
Surveillance for Patients with Oral Squamous Cell Carcinoma after Complete Surgical Resection as Primary Treatment: A Single-Center Retrospective Cohort Study

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Data Sources
2.2. Patients
2.3. Statistical Analysis
3. Results
3.1. Characteristics and Treatment of Patients with OSCC
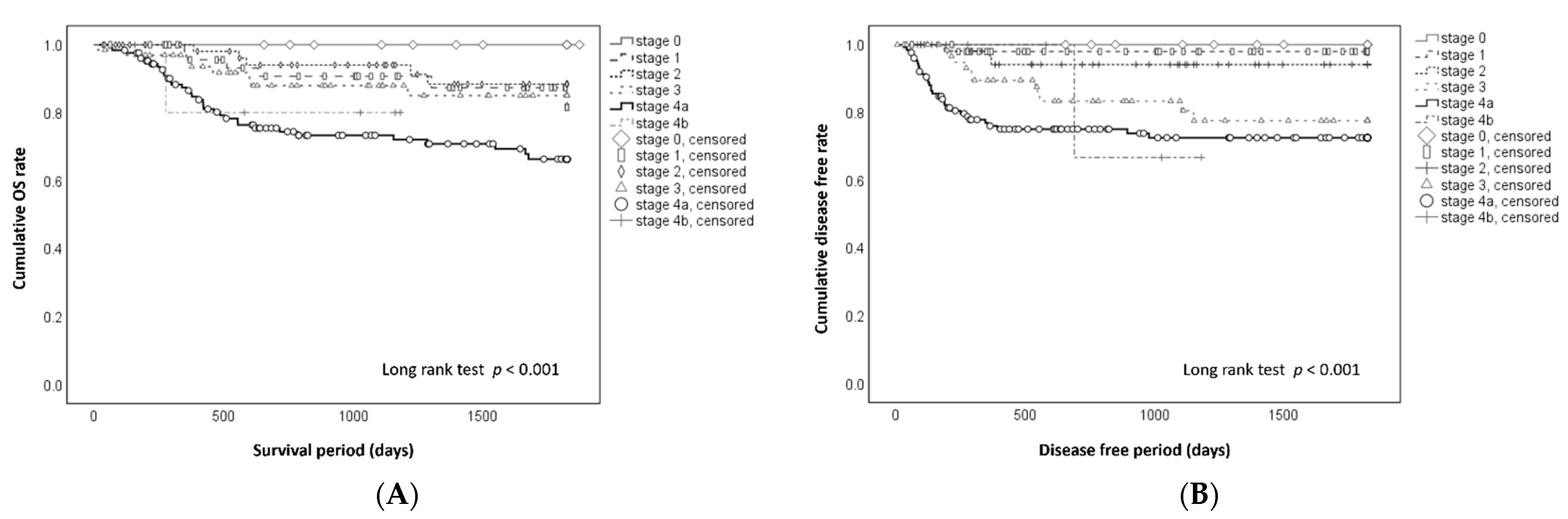
3.2. Prognosis after Surgical Treatment
