
Salvage-Radiation Therapy and Regional Hyperthermia for Biochemically Recurrent Prostate Cancer after Radical Prostatectomy (Results of the Planned Interim Analysis)

 , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract
1. Background
2. Results
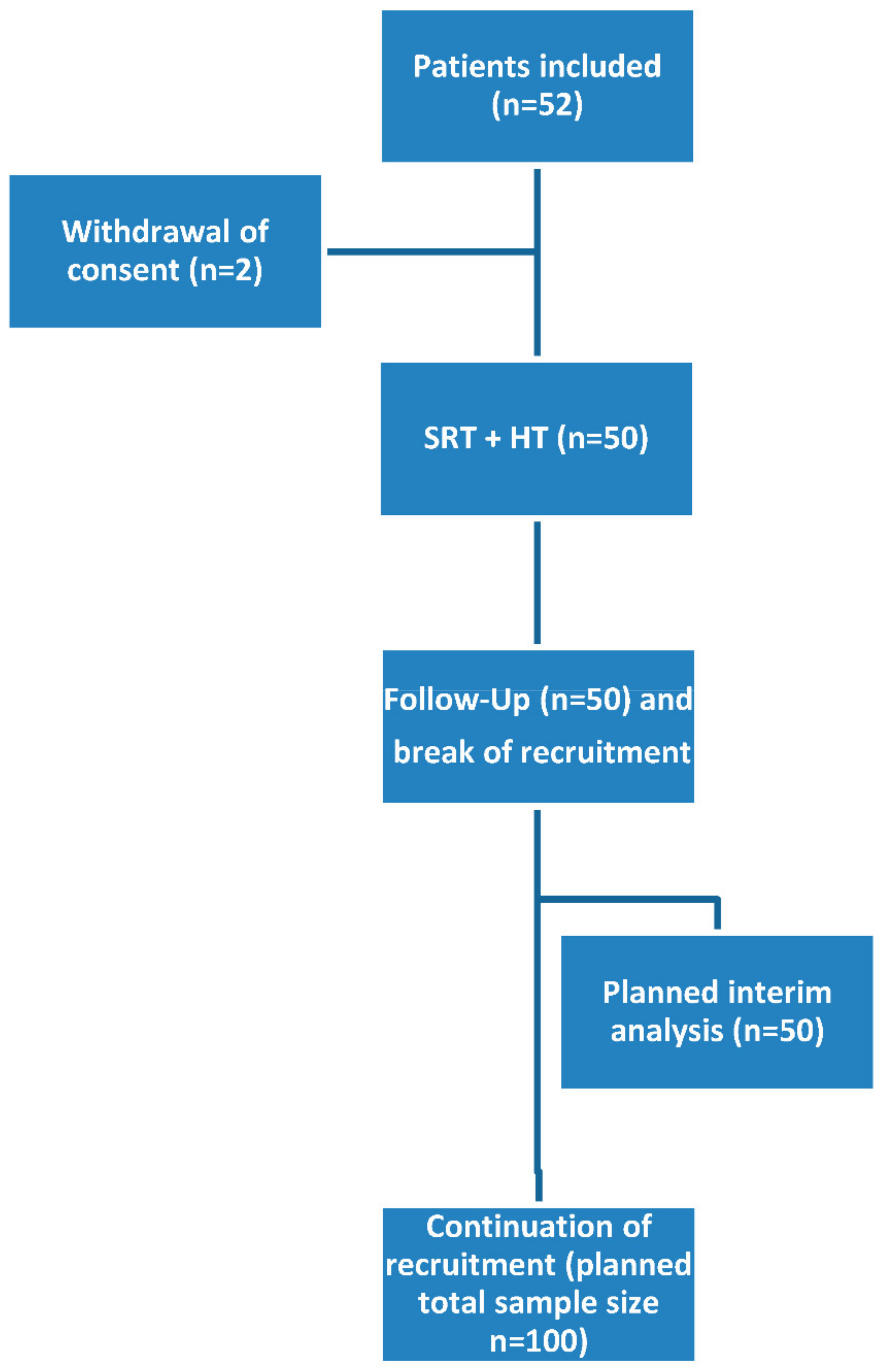
2.1. Patient Characteristics
2.2. Acute GU-, GI- and HT-Specific Toxicity
2.3. Feasibility and Safety
2.3.1. The Numbers and Parameters of Applicated HT and SRT Treatments
2.3.2. Early Quality of Life
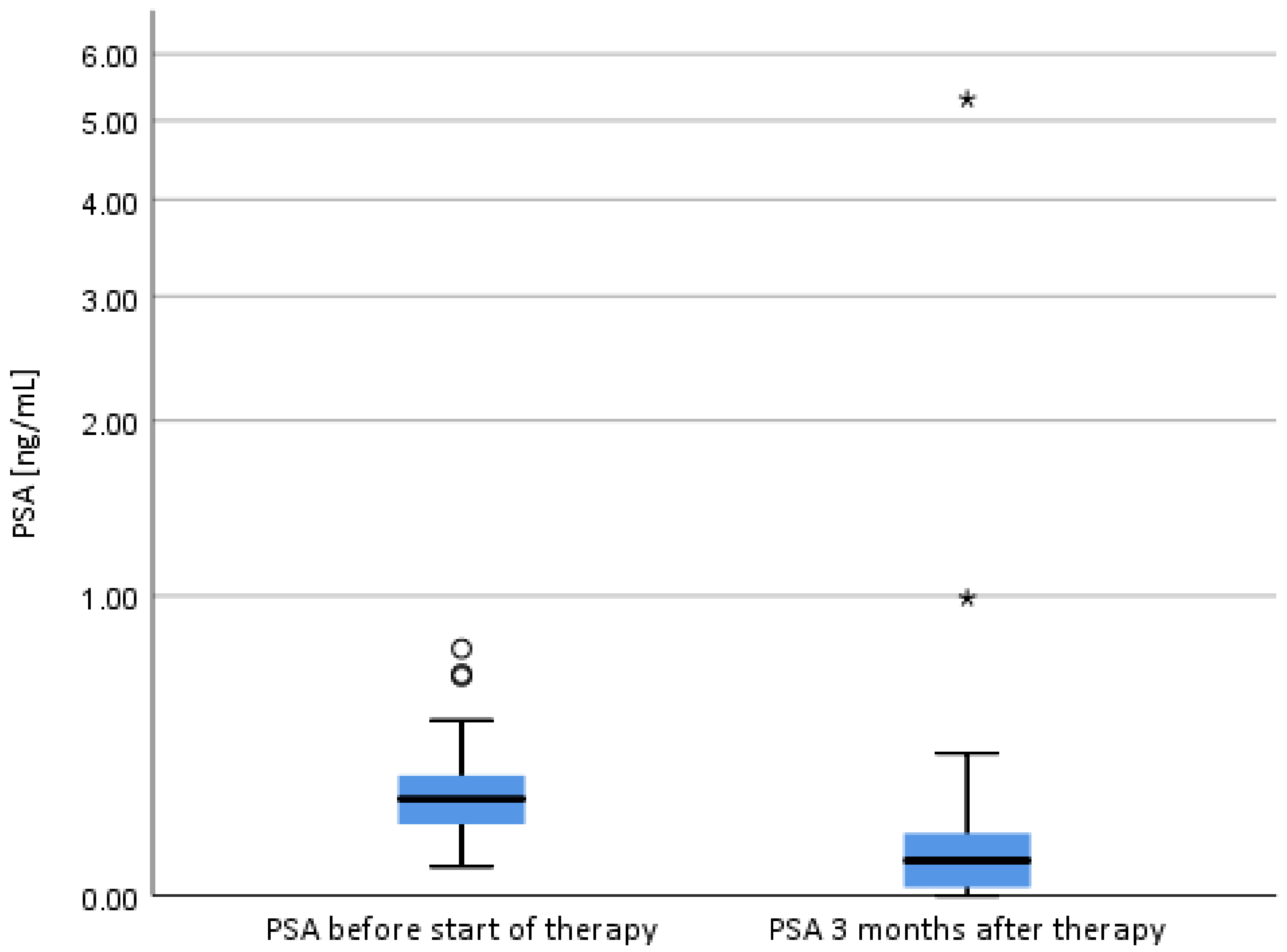
2.3.3. Short-Term PSA-Development
3. Discussion
4. Methods
4.1. Trial Design
4.2. Patients
Main Inclusion Criteria
4.3. Main Exclusion Criteria
4.4. Treatment and Follow-Up Procedures
4.5. Radiation Therapy
4.6. Hyperthermia
4.7. Observation of Toxicity and QoL
4.8. Follow-Up
4.9. End Points, Study Design and Sample Size
4.9.1. Primary Endpoint
4.9.2. Secondary Endpoints
4.9.3. Study Design and Sample Size
4.10. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ward, J.F.; Moul, J.W. Rising prostate-specific antigen after primary prostate cancer therapy. Nat. Clin. Pract. Urol. 2005, 2, 174–182. [Google Scholar] [CrossRef]
- Swanson, G.P.; Hussey, M.A.; Tangen, C.M.; Chin, J.; Messing, E.; Canby-Hagino, E.; Forman, J.D.; Thompson, I.M.; Crawford, E.D. Predominant treatment failure in postprostatectomy patients is local: Analysis of patterns of treatment failure in SWOG 8794. J. Clin. Oncol. 2007, 25, 2225–2229. [Google Scholar] [CrossRef] [Green Version]
- Vale, C.L.; Fisher, D.; Kneebone, A.; Parker, C.; Pearse, M.; Richaud, P.; Sargos, P.; Sydes, M.R.; Brawley, C.; Brihoum, M.; et al. Adjuvant or early salvage radiotherapy for the treatment of localised and locally advanced prostate cancer: A prospectively planned systematic review and meta-analysis of aggregate data. Lancet 2020, 396, 1422–1431. [Google Scholar] [CrossRef]
- Parker, C.C.; Clarke, N.W.; Cook, A.D.; Kynaston, H.G.; Petersen, P.M.; Catton, C.; Cross, W.; Logue, J.; Parulekar, W.; Payne, H.; et al. Timing of radiotherapy after radical prostatectomy (RADICALS-RT): A randomised, controlled phase 3 trial. Lancet 2020, 396, 1413–1421. [Google Scholar] [CrossRef]
- Sargos, P.; Chabaud, S.; Latorzeff, I.; Magne, N.; Benyoucef, A.; Supiot, S.; Pasquier, D.; Abdiche, M.S.; Gilliot, O.; Graff-Cailleaud, P.; et al. Adjuvant radiotherapy versus early salvage radiotherapy plus short-term androgen deprivation therapy in men with localised prostate cancer after radical prostatectomy (GETUG-AFU 17): A randomised, phase 3 trial. Lancet Oncol. 2020, 21, 1341–1352. [Google Scholar] [CrossRef]
