
Heat Shock Proteins 27, 70, and 110: Expression and Prognostic Significance in Colorectal Cancer

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Patient Selection
2.2. Microarrays
2.3. Immunohistochemistry
2.4. Microscopy
2.5. Statistics
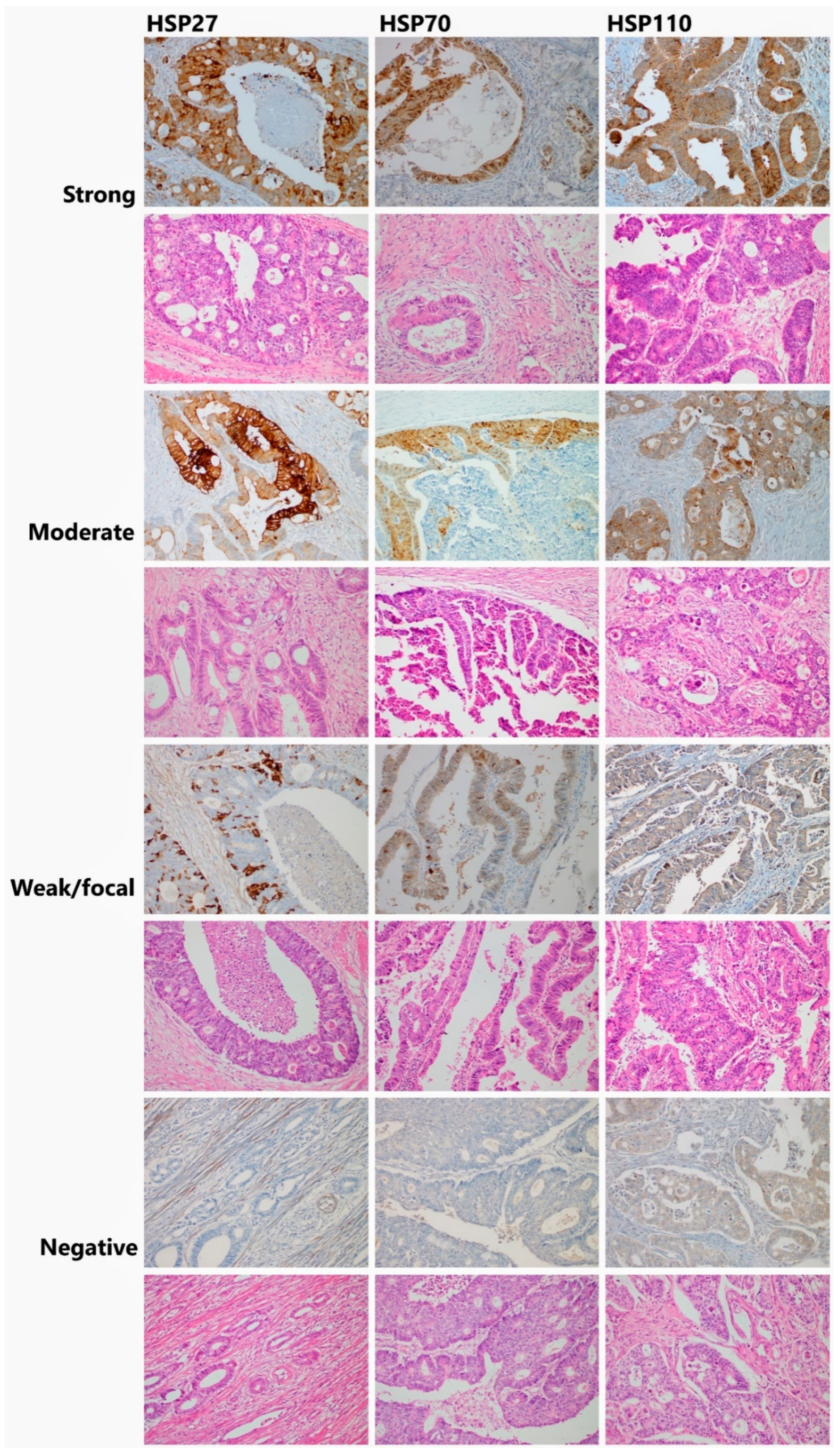
3. Results
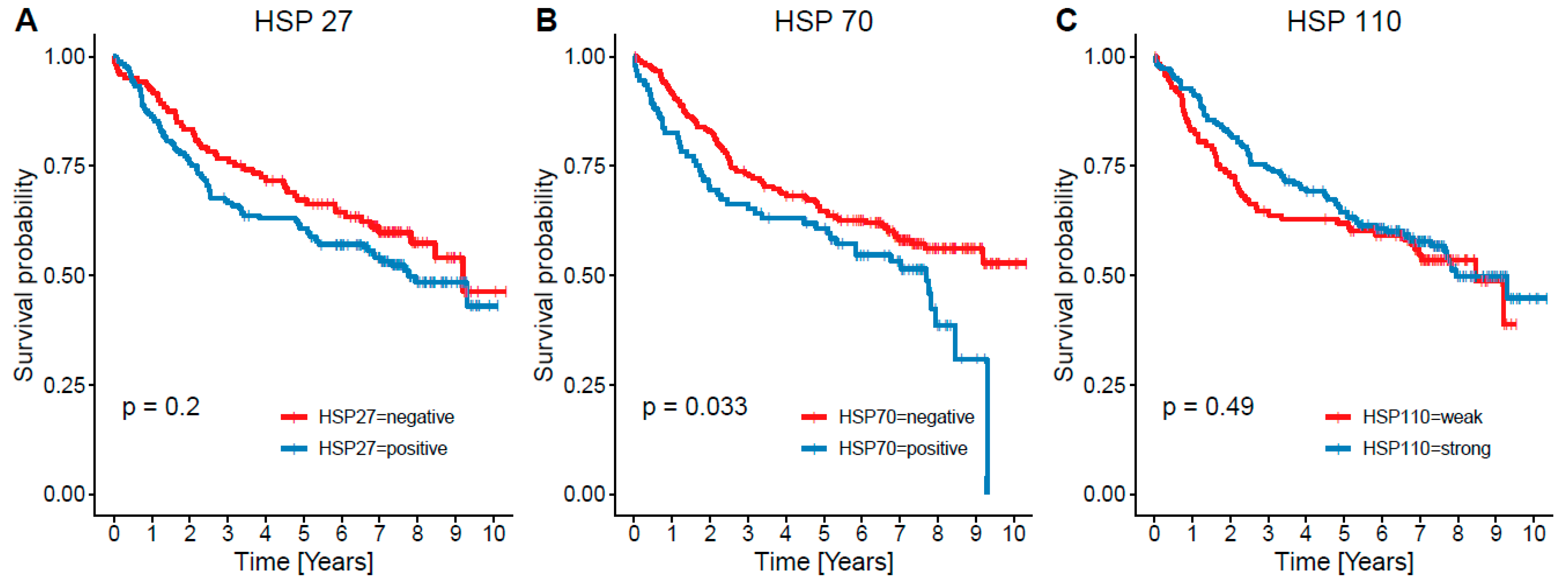
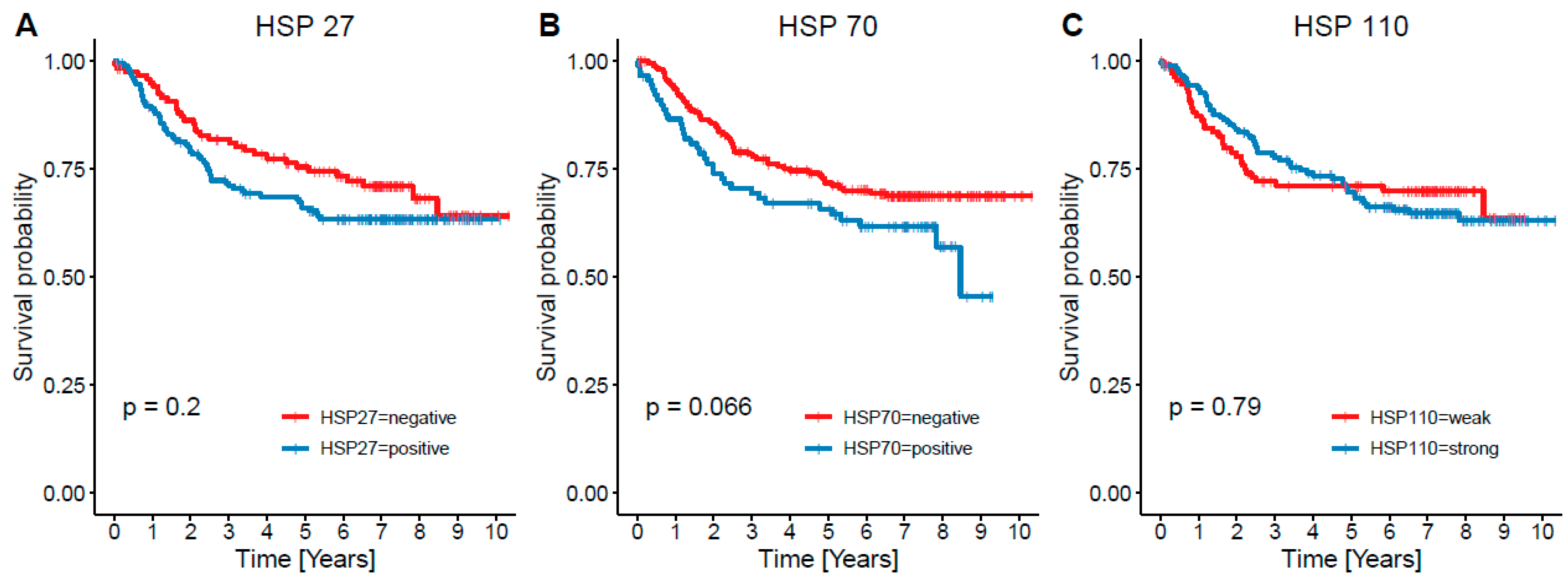
3.1. HSP27
3.2. HSP70
3.3. HSP110
3.4. Traditional Parameters
3.5. Multivariate Cox Regression
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Cronin, K.A.; Bs, A.J.L.; Scott, S.; Sherman, R.L.; Noone, A.-M.; Ms, N.H.; Henley, S.J.; Anderson, R.N.; Bs, A.U.F.; Ma, J.; et al. Annual Report to the Nation on the Status of Cancer, part I: National cancer statistics. Cancer 2018, 124, 2785–2800. [Google Scholar] [CrossRef] [Green Version]
- Pockley, A.G. Heat shock proteins, inflammation, and cardiovascular disease. Circulation 2002, 105, 1012–1017. [Google Scholar] [CrossRef] [Green Version]
- Saini, J.; Sharma, P.K. Clinical, Prognostic and Therapeutic Significance of Heat Shock Proteins in Cancer. Curr. Drug Targets 2018, 19, 1478–1490. [Google Scholar] [CrossRef]
