
The Value of Real-World Data in Understanding Prostate Cancer Risk and Improving Clinical Care: Examples from Swedish Registries


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. What Is Real World Data (RWD) and What Contribution Does It Make?
3. Real-World Prostate Cancer Data from Sweden
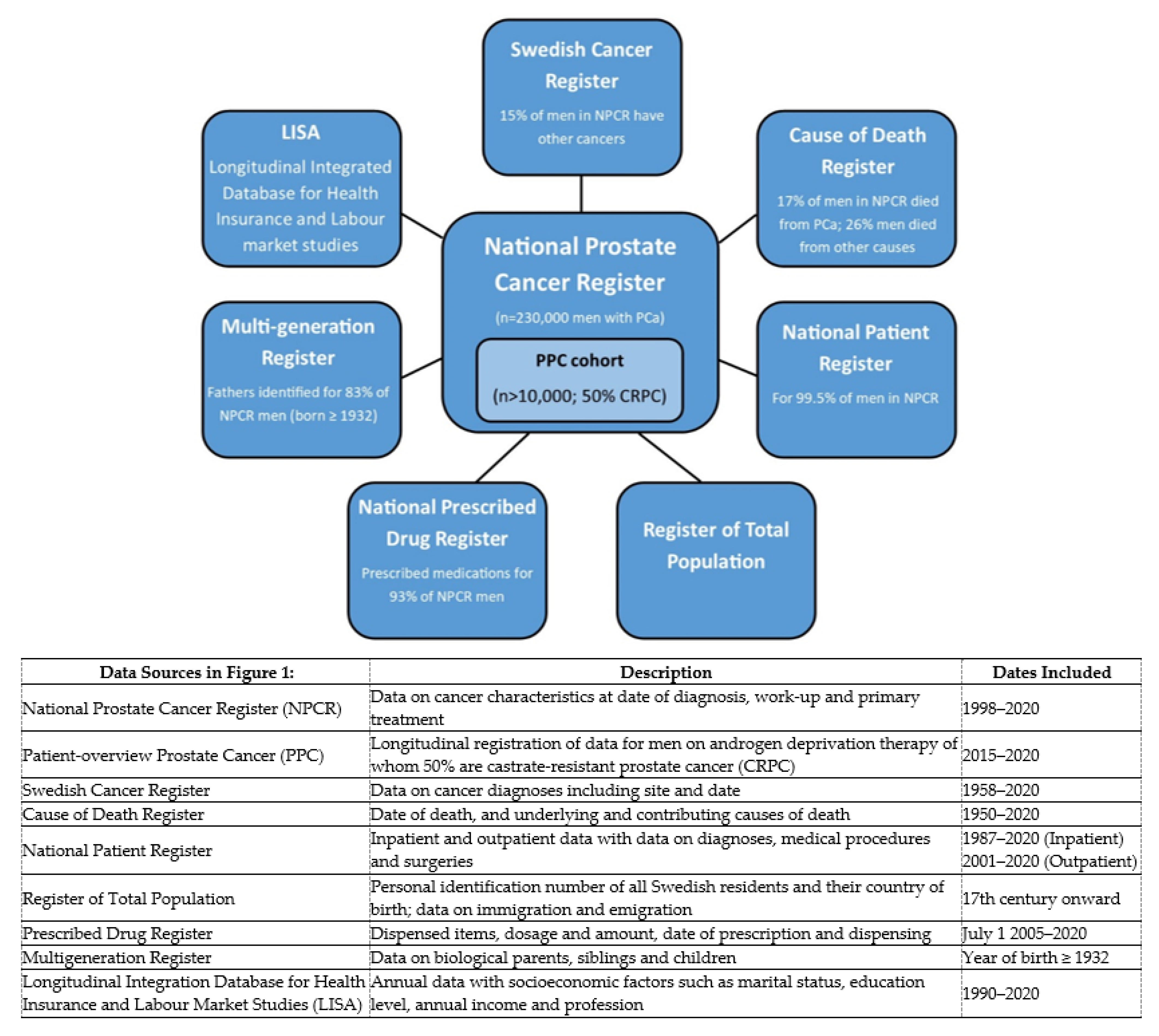
3.1. National Prostate Cancer Register (NPCR) of Sweden
3.2. Prostate Cancer Data Base Sweden (PCBaSe)
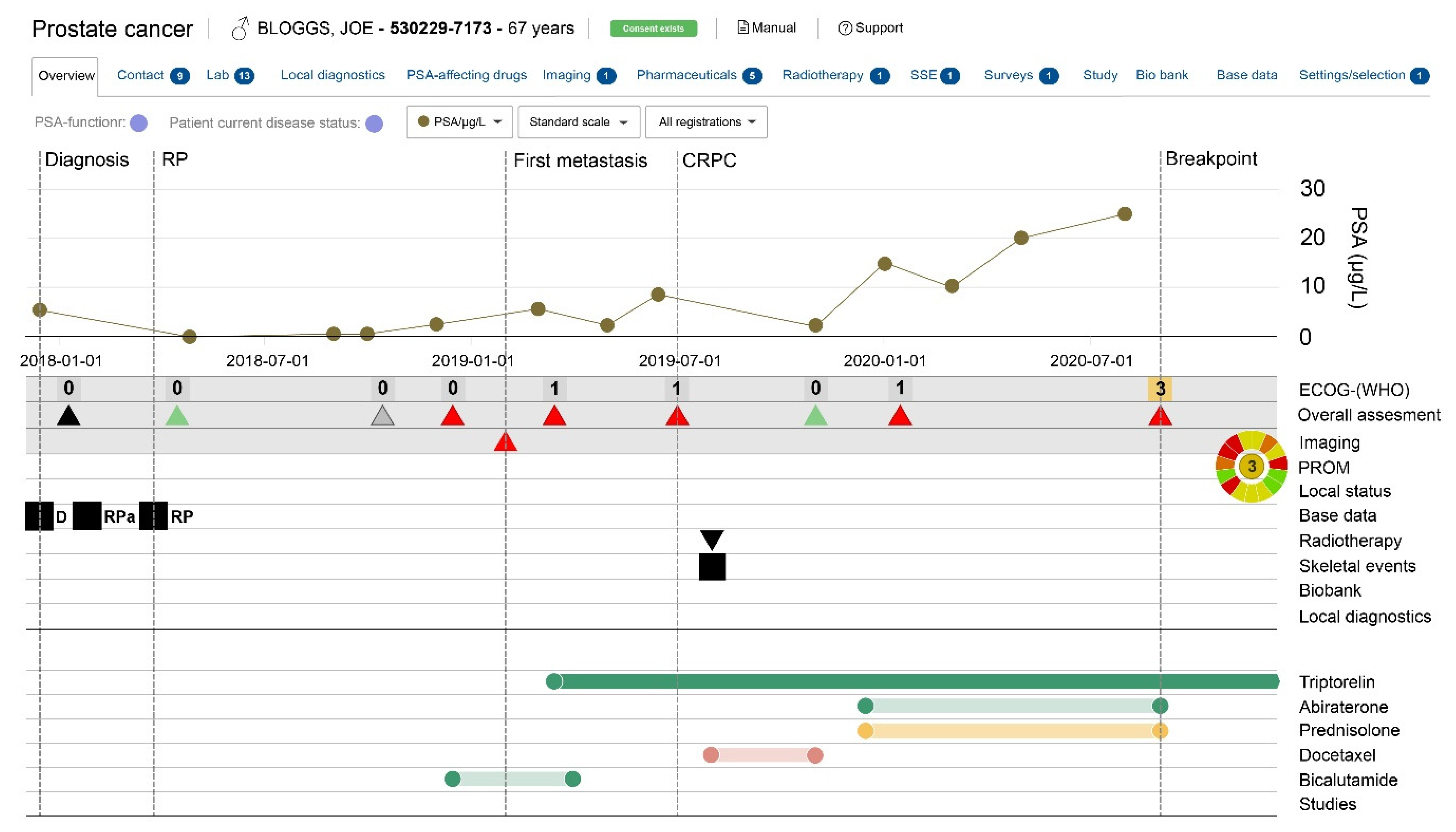
3.3. Patient-Overview Prostate Cancer (PPC)
4. The Value of RWD in Understanding PCa—Examples from Swedish Registers
4.1. Prostate Cancer Aetiology
4.2. Outcomes/Comparative Effectiveness
4.3. Adverse Events/Post-Approval Surveillance
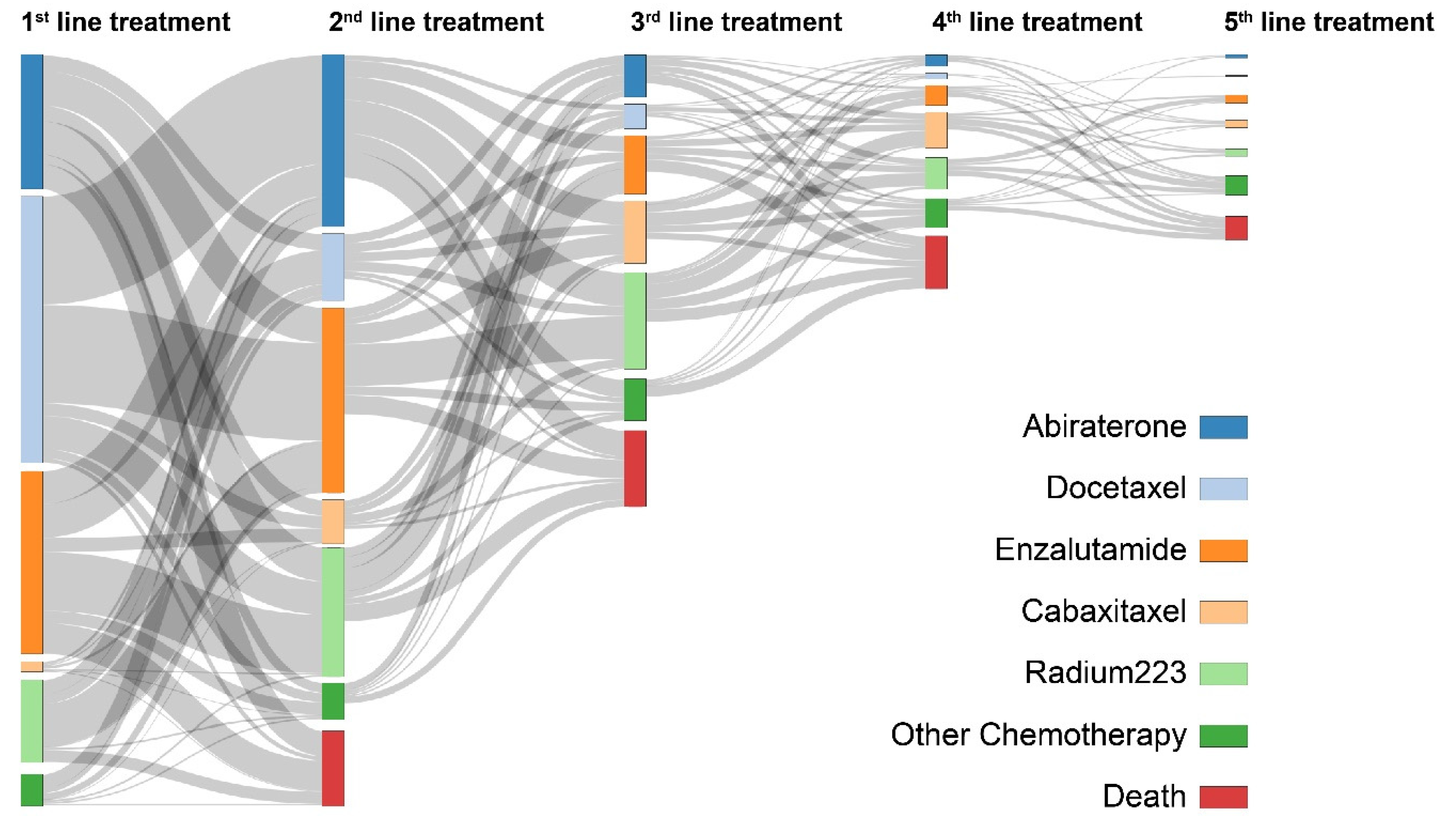
4.4. Treatment Patterns/Disparities in Access to Care
4.5. Health Economics
4.6. Guideline Compliance/Quality Indicators/Impact on Policy and Practice
5. Strengths and Limitations
6. Impact on Knowledge and Practice
7. Future Directions
8. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Burns, P.B.; Rohrich, R.J.; Chung, K.C. The Levels of Evidence and Their Role in Evidence-Based Medicine. Plast. Reconstr. Surg. 2011, 128, 305–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sibbald, B.; Roland, M. Understanding controlled trials: Why are randomised controlled trials important? BMJ 1998, 316, 201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blonde, L.; Khunti, K.; Harris, S.B.; Meizinger, C.; Skolnik, N.S. Interpretation and Impact of Real-World Clinical Data for the Practicing Clinician. Adv. Ther. 2018, 35, 