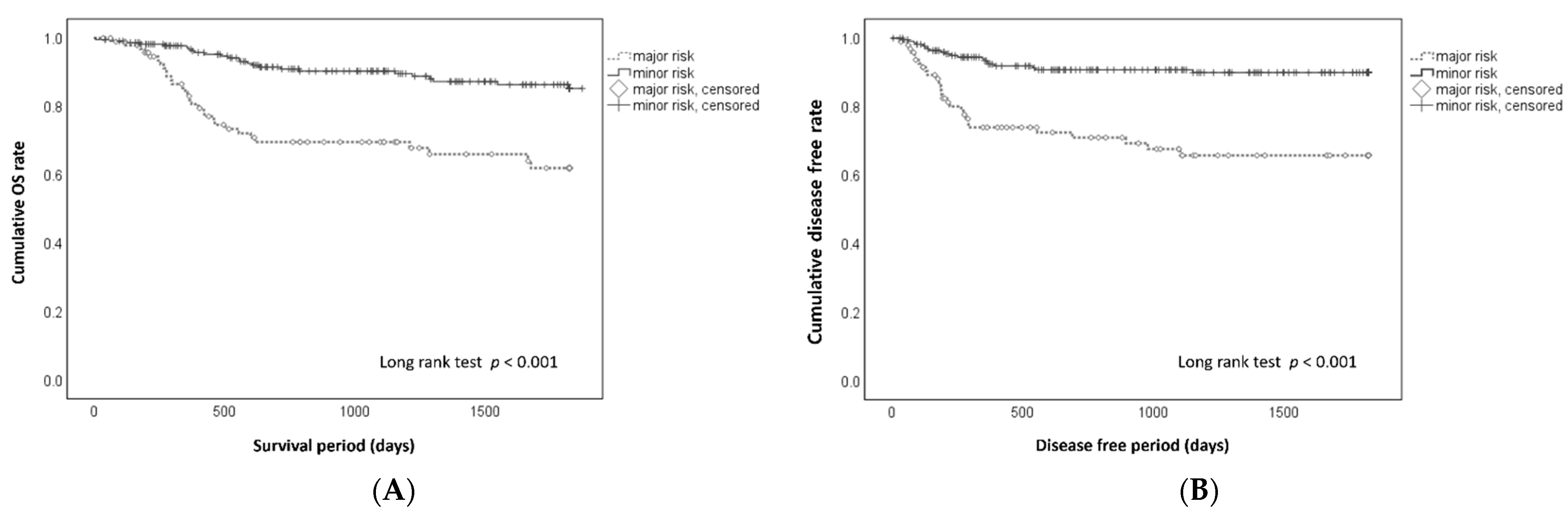
3.3. Mortality and Postsurgical Events in Patients with Major Risk Factors
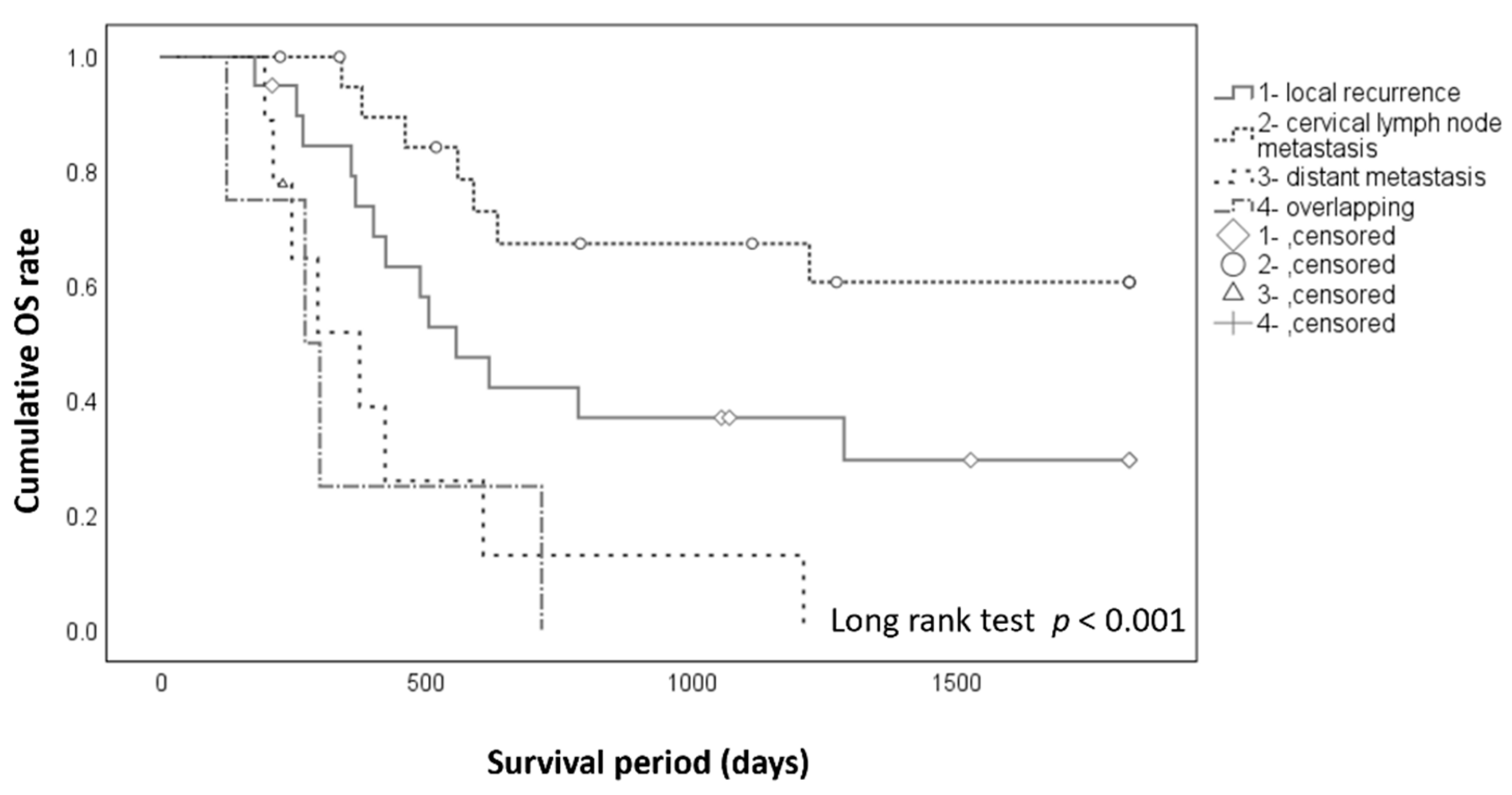
3.4. Prognosis after Occurrence of Postsurgical Events