- Chakraborty, P.K.; Mustafi, S.B. Heat Shock Proteins: Heating Up Skin Cancer Biology. J. Dermat. 2016, 1, 102. [Google Scholar] [CrossRef]
- Lanneau, D.; Brunet, M.; Frisan, E.; Solary, E.; Fontenay, M.; Garrido, C. Heat shock proteins: Essential proteins for apoptosis regulation. J. Cell. Mol. Med. 2008, 12, 743–761. [Google Scholar] [CrossRef] [Green Version]
- Chakafana, G.; Shonhai, A. The Role of Non-Canonical HSP70s (HSP110/Grp170) in Cancer. Cells 2021, 10, 254. [Google Scholar] [CrossRef]
- Eseigneuric, R.; Emjahed, H.; Egobbo, J.; Ejoly, A.-L.; Berthenet, K.; Eshirley, S.; Egarrido, C. Heat shock proteins as danger signals for cancer detection. Front. Oncol. 2011, 1, 37. [Google Scholar] [CrossRef] [Green Version]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumors, 8th ed.; Wiley Blackwell: Hoboken, NJ, USA, 2017; pp. 73–76. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019; Available online: https://www.R-project.org/ (accessed on 1 November 2020).
- Therneau, T. A Package for Survival Analysis in R. Version 3.1–7. 2015. Available online: https://CRAN.R-project.org/package=survival (accessed on 1 November 2020).