1763–1774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Association of the British Pharmaceutical Industry. The Vision for Real World Data—Harnessing the Opportunities in the UK. Demonstrating Value with Real World Data. Available online: http://www.abpi.org.uk/media/1378/vision-for-real-world-data.pdf (accessed on 9 November 2020).
- Averitt, A.J.; Weng, C.; Ryan, P.; Perotte, A. Translating evidence into practice: Eligibility criteria fail to eliminate clinically significant differences between real-world and study populations. NPJ Digit. Med. 2020, 3, 1–10. [Google Scholar] [CrossRef]
- Briel, M.; Olu, K.K.; Von Elm, E.; Kasenda, B.; Alturki, R.; Agarwal, A.; Bhatnagar, N.; Schandelmaier, S. A systematic review of discontinued trials suggested that most reasons for recruitment failure were preventable. J. Clin. Epidemiology 2016, 80, 8–15. [Google Scholar] [CrossRef] [Green Version]
- Kasenda, B.; Von Elm, E.; You, J.; Blümle, A.; Tomonaga, Y.; Saccilotto, R.; Amstutz, A.; Bengough, T.; Meerpohl, J.J.; Stegert, M.; et al. Prevalence, Characteristics, and Publication of Discontinued Randomized Trials. JAMA 2014, 311, 1045–1052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaywitz, D.A. A Drug Is not an Outcome: Extending Translation Through Implementation Using Real-World Data. Clin. Pharmacol. Ther. 2019, 106, 47–49. [Google Scholar] [CrossRef] [PubMed]
- Van Herk-Sukel, M.P.P.; Lemmens, V.E.P.P.; Van De Poll-Franse, L.V.; Herings, R.M.C.; Coebergh, J.W.W.; Herk-Sukel, M.P.P.; Poll-Franse, L.V. Record linkage for pharmacoepidemiological studies in cancer patients. Pharmacoepidemiol. Drug Saf. 2011, 21, 94–103. [Google Scholar] [CrossRef]
