
Amongst Women Stratified to Receive Endocrine Therapy on the Basis of Their Tumor Estrogen and Progesterone Receptor Levels, Those with Higher Tumor Progesterone Receptor Levels Had a Better Outcome Than Those with Lower Levels of Tumor Progesterone Receptor

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
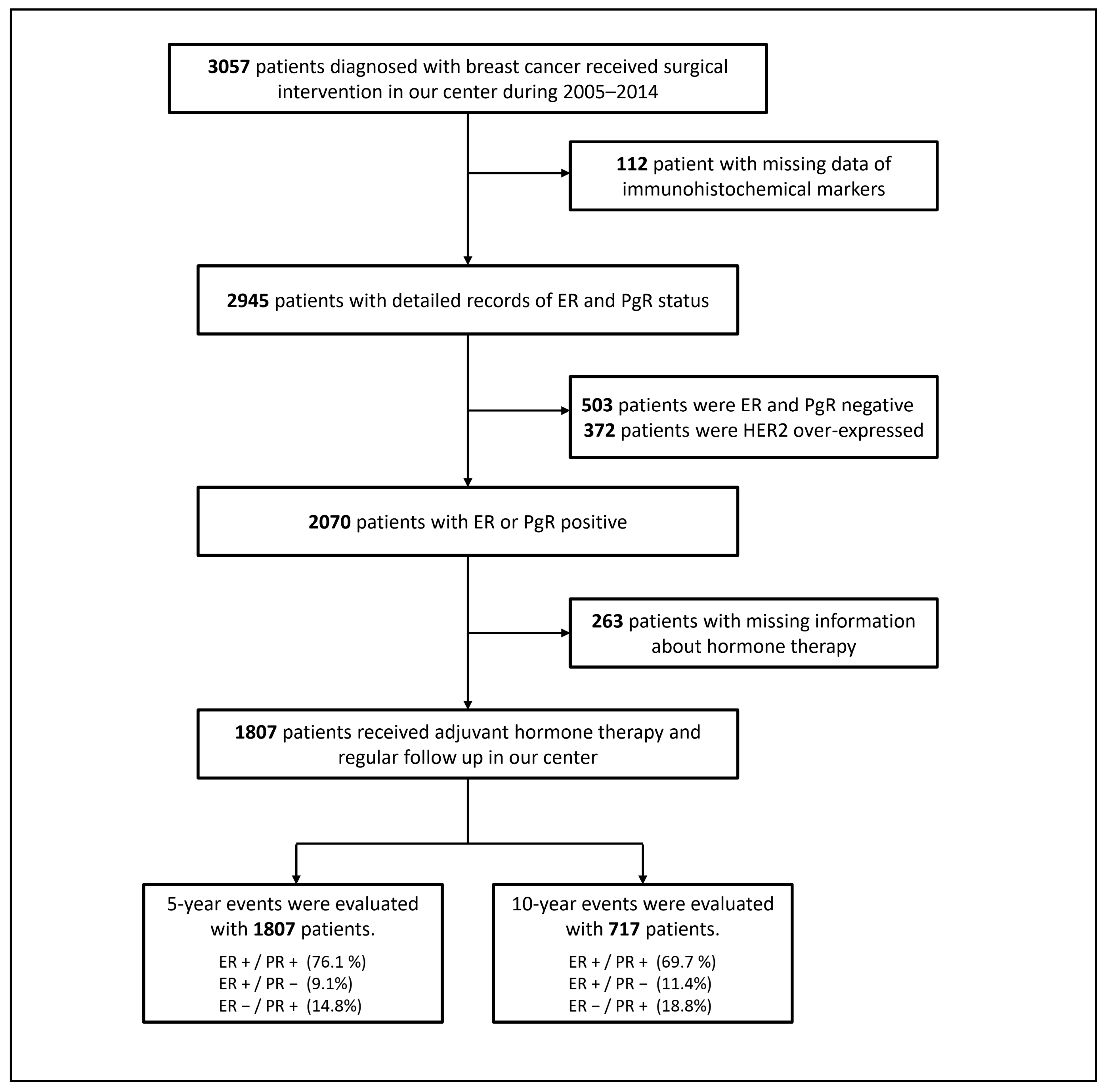
2.1. Characteristics of the Study Population
2.2. Treatment Data
2.3. Cox Regression Analyses of Variables That Affected the Clinical Endpoints after Five Years and Ten Years
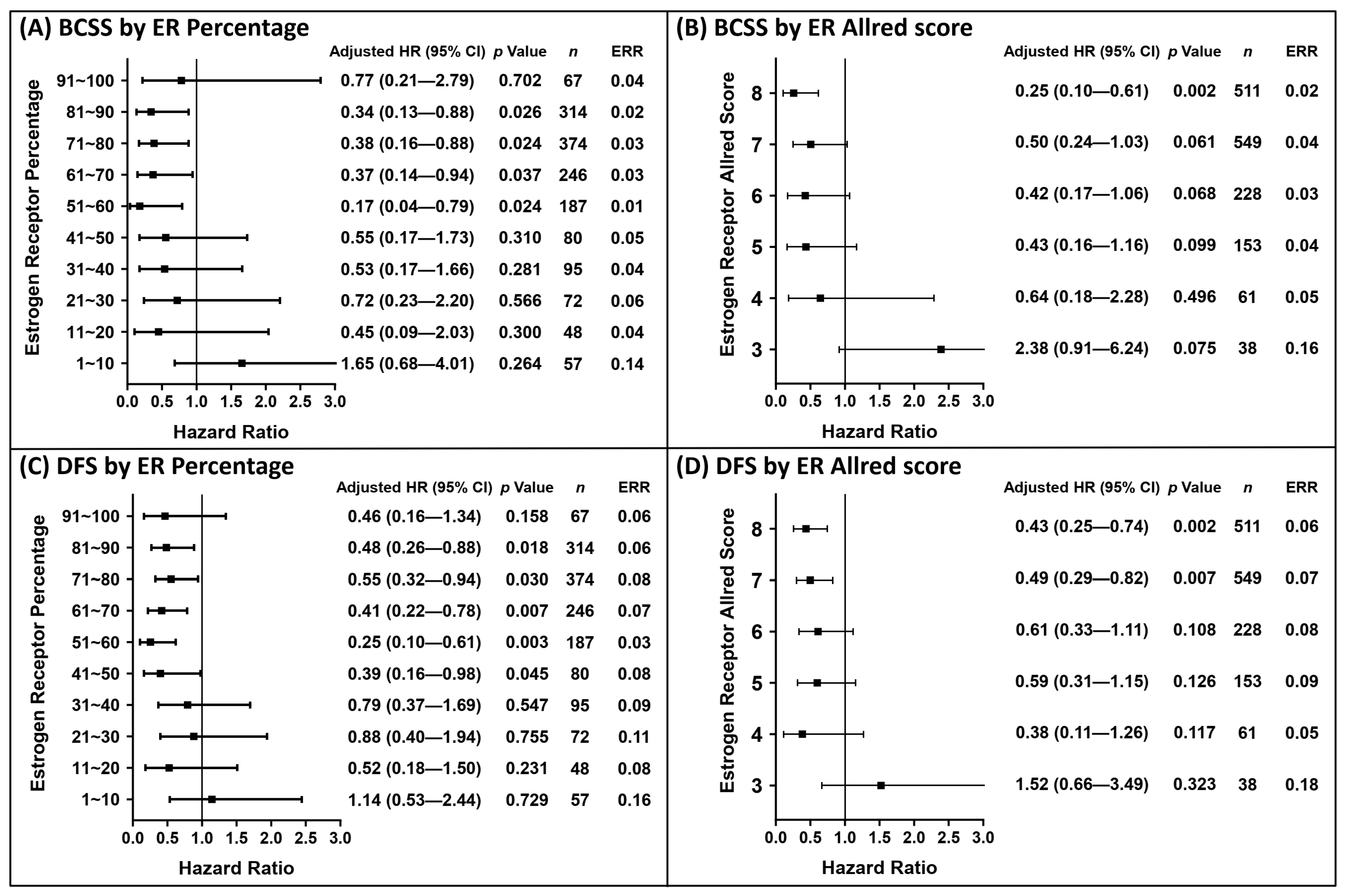
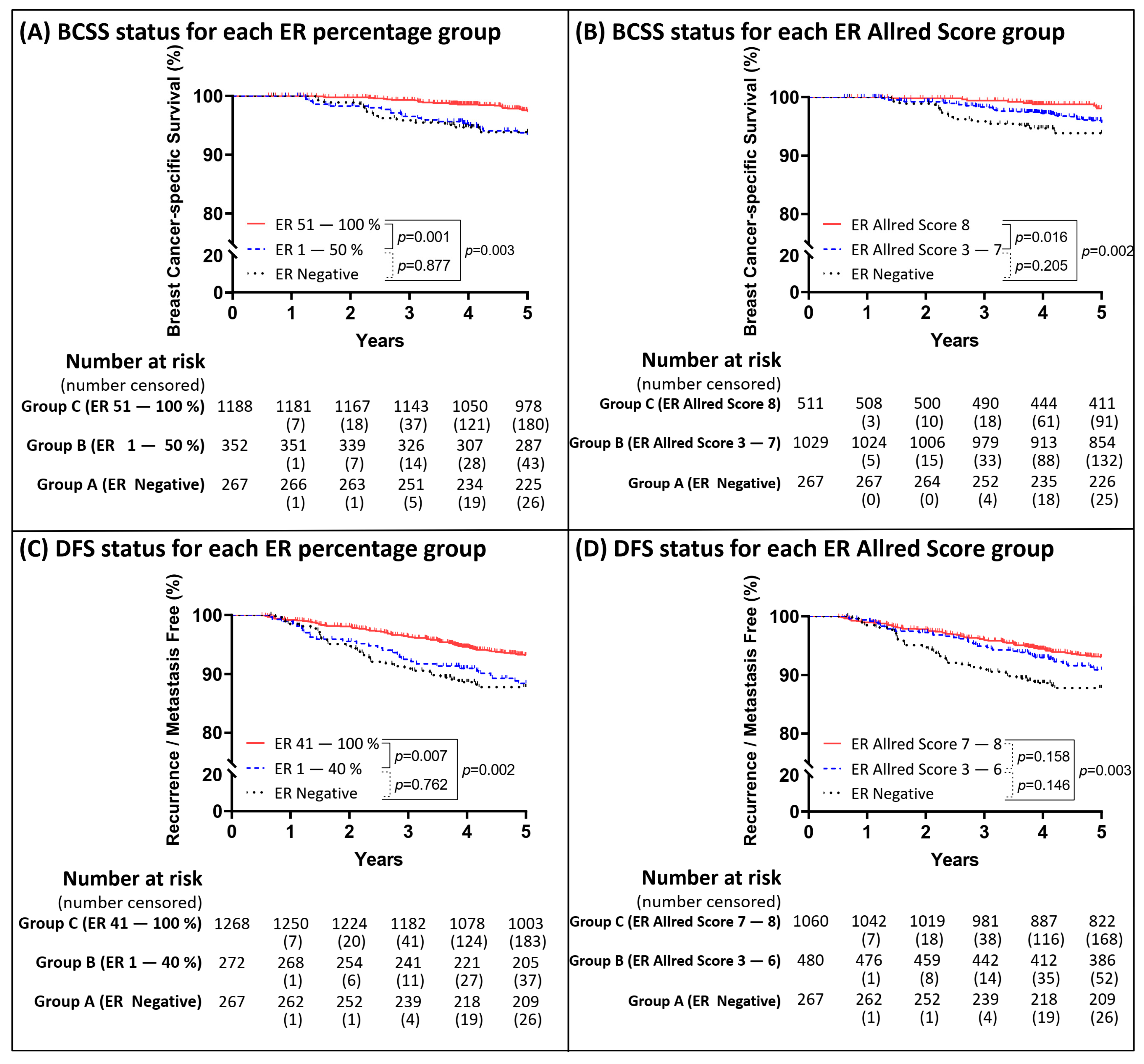
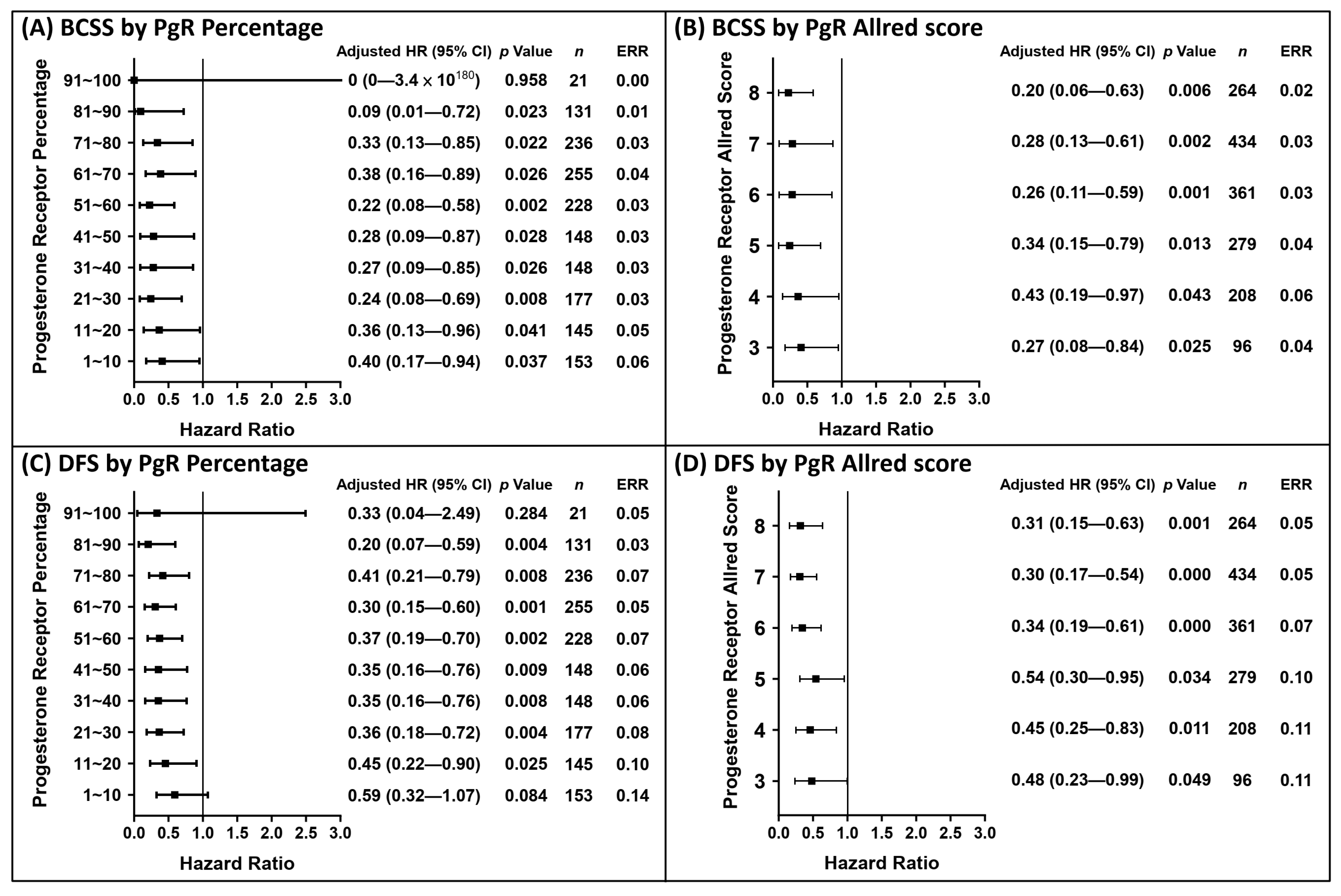
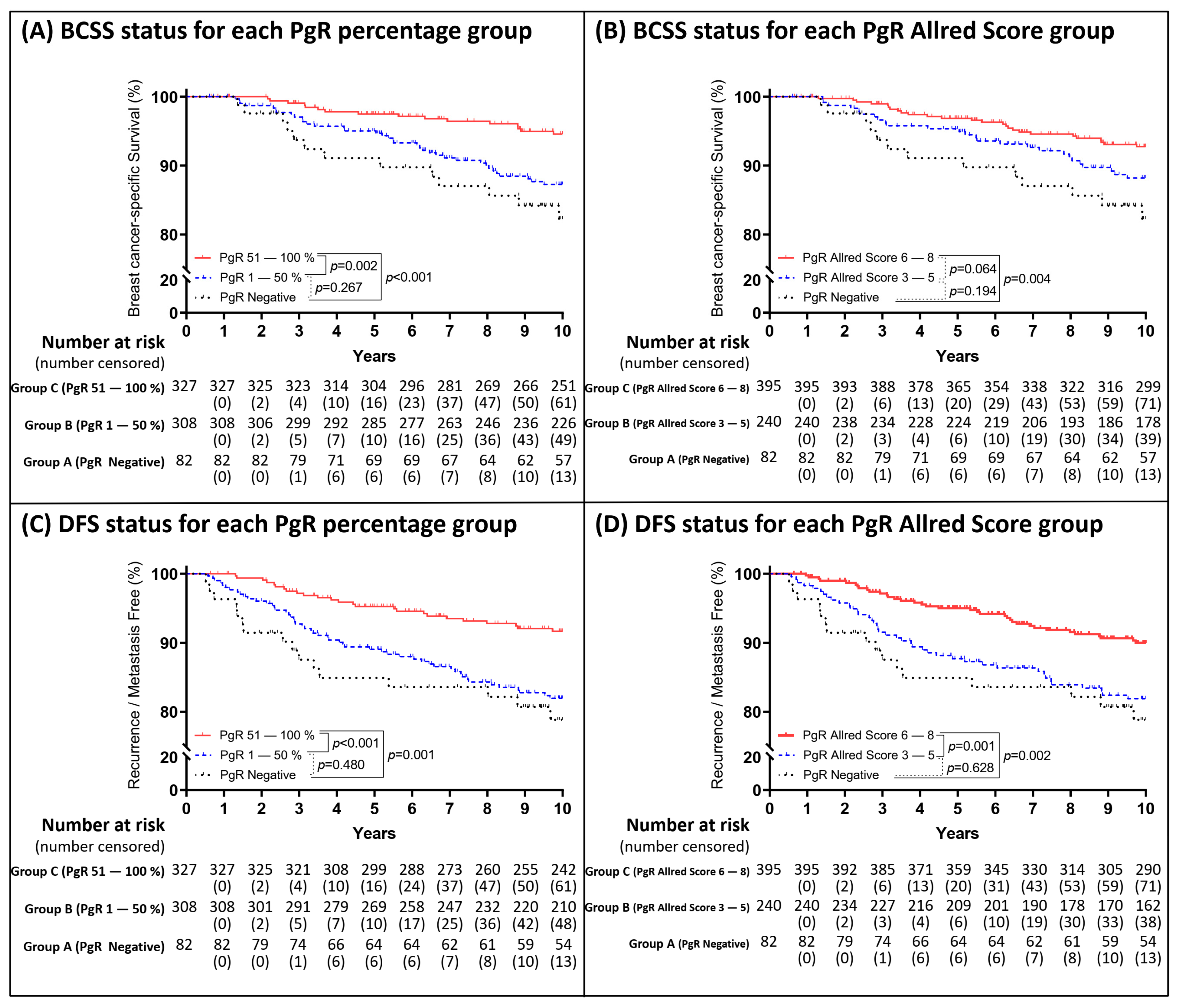
2.4. Optimizing the Cut-Off Value for the IHC Profiles of ER and PgR
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Immunohistochemical Data Collection
4.3. Clinical and Treatment Data
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Tang, P.; Tse, G.M. Immunohistochemical surrogates for molecular classification of breast carcinoma: A 2015 update. Arch. Pathol. Lab. Med. 2016, 140, 806–814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robson, M.; Im, S.-A.; Senkus, E.; Xu, B.; Domchek, S.M.; Masuda, N.; Delaloge, S.; Li, W.; Tung, N.; Armstrong, A.; et al. Olaparib for metastatic breast cancer in patients with a germline BRCA mutation. N. Engl. J. Med. 2017, 377, 523–533. [Google Scholar] [CrossRef] [PubMed]
- Litton, J.K.; Rugo, H.S.; Ettl, J.; Hurvitz, S.A.; Gonçalves, A.; Lee, K.-H.; Fehrenbacher, L.; Yerushalmi, R.; Mina, L.A.; Martin, M.; et al. Talazoparib in Patients with advanced breast cancer and a germline BRCA mutation. N. Engl. J. Med. 2018, 379, 753–763. [Google Scholar] [CrossRef] [PubMed]
- Syed, Y.Y. Sacituzumab Govitecan: First approval. Drugs 2020, 80, 1019–1025. [Google Scholar] [CrossRef]
- Allison, K.H.; Hammond, M.E.H.; Dowsett, M.; McKernin, S.E.; Carey, L.A.; Fitzgibbons, P.L.; Hayes, D.F.; Lakhani, S.R.; Chavez-MacGregor, M.; Perlmutter, J.; et al. Estrogen and progesterone receptor testing in breast cancer: ASCO/CAP guideline update. J. Clin. Oncol. 2020, 38, 1346–1366. [Google Scholar] [CrossRef]
- Dai, X.; Xiang, L.; Li, T.; Bai, Z. Cancer Hallmarks, biomarkers and breast cancer molecular subtypes. J. Cancer 2016, 7, 1281–1294. [Google Scholar] [CrossRef] [Green Version]
