
The Evolution and Prognostic Role of Tumour-Infiltrating Lymphocytes and Peripheral Blood-Based Biomarkers in Inflammatory Breast Cancer Patients Treated with Neoadjuvant Chemotherapy

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors (Year of Publication) | N | Subtype of BC | Type of NACT | Number of sTIL (Pre & Post-NACT) | Change in sTIL after NACT | Correlation between Post-NACT sTIL and Clinicopathological Parameters | Prognostic Effect of Post-NACT sTIL |
|---|---|---|---|---|---|---|---|
| Campedel et al. (2020) [11] | 31 | TN IBC | Anthracycline Taxane-based | Median Pre: 10% Median Post: 1.5% | Median delta TIL was −9% (−50% up to +40%) | Not reported | A positive delta TIL was significantly associated with a decrease of EFS. HR: 1.88; 95% CI: 1.05–3.35; p = 0.01 |
| Lee et al. (2020) [22] | 104 | TNBC | Anthracycline Taxane-based | Mean Pre: 23.3 ± 20.8% Mean Post: 17.1 ± 24.2% | Mean delta TIL: −2.69% - Decrease: 41.3% - No change: 30.8% - Increase: 27.9% | pT stage after NACT | RFS: Positive, HR:0.979, 95% CI: 0.961–0.997, p = 0.023 Change in sTIL level is associated with an increase in RFS: Decrease vs. no change: HR: 0.439, 95% CI: 0.228–0.846, p = 0.014; Increase vs. no change HR: 0.359, 95% CI: 0.158–0.814 p = 0.014) |
| Ochi et al. (2019) [23] | 209 | 80 TNBC 129 HER2+ | Anthracycline Taxane-based | Mean TNBC-Pre: <10%: 31.3% ≥10%: 68.7% TNBC-Post: <10%: 41.8% ≥10%: 58.2% Mean HER2+-Pre: <10%: 38.8% ≥10%: 61.2% HER2+-Post: <10%: 66.7% ≥10%: 33.3% | TNBC: - Increase: 12.7% - No change: 70.9% - Decrease: 16.4% HER2+ BC: - Increase: 4.0% - No change: 76.0% - Decrease: 20.0% | Not reported | RFS: Positive, HR: 2.836, 95% CI: 0.951–8.457, p = 0.06 (only in TNBC) The change in TILs was not associated with RFS. |
| Luen et al. (2019) [8] | 375 | TNBC | Anthracycline Taxane-based (in 62%) | Median Post: 20% | Increase: 48% Decrease: 47% Mean delta TIL: −3% | sTIL levels were significantly lower with increasing post-NACT tumour size and nodal stage, but did not differ by RCB class. | RFS: Positive, HR: 0.86; 95% CI: 0.79–0.92; p < 0.001 OS: Positive, HR: 0.87; 95% CI: 0.80–0.94; p < 0.001 |
| Hwang et al. (2019) [24] | 204 | All subtypes (25% HER2, 31% TN) | Taxane Platinum-based | Median Pre: 14.6% Median post: 10.2%. | Decrease: 44% No change: 39% Increase: 17% | A positive delta TIL was associated with smaller residual tumour size, negative nodal status, and lower RCBs. | High post-NACT sTIL levels (>50%) were associated with longer BCSS and DFS: BCSS: HR: 6.57, 95% CI: 0.87–19.57 p = 0.005 DFS: HR: 2.24, 95% CI: 0.81–5.48 p = 0.025 |
| Hamy et al. (2019) [10] | 718 | All subtypes (320 TN, 175 HER2+, 223 HR+ BC) | 85.0% Anthracycline Taxane-based 8.6% Anthracycline-based 3.2% Taxane-based | Mean pre-NACT: 24.2% (luminal: 16.2%; TNBC: 28.5%; HER2+: 26.5%; p < 0.001) Mean post-NACT: 13% (TNBC: 15.4%; luminal: 11.3%; HER2+: 10.9%, p < 0.001) | Decrease: 61.6% No change: 17.7% Increase: 20.7% | High post-NACT sTIL levels were associated with cellularity in HER2+ BC (p < 0.001) | High post-NACT sTIL levels were associated with impaired DFS in HER2-positive breast cancers (HR 1.04, CI 1.02–1.06, p = 0.001), but not in luminal tumours or TNBC. |