- Penson, D.F.; Albertsen, P.C. Lessons learnt about early prostate cancer from large scale databases: Population-based pearls of wisdom. Surg. Oncol. 2002, 11, 3–11. [Google Scholar] [CrossRef]
- A Cohen, J.; Trojano, M.; Mowry, E.M.; Uitdehaag, B.M.; Reingold, S.C.; Marrie, R.A. Leveraging real-world data to investigate multiple sclerosis disease behavior, prognosis, and treatment. Mult. Scler. J. 2019, 26, 23–37. [Google Scholar] [CrossRef] [Green Version]
- Gandaglia, G.; Bray, F.; Cooperberg, M.R.; Karnes, R.J.; Leveridge, M.J.; Moretti, K.; Murphy, D.G.; Penson, D.F.; Miller, D.C. Prostate Cancer Registries: Current Status and Future Directions. Eur. Urol. 2016, 69, 998–1012. [Google Scholar] [CrossRef] [Green Version]
- Karanatsios, B.; Prang, K.-H.; Verbunt, E.; Yeung, J.M.; Kelaher, M.; Gibbs, P. Defining key design elements of registry-based randomised controlled trials: A scoping review. Trials 2020, 21, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Duggan, M.A.; Anderson, W.F.; Altekruse, S.; Penberthy, L.; Sherman, M.E. The Surveillance, Epidemiology, and End Results (SEER) Program and Pathology. Am. J. Surg. Pathol. 2016, 40, e94–e102. [Google Scholar] [CrossRef]
- Potosky, A.L.; Riley, G.F.; Lubitz, J.D.; Mentnech, R.M.; Kessler, L.G. Potential for cancer related health services research using a linked Medicare-tumor registry database. Med Care 1993, 31, 732–748. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. SEER Linked Databases. Available online: seer.cancer.gov/data-software/linked_databases.html (accessed on 19 February 2021).
