
Optimization of the Clinical Setting Using Numerical Simulations of the Electromagnetic Field in an Obese Patient Model for Deep Regional Hyperthermia of an 8 MHz Radiofrequency Capacitively Coupled Device in the Pelvis

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
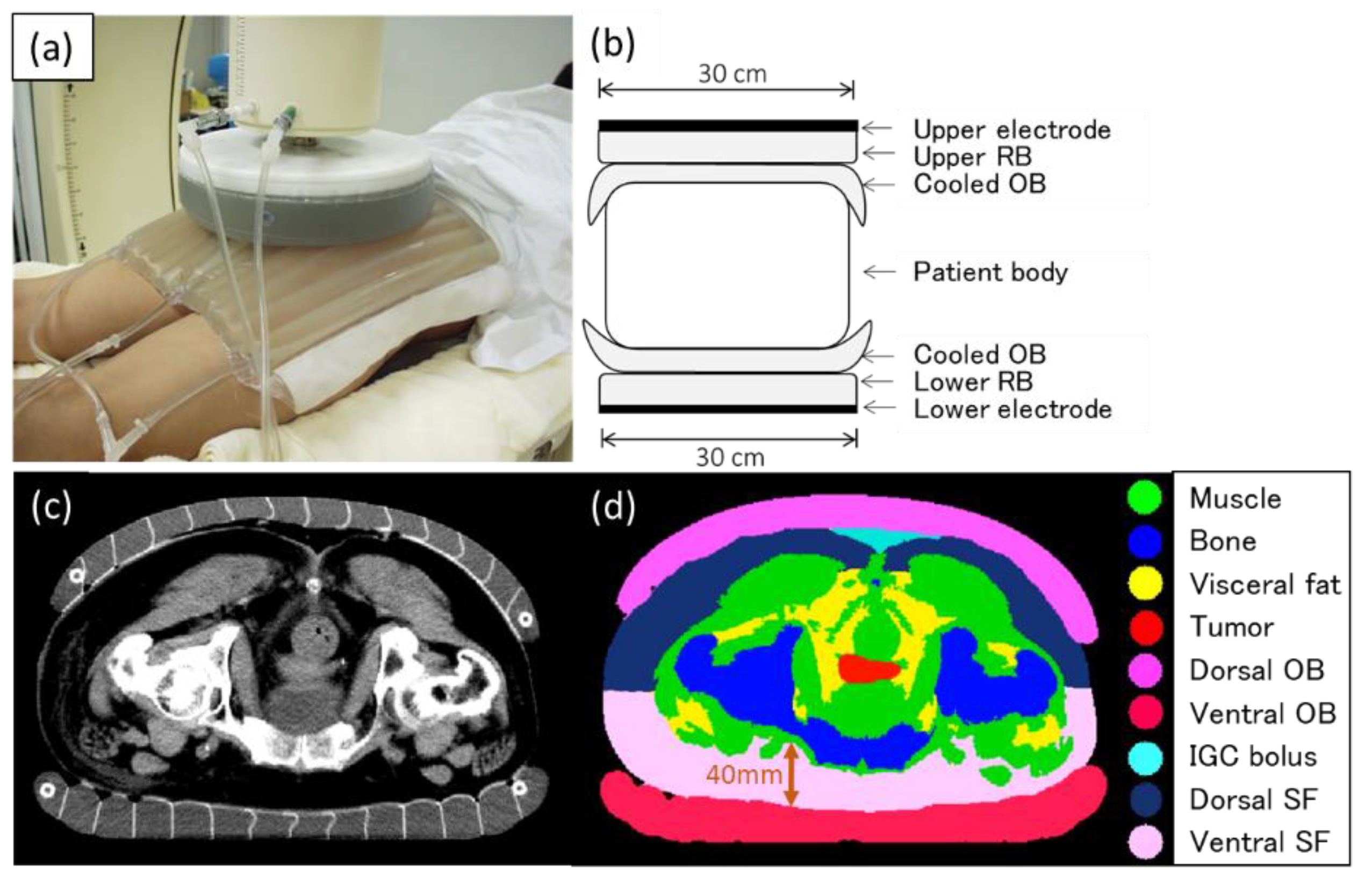
2.1. Patient Model
2.2. Electromagnetic Models
2.3. Evaluated Heating Settings
3. Results
3.1. Effect of the OB
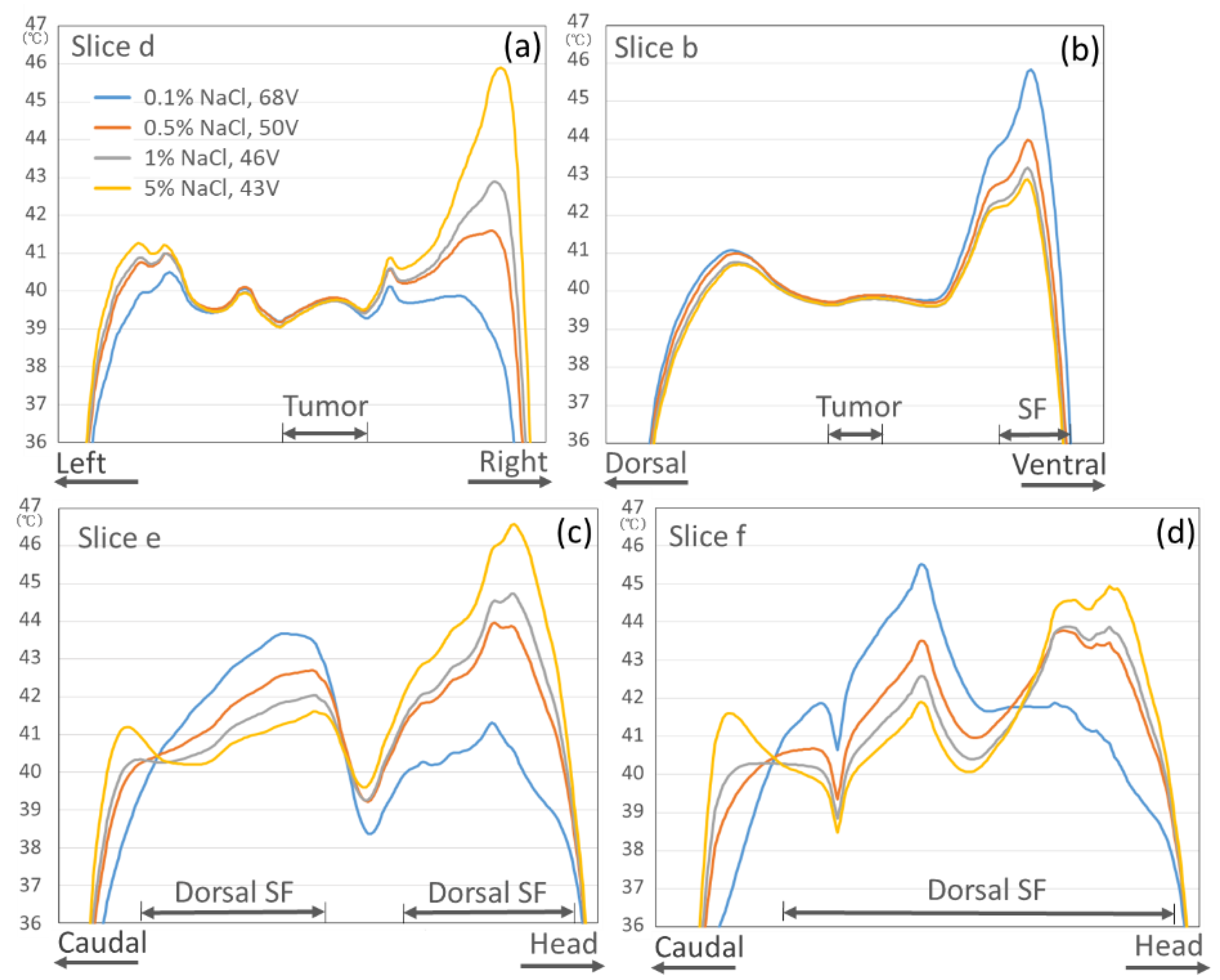
3.2. Effect of the Salt Solution Concentration in the OB
3.3. Effect of the IGC Bolus
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Datta, N.; Ordóñez, S.G.; Gaipl, U.; Paulides, M.; Crezee, H.; Gellermann, J.; Marder, D.; Puric, E.; Bodis, S. Local hyperthermia combined with radiotherapy and-/or chemotherapy: Recent advances and promises for the future. Cancer Treat. Rev. 2015, 41, 742–753. [Google Scholar] [CrossRef]
- van der Zee, J.; Gonzalez Gonzalez, D.; van Rhoon, G.C.; van Dijk, J.D.; van Putten, W.L.; Hart, A.A. Comparison of radiotherapy alone with radiotherapy plus hyperthermia in locally advanced pelvic tumours: A prospective, randomised, multicentre trial. Dutch Deep Hyperthermia Group. Lancet 2000, 355, 1119–1125. [Google Scholar] [CrossRef]
- Overgaard, J.; Gonzalez, D.G.; Hulshof, M.C.C.H.; Arcangeli, G.; Dahl, O.; Mella, O.; Bentzen, S.M. Hyperthermia as an adjuvant to radiation therapy of recurrent or metastatic malignant melanoma. A multicentre randomized trial by the European Society for Hyperthermic Oncology. Int. J. Hyperth. 1996, 12, 3–20. [Google Scholar] [CrossRef]
