
Prognostic Role of PD-L1 Expression in Invasive Breast Cancer: A Systematic Review and Meta-Analysis

 ,
,  , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection
2.4. Risk of Bias and Analysis of the Quality of Evidence
2.5. Training of the Reviewers
2.6. Statistical Analysis
3. Results
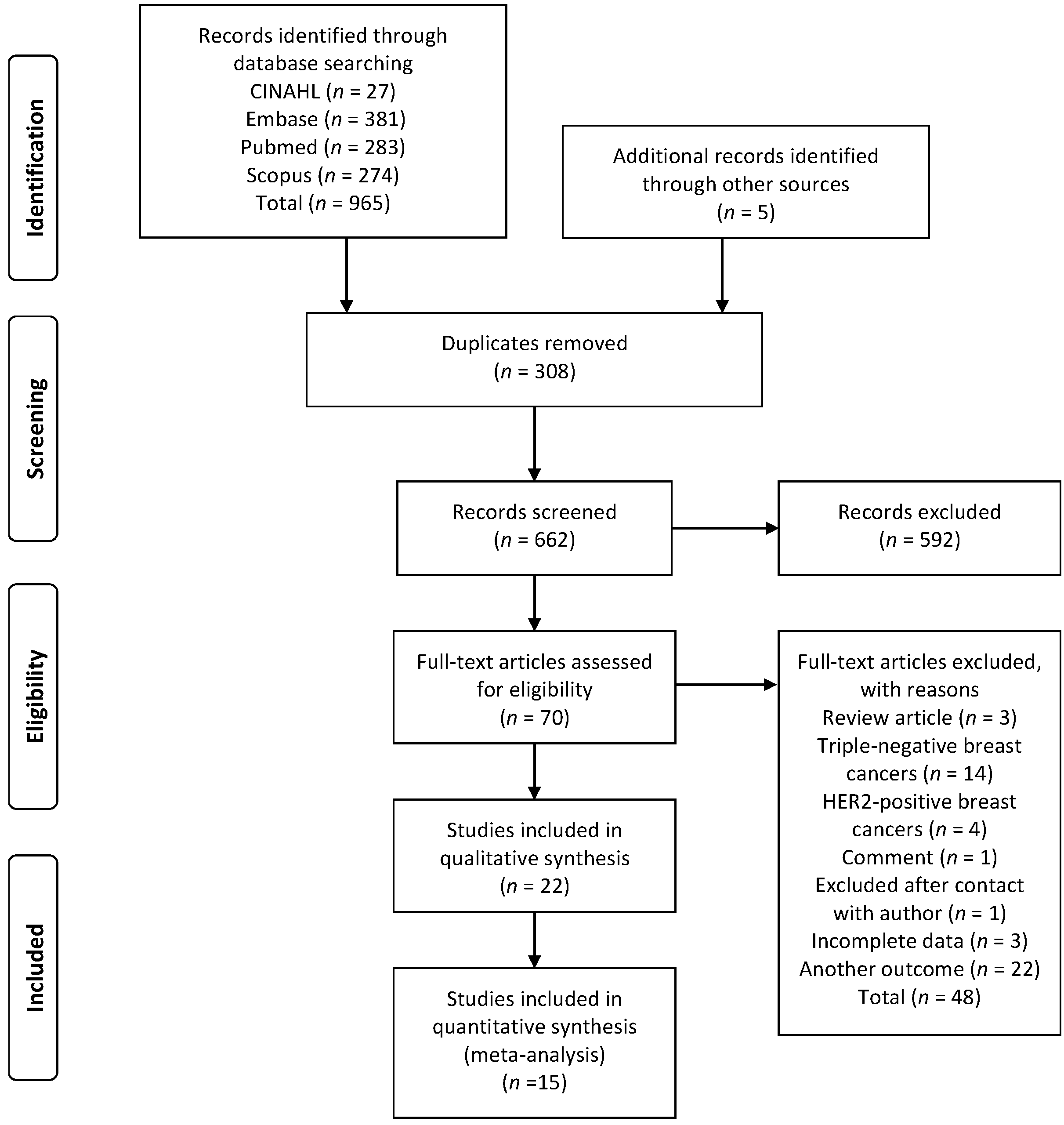
3.1. Identification of Studies
3.2. Study Characteristics
3.3. PD-L1 Expression and Patient Survival
3.4. Meta-Analysis
3.4.1. Expression of PD-L1 in TCs, ICs, and TCICs
3.4.2. PD-L1 Expression and Clinicopathological Characteristics
3.4.3. Age
3.4.4. Lymph Node Status
3.4.5. PR Status
3.4.6. Ki-67 Index
3.4.7. HER2 Status
3.4.8. PD-L1 Expression and OS
3.4.9. PD-L1 Expression and DFS
3.5. Quality Assessment and Risk of Bias
3.6. Publication Bias
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zhang, Y.; Tian, J.; Qu, C.; Tang, Z.; Wang, Y.; Li, K.; Yang, Y.; Liu, S. Prognostic value of programmed cell death ligand-1 expression in breast cancer: A meta-analysis. Medicine 2020, 99, e23359. [Google Scholar] [CrossRef]
- Mina, L.A.; Lim, S.; Bahadur, S.W.; Firoz, A.T. Immunotherapy for the Treatment of Breast Cancer: Emerging New Data. Breast Cancer 2019, 11, 321–328. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Kang, S.; Shen, J.; He, J.; Jiang, L.; Wang, W.; Guo, Z.; Peng, G.; Chen, G.; He, J.; et al. Prognostic significance of programmed cell death 1 (PD-1) or PD-1 ligand 1 (PD-L1) Expression in epithelial-originated cancer: A meta-analysis. Medicine 2015, 94, e515. [Google Scholar] [CrossRef] [PubMed]
- Mittendorf, E.A.; Zhang, H.; Barrios, C.H.; Saji, S.; Jung, K.H.; Hegg, R.; Koehler, A.; Sohn, J.; Iwata, H.; Telli, M.L.; et al. Neoadjuvant atezolizumab in combination with sequential nab-paclitaxel and anthracycline-based chemotherapy versus placebo and chemotherapy in patients with early-stage triple-negative breast cancer (IMpassion031): A randomised, double-blind, phase 3 trial. Lancet 2020, 396, 1090–1100. [Google Scholar] [CrossRef]
- Adams, S.; Loi, S.; Toppmeyer, D.; Cescon, D.W.; De Laurentiis, M.; Nanda, R.; Winer, E.P.; Mukai, H.; Tamura, K.; Armstrong, A.; et al. Pembrolizumab monotherapy for previously untreated, PD-L1-positive, metastatic triple-negative breast cancer: Cohort B of the phase II KEYNOTE-086 study. Ann. Oncol. 2019, 30, 405–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Telli, M.L.; Vinayak, S. Future of checkpoint blockade in triple-negative breast cancer: Combination strategies to lead the way. Ann. Oncol. 2019, 30, 347–348. [Google Scholar] [CrossRef] [PubMed]
- Loibl, S.; Untch, M.; Burchardi, N.; Huober, J.; Sinn, B.V.; Blohmer, J.U.; Grischke, E.M.; Furlanetto, J.; Tesch, H.; Hanusch, C.; et al. A randomised phase II study investigating durvalumab in addition to an anthracycline taxane-based neoadjuvant therapy in early triple-negative breast cancer: Clinical results and biomarker analysis of GeparNuevo study. Ann. Oncol. 2019, 30, 1279–1288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmid, P.; Rugo, H.S.; Adams, S.; Schneeweiss, A.; Barrios, C.H.; Iwata, H.; Diéras, V.; Henschel, V.; Molinero, L.; IMpassion130 Investigators; et al. Atezolizumab plus nab-paclitaxel as first-line treatment for unresectable, locally advanced or metastatic triple-negative breast cancer (IMpassion130): Updated efficacy results from a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2020, 21, 44–59. [Google Scholar] [CrossRef]
- Stovgaard, E.S.; Dyhl-Polk, A.; Roslind, A.; Balslev, E.; Nielsen, D. PD-L1 expression in breast cancer: Expression in subtypes and prognostic significance: A systematic review. Breast Cancer Res Treat. 2019, 174, 571–584. [Google Scholar] [CrossRef]