- Kneebone, A.; Fraser-Browne, C.; Duchesne, G.M.; Fisher, R.; Frydenberg, M.; Herschtal, A.; Williams, S.G.; Brown, C.; Delprado, W.; Haworth, A.; et al. Adjuvant radiotherapy versus early salvage radiotherapy following radical prostatectomy (TROG 08.03/ANZUP RAVES): A randomised, controlled, phase 3, non-inferiority trial. Lancet Oncol. 2020, 21, 1331–1340. [Google Scholar] [CrossRef]
- Trock, B.J.; Han, M.; Freedland, S.J.; Humphreys, E.B.; DeWeese, T.L.; Partin, A.W.; Walsh, P.C. Prostate cancer-specific survival following salvage radiotherapy vs observation in men with biochemical recurrence after radical prostatectomy. JAMA 2008, 299, 2760–2769. [Google Scholar] [CrossRef] [Green Version]
- Stephenson, A.J.; Scardino, P.T.; Kattan, M.W.; Pisansky, T.M.; Slawin, K.M.; Klein, E.A.; Anscher, M.S.; Michalski, J.M.; Sandler, H.M.; Lin, D.W.; et al. Predicting the outcome of salvage radiation therapy for recurrent prostate cancer after radical prostatectomy. J. Clin. Oncol. 2007, 25, 2035–2041. [Google Scholar] [CrossRef] [PubMed]
- Pisansky, T.M.; Kozelsky, T.F.; Myers, R.P.; Hillman, D.W.; Blute, M.L.; Buskirk, S.J.; Cheville, J.C.; Ferrigni, R.G.; Schild, S.E. Radiotherapy for isolated serum prostate specific antigen elevation after prostatectomy for prostate cancer. J. Urol. 2000, 163, 845–850. [Google Scholar] [CrossRef]
- Viani, G.A.; Stefano, E.J.; Afonso, S.L. Higher-than-conventional radiation doses in localized prostate cancer treatment: A meta-analysis of randomized, controlled trials. Int. J. Radiat. Oncol. Biol. Phys. 2009, 74, 1405–1418. [Google Scholar] [CrossRef]
- Ghadjar, P.; Hayoz, S.; Bernhard, J.; Zwahlen, D.R.; Holscher, T.; Gut, P.; Guckenberger, M.; Hildebrandt, G.; Muller, A.C.; Plasswilm, L.; et al. Acute toxicity and quality of life after dose-intensified salvage radiation therapy for biochemically recurrent prostate cancer after prostatectomy: First results of the randomized trial SAKK 09/10. J. Clin. Oncol. 2015, 33, 4158–4166. [Google Scholar] [CrossRef] [PubMed]
- Qi, X.; Li, H.Z.; Gao, X.S.; Qin, S.B.; Zhang, M.; Li, X.M.; Li, X.Y.; Ma, M.W.; Bai, Y.; Li, X.Y.; et al. Toxicity and biochemical outcomes of dose-intensified postoperative radiation therapy for prostate cancer: Results of a randomized Phase III Trial. Int. J. Radiat. Oncol. Biol. Phys. 2020, 106, 282–290. [Google Scholar] [CrossRef] [Green Version]
- King, C.R.; Spiotto, M.T. Improved outcomes with higher doses for salvage radiotherapy after prostatectomy. Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 23–27. [Google Scholar] [CrossRef]
- King, C.R.; Kapp, D.S. Radiotherapy after prostatectomy: Is the evidence for dose escalation out there? Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 346–350. [Google Scholar] [CrossRef] [PubMed]