- Acunzo, J.; Katsogiannou, M.; Rocchi, P. Small heat shock proteins HSP27 (HSPB1), αB-crystallin (HSPB5) and HSP22 (HSPB8) as regulators of cell death. Int. J. Biochem. Cell Biol. 2012, 44, 1622–1631. [Google Scholar] [CrossRef]
- Têtu, B.; Brisson, J.; Landry, J.; Huot, J. Prognostic significance of heat-shock protein-27 in node-positive breast carcinoma: An immunohistochemical study. Breast Cancer Res. Treat. 1995, 36, 93–97. [Google Scholar] [CrossRef]
- Giaginis, C.; Daskalopoulou, S.S.; Vgenopoulou, S.; Sfiniadakis, I.; Kouraklis, G.; E Theocharis, S. Heat Shock Protein-27, -60 and -90 expression in gastric cancer: Association with clinicopathological variables and patient survival. BMC Gastroenterol. 2009, 9, 14. [Google Scholar] [CrossRef] [Green Version]
- Zagorianakou, N.; Ioachim, E.; Mitselou, A.; Kitsou, E.; Zagorianakou, P.; Makrydimas, G.; Salmas, M.; Agnantis, N.J. Immunohistochemical expression of heat shock protein 27, in normal hyperplastic and neoplastic endometrium: Correlation with estrogen and progesterone receptor status, p53, pRb and proliferation associated indices (PCNA, MIB1). Eur. J. Gynaecol. Oncol. 2003, 24, 299–304. [Google Scholar] [PubMed]
- Feng, J.-T.; Liu, Y.-K.; Song, H.-Y.; Dai, Z.; Qin, L.-X.; Almofti, M.R.; Fang, C.-Y.; Lu, H.-J.; Yang, P.-Y.; Tang, Z.-Y. Heat-shock protein 27: A potential biomarker for hepatocellular carcinoma identified by serum proteome analysis. Proteomics 2005, 5, 4581–4588. [Google Scholar] [CrossRef]
- Wang, R.-C.; Huang, C.-Y.; Pan, T.-L.; Chen, W.-Y.; Ho, C.-T.; Liu, T.-Z.; Chang, Y.-J. Proteomic Characterization of Annexin l (ANX1) and Heat Shock Protein 27 (HSP27) as Biomarkers for Invasive Hepatocellular Carcinoma Cells. PLoS ONE 2015, 10, e0139232. [Google Scholar] [CrossRef] [Green Version]
- Storm, F.; Mahvi, D.M.; Gilchrist, K.W. HSP-27 has no diagnostic or prognostic significance in prostate or bladder cancers. Urology 1993, 42, 379–382. [Google Scholar] [CrossRef]
- A Cornford, P.; Dodson, A.R.; Parsons, K.F.; Desmond, A.D.; Woolfenden, A.; Fordham, M.; Neoptolemos, J.; Ke, Y.; Foster, C.S. Heat shock protein expression independently predicts clinical outcome in prostate cancer. Cancer Res. 2000, 60, 7099–7105. [Google Scholar] [PubMed]
- Glaessgen, A.; Jonmarker, S.; Lindberg, A.; Nilsson, B.; Lewensohn, R.; Ekman, P.; Valdman, A.; Egevad, L. Heat shock proteins 27, 60 and 70 as prognostic markers of prostate cancer. APMIS 2008, 116, 888–895. [Google Scholar] [CrossRef] [PubMed]
- Rocchi, P.; So, A.; Kojima, S.; Signaevsky, M.; Beraldi, E.; Fazli, L.; Hurtado-Coll, A.; Yamanaka, K.; Gleave, M. Heat shock protein 27 increases after androgen ablation and plays a cytoprotective role in hormone-refractory prostate cancer. Cancer Res. 2004, 64, 6595–6602. [Google Scholar] [CrossRef] [Green Version]
- Thomas, X.; Campos, L.; Mounier, C.; Cornillon, J.; Flandrin, P.; Le, Q.-H.; Piselli, S.; Guyotat, D. Expression of heat-shock proteins is associated with major adverse prognostic factors in acute myeloid leukemia. Leuk. Res. 2005, 29, 1049–1058. [Google Scholar] [CrossRef]
- Assimakopoulou, M. Human meningiomas: Immunohistochemical localization of progesterone receptor and heat shock protein 27 and absence of estrogen receptor and PS2. Cancer Detect. Prev. 2000, 24, 163–168. [Google Scholar]
- Wang, A.; Liu, X.; Sheng, S.; Ye, H.; Peng, T.; Shi, F.; Crowe, D.L.; Zhou, X. Dysregulation of heat shock protein 27 expression in oral tongue squamous cell carcinoma. BMC Cancer 2009, 9, 167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geisler, J.P.; E Tammela, J.; Manahan, K.J.; E Geisler, H.; A Miller, G.; Zhou, Z.; Wiemann, M.C. HSP27 in patients with ovarian carcinoma: Still an independent prognostic indicator at 60 months follow-up. Eur. J. Gynaecol. Oncol. 2004, 25, 165–168. [Google Scholar]