- Liberati., A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Zhu, H.; Zhou, Y.; Mao, F.; Lin, Y.; Pan, B.; Zhang, X.; Xu, Q.; Huang, X.; Sun, Q. Prognostic Value of PD-L1 in Breast Cancer: A Meta-Analysis. Breast J. 2017, 23, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Yazdanpanah, P.; Alavianmehr, A.; Ghaderi, A.; Monabati, A.; Montazer, M.; Tahmasbi, K.; Farjadian, S. PD-L1 expression in tumor lesions and soluble PD-L1 serum levels in patients with breast cancer: TNBC versus TPBC. Breast Dis. 2021, 40, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Hayden, J.A.; van der Windt, D.A.; Cartwright, J.L.; Côté, P.; Bombardier, C. Assessing bias in studies of prognostic factors. Ann. Intern. Med. 2013, 158, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Carrasco-Labra, A.; Brignardello-Petersen, R.; Santesso, N.; Neumann, I.; Mustafa, R.A.; Mbuagbaw, L.; Etxeandia Ikobaltzeta, I.; De Stio, C.; McCullagh, L.J.; Alonso-Coello, P.; et al. Improving GRADE evidence tables part 1: A randomized trial shows improved understanding of content in summary of findings tables with a new format. J. Clin. Epidemiol. 2016, 74, 7–18. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef]
- Noll, M.; Kjaer, P.; Mendonça, C.R.; Wedderkopp, N. Motor performance and back pain in children and adolescents: A systematic review. Eur. J. Pain 2021. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557. [Google Scholar] [CrossRef] [Green Version]
- Sim, J.; Wright, C.C. The kappa statistic in reliability studies: Use, interpretation, and sample size requirements. Phys. Ther. 2005, 85, 257–268. [Google Scholar] [CrossRef] [Green Version]
- Catacchio, I.; Silvestris, N.; Scarpi, E.; Schirosi, L.; Scattone, A.; Mangia, A. Intratumoral, rather than stromal, CD8+ T cells could be a potential negative prognostic marker in invasive breast cancer patients. Transl. Oncol. 2019, 12, 585–595. [Google Scholar] [CrossRef]
- Evangelou, Z.; Papoudou-Bai, A.; Karpathiou, G.; Kourea, H.; Kamina, S.; Goussia, A.; Harissis, H.; Peschos, D.; Batistatou, A. PD-L1 Expression and Tumor-infiltrating Lymphocytes in Breast Cancer: Clinicopathological Analysis in Women Younger than 40 Years Old. In Vivo 2020, 34, 639–647. [Google Scholar] [CrossRef] [Green Version]
- Guo, H.; Ding, Q.; Gong, Y.; Gilcrease, M.Z.; Zhao, M.; Zhao, J.; Sui, D.; Wu, Y.; Chen, H.; Liu, H.; et al. Comparison of three scoring methods using the FDA-approved 22C3 immunohistochemistry assay to evaluate PD-L1 expression in breast cancer and their association with clinicopathologic factors. Breast Cancer Res. 2020, 22, 69. [Google Scholar] [CrossRef] [PubMed]
- Hong, M.; Kim, J.W.; Kim, M.K.; Chung, B.W.; Ahn, S.K. Programmed cell death-ligand 1 expression in stromal immune cells is a marker of breast cancer outcome. J. Cancer 2020, 11, 7246–7252. [Google Scholar] [CrossRef] [PubMed]
- Karnik, T.; Kimler, B.F.; Fan, F.; Tawfik, O. PD-L1 in breast cancer: Comparative analysis of 3 different antibodies. Hum. Pathol. 2018, 72, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Kurozumi, S.; Inoue, K.; Matsumoto, H.; Fujii, T.; Horiguchi, J.; Oyama, T.; Kurosumi, M.; Shirabe, K. Clinicopathological values of PD-L1 expression in HER2-positive breast cancer. Sci. Rep. 2019, 9, 16662. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.-W.; Ryu, H.S.; Jin, M.-S.; Lee, K.-H.; Suh, K.J.; Youk, J.; Kim, J.Y.; Min, A.; Lee, H.-B.; Moon, H.-G.; et al. Immune recurrence score using 7 immunoregulatory protein expressions can predict recurrence in stage I–III breast cancer patients. Br. J. Cancer. 2019, 121, 230–236. [Google Scholar] [CrossRef]