- Yao, N.; Song, Z.; Wang, X.; Yang, S.; Song, H. Prognostic Impact of progesterone receptor status in chinese estrogen receptor positive invasive breast cancer patients. J. Breast Cancer 2017, 20, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Dowsett, M.; Cuzick, J.; Wale, C.; Howell, T.; Houghton, J.; Baum, M. Retrospective analysis of time to recurrence in the ATAC trial according to hormone receptor status: An hypothesis-generating study. J. Clin. Oncol. 2005, 23, 7512–7517. [Google Scholar] [CrossRef]
- Layfield, L.J.; Gupta, D.; Mooney, E.E. Assessment of tissue estrogen and progesterone receptor levels: A survey of current practice, techniques, and quantitation methods. Breast J. 2000, 6, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Stendahl, M.; Rydén, L.; Nordenskjöld, B.; Jönsson, P.E.; Landberg, G.; Jirström, K. High Progesterone receptor expression correlates to the effect of adjuvant tamoxifen in premenopausal breast cancer patients. Clin. Cancer Res. 2006, 12, 4614–4618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regitnig, P.; Reiner, A.; Dinges, H.-P.; Höfler, G.; Müller-Holzner, E.; Lax, S.F.; Obrist, P.; Rudas, M.; Quehenberger, F. Quality assurance for detection of estrogen and progesterone receptors by immunohistochemistry in Austrian pathology laboratories. Virchows Archiv. 2002, 441, 328–334. [Google Scholar] [CrossRef]
- Yi, M.; Huo, L.; Koenig, K.B.; Mittendorf, E.A.; Meric-Bernstam, F.; Kuerer, H.M.; Bedrosian, I.; Buzdar, A.U.; Symmans, W.F.; Crow, J.R.; et al. Which threshold for ER positivity? A retrospective study based on 9639 patients. Ann. Oncol. 2014, 25, 1004–1011. [Google Scholar] [CrossRef] [PubMed]
- Love, R.R. Adjuvant surgical oophorectomy plus tamoxifen in premenopausal women with operable hormone receptor–positive breast cancer: A global treatment option. Clin. Breast Cancer 2016, 16, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Allred, D.C.; Bustamante, M.A.; Daniel, C.O.; Gaskill, H.V.; Cruz, A.B., Jr. Immunocytochemical analysis of estrogen receptors in human breast carcinomas. Evaluation of 130 cases and review of the literature regarding concordance with biochemical assay and clinical relevance. Arch. Surg. 1990, 125, 107–713. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.-H.; Tseng, H.-S.; Lin, C.; Chen, L.-S.; Chen, S.-T.; Kuo, S.-J.; Chen, D.-R. Survival benefit of tamoxifen in estrogen receptor-negative and progesterone receptor-positive low grade breast cancer patients. J. Breast Cancer 2012, 15, 288–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Early Breast Cancer Trialists’ Collaborative Group. Tamoxifen for early breast cancer. Cochrane Database Syst. Rev. 2001, CD000486. [Google Scholar] [CrossRef]