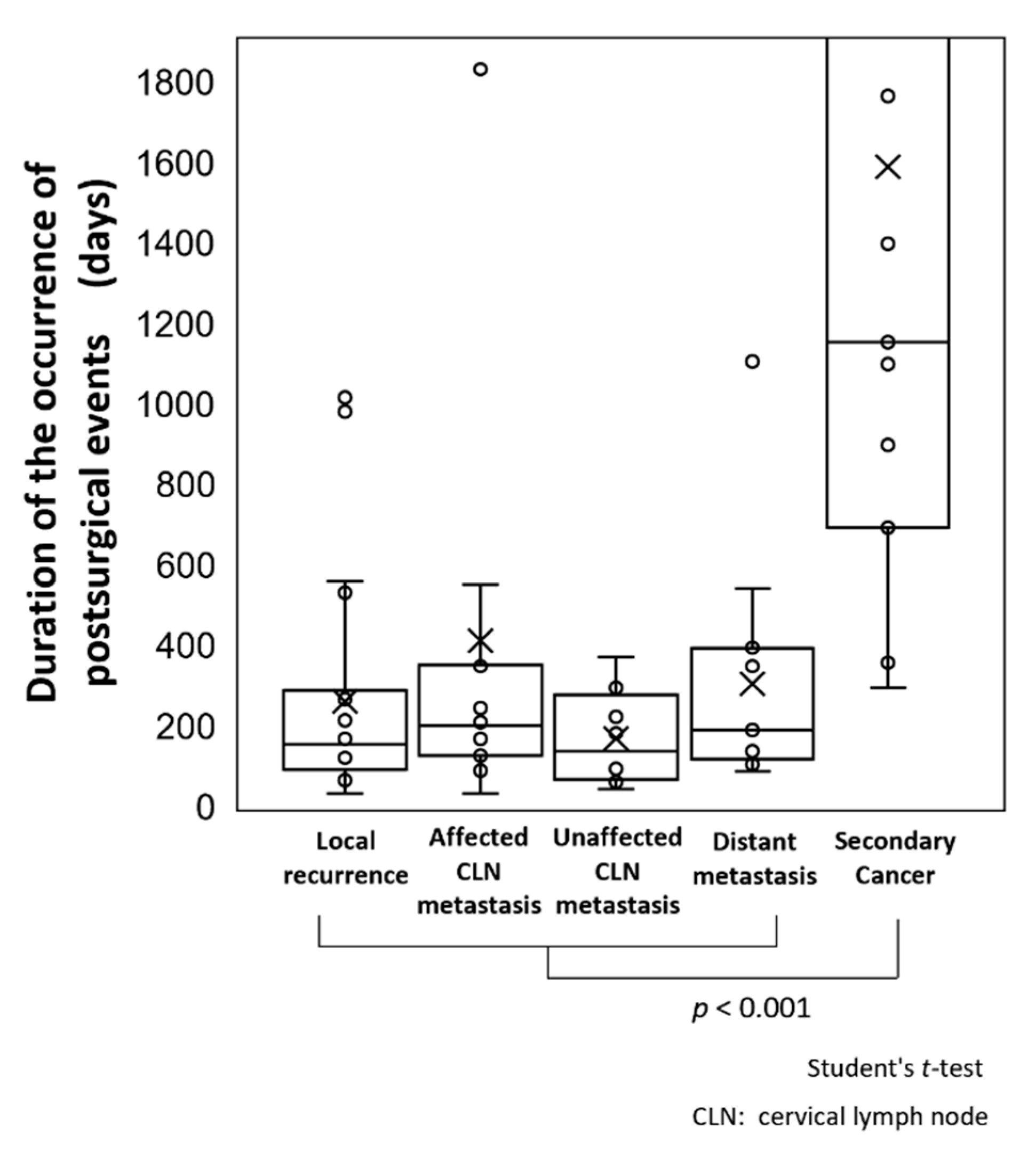
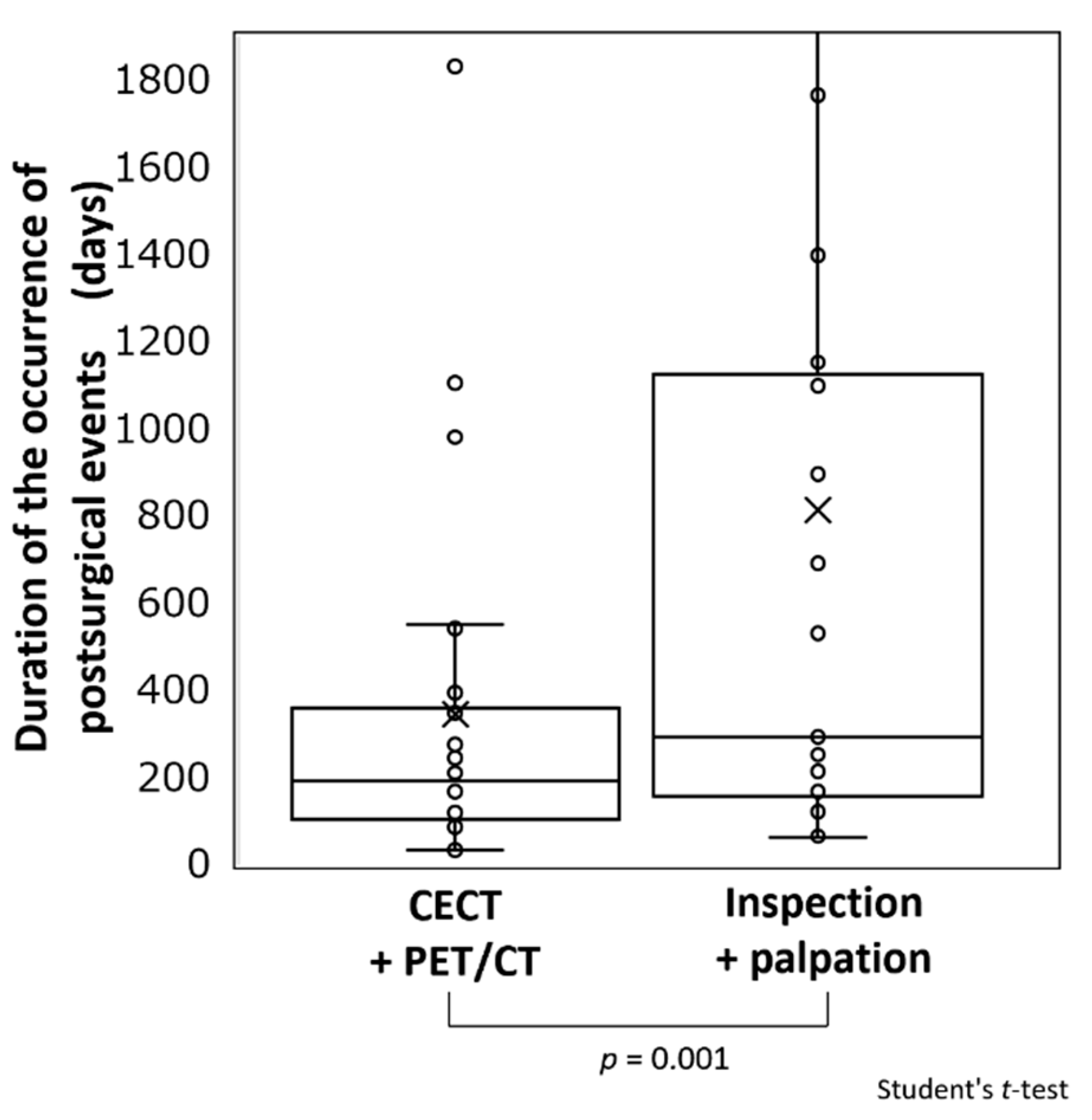
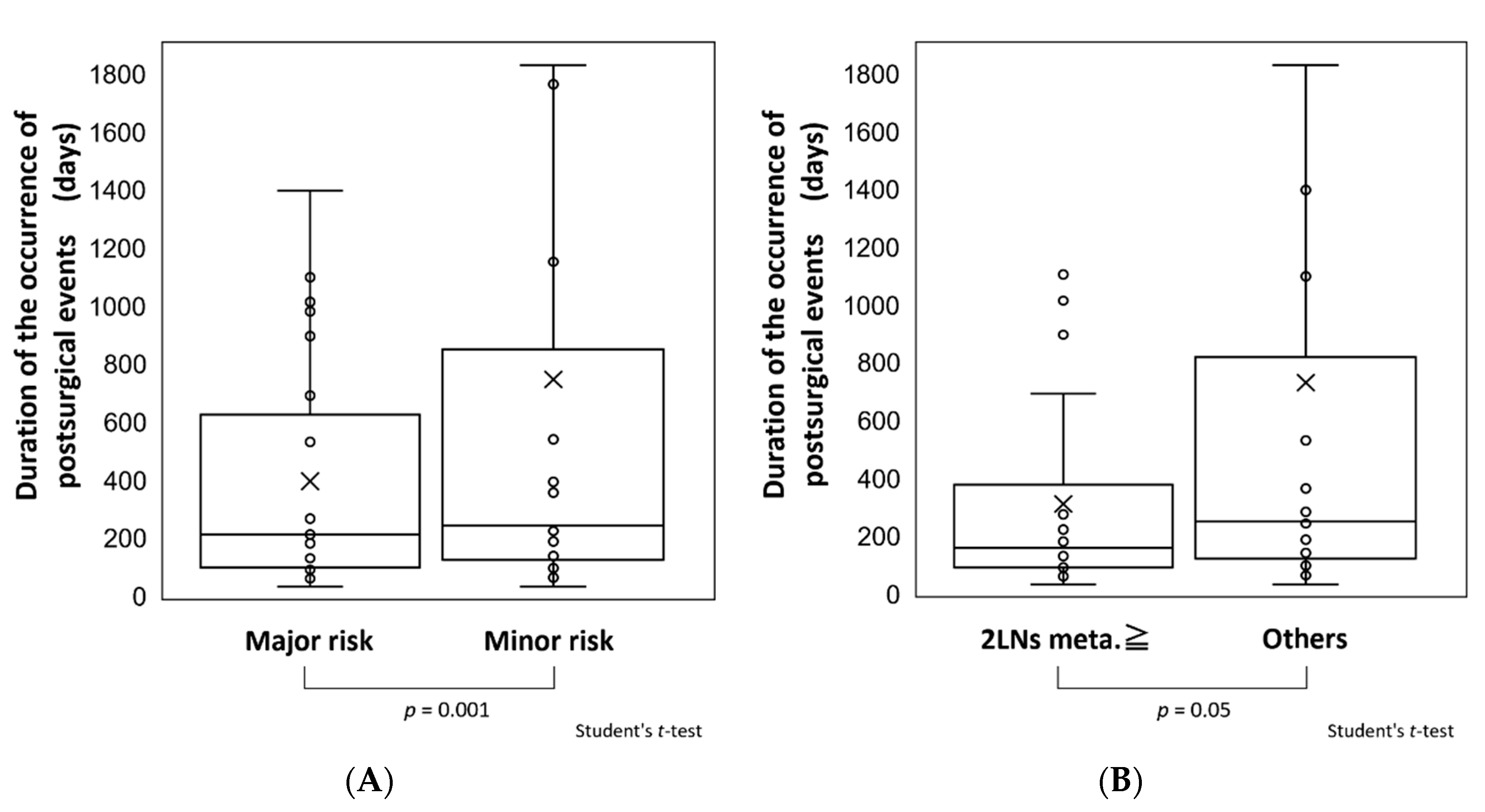
3.5. Comparisons of Periods until Occurrence of Postsurgical Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Comprehensive Cancer Network. NCCN Guidelines for Head and Neck Cancers (Version 2.2020). Available online: https://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf (accessed on 24 August 2020).