- Bauer, K.; Nitsche, U.; Slotta-Huspenina, J.; Drecoll, E.; Von Weyhern, C.H.; Rosenberg, R.; Höfler, H.; Langer, R. High HSP27 and HSP70 expression levels are independent adverse prognostic factors in primary resected colon cancer. Cell. Oncol. 2012, 35, 197–205. [Google Scholar] [CrossRef]
- Yu, Z.; Zhi, J.; Peng, X.; Zhong, X.; Xu, A. Clinical significance of HSP27 expression in colorectal cancer. Mol. Med. Rep. 2010, 3, 953–958. [Google Scholar] [CrossRef] [PubMed]
- Tweedle, E.M.; Khattak, I.; Ang, C.W.; Nedjadi, T.; Jenkins, R.; Park, B.K.; Kalirai, H.; Dodson, A.; Azadeh, B.; Terlizzo, M.; et al. Low molecular weight heat shock protein HSP27 is a prognostic indicator in rectal cancer but not colon cancer. Gut 2010, 59, 1501–1510. [Google Scholar] [CrossRef]
- Zhao, L.; Li, Z.-G.; Ding, Y.-Q. Expression of HSP27 in colorectal carcinoma and its relationship with lymphatic metastasis. Nan Fang Yi Ke Da Xue Xue Bao 2008, 28, 41–44. [Google Scholar] [PubMed]
- Choi, S.-K.; Kam, H.; Kim, K.-Y.; Park, S.I.; Lee, Y.-S. Targeting Heat Shock Protein 27 in Cancer: A Druggable Target for Cancer Treatment? Cancers 2019, 11, 1195. [Google Scholar] [CrossRef] [Green Version]
- Katsogiannou, M.; Andrieu, C.; Baylot, V.; Baudot, A.; Dusetti, N.; Gayet, O.; Finetti, P.; Garrido, C.; Birnbaum, D.; Bertucci, F.; et al. The Functional Landscape of Hsp27 Reveals New Cellular Processes such as DNA Repair and Alternative Splicing and Proposes Novel Anticancer Targets. Mol. Cell. Proteom. 2014, 13, 3585–3601. [Google Scholar] [CrossRef] [Green Version]
- Sakai, A.; Otani, M.; Miyamoto, A.; Yoshida, H.; Furuya, E.; Tanigawa, N. Identification of phosphorylated serine-15 and -82 residues of HSPB1 in 5-fluorouracil-resistant colorectal cancer cells by proteomics. J. Proteom. 2012, 75, 806–818. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, R.; Ishii, Y.; Ochiai, H.; Matsunaga, A.; Endo, T.; Hasegawa, H.; Kitagawa, Y. Suppression of heat shock protein 27 expression promotes 5-fluorouracil sensitivity in colon cancer cells in a xenograft model. Oncol. Rep. 2012, 28, 1269–1274. [Google Scholar] [CrossRef] [Green Version]
- Chatterjee, S.; Burns, T.F. Targeting Heat Shock Proteins in Cancer: A Promising Therapeutic Approach. Int. J. Mol. Sci. 2017, 18, 1978. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.-F.; Nieh, S.; Jao, S.-W.; Liu, C.-L.; Wu, C.-H.; Chang, Y.-C.; Yang, C.-Y.; Lin, Y.-S. Quercetin suppresses drug-resistant spheres via the p38 MAPK–HSP27 apoptotic pathway in oral cancer cells. PLoS ONE 2012, 7, e49275. [Google Scholar] [CrossRef] [Green Version]
- Gibert, B.; Hadchity, E.; Czekalla, A.; Aloy, M.-T.; Colas, P.; Rodriguez-Lafrasse, C.; Arrigo, A.-P.; Diaz-Latoud, C. Inhibition of heat shock protein 27 (HSPB1) tumorigenic functions by peptide aptamers. Oncogene 2011, 30, 3672–3681. [Google Scholar] [CrossRef] [Green Version]
- Heinrich, J.-C.; Tuukkanen, A.; Schroeder, M.; Fahrig, T.; Fahrig, R. RP101 (brivudine) binds to heat shock protein HSP27 (HSPB1) and enhances survival in animals and pancreatic cancer patients. J. Cancer Res. Clin. Oncol. 2011, 137, 1349–1361. [Google Scholar] [CrossRef]
- Choi, S.-H.; Lee, Y.-J.; Seo, W.D.; Lee, H.-J.; Nam, J.-W.; Kim, J.; Seo, E.-K.; Lee, Y.-S.; Lee, Y.J. Altered cross-linking of HSP27 by zerumbone as a novel strategy for overcoming hsp27-mediated radioresistance. Int. J. Radiat. Oncol. 2011, 79, 1196–1205. [Google Scholar] [CrossRef]
- Asaum, J.; Matsuzaki, H.; Kawasak, S.; Kuroda, M.; Takeda, Y.; Kishi, K.; Hiraki, Y. Effects of quercetin on the cell growth and the intracellular accumulation and retention of adriamycin. Anticancer Res. 2000, 20, 2477–2483. [Google Scholar]