- Li, F.; Ren, Y.; Wang, Z. Programmed death 1 Ligand 1 expression in breast cancer and its association with patients’ clinical parameters. Cancer Res. Ther. 2018, 14, 150–154. [Google Scholar] [CrossRef]
- Manson, Q.F.; Schrijver, W.; Ter Hoeve, N.D.; Moelans, C.B.; van Diest, P.J. Frequent discordance in PD-1 and PD-L1 expression between primary breast tumors and their matched distant metastases. Clin. Exp. Metastasis 2019, 36, 29–37. [Google Scholar] [CrossRef] [Green Version]
- Manson, Q.F.; Ter Hoeve, N.D.; Buerger, H.; Moelans, C.B.; van Diest, P.J. PD-1 and PD-L1 Expression in Male Breast Cancer in Comparison with Female Breast Cancer. Target Oncol. 2018, 13, 769–777. [Google Scholar] [CrossRef] [Green Version]
- Noske, A.; Möbus, V.; Weber, K.; Schmatloch, S.; Weichert, W.; Köhne, C.H.; Solbach, C.; Ingold Heppner, B.; Steiger, K.; Müller, V.; et al. Relevance of tumour-infiltrating lymphocytes, PD-1 and PD-L1 in patients with high-risk, nodal-metastasised breast cancer of the German Adjuvant Intergroup Node-positive study. Eur. J. Cancer 2019, 114, 76–88. [Google Scholar] [CrossRef]
- Pelekanou, V.; Barlow, W.E.; Nahleh, Z.A.; Wasserman, B.; Lo, Y.C.; von Wahlde, M.K.; Hayes, D.; Hortobagyi, G.N.; Gralow, J.; Tripathy, D.; et al. Tumor-Infiltrating Lymphocytes and PD-L1 Expression in Pre- and Posttreatment Breast Cancers in the SWOG S0800 Phase II Neoadjuvant Chemotherapy Trial. Mol. Cancer Ther. 2018, 17, 1324–1331. [Google Scholar] [CrossRef] [Green Version]
- Shibel, P.E.E.; Abdelhamid, H.S.; Soliman, S.A.M.; Gabal, S.M. Investigation of Immunohistochemical Expression of Programmed Death-Ligand 1 (PD-L1) in Female Mammary Carcinoma and its Correlation with the Extent of Stromal Tumour Infiltrating Lymphocytes. J. Clin. Diagn. Res. 2019, 13, EC11–EC17. [Google Scholar] [CrossRef]
- Sobral-Leite, M.; Van de Vijver, K.; Michaut, M.; van der Linden, R.; Hooijer, G.K.J.; Horlings, H.M.; Severson, T.M.; Mulligan, A.M.; Weerasooriya, N.; Sanders, J.; et al. Assessment of PD-L1 expression across breast cancer molecular subtypes, in relation to mutation rate, BRCA1-like status, tumor-infiltrating immune cells and survival. Oncoimmunology 2018, 7, e1509820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szekely, B.; Bossuyt, V.; Li, X.; Wali, V.B.; Patwardhan, G.A.; Frederick, C.; Silber, A.; Park, T.; Harigopal, M.; Pelekanou, V.; et al. Immunological differences between primary and metastatic breast cancer. Ann. Oncol. 2018, 29, 2232–2239. [Google Scholar] [CrossRef] [PubMed]
- Tawfik, O.; Kimler, B.F.; Karnik, T.; Shehata, P. Clinicopathological correlation of PD-L1 expression in primary and metastatic breast cancer and infiltrating immune cells. Hum. Pathol. 2018, 80, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Wei, L.; Wu, N.; Wei, F.; Li, F.; Zhang, Y.; Liu, J.; Ren, X. Prognosis significance of indoleamine 2, 3-dioxygenase, programmed death ligand-1 and tumor-infiltrating immune cells in microenvironment of breast cancer. Int. Immunopharmacol. 2020, 84, 106506. [Google Scholar] [CrossRef] [PubMed]
- Yuan, C.; Liu, Z.; Yu, Q.; Wang, X.; Bian, M.; Yu, Z.; Yu, J. Expression of PD-1/PD-L1 in primary breast tumours and metastatic axillary lymph nodes and its correlation with clinicopathological parameters. Sci. Rep. 2019, 9, 14356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zerdes, I.; Sifakis, E.G.; Matikas, A.; Chrétien, S.; Tobin, N.P.; Hartman, J.; Rassidakis, G.Z.; Bergh, J.; Foukakis, T. Programmed death-ligand 1 gene expression is a prognostic marker in early breast cancer and provides additional prognostic value to 21-gene and 70-gene signatures in estrogen receptor-positive disease. Mol. Oncol. 2020, 14, 951–963. [Google Scholar] [CrossRef]