| Zhang et al. (2018) [25] | 58 | TNBC | Anthracycline Taxane-based | Two categories: (cut-off 60%) PRE - High sTIL: 7 - Low sTIL: 22 POST - High sTIL: 5 - Low sTIL: 24 | No statistically significant difference before and after NACT. | Not reported | Not reported |
| Pelekanou et al. (2017) [12] | 58 | All subtypes (79.3% HR+) | 56% Anthracycline Taxane-based | Median Pre: 5% Median Post: 7,5% | Delta sTIL: 5%. Trend towards increase in sTIL (p = 0.09) | Post-NACT sTIL were higher in ER-negative tumours (12.5%) than in ER-positive tumours (5%). | A positive delta TIL was significantly associated with an increase of EFS. HR: 3.9; CI 1.17–15.39; p = 0.02 |
| Castaneda et al. (2016) [26] | 80 | TNBC | 88% Anthracycline Taxane-based 9% Anthracycline -based 3% Taxane-based | Median Pre: 40% Median Post: 20% | Statistically significant decrease after NACT in median TIL percentage (p < 0.0002) | None | None |
| Dieci et al. (2014) [9] | 278 | TNBC | 48%Anthracycline-based 45% Anthracy cline/taxane-based | Two categories: (cut-off 60%) - High sTIL: 27 - Low sTIL: 251 | Pre-NACT slides available for 19 of the 27 patients with High sTIL RD. Change in sTIL: - Decrease: 1 patient - Increase: 18 patients | The presence of high TIL in RD was significantly associated with absence of metastatic axillary nodes and small tumour size (≤2 cm). | RFS: Positive, HR: 0.86, CI 0.79–0.92, p < 0.001 OS: Positive, HR: 0.86, CI 0.77–0.97, p = 0.01 |
2. Materials and Methods
2.1. Study Population
2.2. Blood-Based Biomarkers
2.3. Stromal Tumour-Infiltrating Lymphocytes (sTIL) and Cellularity in the Residual Tumour Bed
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
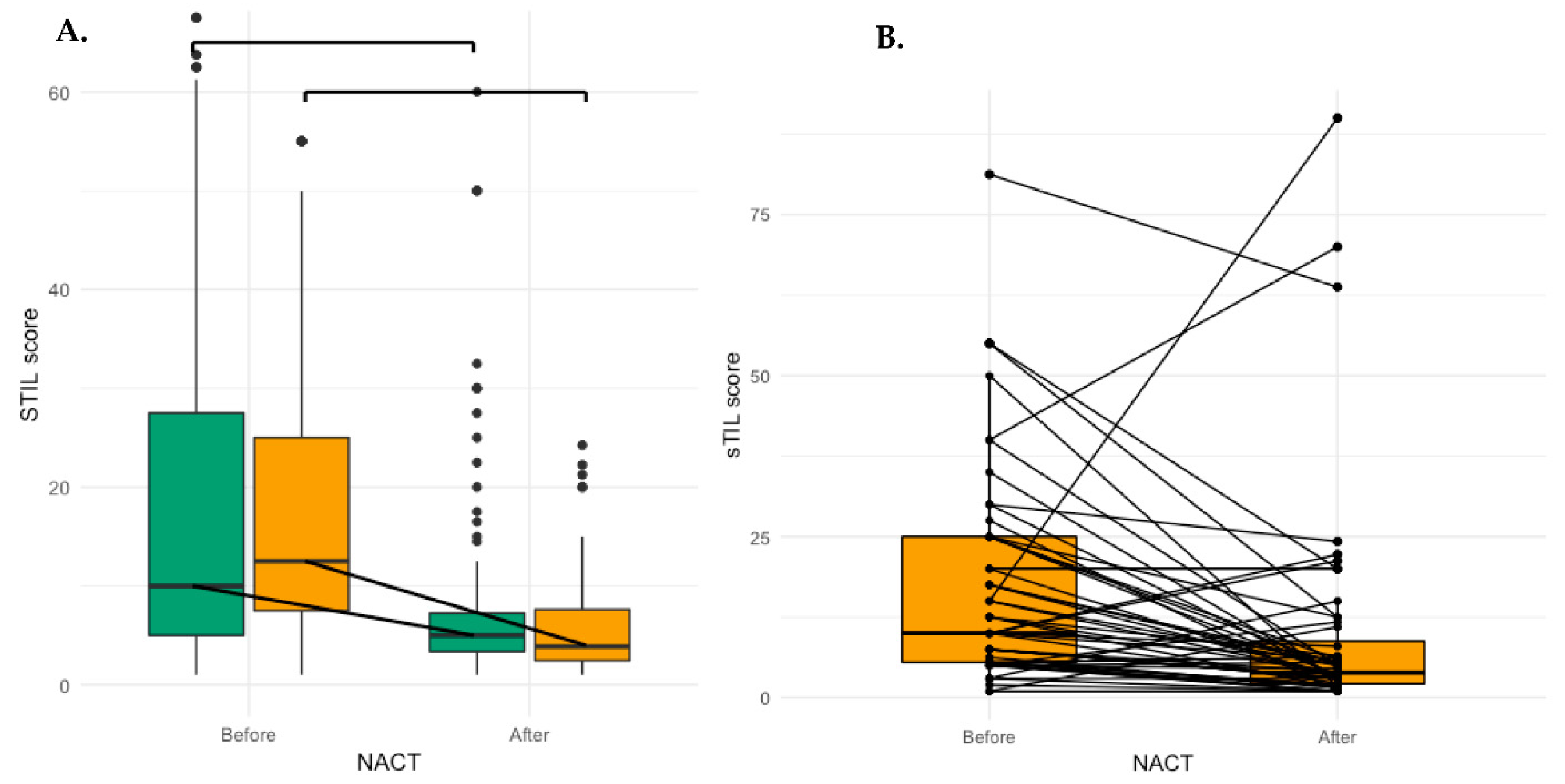
3.2. Evolution of sTIL after NACT
3.3. Evolution of Peripheral Blood-Based Biomarkers after NACT
3.4. Parameters Associated with Lower sTIL after NACT
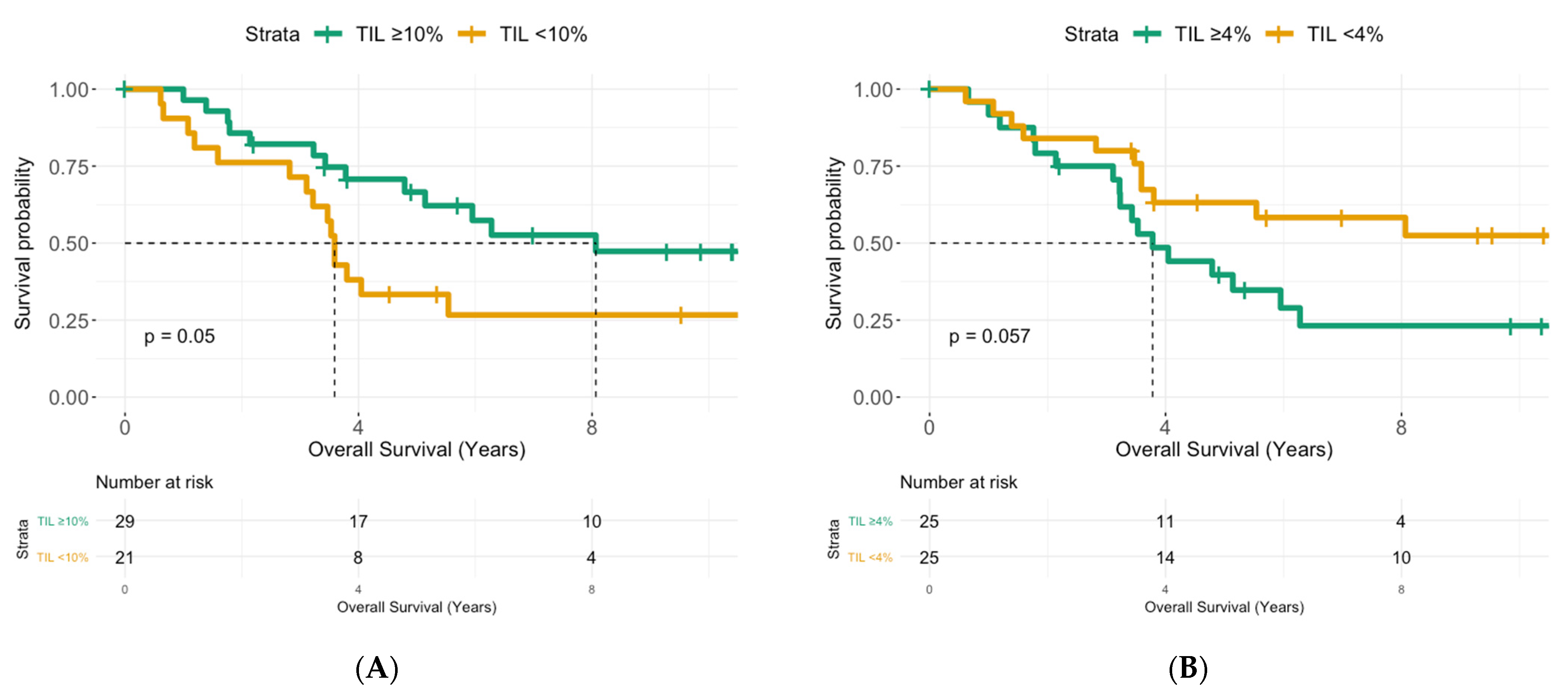
3.5. Prognostic Effects of sTIL and Peripheral Blood-Based Biomarkers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Copson, E.; Shaaban, A.M.; Maishman, T.; Moseley, P.M.; McKenzie, H.; Bradbury, J.; Borley, A.; Brzezinska, M.; Chan, S.; Ching, J.; et al. The presentation, management and outcome of inflammatory breast cancer cases in the UK: Data from a multi-centre retrospective review. Breast 2018, 42, 133–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woodward, W.A. Inflammatory breast cancer: Unique biological and therapeutic considerations. Lancet Oncol. 2015, 16, e568–e576. [Google Scholar] [CrossRef]