- Enewold, L.; Parsons, H.; Zhao, L.; Bott, D.; Rivera, D.R.; Barrett, M.J.; A Virnig, B.; Warren, J.L. OUP accepted manuscript. J. Natl. Cancer Inst. Monogr. 2019, 2020, 3–13. [Google Scholar] [CrossRef]
- Van Hemelrijck, M.; Garmo, H.; Wigertz, A.; Nilsson, P.; Stattin, P. Cohort Profile Update: The National Prostate Cancer Register of Sweden and Prostate Cancer data Base—A refined prostate cancer trajectory. Int. J. Epidemiology 2016, 45, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Van Hemelrijck, M.; Wigertz, A.; Sandin, F.; Garmo, H.; Hellström, K.; Fransson, P.; Widmark, A.; Lambe, M.; Adolfsson, J.; Varenhorst, E.; et al. Cohort Profile: The National Prostate Cancer Register of Sweden and Prostate Cancer data Base Sweden 2.0. Int. J. Epidemiology 2012, 42, 956–967. [Google Scholar] [CrossRef] [Green Version]
- Tomic, K.; Berglund, A.; Robinson, D.; Hjälm-Eriksson, M.; Carlsson, S.; Lambe, M.; Stattin, P. Capture rate and representativity of The National Prostate Cancer Register of Sweden. Acta Oncol. 2015, 54, 158–163. [Google Scholar] [CrossRef] [Green Version]
- Tomic, K.; Sandin, F.; Wigertz, A.; Robinson, D.; Lambe, M.; Stattin, P. Evaluation of data quality in the National Prostate Cancer Register of Sweden. Eur. J. Cancer 2015, 51, 101–111. [Google Scholar] [CrossRef]
- Beckmann, K.; Garmo, H.; Nilsson, P.; Lissbrant, I.F.; Widmark, A.; Stattin, P. Radical radiotherapy for prostate cancer: Patterns of care in Sweden 1998–2016. Acta Oncol. 2020, 59, 549–557. [Google Scholar] [CrossRef] [Green Version]
- Cazzaniga, W.; Ventimiglia, E.; Alfano, M.; Robinson, D.; Lissbrant, I.F.; Carlsson, S.; Styrke, J.; Montorsi, F.; Salonia, A.; Stattin, P. Mini Review on the Use of Clinical Cancer Registers for Prostate Cancer: The National Prostate Cancer Register (NPCR) of Sweden. Front. Med. 2019, 6, 51. [Google Scholar] [CrossRef]
- Lissbrant, I.F.; Eriksson, M.H.; Lambe, M.; Törnblom, M.; Stattin, P. Set-up and preliminary results from the Patient-overview Prostate Cancer. Longitudinal registration of treatment of advanced prostate cancer in the National Prostate Cancer Register of Sweden. Scand. J. Urol. 2020, 54, 227–234. [Google Scholar] [CrossRef] [PubMed]
- The Eastern Cooperative Oncology Group/World Health Organization. The Eastern Cooperative Oncology Group/World Health Organization Performance Status. Available online: https://www.mdcalc.com (accessed on 11 November 2020).
- Groenvold, M.; Petersen, M.A.; Aaronson, N.K.; Arraras, J.I.; Blazeby, J.M.; Bottomley, A.; Fayers, P.M.; de Graeff, A.; Hammerlid, E.; Kaasa, S.; et al. The development of the EORTC QLQ-C15-PAL: A shortened questionnaire for cancer patients in palliative care. Eur. J. Cancer 2006, 42, 55–64. [Google Scholar] [CrossRef]
- Crawley, D.; Garmo, H.; Rudman, S.; Stattin, P.; Zethelius, B.; Holmberg, L.; Adolfsson, J.; Van Hemelrijck, M. Association between type 2 diabetes, curative treatment and survival in men with intermediate- and high-risk localized prostate cancer. BJU Int. 2017, 121, 209–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, D.; Garmo, H.; Bill-Axelson, A.; Mucci, L.; Holmberg, L.; Stattin, P. Use of 5 -reductase inhibitors for lower urinary tract symptoms and risk of prostate cancer in Swedish men: Nationwide, population based case-control study. BMJ 2013, 346, f3406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loeb, S.; Folkvaljon, Y.; Damber, J.-E.; Alukal, J.; Lambe, M.; Stattin, P. Testosterone Replacement Therapy and Risk of Favorable and Aggressive Prostate Cancer. J. Clin. Oncol. 2017, 35, 1430–1436. [Google Scholar] [CrossRef] [PubMed]
- Beckmann, K.; Russell, B.; Josephs, D.; Garmo, H.; Haggstrom, C.; Holmberg, L.; Stattin, P.; Van Hemelrijck, M.; Adolfsson, J. Chronic inflammatory diseases, anti-inflammatory medications and risk of prostate cancer: A population-based case-control study. BMC Cancer 2019, 19, 612. [Google Scholar] [CrossRef]