- Ohri, N.; Dicker, A.P.; Trabulsi, E.J.; Showalter, T.N. Can early implementation of salvage radiotherapy for prostate cancer improve the therapeutic ratio? A systematic review and regression meta-analysis with radiobiological modelling. Eur. J. Cancer 2012, 48, 837–844. [Google Scholar] [CrossRef] [PubMed]
- King, C.R. The dose-response of salvage radiotherapy following radical prostatectomy: A systematic review and meta-analysis. Radiother. Oncol. 2016, 121, 199–203. [Google Scholar] [CrossRef] [Green Version]
- Shipley, W.U.; Seiferheld, W.; Lukka, H.R.; Major, P.P.; Heney, N.M.; Grignon, D.J.; Sartor, O.; Patel, M.P.; Bahary, J.P.; Zietman, A.L.; et al. Radiation with or without antiandrogen therapy in recurrent prostate cancer. N. Engl. J. Med. 2017, 376, 417–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrie, C.; Magne, N.; Burban-Provost, P.; Sargos, P.; Latorzeff, I.; Lagrange, J.L.; Supiot, S.; Belkacemi, Y.; Peiffert, D.; Allouache, N.; et al. Short-term androgen deprivation therapy combined with radiotherapy as salvage treatment after radical prostatectomy for prostate cancer (GETUG-AFU 16): A 112-month follow-up of a phase 3, randomised trial. Lancet Oncol. 2019, 20, 1740–1749. [Google Scholar] [CrossRef]
- Spratt, D.E.; Dess, R.T.; Zumsteg, Z.S.; Lin, D.W.; Tran, P.T.; Morgan, T.M.; Antonarakis, E.S.; Nguyen, P.L.; Ryan, C.J.; Sandler, H.M.; et al. A systematic review and framework for the use of hormone therapy with salvage radiation therapy for recurrent prostate cancer. Eur. Urol. 2018, 73, 156–165. [Google Scholar] [CrossRef]
- Nguyen, P.L.; Alibhai, S.M.; Basaria, S.; D’Amico, A.V.; Kantoff, P.W.; Keating, N.L.; Penson, D.F.; Rosario, D.J.; Tombal, B.; Smith, M.R. Adverse effects of androgen deprivation therapy and strategies to mitigate them. Eur. Urol. 2015, 67, 825–836. [Google Scholar] [CrossRef]
- Gay, H.A.; Sanda, M.G.; Liu, J.; Wu, N.; Hamstra, D.A.; Wei, J.T.; Dunn, R.L.; Klein, E.A.; Sandler, H.M.; Saigal, C.S.; et al. External beam radiation therapy or brachytherapy with or without short-course neoadjuvant androgen deprivation therapy: Results of a multicenter, prospective study of quality of life. Int. J. Radiat. Oncol. Biol. Phys. 2017, 98, 304–317. [Google Scholar] [CrossRef] [Green Version]
- Wust, P.; Hildebrandt, B.; Sreenivasa, G.; Rau, B.; Gellermann, J.; Riess, H.; Felix, R.; Schlag, P.M. Hyperthermia in combined treatment of cancer. Lancet Oncol. 2002, 3, 487–497. [Google Scholar] [CrossRef]
- Peeken, J.C.; Vaupel, P.; Combs, S.E. Integrating hyperthermia into modern radiation oncology: What evidence is necessary? Front. Oncol. 2017, 7, 132. [Google Scholar] [CrossRef] [Green Version]