- Jones, E.L.; Samulski, T.V.; Vujaskovic, Z.; Leonard, R.P.; Dewhirst, M.W. Hyperthermia. In Principles and Practice of Radiation Oncology, 4th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2003. [Google Scholar]
- Ben-Hur, E.; Elkind, M.M. Thermally Enhanced Radioresponse of Cultured Chinese Hamster Cells: Damage and Repair of Single-Stranded DNA and a DNA Complex. Radiat. Res. 1974, 59, 484. [Google Scholar] [CrossRef]
- Issels, R.; Kampmann, E.; Kanaar, R.; Lindner, L.H. Hallmarks of hyperthermia in driving the future of clinical hyperthermia as targeted therapy: Translation into clinical application. Int. J. Hyperth. 2016, 32, 89–95. [Google Scholar] [CrossRef] [Green Version]
- Horsman, M.; Overgaard, J. Hyperthermia: A Potent Enhancer of Radiotherapy. Clin. Oncol. 2007, 19, 418–426. [Google Scholar] [CrossRef]
- Dewey, W.C.; Hopwood, L.E.; Sapareto, S.A.; Gerweck, L.E. Cellular Responses to Combinations of Hyperthermia and Radiation. Radiology 1977, 123, 463–474. [Google Scholar] [CrossRef]
- Van Rhoon, G.C. Is CEM43 still a relevant thermal dose parameter for hyperthermia treatment monitoring? Int. J. Hyperth. 2016, 32, 50–62. [Google Scholar] [CrossRef] [PubMed]
- Franckena, M.; Fatehi, D.; de Bruijne, M.; Canters, R.A.; van Norden, Y.; Mens, J.W.; van Rhoon, G.C.; van der Zee, J. Hyperthermia dose-effect relationship in 420 patients with cervical cancer treated with combined radiotherapy and hyperthermia. Eur. J. Cancer 2009, 45, 1969–1978. [Google Scholar] [CrossRef] [PubMed]