- Van Laere, S.J.; Ueno, N.T.; Finetti, P.; Vermeulen, P.; Lucci, A.; Robertson, F.M.; Marsan, M.; Iwamoto, T.; Krishnamurthy, S.; Masuda, H.; et al. Uncovering the molecular secrets of inflammatory breast cancer biology: An integrated analysis of three distinct affymetrix gene expression datasets. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2013, 19, 4685–4696. [Google Scholar] [CrossRef] [Green Version]
- Van Berckelaer, C.; Rypens, C.; van Dam, P.; Pouillon, L.; Parizel, M.; Schats, K.A.; Kockx, M.; Tjalma, W.A.A.; Vermeulen, P.; Van Laere, S.; et al. Infiltrating stromal immune cells in inflammatory breast cancer are associated with an improved outcome and increased PD-L1 expression. Breast Cancer Res. 2019, 21, 28. [Google Scholar] [CrossRef] [Green Version]
- Lim, B.; Woodward, W.A.; Wang, X.; Reuben, J.M.; Ueno, N.T. Inflammatory breast cancer biology: The tumour microenvironment is key. Nat. Rev. Cancer 2018, 18, 485–499. [Google Scholar] [CrossRef] [PubMed]
- Loi, S.; Drubay, D.; Adams, S.; Pruneri, G.; Francis, P.A.; Lacroix-Triki, M.; Joensuu, H.; Dieci, M.V.; Badve, S.; Demaria, S.; et al. Tumor-Infiltrating Lymphocytes and Prognosis: A Pooled Individual Patient Analysis of Early-Stage Triple-Negative Breast Cancers. J. Clin. Oncol. 2019, 37, 559–569. [Google Scholar] [CrossRef]
- Denkert, C.; von Minckwitz, G.; Darb-Esfahani, S.; Lederer, B.; Heppner, B.I.; Weber, K.E.; Budczies, J.; Huober, J.; Klauschen, F.; Furlanetto, J.; et al. Tumour-infiltrating lymphocytes and prognosis in different subtypes of breast cancer: A pooled analysis of 3771 patients treated with neoadjuvant therapy. Lancet Oncol. 2018, 19, 40–50. [Google Scholar] [CrossRef]
- Luen, S.J.; Salgado, R.; Dieci, M.V.; Vingiani, A.; Curigliano, G.; Gould, R.E.; Castaneda, C.; D’Alfonso, T.; Sanchez, J.; Cheng, E.; et al. Prognostic implications of residual disease tumor-infiltrating lymphocytes and residual cancer burden in triple-negative breast cancer patients after neoadjuvant chemotherapy. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol./ESMO 2019, 30, 236–242. [Google Scholar] [CrossRef] [Green Version]
- Dieci, M.V.; Criscitiello, C.; Goubar, A.; Viale, G.; Conte, P.; Guarneri, V.; Ficarra, G.; Mathieu, M.C.; Delaloge, S.; Curigliano, G.; et al. Prognostic value of tumor-infiltrating lymphocytes on residual disease after primary chemotherapy for triple-negative breast cancer: A retrospective multicenter study. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol./ESMO 2014, 25, 611–618. [Google Scholar] [CrossRef]
- Hamy, A.S.; Pierga, J.Y.; Sabaila, A.; Laas, E.; Bonsang-Kitzis, H.; Laurent, C.; Vincent-Salomon, A.; Cottu, P.; Lerebours, F.; Rouzier, R.; et al. Stromal lymphocyte infiltration after neoadjuvant chemotherapy is associated with aggressive residual disease and lower disease-free survival in HER2-positive breast cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol./ESMO 2017, 28, 2233–2240. [Google Scholar] [CrossRef]