- Lin, E.; Garmo, H.; Van Hemelrijck, M.; Adolfsson, J.; Stattin, P.; Zethelius, B.; Crawley, D. Association of type 2 diabetes mellitus and antidiabetic medication with risk of prostate cancer: A population-based case-control study. BMC Cancer 2020, 20, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Beckmann, K.; Garmo, H.; Lindahl, B.; Holmberg, L.; Stattin, P.; Adolfsson, J.; Cruickshank, J.K.; Van Hemelrijck, M. Spironolactone use is associated with lower prostate cancer risk: A population-wide case-control study. Prostate Cancer Prostatic Dis. 2020, 23, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Loeb, S.; Drevin, L.; Robinson, D.; Holmberg, E.; Carlsson, S.; Lambe, M.; Stattin, P. Risk of localized and advanced prostate cancer among immigrants versus native-born Swedish men: A nation-wide population-based study. Cancer Causes Control. 2012, 24, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Wirén, S.; Drevin, L.; Akre, O.; Robinson, D.; Stattin, P. Fathering of Dizygotic Twins and Risk of Prostate Cancer: Nationwide, Population-Based Case-Control Study. PLoS ONE 2014, 9, e110506. [Google Scholar] [CrossRef]
- Wirén, S.M.; Drevin, L.I.; Carlsson, S.V.; Akre, O.; Holmberg, E.C.; Robinson, D.E.; Garmo, H.G.; Stattin, P.E. Fatherhood status and risk of prostate cancer: Nationwide, population-based case-control study. Int. J. Cancer 2013, 133, 937–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bratt, O.; Drevin, L.; Akre, O.; Garmo, H.; Stattin, P. Family History and Probability of Prostate Cancer, Differentiated by Risk Category: A Nationwide Population-Based Study. J. Natl. Cancer Inst. 2016, 108, djw110. [Google Scholar] [CrossRef] [Green Version]
- Jansson, F.; Drevin, L.; Frisell, T.; Stattin, P.; Bratt, O.; Akre, O. Concordance of Non–Low-Risk Disease Among Pairs of Brothers With Prostate Cancer. J. Clin. Oncol. 2018, 36, 1847–1852. [Google Scholar] [CrossRef] [PubMed]
- Jansson, K.F.; Akre, O.; Garmo, H.; Bill-Axelson, A.; Adolfsson, J.; Stattin, P.; Bratt, O. Concordance of Tumor Differentiation Among Brothers with Prostate Cancer. Eur. Urol. 2012, 62, 656–661. [Google Scholar] [CrossRef] [PubMed]
- Bratt, O.; Garmo, H.; Adolfsson, J.; Bill-Axelson, A.; Holmberg, L.; Lambe, M.; Stattin, P. Effects of Prostate-Specific Antigen Testing on Familial Prostate Cancer Risk Estimates. J. Natl. Cancer Inst. 2010, 102, 1336–1343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bratt, O.; Drevin, L.; Prütz, K.-G.; Carlsson, S.; Wennberg, L.; Stattin, P. Prostate cancer in kidney transplant recipients - a nationwide register study. BJU Int. 2020, 125, 679–685. [Google Scholar] [CrossRef]
- Wilson, K.M.; Markt, S.C.; Fang, F.; Nordenvall, C.; Rider, J.R.; Ye, W.; Adami, H.-O.; Stattin, P.; Nyrén, O.; Mucci, L.A. Snus use, smoking and survival among prostate cancer patients. Int. J. Cancer 2016, 139, 2753–2759. [Google Scholar] [CrossRef] [Green Version]
- Jochems, S.H.J.; Stattin, P.; Häggström, C.; Järvholm, B.; Orho-Melander, M.; Wood, A.M.; Stocks, T. Height, body mass index and prostate cancer risk and mortality by way of detection and cancer risk category. Int. J. Cancer 2020, 147, 3328–3338. [Google Scholar] [CrossRef]
- Elliott, S.P.; Johnson, D.P.; Jarosek, S.L.; Konety, B.R.; Adejoro, O.O.; Virnig, B.A. Bias Due to Missing SEER Data in D’Amico Risk Stratification of Prostate Cancer. J. Urol. 2012, 187, 2026–2031. [Google Scholar] [CrossRef] [PubMed]
- Parker, J.; Crawley, D.; Garmo, H.; Lindahl, B.; Styrke, J.; Adolfsson, J.; Lambe, M.; Stattin, P.; Van Hemelrijck, M.; Beckmann, K. Use of Warfarin or Direct Oral Anticoagulants and Risk of Prostate Cancer in PCBaSe: A Nationwide Case-Control Study. Front. Oncol. 2020, 10, 571838. [Google Scholar] [CrossRef]
- Stattin, P.; Holmberg, E.; Johansson, J.-E.; Adolfsson, J.; Hugosson, J.; National Prostate Cancer Register (NPCR) of Sweden. Outcomes in Localized Prostate Cancer: National Prostate Cancer Register of Sweden Follow-up Study. J. Natl. Cancer Inst. 2010, 102, 950–958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akre, O.; Garmo, H.; Adolfsson, J.; Lambe, M.; Bratt, O.; Stattin, P. Mortality Among Men with Locally Advanced Prostate Cancer Managed with Noncurative Intent: A Nationwide Study in PCBaSe Sweden. Eur. Urol. 2011, 60, 554–563. [Google Scholar] [CrossRef] [PubMed]
- Fossa, S.D.; Wiklund, F.; Klepp, O.; Angelsen, A.; Solberg, A.; Damber, J.-E.; Hoyer, M.; Widmark, A. Ten- and 15-yr Prostate Cancer-specific Mortality in Patients with Nonmetastatic Locally Advanced or Aggressive Intermediate Prostate Cancer, Randomized to Lifelong Endocrine Treatment Alone or Combined with Radiotherapy: Final Results of The Scandinavian Prostate Cancer Group-7. Eur. Urol. 2016, 70, 684–691. [Google Scholar] [CrossRef] [PubMed]