- Ohguri, T.; Harima, Y.; Imada, H.; Sakurai, H.; Ohno, T.; Hiraki, Y.; Tuji, K.; Tanaka, M.; Terashima, H. Relationships between thermal dose parameters and the efficacy of definitive chemoradiotherapy plus regional hyperthermia in the treatment of locally advanced cervical cancer: Data from a multicentre randomised clinical trial. Int. J. Hyperth. 2017, 34, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Sherar, M.; Liu, F.-F.; Pintilie, M.; Levin, W.; Hunt, J.; Hill, R.; Hand, J.; Vernon, C.; Van Rhoon, G.; Van Der Zee, J.; et al. Relationship between thermal dose and outcome in thermoradiotherapy treatments for superficial recurrences of breast cancer: Data from a phase III trial. Int. J. Radiat. Oncol. 1997, 39, 371–380. [Google Scholar] [CrossRef] [Green Version]
- Bruggmoser, G.; Bauchowitz, S.; Canters, R.; Crezee, H.; Ehmann, M.; Gellermann, J.; Lamprecht, U.; Lomax, N.; Messmer, M.B.; Ott, O.; et al. Quality assurance for clinical studies in regional deep hyperthermia. Strahlenther. Onkol. 2011, 187, 605–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Zee, J. Heating the patient: A promising approach? Ann. Oncol. 2002, 13, 1173–1184. [Google Scholar] [CrossRef]
- van der Zee, J.; Vujaskovic, Z.; Kondo, M.; Sugahara, T. The Kadota Fund International Forum 2004—Clinical group consensus. Int. J. Hyperth. 2008, 24, 111–122. [Google Scholar] [CrossRef] [Green Version]
- Abe, M.; Hiraoka, M.; Takahashi, M.; Egawa, S.; Matsuda, C.; Onoyama, Y.; Morita, K.; Kakehi, M.; Sugahara, T. Multi-institutional studies on hyperthermia using an 8-MHz radiofrequency capacitive heating device (thermotron RF-8) in combination with radiation for cancer therapy. Cancer 1986, 58, 1589–1595. [Google Scholar] [CrossRef]
- Ohguri, T.; Imada, H.; Yahara, K.; Kakeda, S.; Tomimatsu, A.; Kato, F.; Nomoto, S.; Terashima, H.; Korogi, Y. Effect of 8-MHz radiofrequency-capacitive regional hyperthermia with strong superficial cooling for unresectable or recurrent colorectal cancer. Int. J. Hyperth. 2004, 20, 465–475. [Google Scholar] [CrossRef]