- Yamamoto, E.; Kohama, G. Mode of invasion.; bleomycin sensitivity and clinical course in squamous cell carcinoma of the oral cavity. Cancer 1983, 51, 2175–2180. [Google Scholar] [CrossRef]
- Yamamoto, E.; Miyakawa, A.; Kohama, G. Mode of invasion and lymph node metastasis in squamous cell carcinoma of the oral cavity. Head Neck Surg. 1984, 6, 938–947. [Google Scholar] [CrossRef] [PubMed]
- Fukumoto, C.; Sawatani, Y.; Shiraishi, R.; Zama, M.; Shimura, M.; Hasegawa, T.; Komiyama, Y.; Fujita, A.; Wakui, T.; Kawamata, H. Effectiveness of cetuximab as preemptive postsurgical therapy for oral squamous cell carcinoma patients with major risk: A single-center retrospective cohort study. Investig. New Drugs 2021, 39, 846–852. [Google Scholar] [CrossRef] [PubMed]
- Sawatani, Y.; Komiyama, Y.; Nakashiro, K.; Uchida, D.; Fukumoto, C.; Shimura, M.; Hasegawa, T.; Kamimura, R.; Hitomi-Koide, M.; Hyodo, T.; et al. Paclitaxel potentiates the anticancer effect of cetuximab by enhancing antibody-dependent cellular cytotoxicity on oral squamous cell carcinoma cells in vitro. Int. J. Mol. Sci. 2020, 21, 6292. [Google Scholar] [CrossRef] [PubMed]
- Dunsky, K.A.; Wehrmann, D.J.; Osman, M.M.; Thornberry, B.M.; Varvares, M.A. PET-CT and the detection of the asymptomatic recurrence or second primary lesions in the treated head and neck cancer patient. Laryngoscope 2013, 123, 2161–2164. [Google Scholar] [CrossRef] [PubMed]
- Heineman, T.E.; Kuan, E.C.; St John, M.A. When should surveillance imaging be performed after treatment for head and neck cancer? Laryngoscope 2017, 127, 533–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, A.S.; Tsao, G.J.; Chen, F.W.; Shen, T.; Kaplam, M.J.; Colevas, A.D.; Fischbein, N.J.; Quon, A.; Le, Q.T.; Pinto, H.A.; et al. Impact of positron emission tomography/computed tomography surveillance at 12 and 24 months for detecting head and neck cancer recurrence. Cancer 2013, 19, 1349–1356. [Google Scholar] [CrossRef] [PubMed]
- Paleri, V.; Urbano, T.G.; Mehanna, H.; Repanos, C.; Lancaster, J.; Roques, T.; Patel, M.; Sen, M. Management of neck metastases in head and neck cancer: United Kingdom National Multidisciplinary Guidelines. J. Laryngol. Otol. 2016, 130, S161–S169. [Google Scholar] [CrossRef] [PubMed]
- Brierley, D.J.; Gospodarowicz, K.M.; Wittekind, C. TNM Classification of Malignant Tumours, 8th ed.; Wiley-Blackwell: London, UK, 2017. [Google Scholar]
- Tsukahara, K.; Kubota, A.; Hasegawa, Y.; Takemura, H.; Terada, T.; Taguchi, T.; Nagahara, K.; Nakatani, H.; Yoshino, K.; Higaki, Y.; et al. Randomized phase III trial of adjuvant chemotherapy with S-1 after curative treatment in patients with squamous-cell carcinoma of the head and neck (ACTS-HNC). PLoS ONE 2015, 10, e0116965. [Google Scholar]
- Chen, S.W.; Zhang, Q.; Guo, Z.M.; Chen, W.K.; Liu, W.W.; Chen, Y.F.; Li, Q.L.; Liu, X.K.; Li, H.; Ou-Yang, D.; et al. Trends in clinical features and survival of oral cavity cancer: Fifty years of experience with 3362 consecutive cases from a single institution. Cancer Manag. Res. 2018, 10, 4523–4535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Cancer Institute. The Surveillance.; Epidemiology.; and End Results (SEER) Program of the National Cancer Institute; US. SEER Cancer Statistics Review (CSR) 1975–2016. Available online: https://seer.cancer.gov/csr/1975_2016/ (accessed on 30 April 2020).
