
Impact of Prostate Size on the Outcomes of Radical Prostatectomy: A Systematic Review and Meta-Analysis


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Data Extraction
2.3. Primary Outcomes
2.4. Statistical Analysis
3. Results
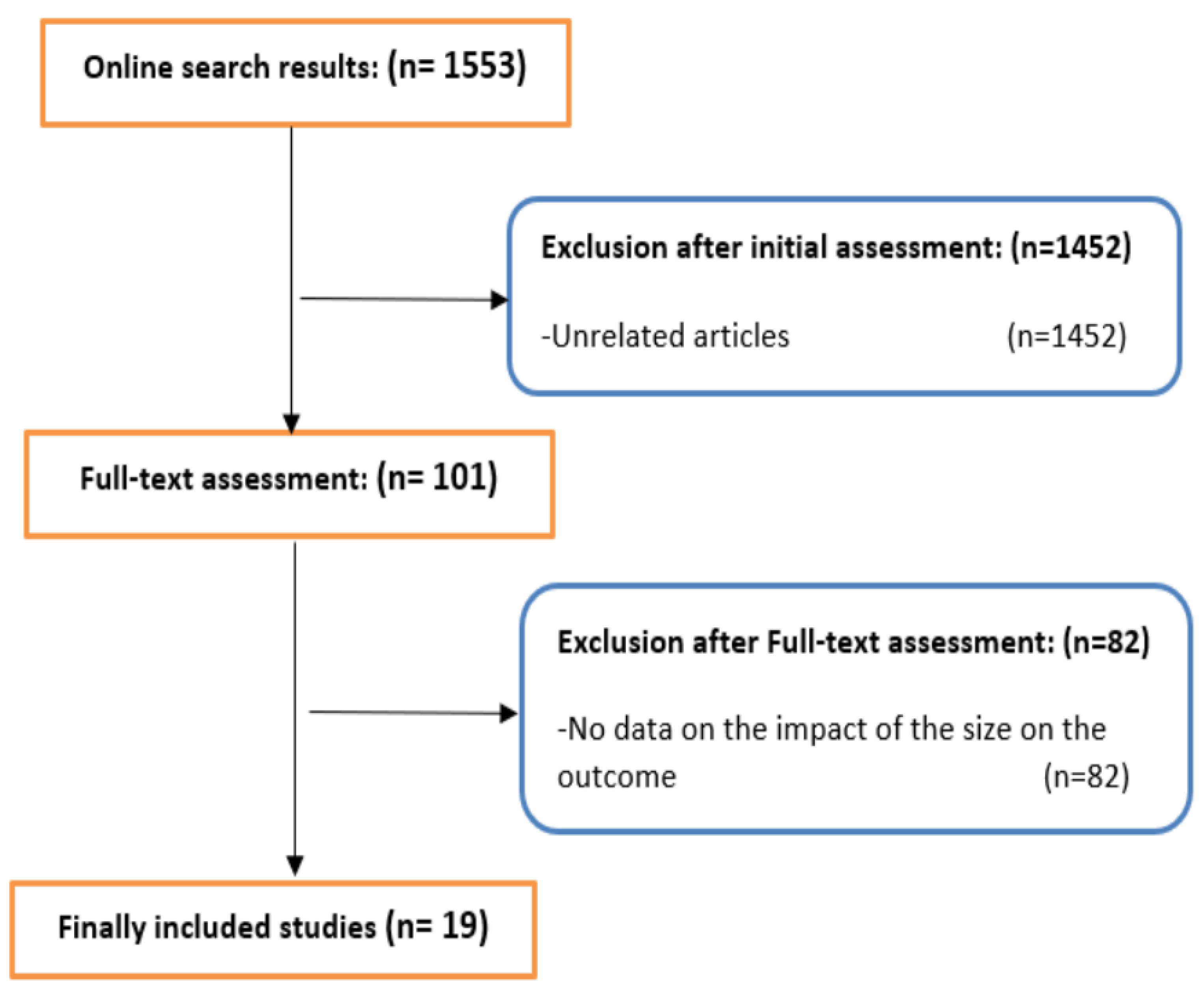
3.1. Search Results
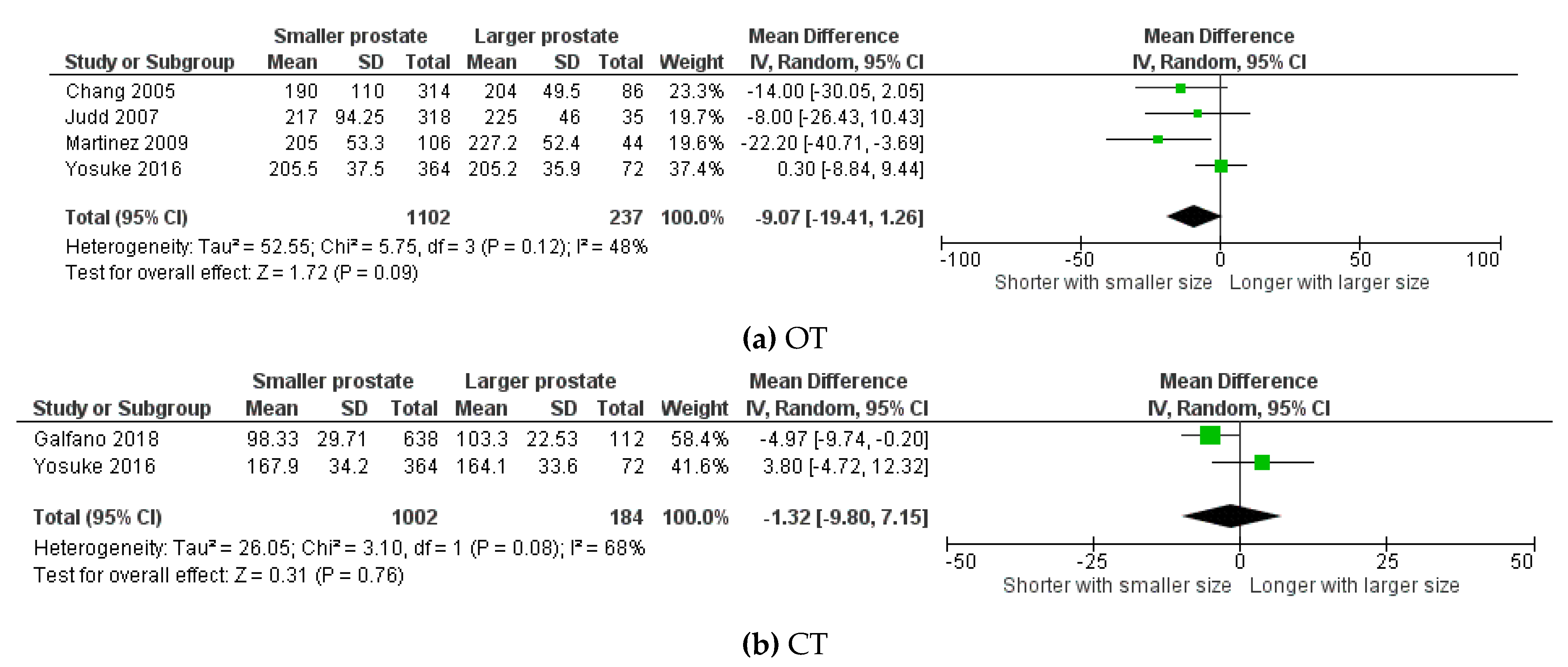
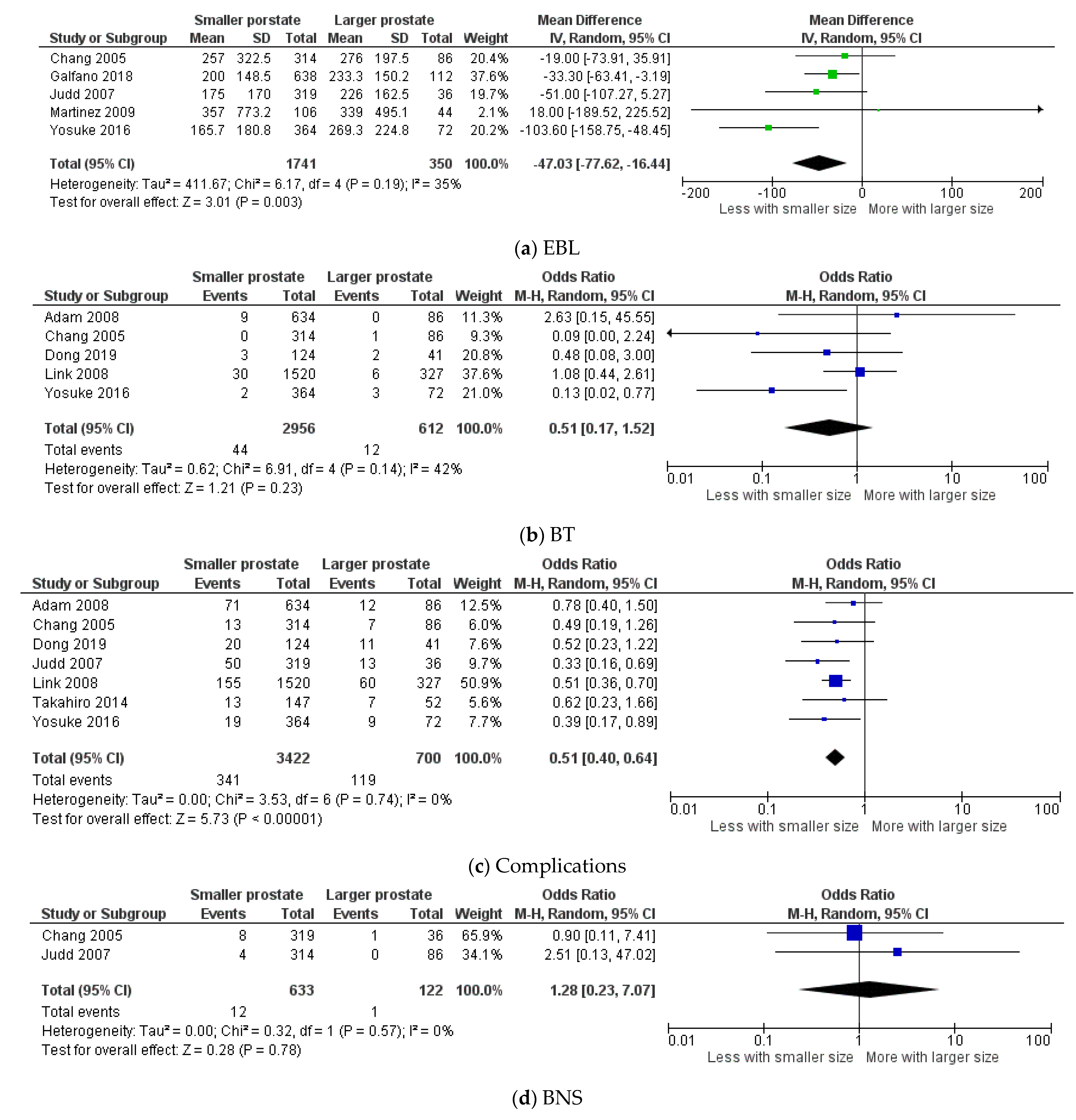
3.2. Perioperative Outcomes
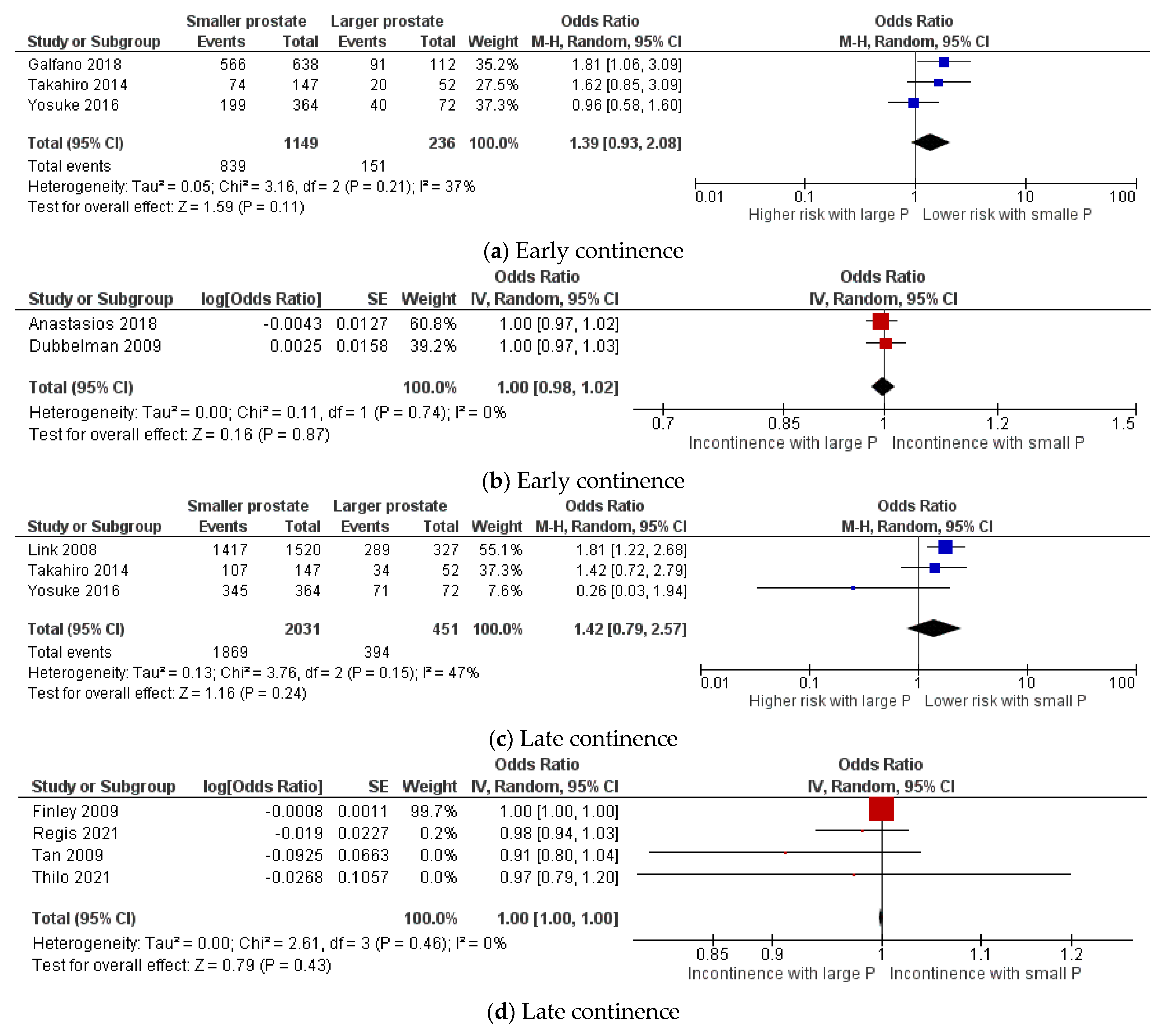
3.3. Functional Outcomes
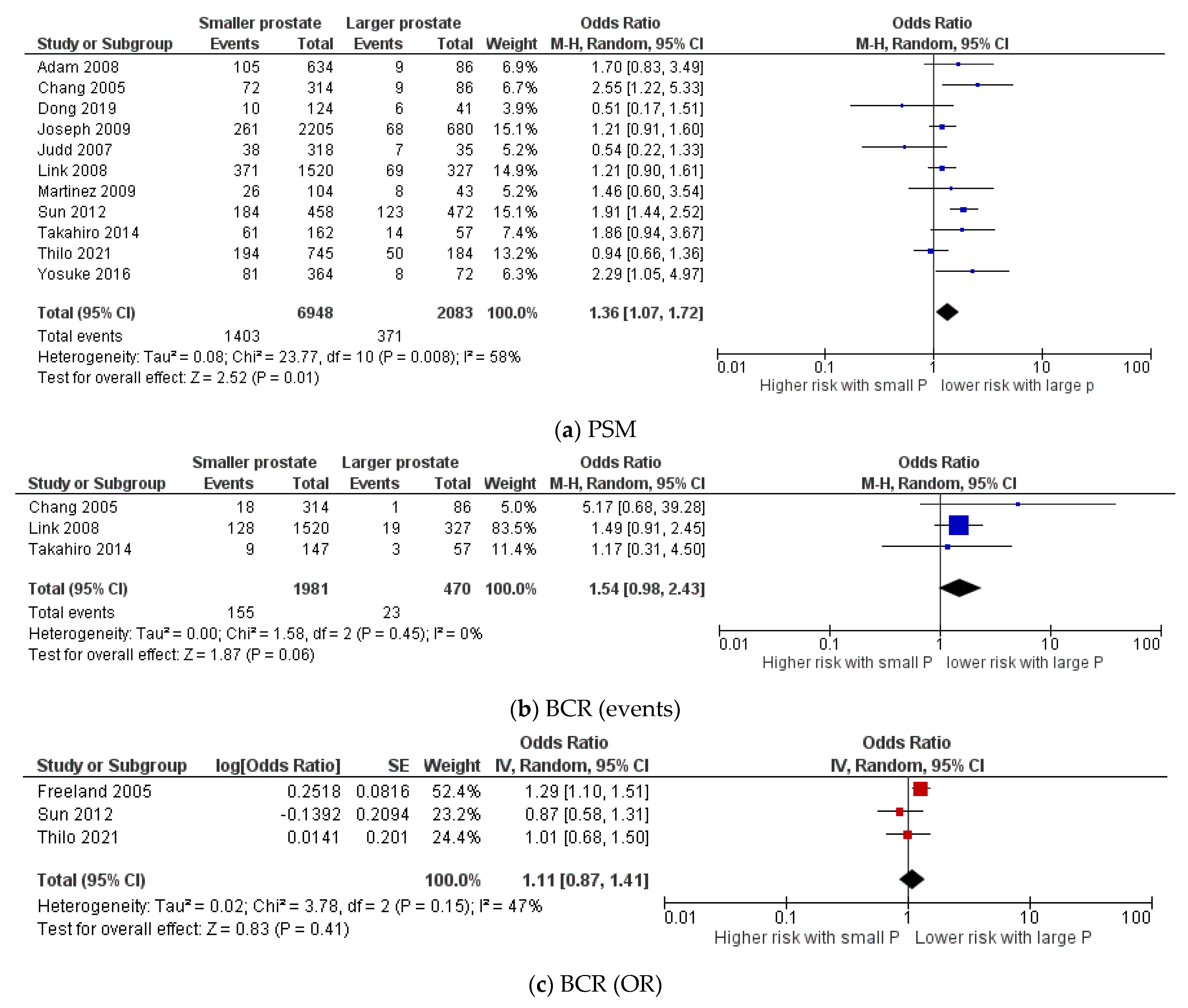
3.4. Oncological Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rawla, P. Epidemiology of Prostate Cancer. World J. Oncol. 2019, 10, 63–89. [Google Scholar] [CrossRef] [Green Version]
- Fahmy, O.; Khairul-Asri, M.G.; Hadi, S.H.; Gakis, G.; Stenzl, A. The Role of Radical Prostatectomy and Radiotherapy in Treatment of Locally Advanced Prostate Cancer: A Systematic Review and Meta-Analysis. Urol. Int. 2017, 99, 249–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Millin, T. Retropubic Prostatectomy: A New Extravesical Technique: Report of 20 Cases. Lancet 1945, 2, 693–696. [Google Scholar] [CrossRef]
- Walsh, P.C.; Lepor, H.; Eggleston, J.C. Radical prostatectomy with preservation of sexual function: Anatomical and pathological considerations. Prostate 1983, 4, 473–485. [Google Scholar] [CrossRef] [PubMed]
- Schuessler, W.W.; Schulam, P.G.; Clayman, R.V.; Kavoussi, L.R. Laparoscopic Radical Prostatectomy: Initial Short-Term Experience. Urology 1997, 50, 854–857. [Google Scholar] [CrossRef]