- Issels, R.D.; Lindner, L.H.; Verweij, J.; Wessalowski, R.; Reichardt, P.; Wust, P.; Ghadjar, P.; Hohenberger, P.; Angele, M.; Salat, C.; et al. Effect of neoadjuvant chemotherapy plus regional hyperthermia on long-term outcomes among patients with localized high-risk soft tissue sarcoma: The EORTC 62961-ESHO 95 randomized clinical trial. JAMA Oncol. 2018, 4, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Anscher, M.S.; Samulski, T.V.; Dodge, R.; Prosnitz, L.R.; Dewhirst, M.W. Combined external beam irradiation and external regional hyperthermia for locally advanced adenocarcinoma of the prostate. Int. J. Radiat. Oncol. Biol. Phys. 1997, 37, 1059–1065. [Google Scholar] [CrossRef]
- Van Vulpen, M.; De Leeuw, J.R.; Van Gellekom, M.P.; Van Der Hoeven, J.; De Graeff, A.; Van Moorselaar, R.J.; Van Der Tweel, I.; Hofman, P.; Lagendijk, J.J.; Battermann, J.J. A prospective quality of life study in patients with locally advanced prostate cancer, treated with radiotherapy with or without regional or interstitial hyperthermia. Int. J. Hyperth. 2003, 19, 402–413. [Google Scholar] [CrossRef] [PubMed]
- Tilly, W.; Gellermann, J.; Graf, R.; Hildebrandt, B.; Weissbach, L.; Budach, V.; Felix, R.; Wust, P. Regional hyperthermia in conjunction with definitive radiotherapy against recurrent or locally advanced prostate cancer T3 pN0 M0. Strahlenther Onkol. 2005, 181, 35–41. [Google Scholar] [CrossRef]
- Maluta, S.; Dall’Oglio, S.; Romano, M.; Marciai, N.; Pioli, F.; Giri, M.G.; Benecchi, P.L.; Comunale, L.; Porcaro, A.B. Conformal radiotherapy plus local hyperthermia in patients affected by locally advanced high risk prostate cancer: Preliminary results of a prospective phase II study. Int. J. Hyperth. 2007, 23, 451–456. [Google Scholar] [CrossRef]
- Van Vulpen, M.; De Leeuw, A.A.; Raaymakers, B.W.; Van Moorselaar, R.J.; Hofman, P.; Lagendijk, J.J.; Battermann, J.J. Radiotherapy and hyperthermia in the treatment of patients with locally advanced prostate cancer: Preliminary results. BJU Int. 2004, 93, 36–41. [Google Scholar] [CrossRef]
- Kok, H.P.; Crezee, J.; Franken, N.A.; Stalpers, L.J.; Barendsen, G.W.; Bel, A. Quantifying the combined effect of radiation therapy and hyperthermia in terms of equivalent dose distributions. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 739–745. [Google Scholar] [CrossRef]
- Muller, A.C.; Zips, D.; Heinrich, V.; Lamprecht, U.; Voigt, O.; Burock, S.; Budach, V.; Wust, P.; Ghadjar, P. Regional hyperthermia and moderately dose-escalated salvage radiotherapy for recurrent prostate cancer. Protocol of a phase II trial. Radiat. Oncol. 2015, 10, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruggmoser, G.; Bauchowitz, S.; Canters, R.; Crezee, H.; Ehmann, M.; Gellermann, J.; Lamprecht, U.; Lomax, N.; Messmer, M.B.; Ott, O.; et al. Quality assurance for clinical studies in regional deep hyperthermia. Strahlenther Onkol. 