- Zhai, J.; Giannini, G.; Ewalt, M.D.; Zhang, E.Y.; Invernizzi, M.; Niland, J.; Lai, L.L. Molecular characterization of metaplastic breast carcinoma via next-generation sequencing. Hum. Pathol. 2019, 86, 85–92. [Google Scholar] [CrossRef]
- Zhao, Q.; Guo, Y.; Liu, C.; Huang, T. Prognostic value of PD-L1 for invasive breast cancer and its miR-34a-related mechanism of regulation. Int. J. Clin. Exp. Med. 2019, 12, 9984–9997. [Google Scholar]
- Zhou, T.; Xu, D.; Tang, B.; Ren, Y.; Han, Y.; Liang, G.; Wang, J.; Wang, L. Expression of programmed death ligand-1 and programmed death-1 in samples of invasive ductal carcinoma of the breast and its correlation with prognosis. Anticancer Drugs 2018, 29, 904–910. [Google Scholar] [CrossRef]
- Rugo, H.S.; Loi, S.; Adams, S.; Schmid, P.; Schneeweiss, A.; Barrios, C.H.; Iwata, H.; Diéras, V.; Winer, E.P.; Kockx, M.M.; et al. PD-L1 Immunohistochemistry Assay Comparison in Atezolizumab plus nab-Paclitaxel-Treated Advanced Triple-Negative Breast Cancer. J. Natl. Cancer Inst 2021, djab108. [Google Scholar] [CrossRef]
- De Melo Gagliato, D.; Buzaid, A.C.; Perez-Garcia, J.; Cortes, J. Immunotherapy in Breast Cancer: Current Practice and Clinical Challenges. BioDrugs 2020, 34, 611–623. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.; Woo, J.W.; Kim, H.; Cho, E.Y.; Kim, A.; Kim, J.Y.; Kim, C.; Lee, H.J.; Lee, J.S.; Bae, Y.K.; et al. Programmed Death Ligand 1 Immunohistochemistry in Triple-Negative Breast Cancer: Evaluation of Inter-Pathologist Concordance and Inter-Assay Variability. J. Breast Cancer 2021, 24, 266–279. [Google Scholar] [CrossRef] [PubMed]
- Pang, J.B.; Castles, B.; Byrne, D.J.; Button, P.; Hendry, S.; Lakhani, S.R.; Sivasubramaniam, V.; Cooper, W.A.; Armes, J.; Millar, E.K.A.; et al. kConFab. SP142 PD-L1 Scoring Shows High Interobserver and Intraobserver Agreement in Triple-negative Breast Carcinoma but Overall Low Percentage Agreement With Other PD-L1 Clones SP263 and 22C3. Am. J. Surg. Pathol. 2021, 45, 1108–1117. [Google Scholar] [CrossRef]
- Cortes, J.; Cescon, D.W.; Rugo, H.S.; Nowecki, Z.; Im, S.A.; Yusof, M.M.; Gallardo, C.; Lipatov, O.; Barrios, C.H.; Holgado, E.; et al. KEYNOTE-355 Investigators. Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer (KEYNOTE-355): A randomised, placebo-controlled, double-blind, phase 3 clinical trial. Lancet 2020, 396, 1817–1828. [Google Scholar] [CrossRef]
- Ahn, S.G.; Kim, S.K.; Shepherd, J.H.; Cha, Y.J.; Bae, S.J.; Kim, C.; Jeong, J.; Perou, C.M. Clinical and genomic assessment of PD-L1 SP142 expression in triple-negative breast cancer. Breast Cancer Res. Treat. 2021, 188, 165–178. [Google Scholar] [CrossRef] [PubMed]
- Dieci, M.V.; Tsvetkova, V.; Griguolo, G.; Miglietta, F.; Tasca, G.; Giorgi, C.A.; Cumerlato, E.; Massa, D.; Lo Mele, M.; Orvieto, E.; et al. Integration of tumour infiltrating lymphocytes, programmed cell-death ligand-1, CD8 and FOXP3 in prognostic models for triple-negative breast cancer: Analysis of 244 stage I-III patients treated with standard therapy. Eur. J. Cancer 2020, 136, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Li, A.; Zhou, S.; Xu, Y.; Xiao, Y.; Bi, R.; Yang, W. Heterogeneity of PD-L1 expression in primary tumors and paired lymph node metastases of triple negative breast cancer. BMC Cancer 2018, 18, 4. [Google Scholar] [CrossRef] [Green Version]
- Boman, C.; Zerdes, I.; Mårtensson, K.; Bergh, J.; Foukakis, T.; Valachis, A.; Matikas, A. Discordance of PD-L1 status between primary and metastatic breast cancer: A systematic review and meta-analysis. Cancer Treat. Rev. 2021, 99, 102257. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Databases | Search Strategy |
|---|---|