- Elattar, T.M.; Virji, A.S. The inhibitory effect of curcumin, genistein, quercetin and cisplatin on the growth of oral cancer cells in vitro. Anticancer Res. 2000, 20, 1733–1738. [Google Scholar]
- Hosokawa, N.; Hirayoshi, K.; Kudo, H.; Takechi, H.; Aoike, A.; Kawai, K.; Nagata, K. Inhibition of the activation of heat shock factor in vivo and in vitro by flavonoids. Mol. Cell. Biol. 1992, 12, 3490–3498. [Google Scholar] [CrossRef] [Green Version]
- Jacquemin, G.; Granci, V.; Gallouet, A.S.; Lalaoui, N.; Morle, A.; Iessi, E.; Morizot, A.; Garrido, C.; Guillaudeux, T.; Micheau, O. Quercetin-mediated Mcl-1 and survivin downregulation restores TRAIL-induced apoptosis in non-Hodgkin’s lymphoma B cells. Haematologica 2011, 97, 38–46. [Google Scholar] [CrossRef] [Green Version]
- Knowles, L.M.; Zigrossi, D.A.; Tauber, R.A.; Hightower, C.; Milner, J.A. Flavonoids suppress androgen-independent human prostate tumor proliferation. Nutr. Cancer 2000, 38, 116–122. [Google Scholar] [CrossRef]
- Nagai, N.; Nakai, A.; Nagata, K. Quercetin Suppresses Heat Shock Response by Down-Regulation of HSF1. Biochem. Biophys. Res. Commun. 1995, 208, 1099–1105. [Google Scholar] [CrossRef] [PubMed]
- Kamada, M.; So, A.; Muramaki, M.; Rocchi, P.; Beraldi, E.; Gleave, M. Hsp27 knockdown using nucleotide-based therapies inhibit tumor growth and enhance chemotherapy in human bladder cancer cells. Mol. Cancer Ther. 2007, 6, 299–308. [Google Scholar] [CrossRef] [Green Version]
- Kumano, M.; Furukawa, J.; Shiota, M.; Zardan, A.; Zhang, F.; Beraldi, E.; Wiedmann, R.M.; Fazli, L.; Zoubeidi, A.; Gleave, M.E. Cotargeting Stress-Activated Hsp27 and Autophagy as a Combinatorial Strategy to Amplify Endoplasmic Reticular Stress in Prostate Cancer. Mol. Cancer Ther. 2012, 11, 1661–1671. [Google Scholar] [CrossRef] [Green Version]
- Hsu, H.-S.; Lin, J.-H.; Huang, W.-C.; Hsu, T.-W.; Su, K.; Chiou, S.-H.; Tsai, Y.-T.; Hung, S.-C. Chemoresistance of lung cancer stemlike cells depends on activation of Hsp27. Cancer 2010, 117, 1516–1528. [Google Scholar] [CrossRef]
- Lelj-Garolla, B.; Kumano, M.; Beraldi, E.; Nappi, L.; Rocchi, P.; Ionescu, D.N.; Fazli, L.; Zoubeidi, A.; Gleave, M.E. Hsp27 Inhibition with OGX-427 Sensitizes Non–Small Cell Lung Cancer Cells to Erlotinib and Chemotherapy. Mol. Cancer Ther. 2015, 14, 1107–1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravagnan, L.; Gurbuxani, S.; Susin, S.A.; Maisse, C.; Daugas, E.; Zamzami, N.; Mak, T.; Jäättelä, M.; Penninger, J.; Garrido, C.; et al. Heat-shock protein 70 antagonizes apoptosis-inducing factor. Nat. Cell Biol. 2001, 3, 839–843. [Google Scholar] [CrossRef]
- Garg, M.; Kanojia, D.; Saini, S.; Suri, S.; Gupta, A.; Surolia, A.; Suri, A. Germ cell-specific heat shock protein 70-2 is expressed in cervical carcinoma and is involved in the growth, migration, and invasion of cervical cells. Cancer 2010, 116, 3785–3796. [Google Scholar] [CrossRef] [PubMed]
- Garg, M.; Kanojia, D.; Seth, A.; Kumar, R.; Gupta, A.; Surolia, A.; Suri, A. Heat-shock protein 70-2 (HSP70-2) expression in bladder urothelial carcinoma is associated with tumour progression and promotes migration and invasion. Eur. J. Cancer 2010, 46, 207–215. [Google Scholar] [CrossRef]
- Piszcz, J.; Bolkun, Ł.; Cichocka, E.; Galar, M.; Hołownia, A.; Kłoczko, J. Prognostic relevance of HSP70 antigen and antibody measurement in patients with acute myeloid leukemia of intermediate and unfavorable cytogenetic risk. Pol. Arch. Intern. Med. 2014, 124, 165–172. [Google Scholar] [CrossRef]