- Campedel, L.; Blanc-Durand, P.; Bin Asker, A.; Lehmann-Che, J.; Cuvier, C.; De Bazelaire, C.; Teixeira, L.; Becourt, S.; LeDoux, F.; Hocini, H.; et al. Prognostic Impact of Stromal Immune Infiltration before and after Neoadjuvant Chemotherapy (NAC) in Triple Negative Inflammatory Breast Cancers (TNIBC) Treated with Dose-Dense Dose-Intense NAC. Cancers 2020, 12, 2657. [Google Scholar] [CrossRef]
- Pelekanou, V.; Carvajal-Hausdorf, D.E.; Altan, M.; Wasserman, B.; Carvajal-Hausdorf, C.; Wimberly, H.; Brown, J.; Lannin, D.; Pusztai, L.; Rimm, D.L. Effect of neoadjuvant chemotherapy on tumor-infiltrating lymphocytes and PD-L1 expression in breast cancer and its clinical significance. Breast Cancer Res. 2017, 19, 91. [Google Scholar] [CrossRef]
- Ethier, J.L.; Desautels, D.; Templeton, A.; Shah, P.S.; Amir, E. Prognostic role of neutrophil-to-lymphocyte ratio in breast cancer: A systematic review and meta-analysis. Breast Cancer Res. 2017, 19, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corbeau, I.; Jacot, W.; Guiu, S. Neutrophil to Lymphocyte Ratio as Prognostic and Predictive Factor in Breast Cancer Patients: A Systematic Review. Cancers 2020, 12, 958. [Google Scholar] [CrossRef] [PubMed]
- Koh, C.H.; Bhoo-Pathy, N.; Ng, K.L.; Jabir, R.S.; Tan, G.H.; See, M.H.; Jamaris, S.; Taib, N.A. Utility of pre-treatment neutrophil-lymphocyte ratio and platelet-lymphocyte ratio as prognostic factors in breast cancer. Br. J. Cancer 2015, 113, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Si, W.; Sun, Q.; Qin, B.; Zhao, W.; Yang, J. Platelet-lymphocyte ratio acts as an indicator of poor prognosis in patients with breast cancer. Oncotarget 2017, 8, 1023–1030. [Google Scholar] [CrossRef] [Green Version]
- Ni, X.J.; Zhang, X.L.; Ou-Yang, Q.W.; Qian, G.W.; Wang, L.; Chen, S.; Jiang, Y.-Z.; Zuo, W.-J.; Wu, J.; Hu, X.; et al. An elevated peripheral blood lymphocyte-to-monocyte ratio predicts favorable response and prognosis in locally advanced breast cancer following neoadjuvant chemotherapy. PLoS ONE 2014, 9, e111886. [Google Scholar] [CrossRef] [Green Version]
- Cuello-Lopez, J.; Fidalgo-Zapata, A.; Lopez-Agudelo, L.; Vasquez-Trespalacios, E. Platelet-to-lymphocyte ratio as a predictive factor of complete pathologic response to neoadjuvant chemotherapy in breast cancer. PLoS ONE 2018, 13, e0207224. [Google Scholar] [CrossRef] [Green Version]
- Asano, Y.; Kashiwagi, S.; Onoda, N.; Noda, S.; Kawajiri, H.; Takashima, T.; Ohsawa, M.; Kitagawa, S.; Hirakawa, K. Predictive Value of Neutrophil/Lymphocyte Ratio for Efficacy of Preoperative Chemotherapy in Triple-Negative Breast Cancer. Ann. Surg. Oncol. 2016, 23, 1104–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Berckelaer, C.; Van Geyt, M.; Linders, S.; Rypens, C.; Trinh, X.B.; Tjalma, W.A.A.; Van Laere, S.; Colpaert, C.; Dirix, L.; van Dam, P. A high neutrophil-lymphocyte ratio and platelet-lymphocyte ratio are associated with a worse outcome in inflammatory breast cancer. Breast 2020, 53, 212–220. [Google Scholar] [CrossRef]