| Medline/PubMed (28 January 2021) | Search: (Breast Cancer) AND (PD-L1 expression). Filters: humans, from 2018–2021, sort by: most recent ((“breast neoplasms”[MeSH Terms] OR (“breast”[All Fields] AND “neoplasms”[All Fields]) OR “breast neoplasms”[All Fields] OR (“breast”[All Fields] AND “cancer”[All Fields]) OR “breast cancer”[All Fields]) AND (“PD-L1”[All Fields] AND (“express”[All Fields] OR “expresse”[All Fields] OR “expresses”[All Fields] OR “expressing”[All Fields] OR “expressions”[All Fields] OR “gene expression”[MeSH Terms] OR (“gene”[All Fields] AND “expression”[All Fields]) OR “gene expression”[All Fields] OR “expressed”[All Fields] OR “expression”[All Fields]))) AND ((humans[Filter]) AND (2018:2021[pdat])) Total: 283 |
| CINAHL (28 January 2021) | Boolean/phrase: breast cancer AND PD-L1 expression Limiters Published date: 2018/01/01–2021/01/28 Gender: female Total: 27 |
| EMBASE (28 January 2021) | 1 breast cancer.mp. or breast cancer/ 543437 2 programmed death 1 ligand 1/ or PD-L1 expression.mp. 32620 3 1 and 2 2698 4 limit to (human and female and yr = “2018–2021”)1029 5 limit to article Total: 381 |
| Scopus (28 January 2021) | TITLE-ABS-KEY (breast AND cancer AND pd-l1 AND expression) AND (LIMIT-TO (PUBYEAR, 2021) OR LIMIT-TO (PUBYEAR, 2020) OR LIMIT-TO (PUBYEAR, 2019) OR LIMIT-TO (PUBYEAR, 2018)) AND (LIMIT-TO (DOCTYPE, “ar”)) AND (LIMIT-TO (EXACTKEYWORD, “Human”)) AND (LIMIT-TO (LANGUAGE, “English”)) AND (LIMIT-TO (SRCTYPE,”j”)) AND (LIMIT-TO (EXACTKEYWORD, “Female”)) Total: 274 |
| Reference | N | Study Designs/Follow-Up (Mean) | Breast Cancer Subtype | Therapeutic Plan | Pathologic Material | Anti-PD-L1 Clone | Determination Criteria | PD-L1 Expression (TC) | PD-L1 Expression (IC) | PD-L1 Expression (TCICs) | Conflict of Interests | Ethical Approval | Quality of Evidence (GRADE) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Catacchio et al., 2019 [20] (Italy) | 180 | Study retrospective—cohort Follow-up: 63 months (range 3–203) | NE | CT: 16.2% (26/160) CT + hormone therapy: 40% (64/160) HT: 43.8% (70/160) Treatment data were not available: 11.1% (20/180) | TMA | SP263 | TC and IC: only membranous staining ≥1% | 7/167 (4.0%) | 35/168 (21.0%) | NR | No | Yes | ⊕⊕⊕◯ moderate |
| Evangelou et al., 2020 [21] (Greece) | 45 | Study retrospective—cohort Follow-up: NR | NE | NR | Full section | E1L3N | TC: only membranous staining ≥1% IC:membranous/cytoplasmic staining ≥1% | 9/45 (20.0%) | 20/45 (44.4%) | NR | No | NR | ⊕⊕◯◯ low |
| Guo et al., 2020 [22] (USA) | 496 | Cohort Follow-up: ranged from 3 months to 154 months (median follow-up, 48 months). | ER/PR pos 73.1% (247/338) HER2 9.2% (31/338) TNBC 17.7% (60/338) | No NACT: 70.4% (349/ 496) NACT at the time of surgical excision: 29.6% (147/496) | TMA | 22C3 | TC and IC: membranous/cytoplasmic staining ≥1% | 46/470 (9.8%) | 77/470 (16.4%) | 94/470 (20.0%) | No | Yes | ⊕⊕⊕◯ moderate |
| Hong et al., 2020 [23] (Korea) | 233 | Cohort Follow-up: 45 months (1–82 months) | Luminal A 32.0% (71/222) Luminal B 41.9% (93/222) Basal 16.2% (36/222) HER2 9.9% (22/222) | CT: 85.1% (194/228) HT: 73.1% (163/223) | TMA | SP263 | TC: membranous/cytoplasmic staining | 28/233 (12.0%) | 66/233 (28.3%) | NR | No | Yes | ⊕⊕⊕◯ moderate |
| Karnik et al., 2018 [24] (USA) | 136 | Cohort Follow-up: NR | Luminal A: 29% (40/136) Luminal B: 40% (55/136) TN: 18% (25/136) HER2: 4% (6/136) Unknown: 7% (10/136) | NR | Full section | SP263 22C3 CAL 10 | TC: only membranous staining ≥1%. IC: Not evaluated | 8/42 (19.0%) | NR | NR | No | Yes | ⊕⊕⊕◯ moderate |