- Early Breast Cancer Trialists’ Collaborative Group. Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: An overview of the randomised trials. Lancet 2005, 365, 1687–1717. [Google Scholar] [CrossRef]
- Hess, K.R.; Pusztai, L.; Buzdar, A.U.; Hortobagyi, G.N. Estrogen receptors and distinct patterns of breast cancer relapse. Breast Cancer Res. Treat. 2003, 78, 105–118. [Google Scholar] [CrossRef]
- Anderson, W.F.; Chen, B.E.; Jatoi, I.; Rosenberg, P.S. Effects of estrogen receptor expression and histopathology on annual hazard rates of death from breast cancer. Breast Cancer Res. Treat. 2006, 100, 121–126. [Google Scholar] [CrossRef]
- Yu, K.-D.; Wu, J.; Shen, Z.-Z.; Shao, Z.-M. Hazard of breast cancer-specific mortality among women with estrogen receptor-positive breast cancer after five years from diagnosis: Implication for extended endocrine therapy. J. Clin. Endocrinol. Metab. 2012, 97, E2201–E2209. [Google Scholar] [CrossRef] [Green Version]
- Dignam, J.J.; Dukic, V.M.; Anderson, S.J.; Mamounas, E.P.; Wickerham, D.L.; Wolmark, N. Hazard of recurrence and adjuvant treatment effects over time in lymph node-negative breast cancer. Breast Cancer Res. Treat. 2008, 116, 595–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuqua, S.A.; Fitzgerald, S.D.; Chamness, G.C.; Tandon, A.K.; McDonnell, D.P.; Nawaz, Z.; O’Malley, B.W.; McGuire, W.L. Variant human breast tumor estrogen receptor with constitutive transcriptional activity. Cancer Res. 1991, 51, 105–109. [Google Scholar] [PubMed]
- Bardou, V.-J.; Arpino, G.; Elledge, R.M.; Osborne, C.K.; Clark, G.M. Progesterone receptor status significantly improves outcome prediction over estrogen receptor status alone for adjuvant endocrine therapy in two large breast cancer databases. J. Clin. Oncol. 2003, 21, 1973–1979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, Z.-Y.; Bay, B.-H.; Aw, S.-E.; Lin, V.C.-L. A Novel antiestrogenic mechanism in progesterone receptor-transfected breast cancer cells. J. Biol. Chem. 2005, 280, 17480–17487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Purdie, C.A.; Quinlan, P.; Jordan, L.B.; Ashfield, A.; Ogston, S.; Dewar, J.A.; Thompson, A.M. Progesterone receptor expression is an independent prognostic variable in early breast cancer: A population-based study. Br. J. Cancer 2014, 110, 565–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordenskjöld, A.; Fohlin, H.; Fornander, T.; Löfdahl, B.; Skoog, L.; Stål, O. Progesterone receptor positivity is a predictor of long-term benefit from adjuvant tamoxifen treatment of estrogen receptor positive breast cancer. Breast Cancer Res. Treat. 2016, 160, 313–322. [Google Scholar] [CrossRef] [Green Version]