- Mego, M.; Gao, H.; Cohen, E.N.; Anfossi, S.; Giordano, A.; Sanda, T.; Fouad, T.; De Giorgi, U.; Giuliano, M.; Woodward, W.; et al. Circulating Tumor Cells (CTC) Are Associated with Defects in Adaptive Immunity in Patients with Inflammatory Breast Cancer. J. Cancer 2016, 7, 1095–1104. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Lee, M.; Seo, J.H.; Gong, G.; Lee, H.J. Changes in Tumor-infiltrating Lymphocytes After Neoadjuvant Chemotherapy and Clinical Significance in Triple Negative Breast Cancer. Anticancer Res. 2020, 40, 1883–1890. [Google Scholar] [CrossRef]
- Ochi, T.; Bianchini, G.; Ando, M.; Nozaki, F.; Kobayashi, D.; Criscitiello, C.; Curigliano, G.; Iwamoto, T.; Niikura, N.; Takei, H.; et al. Predictive and prognostic value of stromal tumour-infiltrating lymphocytes before and after neoadjuvant therapy in triple negative and HER2-positive breast cancer. Eur. J. Cancer 2019, 118, 41–48. [Google Scholar] [CrossRef]
- Hwang, H.W.; Jung, H.; Hyeon, J.; Park, Y.H.; Ahn, J.S.; Im, Y.H.; Nam, S.J.; Kim, S.W.; Lee, J.E.; Yu, J.-H.; et al. A nomogram to predict pathologic complete response (pCR) and the value of tumor-infiltrating lymphocytes (TILs) for prediction of response to neoadjuvant chemotherapy (NAC) in breast cancer patients. Breast Cancer Res. Treat. 2019, 173, 255–266. [Google Scholar] [CrossRef]
- Zhang, L.; Wang, X.I.; Zhang, S. Tumor-infiltrating lymphocyte volume is a better predictor of neoadjuvant therapy response and overall survival in triple-negative invasive breast cancer. Hum. Pathol. 2018, 80, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Castaneda, C.A.; Mittendorf, E.; Casavilca, S.; Wu, Y.; Castillo, M.; Arboleda, P.; Nunez, T.; Guerra, H.; Barrionuevo, C.; Dolores-Cerna, K.; et al. Tumor infiltrating lymphocytes in triple negative breast cancer receiving neoadjuvant chemotherapy. World J. Clin. Oncol. 2016, 7, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Dawood, S.; Merajver, S.D.; Viens, P.; Vermeulen, P.B.; Swain, S.M.; Buchholz, T.A.; Dirix, L.Y.; Levine, P.H.; Lucci, A.; Krishnamurthy, S.; et al. International expert panel on inflammatory breast cancer: Consensus statement for standardized diagnosis and treatment. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol./ESMO 2011, 22, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Dieci, M.V.; Radosevic-Robin, N.; Fineberg, S.; van den Eynden, G.; Ternes, N.; Penault-Llorca, F.; Pruneri, G.; D’Alfonso, T.M.; Demaria, S.; Castaneda, C.; et al. Update on tumor-infiltrating lymphocytes (TILs) in breast cancer, including recommendations to assess TILs in residual disease after neoadjuvant therapy and in carcinoma in situ: A report of the International Immuno-Oncology Biomarker Working Group on Breast Cancer. Semin. Cancer Biol. 2018, 52 Pt 2, 16–25. [Google Scholar]
- RStudio: Integrated Development for R. RStudio; Rstudio Team I: Boston, MA, USA, 2016; Available online: http://www.rstudio.com/ (accessed on 20 September 2020).