- D’Cruz, A.K.; Vaish, R.; Kapre, N.; Dandekar, M.; Gupta, S.; Hawaldar, R.; Agarwal, J.P.; Pantvaidya, G.; Chaukar, D.; Deshmukh, A.; et al. Elective versus therapeutic neck dissection in node-negative oral cancer. N. Engl. J. Med. 2015, 373, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Bree, R.D.; Takes, R.P.; Shah, J.P.; Hamoir, M.; Kowalski, L.P.; Robbins, K.T.; Rodrigo, J.P.; Sanabria, A.; Medina, J.E.; Rinaldo, A.; et al. Elective neck dissection in oral squamous cell carcinoma: Past.; present and future. Oral Oncol. 2019, 90, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Fang, Q.; Gao, H.; Gao, Q.; Sun, J.; Li, P.; Cui, M.; Zhang, E.; Yin, W.; Dong, Y. Elective neck dissection versus wait-and-see policy in cT1N0 buccal squamous cell carcinoma. BMC Cancer 2020, 20, 537. [Google Scholar] [CrossRef] [PubMed]
- Wakui, T.; Izumi, S.; Koshiji, C.; Kuribayashi, N.; Komiyama, Y.; Tuchida, S.; Kinouchi, M.; Hasegawa, T.; Uchida, D.; Kawamata, H. Usefulness and limitations of FDG-PET/contrast-enhanced CT in evaluating cervical lymph node metastasis in patients with oral squamous cell carcinoma. Jpn. J. Oral Maxillofac. Surg. 2018, 64, 568–576. (In Japanese) [Google Scholar] [CrossRef] [Green Version]
- Ferris, R.L.; Blumenschein, J.G.; Fayette, J.; Guigay, J.; Colevas, D.; Licitra, L.; Harrington, K.; Kasper, S.; Vokes, E.E.; Evan, C.; et al. Nivolumab for recurrent squamous-cell carcinoma of the head and neck. N. Engl. J. Med. 2016, 375, 1856–1867. [Google Scholar] [CrossRef] [PubMed]
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulières, D.; Tahara, M.; Castro, G.D., Jr.; Psyrri, A.; Basté, N.; Neupane, P.; Bratland, A.; et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomised.; open-label.; phase 3 study. Lancet 2019, 394, 1915–1928. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | n | % |
|---|---|---|
| Sex, male, n (%) | 190 | (58.6) |
| Age, mean (SD) y | 66.6 | (13.8) |
| Age, median y | 69 | |
| Age group, n (%) | ||
| <65 y | 125 | (38.6) |
| ≥65 to <75 y | 96 | (29.6) |
| ≥75 y | 103 | (31.8) |
| Primary site, n (%) | ||
| Tongue | 156 | (48.1) |
| Lower gingiva | 69 | (21.3) |
| Upper gingiva | 44 | (13.6) |
| Buccal mucosa | 24 | (7.4) |
| Oral floor | 20 | (6.2) |
| Lip | 6 | (1.9) |
| Palate | 5 | (1.5) |
| Clinical T stage, n (%) | ||
| Tis | 13 | (4.0) |
| T1 | 52 | (16.0) |
| T2 | 86 | (26.5) |
| T3 | 56 | (17.3) |
| T4a | 114 | (35.2) |
| T4b | 3 | (0.9) |
| Clinical N stage, n (%) | ||
| N0 | 190 | (58.6) |
| N1 | 65 | (20.1 |
| N2b | 54 | (16.7) |
| N2c | 12 | (3.7) |
| N3b | 3 | (0.9) |
| Clinical Stage, n (%) | ||
| Stage 0 | 13 | (4.0) |
| Stage 1 | 51 | (15.7) |
| Stage 2 | 60 | (18.5) |
| Stage 3 | 66 | (20.4) |
| Stage 4a | 127 | (39.2) |
| Stage 4b | 7 | (2.2) |
| Major risk group, n (%) | 97 | (29.9) |
| Major risk factor, n (%) overlapping distribution | ||
| Extranodal extension | 26 | (8.0) |