- Kocsis, J.; Madaras, B.; Tóth, É.K.; Füst, G.; Prohászka, Z. Serum level of soluble 70-kD heat shock protein is associated with high mortality in patients with colorectal cancer without distant metastasis. Cell Stress Chaperones 2010, 15, 143–151. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.W.; Lee, E.H.; Kim, S.-H.; Roh, M.S.; Jung, S.B.; Choi, Y.C. Heat shock protein 70 (HSP70) expression is associated with poor prognosis in intestinal type gastric cancer. Virchows Arch. 2013, 463, 489–495. [Google Scholar] [CrossRef]
- Gunther, S.; Ostheimer, C.; Stangl, S.; Specht, H.M.; Mozes, P.; Jesinghaus, M.; Vordermark, D.; Combs, S.; Peltz, F.; Jung, M.P.; et al. Correlation of HSP70 Serum Levels with Gross Tumor Volume and Composition of Lymphocyte Subpopulations in Patients with Squamous Cell and Adeno Non-Small Cell Lung Cancer. Front. Immunol. 2015, 6, 556. [Google Scholar] [CrossRef] [Green Version]
- Tavassol, F.; Starke, O.F.; Kokemüller, H.; Wegener, G.; Müller-Tavassol, C.C.; Gellrich, N.-C.; Eckardt, A. Prognostic significance of heat shock protein 70 (HSP70) in patients with oral cancer. Head Neck Oncol. 2011, 3, 10. [Google Scholar] [CrossRef] [Green Version]
- Nakajima, M.; Kato, H.; Miyazaki, T.; Fukuchi, M.; Masuda, N.; Fukai, Y.; Sohda, M.; Ahmad, F.; Kuwano, H. Tumor immune systems in esophageal cancer with special reference to heat-shock protein 70 and humoral immunity. Anticancer Res. 2009, 29, 1595–1606. [Google Scholar]
- Pfister, K.; Radons, J.; Busch, R.; Tidball, J.G.; Pfeifer, M.; Freitag, L.; Feldmann, H.-J.; Milani, V.; Issels, R.; Multhoff, G. Patient survival by hsp70 membrane phenotype. Cancer 2007, 110, 926–935. [Google Scholar] [CrossRef]
- Steiner, K.; Graf, M.; Hecht, K.; Reif, S.; Rossbacher, L.; Pfister, K.; Kolb, H.-J.; Schmetzer, H.M.; Multhoff, G. High HSP70-membrane expression on leukemic cells from patients with acute myeloid leukemia is associated with a worse prognosis. Leukemia 2006, 20, 2076–2079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanazawa, Y.; Isomoto, H.; Oka, M.; Yano, Y.; Soda, H.; Shikuwa, S.; Takeshima, F.; Omagari, K.; Mizuta, Y.; Murase, K.; et al. Expression of Heat Shock Protein (Hsp) 70 and Hsp 40 in Colorectal Cancer. Med. Oncol. 2003, 20, 157–164. [Google Scholar] [CrossRef]
- Gao, G.; Liu, S.; Yao, Z.; Zhan, Y.; Chen, W.; Liu, Y. The Prognostic Significance of HSP70 in Patients with Colorectal Cancer Patients: A PRISMA-Compliant Meta-Analysis. BioMed Res. Int. 2021, 2021, 5526327. [Google Scholar] [CrossRef] [PubMed]
- Hwang, T.S.; Han, H.S.; Choi, H.K.; Lee, Y.J.; Kim, Y.-J.; Han, M.-Y.; Park, Y.-M. Differential, stage-dependent expression of Hsp70, Hsp110 and Bcl-2 in colorectal cancer. J. Gastroenterol. Hepatol. 2003, 18, 690–700. [Google Scholar] [CrossRef]
- Cai, M.-B.; Wang, X.-P.; Zhang, J.-X.; Han, H.-Q.; Liu, C.-C.; Bei, J.-X.; Peng, R.-J.; Liang, Y.; Feng, Q.-S.; Wang, H.-Y.; et al. Expression of heat shock protein 70 in nasopharyngeal carcinomas: Different expression patterns correlate with distinct clinical prognosis. J. Transl. Med. 2012, 10, 96. [Google Scholar] [CrossRef] [Green Version]
- Slaby, O.; Sobkova, K.; Svoboda, M.; Garajova, I.; Fabian, P.; Hrstka, R.; Nenutil, R.; Sachlova, M.; Kocakova, I.; Michalek, J.; et al. Significant overexpression of HSP110 gene during colorectal cancer progression. Oncol. Rep. 2009, 21, 1235–1241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berthenet, K.; Bokhari, A.; Lagrange, A.; Marcion, G.; Boudesco, C.; Causse, S.; De Thonel, A.; Svrcek, M.; Goloudina, A.R.; Dumont, S.; et al. HSP110 promotes colorectal cancer growth through STAT3 activation. Oncogene 2017, 36, 2328–2336. [Google Scholar] [CrossRef] [PubMed]