- Stranne, J.; Brasso, K.; Brennhovd, B.; Johansson, E.; Jäderling, F.; Kouri, M.; Lilleby, W.; Petersen, P.M.; Mirtti, T.; Pettersson, A.; et al. SPCG-15: A prospective randomized study comparing primary radical prostatectomy and primary radiotherapy plus androgen deprivation therapy for locally advanced prostate cancer. Scand. J. Urol. 2018, 52, 313–320. [Google Scholar] [CrossRef]
- Robinson, D.; Garmo, H.; Lissbrant, I.F.; Widmark, A.; Pettersson, A.; Gunnlaugsson, A.; Adolfsson, J.; Bratt, O.; Nilsson, P.; Stattin, P. Prostate Cancer Death After Radiotherapy or Radical Prostatectomy: A Nationwide Population-based Observational Study. Eur. Urol. 2018, 73, 502–511. [Google Scholar] [CrossRef] [Green Version]
- Fridriksson, J.Ö.; Folkvaljon, Y.; Nilsson, P.; Robinson, D.; Franck-Lissbrant, I.; Ehdaie, B.; Eastham, J.A.; Widmark, A.; Karlsson, C.T.; Stattin, P. Long-term adverse effects after curative radiotherapy and radical prostatectomy: Population-based nationwide register study. Scand. J. Urol. 2016, 50, 338–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallis, C.J.; Herschorn, S.; Saskin, R.; Su, J.; Klotz, L.H.; Chang, M.; Kulkarni, G.S.; Lee, Y.; Kodama, R.T.; Narod, S.A.; et al. Complications After Radical Prostatectomy or Radiotherapy for Prostate Cancer: Results of a Population-based, Propensity Score–matched Analysis. Urol. 2015, 85, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Pettersson, A.; Alm, D.; Garmo, H.; Eriksson, M.H.; Castellanos, E.; Åström, L.; Kindblom, J.; Widmark, A.; Gunnlaugsson, A.; Lissbrant, I.F.; et al. Comparative Effectiveness of Different Radical Radiotherapy Treatment Regimens for Prostate Cancer: A Population-Based Cohort Study. JNCI Cancer Spectr. 2020, 4, pkaa006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaorsky, N.G.; Keith, S.W.; Shaikh, T.; Nguyen, P.L.; Horwitz, E.M.; Dicker, A.P.; Den, R.B. Impact of Radiation Therapy Dose Escalation on Prostate Cancer Outcomes and Toxicities. Am. J. Clin. Oncol. 2018, 41, 409–415. [Google Scholar] [CrossRef]
- Kalra, B.S.; Batta, A.; Khirasaria, R. Trends in FDA drug approvals over last 2 decades: An observational study. J. Fam. Med. Prim. Care 2020, 9, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Van Hemelrijck, M.; Garmo, H.; Holmberg, L.; Ingelsson, E.; Bratt, O.; Bill-Axelson, A.; Lambe, M.; Stattin, P.; Adolfsson, J. Absolute and Relative Risk of Cardiovascular Disease in Men With Prostate Cancer: Results From the Population-Based PCBaSe Sweden. J. Clin. Oncol. 2010, 28, 3448–3456. [Google Scholar] [CrossRef]
- O’Farrell, S.; Garmo, H.; Holmberg, L.; Adolfsson, J.; Stattin, P.; Van Hemelrijck, M. Risk and Timing of Cardiovascular Disease After Androgen-Deprivation Therapy in Men With Prostate Cancer. J. Clin. Oncol. 2015, 33, 1243–1251. [Google Scholar] [CrossRef] [Green Version]
- Efstathiou, J.A.; Bae, K.; Shipley, W.U.; Hanks, G.E.; Pilepich, M.V.; Sandler, H.M.; Smith, M.R. Cardiovascular Mortality After Androgen Deprivation Therapy for Locally Advanced Prostate Cancer: RTOG 85-31. J. Clin. Oncol. 2009, 27, 92–99. [Google Scholar] [CrossRef] [Green Version]
- Keating, N.L.; O’Malley, A.J.; Freedland, S.J.; Smith, M.R. Diabetes and Cardiovascular Disease During Androgen Deprivation Therapy: Observational Study of Veterans With Prostate Cancer. J. Natl. Cancer Inst. 2009, 102, 39–46. [Google Scholar] [CrossRef] [Green Version]
- Saigal, C.S.; Gore, J.L.; Krupski, T.L.; Hanley, J.; Schonlau, M.; Litwin, M.S.; Urologic Diseases in America Project. Androgen deprivation therapy increases cardiovascular morbidity in men with prostate cancer. Cancer 2007, 110, 1493–1500. [Google Scholar] [CrossRef]
- Tsai, H.K.; D’Amico, A.V.; Sadetsky, N.; Chen, M.-H.; Carroll, P.R. Androgen Deprivation Therapy for Localized Prostate Cancer and the Risk of Cardiovascular Mortality. J. Natl. Cancer Inst. 2007, 99, 1516–1524. [Google Scholar] [CrossRef] [PubMed]
- US Food and Drug Administration. FDA Drug Safety Communication: Update to Ongoing Safety Review of GnRH Agonists and Notification to Manufacturers of GnRH Agonists to Add New Safety Information to Labelling Regarding Increased Risk of Diabetes and Certain Cardiovas-cular Diseases; US Food and Drug Adminisration: Rockville, MD, USA, 2010. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-update-ongoing-safety-review-gnrh-agonists-and-notification (accessed on 18 February 2021).