- Masood, S. Breast cancer subtypes: Morphologic and biologic characterization. Women’s Health 2016, 12, 103–119. [Google Scholar] [CrossRef] [Green Version]
- Hammond, M.E.; Hayes, D.F.; Dowsett, M.; Allred, D.C.; Hagerty, K.L.; Badve, S.; Fitzgibbons, P.L.; Francis, G.; Goldstein, N.S.; Hayes, M.; et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer (unabridged version). Arch. Pathol. Lab. Med. 2010, 134, e48–e72. [Google Scholar] [CrossRef]
- Wolff, A.C.; Hammond, M.E.H.; Allison, K.H.; Harvey, B.E.; Mangu, P.B.; Bartlett, J.M.S.; Bilous, M.; Ellis, I.O.; Fitzgibbons, P.; Hanna, W.; et al. Human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice guideline focused update. J. Clin. Oncol. 2018, 36, 2105–2122. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | BCSS | DFS | ||||
|---|---|---|---|---|---|---|
| Mortality (n = 68) | Survival (n = 1739) | p | Recurrence (n = 144) | Disease-Free (n = 1663) | p | |
| Age | 0.802 | 0.599 | ||||
| <50 | 27 (39.7%) | 728 (41.9%) | 57 (39.6%) | 698 (42%) | ||
| ≥50 | 41 (60.3%) | 1011 (58.1%) | 87 (60.4%) | 965 (58%) | ||
| Operation type | <0.001 | <0.001 | ||||
| BCS | 11 (16.2%) | 674 (38.8%) | 30 (20.8%) | 655 (39.4%) | ||
| MRM | 57 (83.8%) | 1065 (61.2%) | 114 (79.2%) | 1008 (60.6%) | ||
| Tumor size (cm) | <0.001 | <0.001 | ||||
| ≤2 | 14 (20.6%) | 1172 (67.4%) | 45 (31.2%) | 1141 (68.6%) | ||
| >2, ≤5 | 39 (57.4%) | 513 (29.5%) | 77 (53.5%) | 475 (28.6%) | ||
| >5 | 15 (22.1%) | 54 (3.1%) | 22 (15.3%) | 47 (2.8%) | ||
| Lymph node | <0.001 | <0.001 | ||||
| Negative | 21 (30.9%) | 1272 (73.1%) | 62 (43.1%) | 1231 (74%) | ||
| Positive | 47 (69.1%) | 467 (26.9%) | 82 (56.9%) | 432 (26%) | ||
| Histological subtype | 0.337 | 0.058 | ||||
| Ductal | 52 (76.5%) | 1432 (82.3%) | 114 (79.2%) | 1370 (82.4%) | ||
| Lobular | 5 (7.4%) | 109 (6.3%) | 10 (6.9%) | 104 (6.3%) | ||
| Mixed (ductal and lobular) | 9 (13.2%) | 130 (7.5%) | 18 (12.5%) | 121 (7.3%) | ||
| Others | 2 (2.9%) | 68 (3.9%) | 2 (1.4%) | 68 (4.1%) | ||
| Histologic grade | 0.002 | 0.001 | ||||
| 1 | 3 (4.4%) | 270 (15.6%) | 8 (5.6%) | 265 (16%) | ||
