinkle, M.; Lau, C.; Lashevsky, I.; Connolly, S.J. Effects of magnesium on atrial fibrillation after cardiac surgery: A meta-analysis. Heart 2005, 91, 618–623. [Google Scholar] [CrossRef] [PubMed]
- Terzi, A.; Furlan, G.; Chiavacci, P.; Dal, C.B.; Luzzani, A.; Dalla, V.S. Prevention of atrial tachyarrhythmias after non-cardiac thoracic surgery by infusion of magnesium sulfate. Thorac. Cardiovasc. Surg. 1996, 44, 300–333. [Google Scholar] [CrossRef] [PubMed]
- Marik, P.E.; Fromm, R. The efficacy and dosage effect of corticosteroids for the prevention of atrial fibrillation after cardiac surgery: A systematic review. J. Crit. Care 2009, 24, 458–463. [Google Scholar] [CrossRef]
- Imazio, M.; Brucato, A.; Ferrazzi, P.; Rovere, M.E.; Gandino, A.; Cemin, R.; Ferrua, S.; Belli, R.; Maestroni, S.; Simon, C.; et al. Colchicine reduces postoperative atrial fibrillation: Results of the Colchicine for the Prevention of the Postpericardiotomy Syndrome (COPPS) atrial fibrillation substudy. Circulation 2011, 124, 2290–2295. [Google Scholar] [CrossRef] [Green Version]
- Imazio, M.; Brucato, A.; Ferrazzi, P.; Pullara, A.; Adler, Y.; Barosi, A.; Caforio, A.L.; Cemin, R.; Chirillo, F.; Comoglio, C.; et al. Colchicine for prevention of postpericardiotomy syndrome and postoperative atrial fibrillation: The COPPS-2 randomized clinical trial. JAMA 2014, 312, 1016–1023. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhang, L.; Wang, S.; Lu, F.; Zhen, J.; Chen, W. Dexmedetomidine Reduces Atrial Fibrillation After Adult Cardiac Surgery: A Meta-Analysis of Randomized Controlled Trials. Am. J. Cardiovasc. Drugs 2020, 20, 271–281. [Google Scholar] [CrossRef]
- Turan, A.; Duncan, A.; Leung, S.; Karimi, N.; Fang, J.; Mao, G.; Hargrave, J.; Gillinov, M.; Trombetta, C.; Ayad, S.; et al. Dexmedetomidine for reduction of atrial fibrillation and delirium after cardiac surgery (DECADE): A randomised placebo-controlled trial. Lancet 2020, 396, 177–185. [Google Scholar] [CrossRef]
- Nojiri, T.; Yamamoto, K.; Maeda, H.; Takeuchi, Y.; Ose, N.; Susaki, Y.; Inoue, M.; Okumura, M. A Double-Blind Placebo-Controlled Study of the Effects of Olprinone, a Specific Phosphodiesterase III Inhibitor, for Preventing Postoperative Atrial Fibrillation in Patients Undergoing Pulmonary Resection for Lung Cancer. Chest 2015, 148, 1285–1292. [Google Scholar] [CrossRef] [PubMed]
- Rezaei, Y.; Gholami-Fesharaki, M.; Dehghani, M.R.; Arya, A.; Haghjoo, M.; Arjmand, N. Statin Antiarrhythmic Effect on Atrial Fibrillation in Statin-Naive Patients Undergoing Cardiac Surgery: A Meta-Analysis of Randomized Controlled Trials. J. Cardiovasc. Pharmacol. Ther. 2016, 21, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.; Xue, S.; Hu, Z.L.; Shan, J.G.; Yang, W.G. The use of statins to prevent postoperative atrial fibrillation after coronary artery bypass grafting: A meta-analysis of 12 studies. J. Cardiovasc. Pharmacol. 2014, 64, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Amar, D.; Park, B.; Zhang, H.; Shi, W.; Fleisher, M.; Thaler, H.T.; Rusch, V.W. Beneficial effects of perioperative statins for major pulmonary resection. J. Thorac. Cardiovasc. Surg. 2015, 149, 1532–1538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Auer, J.; Weber, T.; Berent, R.; Puschmann, R.; Hartl, P.; Ng, C.K.; Schwarz, C.; Lehner, E.; Strasser, U.; Lassnig, E.; et al. A comparison between oral antiarrhythmic drugs in the prevention of atrial fibrillation after cardiac surgery: The pilot study of prevention of postoperative atrial fibrillation (SPPAF), a randomized, placebo-controlled trial. Am. Heart J. 2004, 147, 636–643. [Google Scholar] [CrossRef]