- Crawley, D.; Garmo, H.; Rudman, S.; Stattin, P.; Häggström, C.; Zethelius, B.; Holmberg, L.; Adolfsson, J.; Van Hemelrijck, M. Association between duration and type of androgen deprivation therapy and risk of diabetes in men with prostate cancer. Int. J. Cancer 2016, 139, 2698–2704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thorstenson, A.; Bratt, O.; Akre, O.; Hellborg, H.; Holmberg, L.; Lambe, M.; Bill-Axelson, A.; Stattin, P.; Adolfsson, J. Incidence of fractures causing hospitalisation in prostate cancer patients: Results from the population-based PCBaSe Sweden. Eur. J. Cancer 2012, 48, 1672–1681. [Google Scholar] [CrossRef]
- O’Farrell, S.; Sandstrom, K.; Garmo, H.; Stattin, P.; Holmberg, L.; Adolfsson, J.; Van Hemelrijck, M. Risk of thromboembolic disease in men with prostate cancer undergoing androgen deprivation. BJU Int. 2015, 118, 391–398. [Google Scholar] [CrossRef] [Green Version]
- Van Hemelrijck, M.; Adolfsson, J.; Garmo, H.; Bill-Axelson, A.; Bratt, O.; Ingelsson, E.; Lambe, M.; Stattin, P.; Holmberg, L. Risk of thromboembolic diseases in men with prostate cancer: Results from the population-based PCBaSe Sweden. Lancet Oncol. 2010, 11, 450–458. [Google Scholar] [CrossRef] [Green Version]
- Robinson, D.; Garmo, H.; Van Hemelrijck, M.; Damber, J.-E.; Bratt, O.; Holmberg, L.; Wahlund, L.-O.; Stattin, P.; Adolfsson, J. Androgen deprivation therapy for prostate cancer and risk of dementia. BJU Int. 2019, 124, 87–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beckmann, K.; Garmo, H.; Adolfsson, J.; Bosco, C.; Johansson, E.; Robinson, D.; Holmberg, L.; Stattin, P.; Van Hemelrijck, M. Androgen Deprivation Therapies and Changes in Comorbidity: A Comparison of Gonadotropin-releasing Hormone Agonists and Antiandrogen Monotherapy as Primary Therapy in Men with High-risk Prostate Cancer. Eur. Urol. 2019, 75, 676–683. [Google Scholar] [CrossRef] [Green Version]
- Tomic, K.; Ventimiglia, E.; Robinson, D.; Häggström, C.; Lambe, M.; Stattin, P. Socioeconomic status and diagnosis, treatment, and mortality in men with prostate cancer. Nationwide population-based study. Int. J. Cancer 2018, 142, 2478–2484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orrason, A.W.; Westerberg, M.; Garmo, H.; Lissbrant, I.F.; Robinson, D.; Stattin, P. Changes in treatment and mortality in men with locally advanced prostate cancer between 2000 and 2016: A nationwide, population-based study in Sweden. BJU Int. 2020, 126, 142–151. [Google Scholar] [CrossRef]
- Lycken, M.; Garmo, H.; Adolfsson, J.; Stattin, P.; Holmberg, L.; Bill-Axelson, A. Patterns of androgen deprivation therapies among men diagnosed with localised prostate cancer: A population-based study. Eur. J. Cancer 2014, 50, 1789–1798. [Google Scholar] [CrossRef]
- Lissbrant, I.F.; Ventimiglia, E.; Robinson, D.; Törnblom, M.; Hjälm-Eriksson, M.; Lambe, M.; Folkvaljon, Y.; Stattin, P. Nationwide population-based study on the use of novel antiandrogens in men with prostate cancer in Sweden. Scand. J. Urol. 2018, 52, 143–150. [Google Scholar] [CrossRef]
- Lissbrant, I.F.; Garmo, H.; Widmark, A.; Stattin, P. Population-based study on use of chemotherapy in men with castration resistant prostate cancer. Acta Oncol. 2013, 52, 1593–1601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lycken, M.; Drevin, L.; Garmo, H.; Stattin, P.; Adolfsson, J.; Lissbrant, I.F.; Holmberg, L.; Bill-Axelson, A. The use of palliative medications before death from prostate cancer: Swedish population-based study with a comparative overview of European data. Eur. J. Cancer 2018, 88, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Fallara, G.; Franck Lissbrant, I.; Styrke, J.; Montorsi, F.; Gedeborg, R.; Sandin, F.; Stattin, P. Rapid assertainment of uptake of a new indication for abiraterone by use of three nationwide health care registries in Sweden. Acta Oncol. 2020, (in press). [Google Scholar]
- Svensson, J.; Lissbrant, I.F.; Gauffin, O.; Hjälm-Eriksson, M.; Kilany, S.; Fagerlund, K.; Stattin, P. Time spent in hormone-sensitive and castration-resistant disease states in men with advanced prostate cancer, and its health economic impact: Registry-based study in Sweden. Scand. J. Urol. 2020, 1–8. [Google Scholar] [CrossRef]
- Fallara, G.; Lissbrant, I.F.; Styrke, J.; Montorsi, F.; Garmo, H.; Stattin, P. Observational study on time on treatment with abiraterone and enzalutamide. PLoS ONE 2020, 15, e0244462. [Google Scholar] [CrossRef]