| Kurozumi et al., 2019 [25] (Japan) | 248 | Cohort Follow-up: 128 (range, 1–147) months | HR-positive and HER2-negative: 63.7% (158/248) HER2-positive: 17.3% (43/248) Triple-negative: 19.0% (47/248) | All without CT | Full section | SP142 | TC: cytoplasmic and/or membrane staining ≥1%. IC: not reported | 20/248 (8.1%) | NR | NR | Yes | Yes | ⊕⊕⊕◯ moderate |
| Lee D et al., 2019 [26] (Korea) | 392 | Cohort Follow-up: 89 months, 50 recurrent events occurred | Luminal A: 69.1% (271/392) Luminal B: 9.2% (36/392) HER2-positive: 8.2% (32/392) Triple-negative: 13.5% (53/392) | Adjuvant CT 77.8% (305/392) Adjuvant HT 71.9% (282/392) Adjuvant radiotherapy 66.1% (259/392). No NACT | TMA | B7-H1 | TC and IC: not reported | 15/392 (3.8%) | 47/392 (12.0%) | NR | No | Yes | ⊕⊕⊕◯ moderate |
| Li Fei et al., 2018 [27] (China) | 112 | Study retrospective | NR | All without radiotherapy and chemotherapy before the surgery | Full section | Abcam—polyclonal | TC: membranous and cytoplasmic staining | 22/112 (19.6%) | NR | NR | No | NR | ⊕⊕⊕◯ moderate |
| Manson et al., 2018 [29] (The Netherlands) | 246 | Cohort Follow-up: was 8.5 years (range 0.1– 22.1 years) | Luminal: 82.1% (202/246) HER2-driven: 3.7% (9/246) Triple-negative: 14.2% (35/246) | NR | TMA | SP263 | TC and IC: membranous/cytoplasmic staining ≥1% | 44/218 (20.2%) | 95/218 (43.6%) | NR | No | Not required | ⊕⊕⊕◯ moderate |
| Manson et al., 2019 [28] (The Netherlands) | 106 | Cohort Follow-up: 5.1 years (range 1.3–25.9 years) | Luminal: 65.7% (69/105) HER2 driven: 11.4% (12/105) Triple-negative: 22.9% (24/105) | NR | TMA | SP263 | TC and IC: membranous/cytoplasmic staining ≥1% | 18/75 (24.0%) | 32/75 (42.7%) | NR | No | Not required | ⊕⊕⊕◯ moderate |
| Noske et al., 2019 [30] (Germany) | 1318 | GAIN-1 study (ClinicalTRials.gov NCT0019687) was a prospective multicenter phase III trial Follow-up: NR | Luminal A: 42.0% (542/1318) Luminal B: 36.0% (465/1318) ER-/PR-/HER2+: 7.9% (102/1318) Triple-negative: 14.1% (182/1318) | Epirubicin, paclitaxel and cyclophosphamide: 50.4% (664/1318) Epirubicin, cyclophosphamide, paclitaxel and capecitabine: 49.6% (654/1318) | TMA | SP263 | Cellular localization: TC: cell membrane (partially or completely stained). Cytoplasmatic staining was disregarded. IC: any PD-L1 staining (membrane/cytoplasm) | 33/1100 (3.0%) | 178/1100 (16.2%) | NR | Yes | Yes | ⊕⊕⊕⊕ high |
| Pelekanou et al., 2018 [31] (USA) | 211 | Study prospectively—Cohort Follow-up: 3 years | NE | CT: 46,5% (98/211) | Full section | 22C3 | TC and IC: membranous/cytoplasmic staining ≥1% | NR | NR | 52/120 (43%) | No | NR | ⊕⊕⊕⊝ moderate |
| Shibel et al., 2019 [32] (Egypt) | 100 | Cross-sectional study Follow-up: NR | Luminal A: 32% (32/100) Luminal B: 42% (42/100) HER2 enriched: 10% (10/100) Triple-negative: 16% (16/100) | Cases who received neo-adjuvant therapy were excluded; either hormonal or chemotherapy | Full section | Polyclonal (Novus Biologicals) | TC and IC: membranous/cytoplasmic staining ≥1% | 61/100 (61%) | 55/100 (55.0%) | NR | No | Yes | ⊕⊕⊕◯ moderate |
| Sobral-Leite et al., 2018 [33] (The Netherlands) | 118 | Cohort Follow-up: 10-years | NE | CT: 15.4% (25/162) Endocrine therapy: 35.8% (58/162) Radiotherapy 19.1% (31/162) | TMA and full section | E1L3N | TC: membranous/cytoplasmic staining ≥1% IC: membranous/cytoplasmic staining ≥5% | NR | NR | 79/144 (54.9%) | No | Yes | ⊕⊕⊕◯ moderate |
| Szekely et al., 2018 [34] (USA) | 45 | Cohort Follow-up: NR | NE | NR | TMA and full section | E1L3N | TC and IC: membranous/cytoplasmic staining ≥1% | NR | NR | 18/35 (52.0%) | Yes | Yes | ⊕⊕◯◯ low |
| Tawfik et al., 2018 [35] (USA) | 133 | Cohort Follow-up: NR | NE | NR | Full section | SP263 | TC and IC: membranous/cytoplasmic staining ≥1% | 7/41 (17.1%) | 22/41 (53.7%) | NR | No | Yes | ⊕⊕⊕◯ moderate |