- Solomon, A.J.; Greenberg, M.D.; Kilborn, M.J.; Katz, N.M. Amiodarone versus a beta-blocker to prevent atrial fibrillation after cardiovascular surgery. Am. Heart J. 2001, 142, 811–815. [Google Scholar] [CrossRef]
- Burgess, D.C.; Kilborn, M.J.; Keech, A.C. Interventions for prevention of post-operative atrial fibrillation and its complications after cardiac surgery: A meta-analysis. Eur. Heart J. 2006, 27, 2846–2857. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [PubMed]
- Makhija, Z.; Allen, M.S.; Wigle, D.A.; Shen, K.R.; Cassivi, S.D.; Nichols, F.C., 3rd; Deschamps, C. Routine anticoagulation is not indicated for postoperative general thoracic surgical patients with new-onset atrial fibrillation. Ann. Thorac. Surg. 2011, 92, 421–427. [Google Scholar] [CrossRef]
- Anderson, E.; Dyke, C.; Levy, J.H. Anticoagulation strategies for the management of postoperative atrial fibrillation. Clin. Lab. Med. 2014, 34, 537–561. [Google Scholar] [CrossRef]
- Smith, H.; Yeung, C.; Gowing, S.; Sadek, M.; Maziak, D.; Gilbert, S.; Shamji, F.; Villeneuve, P.; Sundaresan, S.; Seely, A. A review and analysis of strategies for prediction, prevention and management of post-operative atrial fibrillation after non-cardiac thoracic surgery. J. Thorac. Dis. 2018, 10, S3799–S3808. [Google Scholar] [CrossRef]
- Yao, R.J.R.; Hawkins, N.M.; Lavaie, Y.; Deyell, M.W.; Andrade, J.G.; Bashir, J. Anticoagulation management of postoperative atrial fibrillation after cardiac surgery: A systematic review. J. Card. Surg. 2021, 36, 2081–2094. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Number of Studies/Patients | Short Term (1 Month) Stroke Risk Increase | Short Term (1 Month) Mortality Risk Increase | Long Term Stroke Risk Increase | Long Term Mortality Risk Increase |
|---|---|---|---|---|---|---|
| Lin et al. [13] | 2019 | 35/2,458,010 | ×1.6 | ×1.4 | ×1.4 | ×1.4 |
| Koshy et al. [14] | 2019 | 14/3,536,291 | - | ×3 | ×2.5 | - |
| AlTurki et al. [15] | 2020 | 28/2,612,816 | ×3 | - | ×4 | - |
| Albini et al. [16] | 2021 | 8/3,718,587 | - | - | ×4 | ×3.6 |
| Title | Low Risk | Intermediate Risk | High Risk |
|---|---|---|---|
| Procedure | Flexible bronchoscopy Tracheal stenting Thoracostomy Pleurodesis Tracheostomy Rigid broncoscopy Mediastinoscopy Toracoscopic wedge resection | Simpathectomy Segmentectomy | Pleurectomy Lobectomy Lung transplantation Fistula repair Bullectomy Pneumonectomy Tracheal resection Anterior mediastinal resection |
| POAF incidence | <5% | 5–15% | >15% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Semeraro, G.C.; Meroni, C.A.; Cipolla, C.M.; Cardinale, D.M. Atrial Fibrillation after Lung Cancer Surgery: Prediction, Prevention and Anticoagulation Management. Cancers 2021, 13, 4012. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13164012
Semeraro GC, Meroni CA, Cipolla CM, Cardinale DM. Atrial Fibrillation after Lung Cancer Surgery: Prediction, Prevention and Anticoagulation Management. Cancers. 2021; 13(16):4012. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13164012
Chicago/Turabian StyleSemeraro, Gennaro Carmine, Carlo Ambrogio Meroni, Carlo Maria Cipolla, and Daniela Maria Cardinale. 2021. "Atrial Fibrillation after Lung Cancer Surgery: Prediction, Prevention and Anticoagulation Management" Cancers 13, no. 16: 4012. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13164012