- Fridriksson, J.; Gunseus, K.; Stattin, P. Information on pros and cons of prostate-specific antigen testing to men prior to blood draw: A study from the National Prostate Cancer Register (NPCR) of Sweden. Scand. J. Urol. Nephrol. 2012, 46, 326–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loeb, S.; Folkvaljon, Y.; Makarov, D.V.; Bratt, O.; Bill-Axelson, A.; Stattin, P. Five-year nationwide follow-up study of active surveillance for prostate cancer. Eur. Urol. 2015, 67, 233–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makarov, D.V.; Loeb, S.; Ulmert, D.; Drevin, L.; Lambe, M.; Stattin, P. Prostate Cancer Imaging Trends After a Nationwide Effort to Discourage Inappropriate Prostate Cancer Imaging. J. Natl. Cancer Inst. 2013, 105, 1306–1313. [Google Scholar] [CrossRef]
- Nugin, H.; Folkvaljon, Y.; Damber, J.-E.; Adolfsson, J.; Robinson, D.; Stattin, P. Work-up and treatment of prostate cancer before and after publication of the first national guidelines on prostate cancer care in Sweden. Scand. J. Urol. 2018, 52, 277–284. [Google Scholar] [CrossRef]
- Robertson, S.; Adolfsson, J.; Stattin, P.; Sjövall, A.; Winnersjö, R.; Hanning, M.; Sandelin, K. Waiting times for cancer patients in Sweden: A nationwide population-based study. Scand. J. Public Heal. 2017, 45, 230–237. [Google Scholar] [CrossRef]
- Stattin, P.; Sandin, F.; Sandbäck, T.; Damber, J.-E.; Lissbrant, I.F.; Robinson, D.; Bratt, O.; Lambe, M. Dashboard report on performance on select quality indicators to cancer care providers. Scand. J. Urol. 2015, 50, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Bratt, O.; Folkvaljon, Y.; Loeb, S.; Klotz, L.; Egevad, L.; Stattin, P. Upper limit of cancer extent on biopsy defining very low-risk prostate cancer. BJU Int. 2015, 116, 213–219. [Google Scholar] [CrossRef] [Green Version]
- Confederation of Regional Cancer Centres. The National Clinical Prostate Cancer Care Guidelines. 2014. Available online: https://kunskapsbanken.cancercentrum.se/diagnoser/prostatacancer/vardprogram/ (accessed on 18 February 2021).
- Loeb, S.; Folkvaljon, Y.; Curnyn, C.; Robinson, D.; Bratt, O.; Stattin, P. Uptake of Active Surveillance for Very-Low-Risk Prostate Cancer in Sweden. JAMA Oncol. 2017, 3, 1393–1398. [Google Scholar] [CrossRef] [PubMed]
- Stattin, P.; Sandin, F.; Loeb, S.; Robinson, D.; Lissbrant, I.F.; Lambe, M. Public online reporting from a nationwide population-based clinical prostate cancer register. BJU Int. 2018, 122, 8–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordström, T.; Aly, M.; Clements, M.S.; Weibull, C.E.; Adolfsson, J.; Grönberg, H. Prostate-specific Antigen (PSA) Testing Is Prevalent and Increasing in Stockholm County, Sweden, Despite No Recommendations for PSA Screening: Results from a Population-based Study, 2003–2011. Eur. Urol. 2013, 63, 419–425. [Google Scholar] [CrossRef]
- Patsopoulos, N.A. A pragmatic view on pragmatic trials. Dialog-Clin. Neurosci. 2011, 13, 217–224. [Google Scholar]
- James, S. Changing the paradigm: Registry-based randomized trials. In Proceedings of European Society of Cardiology; World Congress of Cardiology: Paris, France, 2019. [Google Scholar]
- Li, G.; Sajobi, T.T.; Menon, B.K.; Korngut, L.; Lowerison, M.; James, M.; Wilton, S.B.; Williamson, T.; Gill, S.; Drogos, L.L.; et al. Registry-based randomized controlled trials- what are the advantages, challenges, and areas for future research? J. Clin. Epidemiology 2016, 80, 16–24. [Google Scholar] [CrossRef]
- James, S.; Rao, S.V.; Granger, C.B. Registry-based randomized clinical trials—A new clinical trial paradigm. Nat. Rev. Cardiol. 2015, 12, 312–316. [Google Scholar] [CrossRef]
- Jernberg, T.; Attebring, M.F.; Hambraeus, K.; Ivert, T.; James, S.; Jeppsson, A.; Lagerqvist, B.; Lindahl, B.; Stenestrand, U.; Wallentin, L. The Swedish Web-system for Enhancement and Development of Evidence-based care in Heart disease Evaluated According to Recommended Therapies (SWEDEHEART). Heart 2010, 96, 1617–1621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buccheri, S.; Sarno, G.; Fröbert, O.; Gudnason, T.; Lagerqvist, B.; Lindholm, D.; Maeng, M.; Olivecrona, G.; James, S. Assessing the Nationwide Impact of a Registry-Based Randomized Clinical Trial on Cardiovascular Practice. Circ. Cardiovasc. Interv. 2019, 12, e007381. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beckmann, K.; Garmo, H.; Franck Lissbrant, I.; Stattin, P. The Value of Real-World Data in Understanding Prostate Cancer Risk and Improving Clinical Care: Examples from Swedish Registries. Cancers 2021, 13, 875. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040875
Beckmann K, Garmo H, Franck Lissbrant I, Stattin P. The Value of Real-World Data in Understanding Prostate Cancer Risk and Improving Clinical Care: Examples from Swedish Registries. Cancers. 2021; 13(4):875. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040875
Chicago/Turabian StyleBeckmann, Kerri, Hans Garmo, Ingela Franck Lissbrant, and Pär Stattin. 2021. "The Value of Real-World Data in Understanding Prostate Cancer Risk and Improving Clinical Care: Examples from Swedish Registries" Cancers 13, no. 4: 875. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040875