- Berthenet, K.; Boudesco, C.; Collura, A.; Svrcek, M.; Richaud, S.; Hammann, A.; Causse, S.; Yousfi, N.; Wanherdrick, K.; Duplomb, L.; et al. Extracellular HSP110 skews macrophage polarization in colorectal cancer. Oncoimmunology 2016, 5, e1170264. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.H.; Kim, K.-J.; Rhee, Y.-Y.; Oh, S.; Cho, N.-Y.; Lee, H.S.; Kang, G.H. Expression status of wild-type HSP110 correlates with HSP110 T17 deletion size and patient prognosis in microsatellite-unstable colorectal cancer. Mod. Pathol. 2013, 27, 443–453. [Google Scholar] [CrossRef] [Green Version]
- Oh, H.J.; Kim, J.H.; Lee, T.H.; Park, H.E.; Bae, J.M.; Lee, H.S.; Kang, G.H. Dominant high expression of wild-type HSP110 defines a poor prognostic subgroup of colorectal carcinomas with microsatellite instability: A whole-section immunohistochemical analysis. APMIS 2017, 125, 1076–1083. [Google Scholar] [CrossRef]
- Kim, K.-J.; Lee, T.H.; Kim, J.H.; Cho, N.-Y.; Kim, W.H.; Kang, G.H. Deletion in HSP110 T17: Correlation with wild-type HSP110 expression and prognostic significance in microsatellite-unstable advanced gastric cancers. Hum. Pathol. 2017, 67, 109–118. [Google Scholar] [CrossRef]
- Popat, S.; Hubner, R.; Houlston, R. Systematic review of microsatellite instability and colorectal cancer prognosis. J. Clin. Oncol. 2005, 23, 609–618. [Google Scholar] [CrossRef]
- Kim, J.H.; Kang, G.H. Molecular and prognostic heterogeneity of microsatellite-unstable colorectal cancer. World J. Gastroenterol. 2014, 20, 4230–4243. [Google Scholar] [CrossRef] [PubMed]
- Kimura, A.; Ogata, K.; Altan, B.; Yokobori, T.; Ide, M.; Mochiki, E.; Toyomasu, Y.; Kogure, N.; Yanoma, T.; Suzuki, M.; et al. Nuclear heat shock protein 110 expression is associated with poor prognosis and chemotherapy resistance in gastric cancer. Oncotarget 2016, 7, 18415–18423. [Google Scholar] [CrossRef] [Green Version]
- Nakajima, M.; Kato, H.; Miyazaki, T.; Fukuchi, M.; Masuda, N.; Fukai, Y.; Sohda, M.; Inose, T.; Sakai, M.; Sano, A.; et al. Prognostic significance of heat shock protein 110 expression and T lymphocyte infiltration in esophageal cancer. Hepatogastroenterology 2011, 58, 1555–1560. [Google Scholar] [CrossRef]
- Ullmann, R.; Morbini, P.; Halbwedl, I.; Bongiovanni, M.; Gogg-Kammerer, M.; Papotti, M.; Gabor, S.; Renner, H.; Popper, H.H. Protein expression profiles in adenocarcinomas and squamous cell carcinomas of the lung generated using tissue microarrays. J. Pathol. 2004, 203, 798–807. [Google Scholar] [CrossRef] [PubMed]
- Fan, G.; Tu, Y.; Wu, N.; Xiao, H. The expression profiles and prognostic values of HSPs family members in Head and neck cancer. Cancer Cell Int. 2020, 20, 220. [Google Scholar] [CrossRef]
- Gotoh, K.; Nonoguchi, K.; Higashitsuji, H.; Kaneko, Y.; Sakurai, T.; Sumitomo, Y.; Itoh, K.; Subjeck, J.R.; Fujita, J. Apg-2 has a chaperone-like activity similar to HSP110 and is overexpressed in hepatocellular carcinomas. FEBS Lett. 2004, 560, 19–24. [Google Scholar] [CrossRef] [Green Version]
- Muchemwa, F.C.; Nakatsura, T.; Fukushima, S.; Nishimura, Y.; Kageshita, T.; Ihn, H. Differential expression of heat shock protein 105 in melanoma and melanocytic naevi. Melanoma Res. 2008, 18, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, Y.; Yoshikawa, T.; Kojima, T.; Shoda, K.; Nosaka, K.; Mizuno, S.; Wada, S.; Fujimoto, Y.; Sasada, T.; Kohashi, K.; et al. Heat shock protein 105 peptide vaccine could induce antitumor immune reactions in a phase I clinical trial. Cancer Sci. 2019, 110, 3049–3060. [Google Scholar] [CrossRef] [Green Version]
- Jagadish, N.; Parashar, D.; Gupta, N.; Agarwal, S.; Suri, V.; Kumar, R.; Suri, V.; Sadasukhi, T.C.; Gupta, A.; Ansari, A.S.; et al. Heat shock protein 70–2 (HSP70-2) is a novel therapeutic target for colorectal cancer and is associated with tumor growth. BMC Cancer 2016, 16, 561. [Google Scholar] [CrossRef] [Green Version]