- Seo, A.N.; Lee, H.J.; Kim, E.J.; Kim, H.J.; Jang, M.H.; Lee, H.E.; Kim, Y.J.; Kim, J.H.; Park, S.Y. Tumour-infiltrating CD8+ lymphocytes as an independent predictive factor for pathological complete response to primary systemic therapy in breast cancer. Br. J. Cancer 2013, 109, 2705–2713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shou, J.; Zhang, Z.; Lai, Y.; Chen, Z.; Huang, J. Worse outcome in breast cancer with higher tumor-infiltrating FOXP3+ Tregs: A systematic review and meta-analysis. BMC Cancer 2016, 16, 687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Martinez, E.; Gil, G.L.; Benito, A.C.; Gonzalez-Billalabeitia, E.; Conesa, M.A.; Garcia Garcia, T.; García-Garre, E.; Vicente, V.; de la Peña, F.A. Tumor-infiltrating immune cell profiles and their change after neoadjuvant chemotherapy predict response and prognosis of breast cancer. Breast Cancer Res. 2014, 16, 488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruffell, B.; Au, A.; Rugo, H.S.; Esserman, L.J.; Hwang, E.S.; Coussens, L.M. Leukocyte composition of human breast cancer. Proc. Natl. Acad. Sci. USA 2012, 109, 2796–2801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eiró, N.; Pidal, I.; Fernandez-Garcia, B.; Junquera, S.; Lamelas, M.L.; del Casar, J.M.; González, L.O.; López-Muñiz, A.; Vizoso, F.J. Impact of CD68/(CD3+CD20) ratio at the invasive front of primary tumors on distant metastasis development in breast cancer. PLoS ONE 2012, 7, e52796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertucci, F.B.L.; Finetti, P.; Van Berckelaer, C.; Van Dam, P.; Dirix, L.; Viens, P.; Goncalves, A.; Ueno, N.T.; Van Laere, S.; Birnbaum, D.; et al. Immune landscape of inflammatory breast cancer suggests vulnerability to immune checkpoint inhibitors. Oncoimmunology 2021, 10, 1929724. [Google Scholar] [CrossRef]
- Lee, H.; Na, K.J.; Choi, H. Differences in Tumor Immune Microenvironment in Metastatic Sites of Breast Cancer. Front. Oncol. 2021, 11, 649004. [Google Scholar] [CrossRef]
- Larsson, A.M.; Roxå, A.; Leandersson, K.; Bergenfelz, C. Impact of systemic therapy on circulating leukocyte populations in patients with metastatic breast cancer. Sci. Rep. 2019, 9, 13451. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, P.; Scaife, J.; Freeman, S. Validation of a predictive model that identifies patients at high risk of developing febrile neutropaenia following chemotherapy for breast cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol./ESMO 2012, 23, 1766–1771. [Google Scholar] [CrossRef]





| Parameters | nIBC | IBC | p-Value |
|---|---|---|---|
| Hormonal receptor state | 0.57 | ||
| Negative | 48 | 50 | |
| Positive | 86 | 75 | |
| HER2 state | 0.91 | ||
| Negative | 86 | 74 | |
| Positive | 48 | 44 | |
| Receptor subtypes | 0.16 | ||
| HR+/HER2− | 50 | 48 | |
| HR+/HER2+ | 36 | 24 | |
| HR−/HER2+ | 12 | 20 | |
| HR−/HER2− | 36 | 26 | |
| Differentiation grade | 0.001 | ||
| Well | 12 | 6 | |
| Moderate | 47 | 35 | |
| Poor | 42 | 79 | |
| Stage | <0.001 | ||
| Stage I or II | 103 | 0 | |
| Stage III | 28 | 125 | |
| Response to NACT | 0.87 | ||
| RD | 78 | 75 | |
| pCR | 56 | 50 | |
| Pre-NACT sTIL (cat) (%) * | 0.24 | ||
| <12.5% | 62 | 68 | |
| ≥12.5% | 72 | 57 | |
| Post-NACT sTIL (cat) in RD (%) * | 0.54 | ||
| <5% | 42 | 24 | |
| ≥5% | 37 | 28 | |
| Difference in sTIL before and after NACT | 0.034 | ||
| Increase (>5%) | 13 | 7 | |