| Wei et al., 2020 [36] (China) | 77 | Cohort Follow-up: NR | Luminal A: 11.69% (9/77) Luminal B: 61.04% (47/77) HER2-positive: 6.49% (5/77) Triple-negative: 20.78% (16/77) | Patients did not receive chemotherapy, hormone therapy or immunotherapy before surgery | Full section | EPR19759 | TC: only membranous staining ≥ 25%. IC: not evaluated | 19/77 (24.68%) | NR | NR | No | Yes | ⊕⊕◯◯ low |
| Yuan et al., 2019 [37] (China) | 47 | Cohort Follow-up: NR | Luminal A: 21% (10/47) Luminal B: 49% (23/47) HER-2+: 21% (10/47) Triple-negative: 9% (4/47) | NR | Full section | Not reported | Not reported | NR | NR | 14/47 (29.8%) | No | Yes | ⊕⊕◯◯ low |
| Zerdes et al., 2020 [38] (Sweden) | Cohort 1 (562)Cohort 2 (1081) | Cohort Follow-up: 12.4 years and 15 years | Luminal A: 44.3% (249/562) Luminal B: 19.0% (107/562) HER2-enriched: 11.4% (64/562) Basal-like: 21.7% (122/562) Normal-like: 3.2% (18/562) Unknown: 0.4% (2/562) | ET: 29.7% (167/562) CT: 27.8% (156/562) ET/CT: 39.5% (222/562) | TMA | SP263 | Not reported | 48/490 (9.8%) | 116/490 (23.7%) | 121/490 (24.7%) | Yes | Yes | ⊕⊕⊕⊕ high |
| Zhai et al., 2019 [39] (China) | 160 | Cohort Follow-up: 118 months | Luminal A: 50/160 (31.6%) Luminal B: 27.5% (44/160) Basal-like: 5.6% (9/160) Triple-negative: 23.8% (38/160) | NR | TMA | E1L3N | Not reported | 11/149 (7.4%) | 29/149 (19.5%) | NR | Yes | Yes | ⊕⊕⊕◯ moderate |
| Zhao et al., 2019 [40] (China) | 286 | Cohort Follow-up: NR | Luminal A: 43,7% 125/286 Luminal B: 24.8% 71/286 Her2 overexpression: 11.2% 32/286 Triple-negative: 20.3% 58/286 | All patients included in this study had received standardized surgery, chemotherapy, radiotherapy, endocrine therapy, and targeted therapy according to NCCN guidelines | TMA | E1L3N | TC:intensity and the percentage of cytoplasmic staining. IC: not evaluated | 165/286 (57.7%) | NR | NR | No | Yes | ⊕⊕⊕◯ moderate |
| Zhou et al., 2018 [41] (China) | 136 | Cohort Follow-up: 2 months and the median follow-up duration was 45.3 months | Luminal A: type 19.9% (27/136) Luminal B: type 14% (19/136) Luminal B +: type 18.4% (25/136) Her-2 Overexpression: 13.9% (19/136) Triple-negative: 33.8% (46/136) | None of the 136 patients received any form of chemotherapy, radiotherapy, endocrine therapy, or targeted therapy before surgery | Full section | Ab213524 | TC: intensity and the percentage of cytoplasmic staining. IC: not evaluated | 45/136 (33.1%) | NR | NR | No | Yes | ⊕⊕⊕◯ moderate |
| Survival | ||
|---|---|---|
| Overall Survival | ||
| Reference | Follow-Up | Association—Descriptive Statistics |
| Guo et al., 2020 [22] | Ranged from 3 months to 154 months (median follow-up, 48 months) | Kaplan–Meier curves Positive PD-L1 staining by IC was significantly associated with worse overall survival in the subgroup with NACT (p= 0.021) PD-L1 staining by TCICs showed a trend for worse overall survival (p= 0.064) |
| Manson et al., 2018 [29] | 8.5 years (range 0.1–22.1 years) | Kaplan–Meier curves PD-L1 p = 0.564 PD-L1 tumor cells (p = 0.776) PD-L1 immune cells (p = 0.83) |
| Manson Quirine et al., 2019 [28] | 5.1 years (range 1.3–25.9 years) | Kaplan–Meier curves PD-L1 tumor cells (p = 0.449) Univariate Cox regression analysis HR 3.013, CI 1201–7561, p = 0.019 |
| Zhai et al., 2019 [39] | 118 months | Kaplan–Meier curves Tumoral or stromal PD-L1 expression were linked to better survival outcome (p = 0.047 and p = 0.026) |
| Zhao et al., 2019 [40] | NR | Kaplan–Meier curves Expression of PD-L1 is significantly associated with OS (p = 0.001) High PD-L1 expression patients had significantly shorter OS Univariate Cox regression analysis PD-L1 HR 2.299, 95% CI 1.389–3.803, p= 0.001 |
| Disease-Free Survival | ||
| Reference | Follow-Up | Association—Descriptive Statistics |