| 2 | 18 (26.5%) | 622 (35.9%) | 47 (32.6%) | 593 (35.8%) | ||
| 3 | 47 (69.1%) | 842 (48.6%) | 89 (61.8%) | 800 (48.3%) | ||
| Unknown (n = 5) | - | - | ||||
| ER | 0.052 | 0.014 | ||||
| Negative | 16 (23.5%) | 251 (14.4%) | 32 (22.2%) | 235 (14.1%) | ||
| ≥1% | 52 (76.5%) | 1488 (85.6%) | 112 (77.8%) | 1428 (85.9%) | ||
| ER intensity | 0.029 | 0.029 | ||||
| 0 | 16 (23.5%) | 251 (14.4%) | 32 (22.2%) | 235 (14.1%) | ||
| 1 | 11 (16.2%) | 195 (11.2%) | 18 (12.5%) | 188 (11.3%) | ||
| 2 | 27 (39.7%) | 683 (39.3%) | 56 (38.9%) | 654 (39.3%) | ||
| 3 | 14 (20.6%) | 610 (35.1%) | 38 (26.4%) | 586 (35.2%) | ||
| PgR | 0.001 | 0.002 | ||||
| Negative | 15 (22.1%) | 150 (8.6%) | 24 (16.7%) | 141 (8.5%) | ||
| ≥1% | 53 (77.9%) | 1589 (91.4%) | 120 (83.3%) | 1522 (91.5%) | ||
| PgR intensity | <0.001 | 0.001 | ||||
| 0 | 15 (22.1%) | 150 (8.6%) | 24 (16.7%) | 141 (8.5%) | ||
| 1 | 21 (30.9%) | 454 (26.1%) | 45 (31.2%) | 430 (25.9%) | ||
| 2 | 24 (35.3%) | 700 (40.3%) | 52 (36.1%) | 672 (40.4%) | ||
| 3 | 8 (11.8%) | 435 (25%) | 23 (16%) | 420 (25.3%) | ||
| Hormone therapy | <0.001 | <0.001 | ||||
| Anti-estrogens | 28 (41.2%) | 1118 (64.3%) | 47 (32.6%) | 1099 (66.1%) | ||
| Enzyme-inhibitors | 16 (23.5%) | 179 (10.3%) | 28 (19.4%) | 167 (10%) | ||
| Both | 24 (35.3%) | 442 (25.4%) | 69 (47.9%) | 397 (23.9%) | ||
| Chemotherapy | <0.001 | <0.001 | ||||
| No | 12 (17.6%) | 780 (44.9%) | 33 (22.9%) | 759 (45.6%) | ||
| Yes | 56 (82.4%) | 959 (55.1%) | 111 (77.1%) | 904 (54.4%) | ||
| Radiotherapy | 0.062 | 0.488 | ||||
| No | 27 (39.7%) | 903 (51.9%) | 70 (48.6%) | 860 (51.7%) | ||
| Yes | 41 (60.3%) | 836 (48.1%) | 74 (51.4%) | 803 (48.3%) | ||
| Characteristic | BCSS | DFS | |||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Univariate | Multivariate | Univariate | Multivariate | |||||
| 1807 | HR (95% CI) a | p | HR (95% CI) a | p | HR (95% CI) a | p | HR (95% CI) a | p | |
| Age | |||||||||
| <50 | 755 | 1 (ref) | - | 1 (ref) | - | ||||
| ≥50 | 1052 | 1.12 (0.689–1.821) | 0.647 | 1.125 (0.806–1.571) | 0.489 | ||||
| Operation type | |||||||||
| BCS | 685 | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - |
| MRM | 1122 | 3.261 (1.71–6.218) | <0.001 | 1.849 (0.951–3.595) | 0.07 | 2.413 (1.614–3.608) | <0.001 | 1.596 (1.054–2.418) | 0.027 |
| Tumor size (cm) | <0.001 | <0.001 | <0.001 | <0.001 | |||||
| ≤2 | 1186 | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - |
| >2, ≤5 | 552 | 6.104 (3.314–11.241) | <0.001 | 3.688 (1.871–7.267) | <0.001 | 3.817 (2.642–5.514) | <0.001 | 2.569 (1.682–3.922) | <0.001 |