| Positive or close margins | 12 | (3.7) |
| Metastasis of 2 ≥ LNs | 41 | (12.7) |
| YK-4C or YK-4D | 32 | (9.9) |
| Treatment, n (%) | ||
| Surgery only | 254 | (78.4) |
| Surgery + postsurgical treatment | 70 | (21.6) |
| Postsurgical chemotherapy with cisplatin | 12 | |
| Postsurgical chemotherapy with cetuximab + paclitaxel | 15 | |
| Postsurgical radiation | 10 | |
| Postsurgical chemoradiation with cisplatin | 22 | |
| Postsurgical chemoradiation with cetuximab | 7 | |
| Postsurgical chemoradiation with cetuximab, followed by chemotherapy with cetuximab + paclitaxel | 4 | |
| Adjuvant therapy (S-1 or UFT) | 129 | (39.8) |
| Postsurgical event, n (%) | 65 | (20.1) |
| Death in 5-year period, n (%) | 55 | (17.0) |
| Item | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| Crude HR | 95% CI | p Value a | Adjusted HR | 95% CI | p Value a | |
| YK-4C and 4D | 1.068 | 0.426–2.681 | 0.888 | 1.276 | 0.504–3.230 | 0.607 |
| Positive or close margin | 1.161 | 0.283–4.764 | 0.836 | 1.401 | 0.339–5.786 | 0.641 |
| ENE | 3.285 | 1.696–6.366 | <0.001 | 1.676 | 0.769–3.650 | 0.194 |
| Metastasis to ≥2 LNs | 4.006 | 2.278–7.043 | <0.001 | 3.342 | 1.720–6.492 | <0.001 |
| Item | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| Crude HR | 95% CI | p Value a | Adjusted HR | 95% CI | p Value a | |
| YK-4C and 4D | 0.853 | 0.426–2.528 | 0.908 | 1.136 | 0.403–3.201 | 0.810 |
| Positive or close margin | 1.992 | 0.619–6.411 | 0.248 | 2.100 | 0.647–6.817 | 0.217 |
| ENE | 4.397 | 2.287–8.457 | <0.001 | 2.425 | 1.101–5.339 | 0.028 |
| Metastasis to ≥2 LNs | 4.175 | 2.289–7.613 | <0.001 | 2.955 | 1.437–6.078 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fukumoto, C.; Oshima, R.; Sawatani, Y.; Shiraishi, R.; Hyodo, T.; Kamimura, R.; Hasegawa, T.; Komiyama, Y.; Izumi, S.; Fujita, A.; et al. Surveillance for Patients with Oral Squamous Cell Carcinoma after Complete Surgical Resection as Primary Treatment: A Single-Center Retrospective Cohort Study. Cancers 2021, 13, 5843. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13225843
Fukumoto C, Oshima R, Sawatani Y, Shiraishi R, Hyodo T, Kamimura R, Hasegawa T, Komiyama Y, Izumi S, Fujita A, et al. Surveillance for Patients with Oral Squamous Cell Carcinoma after Complete Surgical Resection as Primary Treatment: A Single-Center Retrospective Cohort Study. Cancers. 2021; 13(22):5843. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13225843
Chicago/Turabian StyleFukumoto, Chonji, Ryo Oshima, Yuta Sawatani, Ryo Shiraishi, Toshiki Hyodo, Ryouta Kamimura, Tomonori Hasegawa, Yuske Komiyama, Sayaka Izumi, Atsushi Fujita, and et al. 2021. "Surveillance for Patients with Oral Squamous Cell Carcinoma after Complete Surgical Resection as Primary Treatment: A Single-Center Retrospective Cohort Study" Cancers 13, no. 22: 5843. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13225843