| No change (≥−5–≤5%) | 48 | 22 | |
| Decrease (<−5%) | 18 | 23 | |
| Change in sTIL after NACT | 0.044 | ||
| Increase/stable (≥0%) | 33 | 12 | |
| Decrease (<0%) | 46 | 40 |
| Parameters | nIBC | n | IBC | n | p-Value |
|---|---|---|---|---|---|
| Age (years) | 53.3 (27.2–82.4) | 134 | 56.6 (33.3–83) | 125 | 0.087 |
| Residual Cancer Cellularity | 20 (1–90) | 70 | 15 (1–90) | 52 | 0.38 |
| NLR (Moment of diagnosis) | 2.68 (0.86–12.9) | 129 | 2.53 (0.85–9.11) | 56 | 0.46 |
| PLR (Moment of diagnosis) | 150 (61–569) | 129 | 150 (73–299) | 56 | 0.79 |
| LMR (Moment of diagnosis) | 4.35 (0.69–23.7) | 129 | 3.43 (1–9.5) | 56 | <0.001 |
| NLR (After NACT) | 4.02 (0.28–60) | 86 | 3.43 (0.04–21.0) | 42 | 0.11 |
| PLR (After NACT) | 274 (43–1006) | 86 | 204 (51.5–840) | 42 | 0.005 |
| LMR (After NACT) | 1.74 (0.52–13.9) | 86 | 2.28 (0.79–7.2) | 39 | 0.03 |
| Pre-NACT sTIL (%) | 10 (1–85) | 134 | 12.5 (1–80) | 125 | 0.13 |
| Post-NACT sTIL in RD (%) | 5 (1–60) | 79 | 4 (1–90) | 52 | 0.16 |
| Difference in sTIL before and after NACT (%) | −1.25 (−81–32.5) | 79 | −4.5 (−48–75) | 52 | 0.018 |
| Parameters | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| nIBC vs. IBC | 0.23 (0.106–0.481) | <0.001 | 0.247 (0.073–0.761) | 0.02 |
| HR− vs. HR+ | 2.174 (1.019–4.756) | 0.047 | 2.277 (0.729–7.43) | 0.16 |
| HER2− vs. HER2+ | 0.749 (0.333–1.667) | 0.479 | ||
| Differentiation: Low vs. Moderate Low vs. High | 0.847 (0.246–2.801) 0.643 (0.188–2.11) | 0.787 0.47 | ||
| sTIL pre-NACT: <12.5% vs. ≥12.5% | 0.099 (0.04–0.223) | <0.001 | 0.022 (0.003–0.095) | <0.001 |
| sTIL post-NACT: <5% vs. ≥5% | 2.032 (1.018–4.115) | 0.046 | 13.12 (3.181–93.55) | 0.002 |
| Nodal status: cN0/1 vs. cN2/3 | 0.886 (0.389–2.028) | 0.774 | ||
| Cellularity: <20% vs. >20% | 2.021 (0.963–4.31) | 0.065 | ||
| NLR: <2.64 vs. ≥2.64 | 1.832 (0.854–3.982) | 0.122 | ||
| PLR: <150 vs. ≥ 150 | 2.289 (1.062–5.027) | 0.036 | 2.005 (0.730–5.673) | 0.18 |
| LMR: <4.05 vs. ≥ 4.05 | 1.909 (0.898–4.107) | 0.094 | ||
| NLR after NACT: <2.64 vs. ≥2.64 | 1.059 (0.499–2.252) | 0.879 | ||
| PLR after NACT: <250 vs. ≥250 | 1.595 (0.649–4.127) | 0.318 | ||
| LMR after NACT: <1.82 vs. ≥1.82 | 1.158 (0.445–3.017) | 0.762 | ||
| Age: <54.45 vs. ≥54.45 | 0.611 (0.226–1.616) | 0.324 | ||
| Parameters | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| HR− vs. HR+ | 0.472 (0.145–1.473) | 0.201 | ||
| HER2− vs. HER2+ | 0.694 (0.181–2.473) | 0.578 | ||
| Differentiation: Low vs. Moderate Low vs. High | 1.199 (0.093–29.14) 2.428 (0.211–55.54) | 0.891 0.487 | ||
| sTIL pre-NACT: <12.5% vs. ≥12.5% | 2.999 (0.987–9.648) | 0.057 | 2.13 (0.51–9.73) | 0.30 |
| Nodal status: cN0/1 vs. cN2/3 | 2.142 (0.583–8.317) | 0.257 | ||
| Cellularity: <20% vs. >20% | 11.519 (3.03–52.582) | 0.001 | 11.64 (2.99–55.29) | <0.001 |
| NLR: <2.64 vs. ≥2.64 | 1.333 (0.327–5.607) | 0.688 | ||
| PLR: <150 vs. ≥ 150 | 1.285 (0.318–5.298) | 0.723 | ||
| LMR: <4.05 VS. ≥4.05 | 1.4 (0.34–6.058) | 0.642 | ||
| Age: <54.45 vs. ≥54.45 | 1.111 (0.29–4.272) | 0.877 | ||
| NLR after NACT: <2.64 vs. ≥2.64 | 1.23 (0.225–7.353) | 0.810 | ||
| PLR after NACT: <250 vs. ≥250 | 1.296 (0.23–8.148) | 0.770 | ||
| LMR after NACT: <1.82 vs. ≥1.82 | 2.999 (0.437–27.129) | 0.279 | ||
| PDL1: <1% vs. >1% | 1.217 (0.606–2.493) | 0.58 |
| Parameters | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age: <56.6 vs. ≥56.6 | 1.86 (0.75–4.61) | 0.17 | ||