| >5 | 69 | 19.335 (9.333–40.056) | <0.001 | 9.204 (4.05–20.919) | <0.001 | 9.552 (5.736–15.907) | <0.001 | 5.408 (3.028–9.661) | <0.001 |
| Lymph node | |||||||||
| Negative | 1293 | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - |
| Positive | 514 | 5.704 (3.41–9.541) | <0.001 | 2.814 (1.535–5.161) | <0.001 | 3.455 (2.484–4.805) | <0.001 | 1.617 (1.089–2.403) | 0.017 |
| Histological subtype | 0.177 | 0.709 | 0.031 | 0.347 | |||||
| Ductal | 1484 | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - | ||
| Lobular | 114 | 1.251 (0.500–3.133) | 0.632 | 1.132 (0.593–2.16) | 0.708 | 0.934 (0.472–1.849) | 0.845 | ||
| Mixed (ductal and lobular) | 139 | 1.877 (0.925–3.809) | 0.081 | 1.703 (1.036–2.8) | 0.036 | 1.336 (0.802–2.226) | 0.265 | ||
| Others | 70 | 0.805 (0.196–3.304) | 0.763 | 0.365 (0.09–1.477) | 0.158 | 0.376 (0.092–1.546) | 0.175 | ||
| Histologic grade | 0.005 | 0.347 | 0.002 | 0.706 | |||||
| 1 | 273 | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - |
| 2 | 640 | 2.605 (0.767–8.845) | 0.125 | 1.315 (0.38–4.55) | 0.666 | 2.563 (1.211–5.424) | 0.014 | 1.362 (0.629–2.951) | 0.433 |
| 3 | 889 | 4.787 (1.49–15.38) | 0.009 | 1.86 (0.557–6.208) | 0.313 | 3.481 (1.689–7.177) | <0.001 | 1.377 (0.643–2.95) | 0.41 |
| Unknown | 5 | - | - | ||||||
| ER | |||||||||
| Negative | 267 | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - |
| ≥1% | 1540 | 0.56 (0.32–0.98) | 0.042 | 0.482 (0.26–0.895) | 0.021 | 0.594 (0.401–0.88) | 0.009 | 0.513 (0.331–0.794) | 0.003 |
| PgR | |||||||||
| Negative | 165 | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - |
| ≥1% | 1642 | 0.347 (0.196–0.616) | <0.001 | 0.298 (0.162–0.548) | <0.001 | 0.472 (0.304–0.731) | <0.001 | 0.389 (0.246–0.615) | <0.001 |
| Hormone therapy type | <0.001 | 0.706 | <0.001 | <0.001 | |||||
| Anti-estrogens | 1146 | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - |
| Enzyme-inhibitors | 195 | 3.475 (1.88–6.424) | <0.001 | 1.298 (0.676–2.49) | 0.433 | 3.694 (2.313–5.898) | <0.001 | 1.981 (1.202–3.265) | 0.007 |
| Both | 466 | 2.068 (1.199–3.567) | 0.009 | 1.032 (0.581–1.833) | 0.915 | 3.727 (2.573–5.4) | <0.001 | 2.417 (1.627–3.593) | <0.001 |
| Chemotherapy | |||||||||
| No | 792 | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - |
| Yes | 1015 | 3.574 (1.916–6.667) | <0.001 | 0.829 (0.405–1.696) | 0.607 | 2.632 (1.785–3.882) | <0.001 | 0.811 (0.506–1.298) | 0.382 |