- Binder, J.; Kramer, W. Robotically-Assisted Laparoscopic Radical Prostatectomy. BJU Int. 2001, 87, 408–410. [Google Scholar] [CrossRef] [PubMed]
- Oberlin, D.T.; Flum, A.S.; Lai, J.D.; Meeks, J.J. The Effect of Minimally Invasive Prostatectomy on Practice Patterns of American Urologists. Urol. Oncol. 2016, 34, e1–e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levinson, A.W.; Ward, N.T.; Sulman, A.; Mettee, L.Z.; Link, R.E.; Su, L.M.; Pavlovich, C.P. The Impact of Prostate Size on Perioperative Outcomes in a Large Laparoscopic Radical Prostatectomy Series. J. Endourol. 2009, 23, 147–152. [Google Scholar] [CrossRef]
- Boczko, J.; Erturk, E.; Golijanin, D.; Madeb, R.; Patel, H.; Joseph, J.V. Impact of Prostate Size in Robot-Assisted Radical Prostatectomy. J. Endourol. 2007, 21, 184–188. [Google Scholar] [CrossRef]
- Chang, C.M.; Moon, D.; Gianduzzo, T.R.; Eden, C.G. The Impact of Prostate Size in Laparoscopic Radical Prostatectomy. Eur. Urol. 2005, 48, 285–290. [Google Scholar] [CrossRef]
- Galfano, A.; Panarello, D.; Secco, S.; Di Trapani, D.; Barbieri, M.; Napoli, G.; Strada, E.; Petralia, G.; Bocciardi, A.M. Does Prostate Volume Have an Impact on the Functional and Oncological Results of Retzius-Sparing Robot-Assisted Radical Prostatectomy? Minerva Urol. E Nefrol.—Ital. J. Urol. Nephrol. 2018, 70, 408–413. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 148–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the Sample Mean and Standard Deviation from the Sample Size, Median, Range and/or Interquartile Range. BMC Med Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Asimakopoulos, A.D.; Topazio, L.; De Angelis, M.; Agrò, E.F.; Pastore, A.L.; Fuschi, A.; Annino, F. Retzius-Sparing versus Standard Robot-Assisted Radical Prostatectomy: A Prospective Randomized Comparison on Immediate Continence Rates. Surg. Endosc. 2019, 33, 2187–2196. [Google Scholar] [CrossRef] [PubMed]
- Dubbelman, Y.; Groen, J.; Wildhagen, M.; Rikken, B.; Bosch, R. The Recovery of Urinary Continence after Radical Retropubic Prostatectomy: A Randomized Trial Comparing the Effect of Physiotherapist-Guided Pelvic Floor Muscle Exercises with Guidance by an Instruction Folder Only. BJU Int. 2010, 106, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Martínez, C.H.; Chalasani, V.; Lim, D.; Nott, L.; Al-Bareeq, R.J.; Wignall, G.R.; Stitt, L.; Pautler, S.E. Effect of Prostate Gland Size on the Learning Curve for Robot-Assisted Laparoscopic Radical Prostatectomy: Does Size Matter Initially? J. Endourol. 2010, 24, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Regis, L.; Salazar, A.; Planas, J.; Celma, A.; Cuadras, M.; Roche, S.; Mast, R.; Morote, J.; Trilla, E. The Position of Urethrovesical Anastomosis after Robotic Radical Prostatectomy Assessed by MRI Predicts Early Functional Recovery: A Cohort Analyses from a Randomized Clinical Trial. Eur. J. Radiol. 2021, 137, 109589. [Google Scholar] [CrossRef] [PubMed]