2011, 187, 605–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lagendijk, J.J.; Van Rhoon, G.C.; Hornsleth, S.N.; Wust, P.; De Leeuw, A.C.; Schneider, C.J.; Van Dijk, J.D.; Van Der Zee, J.; Van Heek-Romanowski, R.; Rahman, S.A.; et al. ESHO quality assurance guidelines for regional hyperthermia. Int. J. Hyperth. 1998, 14, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Sreenivasa, G.; Gellermann, J.; Rau, B.; Nadobny, J.; Schlag, P.; Deuflhard, P.; Felix, R.; Wust, P. Clinical use of the hyperthermia treatment planning system HyperPlan to predict effectiveness and toxicity. Int. J. Radiat. Oncol. Biol. Phys. 2003, 55, 407–419. [Google Scholar] [CrossRef]
- Fatehi, D.; Van der Zee, J.; De Bruijne, M.; Franckena, M.; Van Rhoon, G.C. RF-power and temperature data analysis of 444 patients with primary cervical cancer: Deep hyperthermia using the Sigma-60 applicator is reproducible. Int. J. Hyperth. 2007, 23, 623–643. [Google Scholar] [CrossRef] [PubMed]
- Tilly, W.; Wust, P.; Rau, B.; Harder, C.; Gellermann, J.; Schlag, P.; Budach, V.; Felix, R. Temperature data and specific absorption rates in pelvic tumours: Predictive factors and correlations. Int. J. Hyperth. 2001, 17, 172–188. [Google Scholar] [CrossRef]
- Carrie, C.; Hasbini, A.; De Laroche, G.; Richaud, P.; Guerif, S.; Latorzeff, I.; Supiot, S.; Bosset, M.; Lagrange, J.L.; Beckendorf, V.; et al. Salvage radiotherapy with or without short-term hormone therapy for rising prostate-specific antigen concentration after radical prostatectomy (GETUG-AFU 16): A randomised, multicentre, open-label phase 3 trial. Lancet Oncol. 2016, 17, 747–756. [Google Scholar] [CrossRef]
- Ghadjar, P.; Aebersold, D.M.; Albrecht, C.; Bohmer, D.; Flentje, M.; Ganswindt, U.; Hocht, S.; Holscher, T.; Sedlmayer, F.; Wenz, F.; et al. Use of androgen deprivation and salvage radiation therapy for patients with prostate cancer and biochemical recurrence after prostatectomy. Strahlenther Onkol. 2018, 194, 619–626. [Google Scholar] [CrossRef] [PubMed]
- Yokomizo, A.; Wakabayashi, M.; Satoh, T.; Hashine, K.; Inoue, T.; Fujimoto, K.; Egawa, S.; Habuchi, T.; Kawashima, K.; Ishizuka, O.; et al. Salvage radiotherapy versus hormone therapy for prostate-specific antigen failure after radical prostatectomy: A randomised, multicentre, open-label, Phase 3 Trial (JCOG0401)(dagger). Eur. Urol. 2019. [Google Scholar] [CrossRef]
- Poortmans, P.; Bossi, A.; Vandeputte, K.; Bosset, M.; Miralbell, R.; Maingon, P.; Boehmer, D.; Budiharto, T.; Symon, Z.; Van den Bergh, A.C.; et al. Guidelines for target volume definition in post-operative radiotherapy for prostate cancer, on behalf of the EORTC radiation oncology group. Radiother Oncol. 2007, 84, 121–127. [Google Scholar] [CrossRef]