| Radiotherapy | |||||||||
| No | 930 | 1 (ref) | - | 1 (ref) | - | ||||
| Yes | 877 | 1.57 (0.966–2.551) | 0.069 | 1.097 (0.791–1.521) | 0.58 | ||||
| Characteristic | BCSS | DFS | |||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Univariate | Multivariate | Univariate | Multivariate | |||||
| 717 | HR (95% CI) a | p | HR (95% CI) a | p | HR (95% CI) a | p | HR (95% CI) a | p | |
| Age | |||||||||
| <50 | 333 | 1 (ref) | - | 1 (ref) | - | ||||
| ≥50 | 384 | 1.137 (0.697–1.855) | 0.606 | 0.97 (0.646–1.457) | 0.883 | ||||
| Operation type | |||||||||
| BCS | 284 | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - |
| MRM | 433 | 3.173 (1.695–5.939) | <0.001 | 1.952 (1.187–3.209) | 0.008 | 2.333 (1.446–3.764) | <0.001 | 1.484 (1.047–2.104) | 0.027 |
| Tumor size (cm) | <0.001 | <0.001 | <0.001 | <0.001 | |||||
| ≤2 | 448 | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - |
| >2, ≤5 | 239 | 4.663 (2.6–8.363) | <0.001 | 2.654 (1.64–4.295) | <0.001 | 3.654 (2.32–5.755) | <0.001 | 2.367 (1.655–3.384) | <0.001 |
| >5 | 30 | 11.627 (5.394–25.065) | <0.001 | 5.821 (3.128–10.831) | <0.001 | 7.468 (3.81–14.639) | <0.001 | 4.533 (2.712–7.576) | <0.001 |
| Lymph node | |||||||||
| Negative | 512 | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - |
| Positive | 205 | 5.155 (3.084–8.617) | <0.001 | 2.496 (1.564–3.984) | <0.001 | 3.393 (2.253–5.11) | <0.001 | 1.578 (1.117–2.23) | 0.01 |
| Histological subtype | 0.019 | 0.493 | 0.081 | 0.256 | |||||
| Ductal | 626 | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - |
| Lobular | 35 | 2.576 (1.168–5.681) | 0.019 | 1.023 (0.494–2.12) | 0.951 | 2.264 (1.134–4.521) | 0.021 | 0.913 (0.513–1.625) | 0.757 |
| Mixed (ductal and lobular) | 30 | 2.732 (1.171–6.372) | 0.02 | 1.501 (0.875–2.575) | 0.14 | 1.764 (0.768–4.052) | 0.181 | 1.423 (0.932–2.173) | 0.102 |
| Others | 26 | 0.961 (0.234–3.951) | 0.957 | 0.803 (0.247–2.614) | 0.716 | 0.96 (0.303–3.044) | 0.945 | 0.604 (0.22–1.662) | 0.329 |
| Histologic grade | 0.111 | 0.314 | 0.024 | 0.226 | |||||
| 1 | 113 | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - |
| 2 | 244 | 2.997 (1.043–8.612) | 0.042 | 1.881 (0.654–5.408) | 0.241 | 3.268 (1.386–7.709) | 0.007 | 1.872 (0.918–3.82) | 0.085 |
| 3 | 357 | 2.918 (1.039–8.199) | 0.042 | 2.168 (0.765–6.142) | 0.145 | 2.584 (1.105–6.045) | 0.029 | 1.749 (0.863–3.545) | 0.121 |
| Unknown | 3 | - | - | ||||||
| ER | |||||||||
| Negative | 135 | 1 (ref) | - | 1 (ref) | - | ||||