- Si-Tu, J.; Lu, M.H.; Li, L.Y.; Sun, Q.P.; Zhou, X.F.; Qiu, J.G.; Gao, X. Prospective Evaluation of Pentafecta Outcomes at 5 Years after Laparoscopic Radical Prostatectomy: Results of 170 Patients at a Single Center. Neoplasma 2013, 60, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Min, S.H.; Park, Y.H.; Lee, S.B.; Ku, J.H.; Kwak, C.; Kim, H.H. Impact of Prostate Size on Pathologic Outcomes and Prognosis after Radical Prostatectomy. Korean J. Urol. 2012, 53, 463–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasui, T.; Tozawa, K.; Kurokawa, S.; Okada, A.; Mizuno, K.; Umemoto, Y.; Kawai, N.; Sasaki, S.; Hayashi, Y.; Kojima, Y.; et al. Impact of Prostate Weight on Perioperative Outcomes of Robot-Assisted Laparoscopic Prostatectomy with a Posterior Approach to the Seminal Vesicle. BMC Urol. 2014, 14, 6. [Google Scholar] [CrossRef] [Green Version]
- Westhofen, T.; Buchner, A.; Schlenker, B.; Becker, A.; Chaloupka, M.; Bischoff, R.; Stief, C.G.; Kretschmer, A. Matter of Size? Health-Related Quality of Life after Radical Prostatectomy for Patients with Giant Prostates. Prostate 2021, 81, 443–451. [Google Scholar] [CrossRef]
- Finley, D.S.; Osann, K.; Chang, A.; Santos, R.; Skarecky, D.; Ahlering, T.E. Hypothermic Robotic Radical Prostatectomy: Impact on Continence. J. Endourol. 2009, 23, 1443–1450. [Google Scholar] [CrossRef] [PubMed]
- Pettus, J.A.; Masterson, T.; Sokol, A.; Cronin, A.M.; Savage, C.; Sandhu, J.S.; Mulhall, J.P.; Scardino, P.T.; Rabbani, F. Prostate Size Is Associated with Surgical Difficulty but Not Functional Outcome at 1 Year after Radical Prostatectomy. J. Urol. 2009, 182, 949–955. [Google Scholar] [CrossRef]