| HR− vs. HR+ | 0.54 (0.25–1.13) | 0.11 | ||
| HER2− vs. HER2+ | 1.49 (0.65–3.41) | 0.34 | ||
| Differentiation: Moderate vs. High | 0.88 (0.4–1.89) | 0.74 | ||
| Nodal status: cN0/1 vs. cN2/3 | 2.97 (1.13–7.81) | 0.03 | 1.93 (0.64–5.80) | 0.24 |
| PDL1: <1% vs. >1% | 0.91 (0.56–1.50) | 0.72 | ||
| TIL pre-NACT: <10% vs. ≥10% | 2.08 (0.98–4.41) | 0.05 | 4.47 (1.37–14.5) | 0.01 |
| TIL post-NACT: <4% vs. ≥4% | 0.48 (0.22–1.04) | 0.06 | 0.23 (0.05–1.02) | 0.05 |
| Cellularity: <17.5% vs. ≥17.5% | 0.23 (0.09–0.53) | <0.001 | 0.67 (0.20–2.19) | 0.50 |
| NLR: <2.4 vs. ≥2.4 | 1.42 (0.57–3.53) | 0.44 | ||
| PLR: <163 vs. ≥163 | 1.09 (0.44–2.71) | 0.84 | ||
| LMR: <3.6 vs. ≥3.6 | 0.93 (0.36–2.38) | 0.88 | ||
| NLR after NACT: <3.3 vs. ≥3.3 | 1.31 (0.43–4.01) | 0.63 | ||
| PLR after NACT: <171 vs. ≥171 | 1.27 (0.33–4.84) | 0.71 | ||
| LMR after NACT: <2.6 vs. ≥2.6 | 0.27 (0.07–1.12) | 0.07 | ||
| Change: increase vs. decrease | 1.85 (0.80–4.28) | 0.15 |
| Parameters | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age: <56.6 vs. ≥56.6 | 1.88 (0.82–4.32) | 0.13 | ||
| HR− vs. HR+ | 0.53 (0.26–1.08) | 0.08 | ||
| HER2− vs. HER2+ | 1.17 (0.52–2.64) | 0.7 | ||
| Differentiation: Moderate vs. High | 1.17 (0.57–2.38) | 0.66 | ||
| Nodal status: cN0/1 vs. cN2/3 | 1.83 (0.80–4.22) | 0.15 | ||
| PDL1: <1% vs. > 1% | 1.13 (0.75–1.68) | 0.56 | ||
| TIL pre-NACT: <10% vs. ≥10% | 1.28 (0.63–2.61) | 0.49 | ||
| TIL post-NACT: <4% vs. ≥4% | 0.31 (0.14–0.68) | 0.003 | 0.33 (0.11–0.98) | 0.046 |
| Cellularity: <17.5% vs. ≥17.5% | 0.14 (0.06–0.33) | <0.001 | 0.20 (0.08–0.52) | <0.001 |
| NLR: <2.4 vs. ≥2.4 | 1.38 (0.61–3.14) | 0.43 | ||
| PLR: <163 vs. ≥163 | 1.47 (0.65–3.33) | 0.35 | ||
| LMR: <3.6 vs. ≥3.6 | 0.48 (0.21–1.11) | 0.09 | ||
| NLR after NACT: <3.3 vs. ≥3.3 | 1.38 (0.54–3.50) | 0.49 | ||
| PLR after NACT: <171 vs. ≥171 | 2.32 (0.75–7.15) | 0.13 | ||
| LMR after NACT: <2.6 vs. ≥2.6 | 0.54 (0.15–1.92) | 0.34 | ||
| Change: increase vs. decrease | 2.26 (1.03–4.96) | 0.04 | 2.08 (0.85–5.13) | 0.11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Berckelaer, C.; Vermeiren, I.; Vercauteren, L.; Rypens, C.; Oner, G.; Trinh, X.B.; Tjalma, W.A.A.; Broeckx, G.; Charafe-Jauffret, E.; Van Laere, S.; et al. The Evolution and Prognostic Role of Tumour-Infiltrating Lymphocytes and Peripheral Blood-Based Biomarkers in Inflammatory Breast Cancer Patients Treated with Neoadjuvant Chemotherapy. Cancers 2021, 13, 4656. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13184656
Van Berckelaer C, Vermeiren I, Vercauteren L, Rypens C, Oner G, Trinh XB, Tjalma WAA, Broeckx G, Charafe-Jauffret E, Van Laere S, et al. The Evolution and Prognostic Role of Tumour-Infiltrating Lymphocytes and Peripheral Blood-Based Biomarkers in Inflammatory Breast Cancer Patients Treated with Neoadjuvant Chemotherapy. Cancers. 2021; 13(18):4656. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13184656
Chicago/Turabian StyleVan Berckelaer, Christophe, Iris Vermeiren, Leonie Vercauteren, Charlotte Rypens, Gizem Oner, Xuan Bich Trinh, Wiebren A. A. Tjalma, Glenn Broeckx, Emmanuelle Charafe-Jauffret, Steven Van Laere, and et al. 2021. "The Evolution and Prognostic Role of Tumour-Infiltrating Lymphocytes and Peripheral Blood-Based Biomarkers in Inflammatory Breast Cancer Patients Treated with Neoadjuvant Chemotherapy" Cancers 13, no. 18: 4656. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13184656