| ≥1% | 582 | 0.785 (0.441–1.399) | 0.412 | 0.794 (0.488–1.291) | 0.352 | ||||
| PgR | |||||||||
| Negative | 82 | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - |
| ≥1% | 635 | 0.484 (0.263–0.888) | 0.019 | 0.374 (0.234–0.597) | <0.001 | 0.572 (0.334–0.98) | 0.042 | 0.466 (0.314–0.693) | <0.001 |
| Hormone therapy type | <0.001 | 0.018 | <0.001 | <0.001 | |||||
| Anti-estrogens | 497 | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - |
| Enzyme-inhibitors | 44 | 2.862 (1.246–6.571) | 0.013 | 1.707 (0.987–2.954) | 0.056 | 3.663 (1.865–7.196) | <0.001 | 2.227 (1.43–3.467) | <0.001 |
| Both | 176 | 3.12 (1.862–5.227) | <0.001 | 1.892 (1.21–2.956) | 0.005 | 3.707 (2.397–5.734) | <0.001 | 2.686 (1.895–3.807) | <0.001 |
| Chemotherapy | |||||||||
| No | 294 | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - | 1 (ref) | - |
| Yes | 423 | 2.694 (1.467–4.947) | 0.001 | 0.985 (0.564–1.72) | 0.957 | 2.248 (1.393–3.626) | <0.001 | 0.904 (0.602–1.358) | 0.628 |
| Radiotherapy | |||||||||
| No | 357 | 1 (ref) | - | 1 (ref) | - | ||||
| Yes | 360 | 1.02 (0.627–1.659) | 0.937 | 1.106 (0.736–1.663) | 0.627 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, T.-H.; Gao, H.-W.; Liao, G.-S.; Yu, J.-C.; Dai, M.-S.; Ho, J.-Y.; Yu, C.-P. Amongst Women Stratified to Receive Endocrine Therapy on the Basis of Their Tumor Estrogen and Progesterone Receptor Levels, Those with Higher Tumor Progesterone Receptor Levels Had a Better Outcome Than Those with Lower Levels of Tumor Progesterone Receptor. Cancers 2021, 13, 905. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040905
Lin T-H, Gao H-W, Liao G-S, Yu J-C, Dai M-S, Ho J-Y, Yu C-P. Amongst Women Stratified to Receive Endocrine Therapy on the Basis of Their Tumor Estrogen and Progesterone Receptor Levels, Those with Higher Tumor Progesterone Receptor Levels Had a Better Outcome Than Those with Lower Levels of Tumor Progesterone Receptor. Cancers. 2021; 13(4):905. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040905
Chicago/Turabian StyleLin, Tai-Han, Hong-Wei Gao, Guo-Shiou Liao, Jyh-Cherng Yu, Ming-Shen Dai, Jar-Yi Ho, and Cheng-Ping Yu. 2021. "Amongst Women Stratified to Receive Endocrine Therapy on the Basis of Their Tumor Estrogen and Progesterone Receptor Levels, Those with Higher Tumor Progesterone Receptor Levels Had a Better Outcome Than Those with Lower Levels of Tumor Progesterone Receptor" Cancers 13, no. 4: 905. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040905