- Van Andel, G.; Bottomley, A.; Fossa, S.D.; Efficace, F.; Coens, C.; Guerif, S.; Kynaston, H.; Gontero, P.; Thalmann, G.; Akdas, A.; et al. An international field study of the EORTC QLQ-PR25: A questionnaire for assessing the health-related quality of life of patients with prostate cancer. Eur. J. Cancer 2008, 44, 2418–2424. [Google Scholar] [CrossRef] [PubMed]
- Roth, A.J.; Rosenfeld, B.; Kornblith, A.B.; Gibson, C.; Scher, H.I.; Curley-Smart, T.; Holland, J.C.; Breitbart, W. The memorial anxiety scale for prostate cancer: Validation of a new scale to measure anxiety in men with with prostate cancer. Cancer 2003, 97, 2910–2918. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | (N = 50) n (%) |
|---|---|
| Resection margins | |
| R0 | 31 (62.0) |
| R1 | 19 (38.0) |
| Gleason score | |
| ≤6 | 2 (4.0) |
| 7 | 36 (72.0) |
| ≥8 | 12 (24.0) |
| Tumor classification | |
| pT2a | 9 (18.0) |
| pT2b | 0 |
| pT2c | 22 (44.0) |
| pT3a | 8 (16.0) |
| pT3b | 11(22.0) |
| pT4 | 0 |
| Lymphadenectomy performed | |
| No | 1 (2.0) |
| Yes | 49 (98.0) |
| Lymphnode classification | |
| N0 | 50(100.0) |
| pN0 | 49 (98.0) |
| cN0 | 1 (2.0) |
| PSA at start of RT (ng/mL), median range | 0.25 (0.07–0.77) |
| Age at start of RT median (range) in years | 65.5 (51–79) |
| Time from surgery to RT start, median (range) in months | 21.5 (3–128) |
| WHO performance status at treatment start | |
| 0 | 47 (94.0) |
| 1 | 3 (6.0) |
| GU Toxicity | CTCAE Grade | Baseline Symptoms n (%) | During Treatment n (%) | Follow-Up at 3 Months n (%) |
|---|---|---|---|---|
| Cystitis | 0 | 48 (96.0) | 49 (98.0) | 48 (96.0) |
| 1 | 1 (2.0) | 1 (2.0) | 1 (2.0) | |
| 2 | 0 | 0 | 0 | |
| 3 | 0 | 0 | 0 | |
| missing | 1 (2.0) | 0 | 1 (2.0) | |
| Urinary | 0 | 36 (72.0) | 45(90.0) | 33 (66.0) |
| incontinence | 1 | 10 (20.0) | 4(8.0) | 13 (26.0) |
| 2 | 3 (6.0) | 1(2.0) | 3 (6.0) | |
| 3 | 0 | 0 | 0 | |
| missing | 1 (2.0) | 0 | 1 (2.0) | |
| Urinary | 0 | 46 (92.0) | 50 (100.0) | 46 (92.0) |
| retention | 1 | 3 (6.0) | 0 | 3 (6.0) |
| 2 | 0 | 0 | 0 | |
| 3 | 0 | 0 | 0 | |
| missing | 1 (2.0) | 0 | 1(2.0) | |
| Urinary | 0 | 34(68.0) | 20 (40.0) | 33 (66.0) |
| frequency | 1 | 15(30.0) | 26 (52.0) | 14 (28.0) |
| 2 | 1(2.0) | 4 (8.0) | 1 (2.0) | |
| 3 | 0 | 0 | 0 | |
| missing | 0 | 0 | 2 (4.0) | |
| Urinary | 0 | 39 (78.0) | 22 (44.0) | 36 (72.0) |
| urgency | 1 | 11(22.0) | 25 (50.0) | 12 (24.0) |
| 2 | 0 | 3 (6.0) | 0 | |
| 3 | 0 | 0 | 0 | |
| missing | 0 | 0 | 2 (4.0) | |
| Urinary | 0 | 47 (94.0) | 49 (98.0) | 48 (96.0) |
| hemorrhage | 1 | 0 | 1 (2.0) | 0 |
| 2 | 0 | 0 | 0 | |