- Link, B.A.; Nelson, R.; Josephson, D.Y.; Yoshida, J.S.; Crocitto, L.E.; Kawachi, M.H.; Wilson, T.G. The Impact of Prostate Gland Weight in Robot Assisted Laparoscopic Radical Prostatectomy. J. Urol. 2008, 180, 928–932. [Google Scholar] [CrossRef] [PubMed]
- Tan, G.; Srivastava, A.; Grover, S.; Peters, D.; Dorsey, P., Jr.; Scott, A.; Jhaveri, J.; Tilki, D.; Te, A.; Tewari, A. Optimizing Vesicourethral Anastomosis Healing after Robot-Assisted Laparoscopic Radical Prostatectomy: Lessons Learned from Three Techniques in 1900 Patients. J. Endourol. 2010, 24, 1975–1983. [Google Scholar] [CrossRef]
- Hirasawa, Y.; Ohno, Y.; Nakashima, J.; Shimodaira, K.; Hashimoto, T.; Gondo, T.; Ohori, M.; Tachibana, M.; Yoshioka, K. Impact of a Preoperatively Estimated Prostate Volume Using Transrectal Ultrasonography on Surgical and Oncological Outcomes in a Single Surgeon’s Experience with Robot-Assisted Radical Prostatectomy. Surg. Endosc. 2016, 30, 3702–3708. [Google Scholar] [CrossRef]
- Jiang, D.G.; Xiao, C.T.; Mao, Y.H.; Qiu, J.G.; Si-Tu, J.; Lu, M.H.; Gao, X. Impact and Predictive Value of Prostate Weight on the Outcomes of Nerve Sparing Laparoscopic Radical Prostatectomy in Patients with Low Risk Prostate Cancer. Urol. J. 2019, 16, 260–266. [Google Scholar] [CrossRef]
- Freedland, S.J.; Isaacs, W.B.; Platz, E.A.; Terris, M.K.; Aronson, W.J.; Amling, C.L.; Presti, J.C.; Kane, C.J. Prostate size and risk of high-grade, advanced prostate cancer and biochemical progression after radical prostatectomy: A search database study. JCO 2005, 23, 7546–7554. [Google Scholar] [CrossRef]