- Jourdan, F.; Sebbagh, N.; Comperat, E.; Mourra, N.; Flahault, A.; Olschwang, S.; Duval, A.; Hamelin, R. Tissue microarray technology: Validation in colorectal carcinoma and analysis of p53, hMLH1, and hMSH2 immunohistochemical expression. Virchows Arch. 2003, 443, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Yahagi, M.; Okabayashi, K.; Hasegawa, H.; Tsuruta, M.; Kitagawa, Y. The Worse Prognosis of Right-Sided Compared with Left-Sided Colon Cancers: A Systematic Review and Meta-analysis. J. Gastrointest. Surg. 2015, 20, 648–655. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| - | HSP27+ | HSP27- | HSP70+ | HSP70- | HSP110+ | HSP110- |
|---|---|---|---|---|---|---|
| Age group | - | - | - | - | - | - |
| <50 | 12 (6.8%) | 3 (2.5%) | 6 (6.5%) | 9 (4.3%) | 11 (6.2%) | 2 (1.8%) |
| 50–59 | 28 (15.9%) | 13 (10.8%) | 17 (18.5%) | 24 (11.7%) | 29 (16.3%) | 12 (10.5%) |
| 60–69 | 56 (31.8%) | 41 (34.2%) | 29 (31.5%) | 69 (33.7%) | 57 (32.0%) | 38 (33.3%) |
| 70–79 | 49 (27.8%) | 39 (32.5%) | 21 (22.8%) | 67 (32.7%) | 48 (27.0%) | 40 (35.1%) |
| 80+ | 31 (17.6%) | 24 (20%) | 19 (20.7%) | 36 (17.6%) | 33 (18.5%) | 22 (19.3%) |
| - | p = 0.307 | - | p = 0.270 | - | p = 0.179 | - |
| Gender | - | - | - | - | - | - |
| F | 88 (50%) | 42 (35%) | 41 (45%) | 89 (43%) | 80 (45%) | 48 (42%) |
| M | 88 (50%) | 78 (65%) | 51 (55%) | 116 (57%) | 98 (55%) | 66 (58%) |
| - | p = 0.015 | - | p = 0.953 | - | p = 0.722 | - |
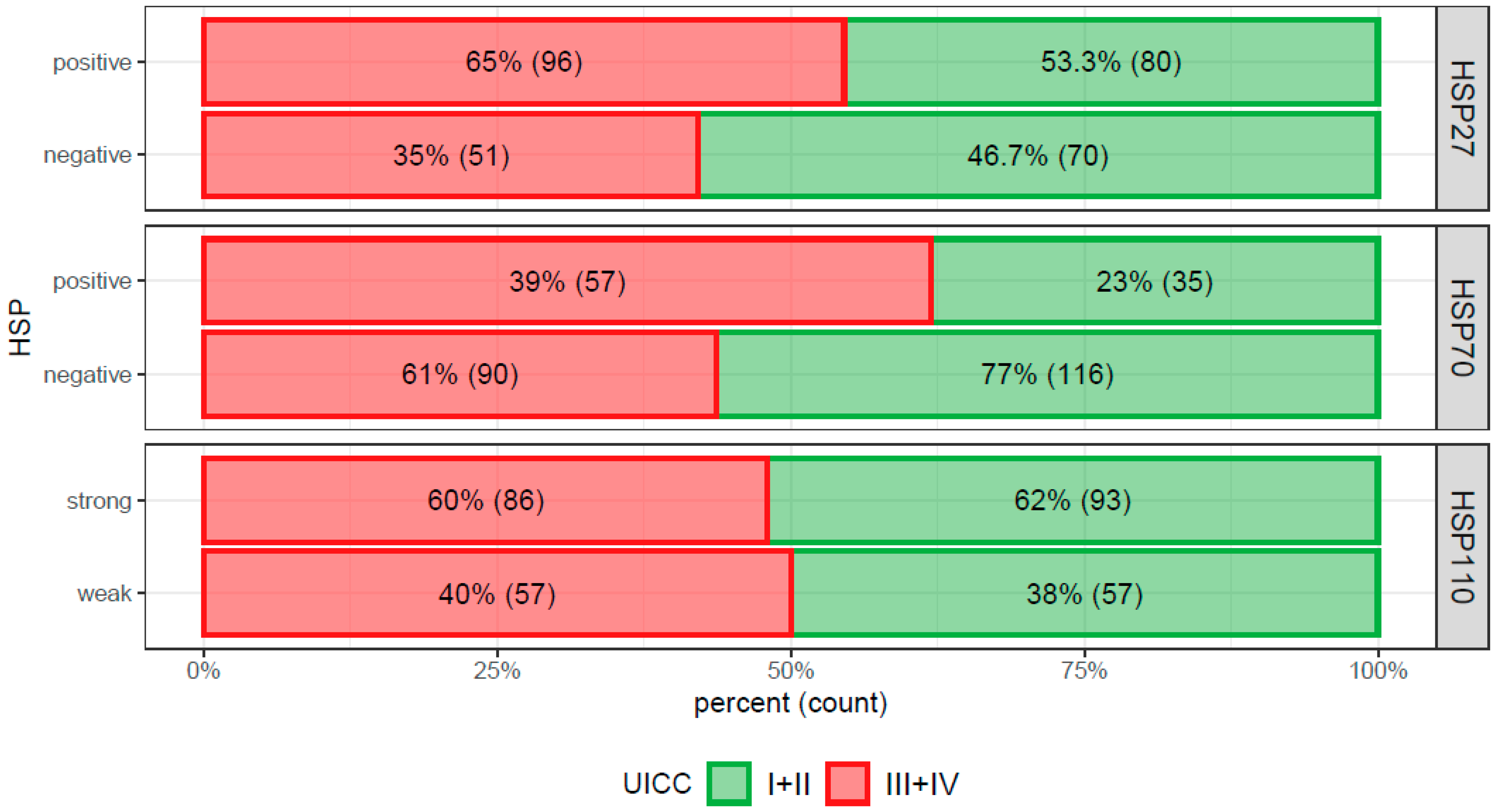
| UICC stage | - | - | - | - | - | - |
| I + II | 80 (45.5%) | 70 (58%) | 35 (38%) | 116 (56%) | 93 (52%) | 57 (50%) |
| III + IV | 96 (54.5%) | 51 (42%) | 57 (62%) | 90 (44%) | 86 (48%) | 57 (50%) |
| - | p = 0.048 | - | p = 0.005 | - | p = 0.836 | - |
| Side | - | - | - | - | - | - |
| right | 65 (37%) | 52 (43%) | 30 (33%) | 87 (42%) | 61 (34%) | 55 (48.2%) |
| left | 111 (63%) | 68 (57%) | 61 (67%) | 119 (58%) | 118 (66%) | 59 (51.8%) |
| - | p = 0.325 | - | p = 0.168 | - | p = 0.022 | - |
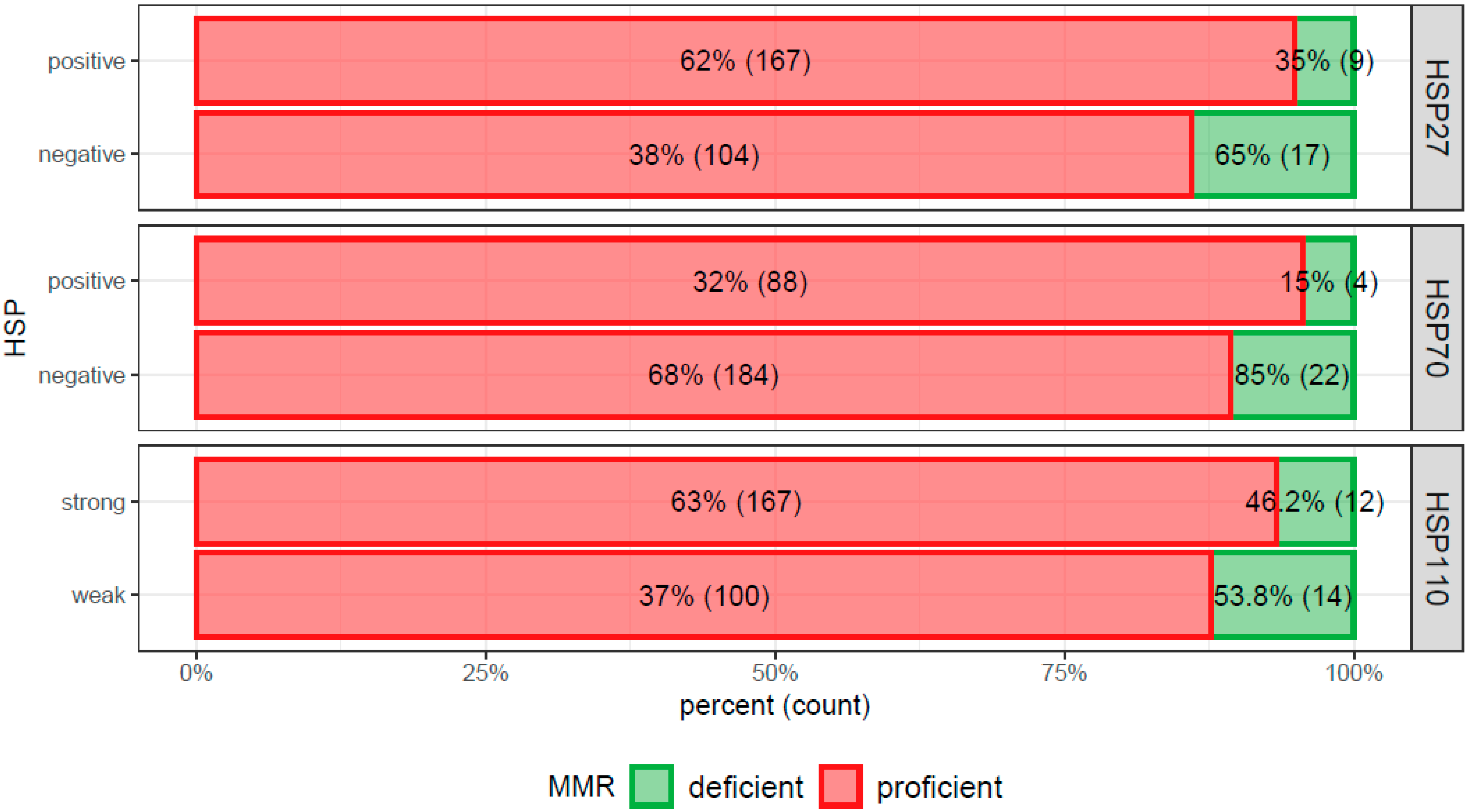
| MMR | - | - | - | - | - | - |
| Deficient | 9 (5%) | 17 (14%) | 4 (4%) | 22 (11%) | 12 (7%) | 14 (12%) |
| Proficient | 167 (95%) | 104 (86%) | 88 (96%) | 184 (89%) | 167 (93%) | 100 (88%) |
| - | p = 0.013 | - | p = 0.117 | - | p = 0.154 | - |
| Grade | - | - | - | - | - | - |
| low grade (1 + 2) | 124 (74%) | 88 (79%) | 68 (79%) | 145 (75%) | 131 (78%) | 79 (74%) |
| high grade (3) | 43 (26%) | 24 (21%) | 18 (21%) | 49 (25%) | 37 (22%) | 28 (26%) |
| - | p = 0.493 | - | p = 0.528 | - | p = 0.520 | - |
| Morphology | - | - | - | - | - | - |
| mucinous + signet ring | 11 (6%) | 7 (6%) | 2 (2%) | 16 (8%) | 9 (5%) | 7 (6%) |
| NOS | 165 (94%) | 114 (94%) | 90 (98%) | 190 (92%) | 170 (95%) | 107 (94%) |
| - | p = 1 | - | p = 0.061 | - | p = 0.885 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hrudka, J.; Jelínková, K.; Fišerová, H.; Matěj, R.; Mandys, V.; Waldauf, P. Heat Shock Proteins 27, 70, and 110: Expression and Prognostic Significance in Colorectal Cancer. Cancers 2021, 13, 4407. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13174407
Hrudka J, Jelínková K, Fišerová H, Matěj R, Mandys V, Waldauf P. Heat Shock Proteins 27, 70, and 110: Expression and Prognostic Significance in Colorectal Cancer. Cancers. 2021; 13(17):4407. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13174407
Chicago/Turabian StyleHrudka, Jan, Karolína Jelínková, Hana Fišerová, Radoslav Matěj, Václav Mandys, and Petr Waldauf. 2021. "Heat Shock Proteins 27, 70, and 110: Expression and Prognostic Significance in Colorectal Cancer" Cancers 13, no. 17: 4407. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13174407