| 3 | 0 | 0 | 0 | |
| missing | 3 (6.0) | 0 | 2 (4.0) | |
| Highest | 0 | 29 (58.0) | 18 (36.0) | 27 (54.0) |
| grade of GU | 1 | 18 (36.0) | 27 (54.0) | 19 (38.0) |
| symptoms / | 2 | 3 (6.0) | 5 (10.0) | 3 (6.0) |
| toxicity | 3 | 0 | 0 | 0 |
| missing | 0 | 0 | 1 (2.0) |
| GI Toxicity | CTCAE Grade | Baseline Symptoms n (%) | During Treatment n (%) | Follow-Up at 3 Months n (%) |
|---|---|---|---|---|
| Anal or | 0 | 49 (98.0) | 46 (92.0) | 47(94.0) |
| rectal | 1 | 0 | 2 (4.0) | 1 (2.0) |
| hemorrhage | 2 | 0 | 2 (4.0) | 1 (2.0) |
| 3 | 0 | 0 | 0 | |
| missing | 1 (2.0) | 0 | 1 (2.0) | |
| Diarrhea | 0 | 48 (96.0) | 45 (90.0) | 47 (94.0) |
| 1 | 1 (2.0) | 5 (10.0) | 2 (4.0) | |
| 2 | 0 | 0 | 0 | |
| 3 | 0 | 0 | 0 | |
| missing | 1 (2.0) | 0 | 1 (2.0) | |
| Rectal pain | 0 | 48 (96.0) | 41 (82.0) | 48 (96.0) |
| 1 | 2 (4.0) | 8 (16.0) | 1 (2.0) | |
| 2 | 0 | 1 (2.0) | 0 | |
| 3 | 0 | 0 | 0 | |
| missing | 0 | 0 | 1 (2.0) | |
| Fecal | 0 | 50(100.0) | 49 (98.0) | 48 (96.0) |
| incontinence | 1 | 0 | 1 (2.0) | 1 (2.0) |
| 2 | 0 | 0 | 0 | |
| 3 | 0 | 0 | 0 | |
| missing | 0 | 0 | 1 (2.0) | |
| Highest | 0 | 47(94.0) | 36 (72.0) | 43 (86.0) |
| grade of GI | 1 | 3 (6.0) | 12 (24.0) | 5 (10.0) |
| symptoms / | 2 | 0 | 2 (4.0) | 1 (2.0) |
| toxicity | 3 | 0 | 0 | 0 |
| Highest | missing | 0 | 0 | 1 (2.0) |
| HT Symptoms | CTCAE Grade | During Treatment n (%) | Follow-Up at 3 Months n (%) |
|---|---|---|---|
| Skin pain | 0 | 45 (90.0) | 49 (98.0) |
| 1 | 5 (10.0) | 0 | |
| 2 | 0 | 0 | |
| 3 | 0 | 0 | |
| missing | 0 | 1 (2.0) | |
| Abdominal pain | 0 | 44 (88.0) | 47 (94.0) |
| 1 | 5 (10.0) | 1 (2.0) | |
| 2 | 0 | 1 (2.0) | |
| 3 | 1 (2.0) | 0 | |
| missing | 0 | 1 (2.0) | |
| Edema | 0 | 48 (96.0) | 46 (92.0) |
| 1 | 2(4.0) | 2 (4.0) | |
| 2 | 0 | 1 (2.0) | |
| 3 | 0 | 0 | |
| missing | 0 | 1 (2.0) | |
| Burn | 0 | 46 (92.0) | 49 (98.0) |
| 1 | 3 (6.0) | 0 | |
| 2 | 1 (2.0) | 0 | |
| 3 | 0 | 0 | |
| missing | 0 | 1 (2.0) | |
| Claustrophobia | 0 | 49(98.0) | # |
| 1 | 1(2.0) | # | |
| 2 | 0 | # | |
| 3 | 0 | # | |
| missing | 0 | # | |
| Hot spots | 0 | 41 (82) | # |
| 1 | 9 (18.0) | # | |
| 2 | 0 | # | |
| missing | 0 | # | |
| Bolus pressure | 0 | 41 (82.0) | # |
| 1 | 9 (18.0) | # | |
| 2 | 0 | # | |
| missing | 0 | # | |
| Highest | 0 | 27 (54.0) | 44 (88.0) |
| grade of HT | 1 | 21 (42.0) | 3 (6.0) |
| symptoms | 2 | 1 (2.0) | 2 (4.0) |
| 3 | 1 (2.0) | 0 | |
| missing | 0 | 1 (2.0) |
| QLQ-PR25 | Baseline | 3-Months-Follow-Up | |||
|---|---|---|---|---|---|
| Number of Respondents | Mean (sd) | Number of Respondents | Mean (sd) | p-Value # | |
| Symptom Scales: * | |||||
| Urinary symptoms (PRURI) | 44 | 23.1 (16.8) | 32 | 23.4 (16.1) | 0.672 |