- Neal, D.E.; Metcalfe, C.; Donovan, J.L.; Lane, J.A.; Davis, M.; Young, G.J.; Dutton, S.J.; Walsh, E.I.; Martin, R.M.; Peters, T.J.; et al. Ten-Year Mortality, Disease Progression, and Treatment-Related Side Effects in Men with Localised Prostate Cancer from the ProtecT Randomised Controlled Trial According to Treatment Received. Eur. Urol. 2020, 77, 320–330. [Google Scholar] [CrossRef] [PubMed]
- Moris, L.; Gandaglia, G.; Vilaseca, A.; Van den Broeck, T.; Briers, E.; De Santis, M.; Gillessen, S.; Grivas, N.; O’Hanlon, S.; Henry, A.; et al. Evaluation of Oncological Outcomes and Data Quality in Studies Assessing Nerve-Sparing Versus Non-Nerve-Sparing Radical Prostatectomy in Nonmetastatic Prostate Cancer: A Systematic Review. Eur. Urol. Focus 2021, in press. [Google Scholar] [CrossRef]
- Mottet, N.; van den Bergh, R.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef] [PubMed]
- Wu, E.H.; De Cicco, F.L. Anatomy, Abdomen and Pelvis, Male Genitourinary Tract. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Lee, J.S.; Chung, B.H. Transrectal ultrasound versus magnetic resonance imaging in the estimation of prostate volume as compared with radical prostatectomy specimens. Urol. Int. 2007, 78, 323–327. [Google Scholar] [CrossRef]
- Nunez-Nateras, R.; Andrews, J.R.; Martin, G.L.; Andrews, P.E.; Humphreys, M.R.; Ferrigni, R.G.; Eversman, W.G.; Castle, E.P. Accuracy of ultrasound in estimation of prostate weight: Comparison of urologists and radiologists. CJU 2010, 17, 4985–4988. [Google Scholar]