| Catacchio et al., 2019 [20] | 63 months (range 3–203) | Univariate Cox regression analysis TILs HR 2.06, 95% CI 0.62–6.85, p= 0.228 Tumor cells HR 1.89, 95% CI 0.24–14.69, p= 0.534 |
| Hong et al., 2020 [23] | 45 months (1–82 months) | Univariate Cox regression analysis HR 0.084,95%, CI 0.011–0.645, p= 0.017 |
| Lee D et al., 2019 [26] | 89 months, 50 recurrent events occurred | Kaplan–Meier curves Expression of PD-L1 (TILs) (5-year DFS 100.0% vs. 87.7%, p =0.090) The estimated 5-year DFS of the entire cohort was 89.1% |
| Zhou et al., 2018 [41] | 2 months and the median follow-up duration was 45.3 months | Multivariate Cox regression analysis PD-L1 in tumor cells was found to be an independent prognostic risk factor with the PFS rate for breast invasive ductal carcinoma, HR = 3.93, 95% CI 1.15–13.46, p =0.003) Kaplan–Meier curves Kaplan–Meier estimates of the progression-free survival of patients with PD-L1 expression (p =0.018) |
| Kurozumi et al., 2019 [25] | 128 (range, 1–147) months | Kaplan–Meier curves of overall survival PD-L1 expression was not an independent prognostic facto (HR = 0.51, 95% CI 0.17–1.56, p = 0.24). |
| PD-L1-TC | p Value | References | PD-L1-IC | p Value | References | |
|---|---|---|---|---|---|---|
| Age (years) | <0.001 | [20,23,39,41] | <0.001 | [22,23,39] | ||
| <50 | 33% | 38% | ||||
| ≥50 | 67% | 62% | ||||
| Tumor size (cm) | 0.990 | [20,22,23,25,27,29] | 0.791 | [20,22,23,29] | ||
| ≤2 | 49% | 51% | ||||
| >2 | 49% | 49% | ||||
| Lymph node status | 0.190 | [20,21,27,41] | <0.001 | [20,21] | ||
| (–) | 42% | 66% | ||||
| (+) | 48% | 34% | ||||
| ER | 0.094 | [20,21,22,23,28,29,32,33,40,41] | 0.076 | [20,21,22,23,28,29,32,39] | ||
| (–) | 60% | 44% | ||||
| (+) | 47% | 56% | ||||
| PR | <0.001 | [20,21,22,23,24,28,29,32,33,40,41] | 0.182 | [20,21,22,23,28,29,32,39] | ||
| (–) | 62% | 56% | ||||
| (+) | 38% | 46% | ||||
| MIB1/ki67 expression | 0.023 | [20,21,23,25,32,40,41] | 0.005 | [20,21,23,32] | ||
| Low | 36% | 35% | ||||
| High | 72% | 65% | ||||
| HER2 | <0.001 | [20,21,22,23,24,28,29,30,40,41] | <0.001 | [20,21,22,23,28,29,30,39] | ||
| (–) | 76% | 74% | ||||
| (+) | 24% | 26% | ||||
| Molecular subtypes | ||||||
| - | [23,26,30,32,37,40] | 0.478 | [23,26,30,31,39] | |||
| Luminal A | 21% | 16% | ||||
| - | [23,26,32,37,39,40,41] | 0.610 | [23,26,32,39] | |||
| Luminal B | 24% | 29% | ||||
| - | [30,32,37,40] | 0.639 | [30,32] | |||
| HER2 overexpression | 13% | 11% | ||||
| - | [24,26,30,32,37,40] | 0.751 | [26,30,32,39] | |||
| TNBC | 40% | 37% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cirqueira, M.B.; Mendonça, C.R.; Noll, M.; Soares, L.R.; de Paula Carneiro Cysneiros, M.A.; Paulinelli, R.R.; Moreira, M.A.R.; Freitas-Junior, R. Prognostic Role of PD-L1 Expression in Invasive Breast Cancer: A Systematic Review and Meta-Analysis. Cancers 2021, 13, 6090. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13236090
Cirqueira MB, Mendonça CR, Noll M, Soares LR, de Paula Carneiro Cysneiros MA, Paulinelli RR, Moreira MAR, Freitas-Junior R. Prognostic Role of PD-L1 Expression in Invasive Breast Cancer: A Systematic Review and Meta-Analysis. Cancers. 2021; 13(23):6090. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13236090
Chicago/Turabian StyleCirqueira, Magno Belém, Carolina Rodrigues Mendonça, Matias Noll, Leonardo Ribeiro Soares, Maria Auxiliadora de Paula Carneiro Cysneiros, Regis Resende Paulinelli, Marise Amaral Rebouças Moreira, and Ruffo Freitas-Junior. 2021. "Prognostic Role of PD-L1 Expression in Invasive Breast Cancer: A Systematic Review and Meta-Analysis" Cancers 13, no. 23: 6090. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13236090