| Bowel symptoms (PRBOW) | 40 | 4.9 (6.8) | 31 | 4.8 (9.6) | 0.845 |
| Functional Scales: ** | |||||
| Sexual activity (PRSAC) | 42 | 59.5 (31.7) | 30 | 62.8 (28.9) | 0.780 |
| Sexual functioning (PRSFU) | 20 | 52.3 (18.6) | 15 | 58.0 (28.6) | 0.621 |
| QLQ-C30 | Baseline | 3-Months-Follow-Up | |||
| Number of Respondents | Mean (sd) | Number of Respondents | Mean (sd) | p-Value # | |
| Symptom Scales: * | |||||
| Fatigue (FA) | 45 | 17.5 (19.4) | 33 | 15.3 (21.8) | 0.386 |
| Nausea and Vomiting (NV) | 45 | 0.37 (2.5) | 32 | 2.1 (7.0) | 0.263 |
| Pain (PA) | 45 | 9.6 (16.9) | 33 | 8.1 (16.7) | 0.707 |
| Dyspnoe (DY) | 45 | 8.1 (17.6) | 32 | 10.4 (23.1) | 0.831 |
| Insomnia (SL) | 45 | 21.5 (24.8) | 33 | 19.2 (26.4) | 0.662 |
| Appetite Loss (AP) | 45 | 5.9 (17.8) | 32 | 4.2 (11.2) | 0.325 |
| Constipation (CO) | 45 | 2.2 (8.4) | 32 | 2.1 (8.2) | 1.0 |
| Diarrhoea (DI) | 43 | 7.7 (19.0) | 29 | 10.3 (20.1) | 0.17 |
| Financial Difficulties (FI) | 44 | 0 (0) | 29 | 2.3 (8.6) | 0.161 |
| Functional Scales: ** | |||||
| Physical Functioning (PF2) | 45 | 93.5 (11.2) | 32 | 92.3 (13.2) | 0.946 |
| Role Functioning (RF2) | 45 | 89.3 (18.5) | 32 | 83.9 (24.4) | 0.347 |
| Emotional Functioning (EF) | 44 | 77.5 (21.6) | 29 | 82.1 (21.0) | 0.770 |
| Cognitive Functioning (CF) | 44 | 93.6 (12.0) | 29 | 90.8 (14.5) | 0.394 |
| Social Functioning (SF) | 44 | 85.6 (19.2) | 29 | 82.2 (24.8) | 0.259 |
| Global health status (QOL): | |||||
| 44 | 72.9 (17.7) | 29 | 72.7 (17.2) | 0.458 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beck, M.; Ghadjar, P.; Mehrhof, F.; Zips, D.; Paulsen, F.; Wegener, D.; Burock, S.; Kaul, D.; Stromberger, C.; Nadobny, J.; et al. Salvage-Radiation Therapy and Regional Hyperthermia for Biochemically Recurrent Prostate Cancer after Radical Prostatectomy (Results of the Planned Interim Analysis). Cancers 2021, 13, 1133. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13051133
Beck M, Ghadjar P, Mehrhof F, Zips D, Paulsen F, Wegener D, Burock S, Kaul D, Stromberger C, Nadobny J, et al. Salvage-Radiation Therapy and Regional Hyperthermia for Biochemically Recurrent Prostate Cancer after Radical Prostatectomy (Results of the Planned Interim Analysis). Cancers. 2021; 13(5):1133. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13051133
Chicago/Turabian StyleBeck, Marcus, Pirus Ghadjar, Felix Mehrhof, Daniel Zips, Frank Paulsen, Daniel Wegener, Susen Burock, David Kaul, Carmen Stromberger, Jacek Nadobny, and et al. 2021. "Salvage-Radiation Therapy and Regional Hyperthermia for Biochemically Recurrent Prostate Cancer after Radical Prostatectomy (Results of the Planned Interim Analysis)" Cancers 13, no. 5: 1133. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13051133