- He, M.; Muro, S.; Akita, K. Positional Relationship between the Lateral Border of Denonvilliers’ Fascia and Pelvic Plexus. Anat. Sci. Int. 2021. [Google Scholar] [CrossRef] [PubMed]
- Grivas, N.; Zachos, I.; Georgiadis, G.; Karavitakis, M.; Tzortzis, V.; Mamoulakis, C. Learning Curves in Laparoscopic and Robot-Assisted Prostate Surgery: A Systematic Search and Review. World J. Urol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Roldán Gallardo, F.F.; Quintar, A.A. The Pathological Growth of the Prostate Gland in Atherogenic Contexts. Exp. Gerontol. 2021, 148, 111304. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Type | Country | Technique | Size Measurement | Time Frame | Number of Patients |
|---|---|---|---|---|---|---|
| Chang 2005 [10] | Retrospective | UK | LRP | HPE | 2000–2004 | 400 |
| Freedland 2005 [28] | Retrospective | USA | Open | HPE | 1988–2003 | 1602 |
| Judd 2007 [9] | Retrospective | USA, UK | RARP | HPE | 2004–2005 | 355 |
| Adam 2008 [8] | Retrospective | USA | LRP | HPE | 2001–2007 | 720 |
| link 2008 [24] | Retrospective | USA | RARP | HPE | 2003–2007 | 1847 |
| Dubbelman 2009 [15] | RCT | Netherlands | Open | NA | NA | 70 |
| Finely 2009 [22] | Retrospective | USA | RARP | NA | NA | 115 |
| Joseph 2009 [23] | Retrospective | USA | Open+LRP | MRI | 1998–2007 | 3067 |
| Marteniz 2009 [16] | Retrospective | Canada | RARP | HPE | 2005–2008 | 150 |
| Tan 2009 [25] | Retrospective | USA | RARP | NA | 2005–2009 | 1900 |
| Sun 2012 [19] | Retrospective | Korea | Open | HPE | 1993–2009 | 830 |
| Si 2013 [18] | Retrospective | China | LRP | NA | NA | 170 |
| Takahiro 2014 [20] | Retrospective | Japan | RARP | HPE | 2011–2013 | 219 |
| Yosuke 2016 [26] | Retrospective | Japan | RARP | Ultrasound | 2006–2013 | 436 |
| Anastasios 2018 [14] | RCT | Italy | RARP | NA | 2011–2014 | 79 |
| Galfano 2018 [11] | Retrospective | Italy | RARP | HPE | 2010–2015 | 750 |
| Dong 2019 [27] | Retrospective | China | LRP | HPE | 2002–2014 | 165 |
| Regis 2021 [17] | RCT | Spain | RARP | MRI | NA | 40 |
| Thilo 2021 [21] | Retrospective | Germany | Open+RARP | HPE | 2013–2018 | 929 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fahmy, O.; Alhakamy, N.A.; Ahmed, O.A.A.; Khairul-Asri, M.G. Impact of Prostate Size on the Outcomes of Radical Prostatectomy: A Systematic Review and Meta-Analysis. Cancers 2021, 13, 6130. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13236130
Fahmy O, Alhakamy NA, Ahmed OAA, Khairul-Asri MG. Impact of Prostate Size on the Outcomes of Radical Prostatectomy: A Systematic Review and Meta-Analysis. Cancers. 2021; 13(23):6130. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13236130
Chicago/Turabian StyleFahmy, Omar, Nabil A. Alhakamy, Osama A. A. Ahmed, and Mohd Ghani Khairul-Asri. 2021. "Impact of Prostate Size on the Outcomes of Radical Prostatectomy: A Systematic Review and Meta-Analysis" Cancers 13, no. 23: 6130. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13236130