- Yahara, K.; Ohguri, T.; Yamaguchi, S.; Imada, H.; Narisada, H.; Ota, S.; Tomura, K.; Sakagami, M.; Fujimoto, N.; Korogi, Y. Definitive radiotherapy plus regional hyperthermia for high-risk and very high-risk prostate carcinoma: Thermal parameters correlated with biochemical relapse-free survival. Int. J. Hyperth. 2015, 31, 600–608. [Google Scholar] [CrossRef]
- Kok, H.P.; Wust, P.; Stauffer, P.R.; Bardati, F.; Van Rhoon, G.C.; Crezee, J. Current state of the art of regional hyperthermia treatment planning: A review. Radiat. Oncol. 2015, 10, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Canters, R.A.M.; Paulides, M.M.; Franckena, M.F.; Van Der Zee, J.; Van Rhoon, G.C. Implementation of treatment planning in the routine clinical procedure of regional hyperthermia treatment of cervical cancer: An overview and the Rotterdam experience. Int. J. Hyperth. 2012, 28, 570–581. [Google Scholar] [CrossRef] [PubMed]
- Kroeze, H.; Van De Kamer, J.B.; De Leeuw, A.A.C.; Kikuchi, M.; Lagendijk, J.J.W. Treatment planning for capacitive regional hyperthermia. Int. J. Hyperth. 2003, 19, 58–73. [Google Scholar] [CrossRef] [PubMed]
- Kok, H.P.; Navarro, F.; Strigari, L.; Cavagnaro, M.; Crezee, J. Locoregional hyperthermia of deep-seated tumours applied with capacitive and radiative systems: A simulation study. Int. J. Hyperth. 2018, 34, 714–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imada, H.; Nomoto, S.; Tomimatsu, A.; Kosaka, K.; Kusano, S.; Ostapenko, V.V.; Terashima, H. Importance of Patient Positioning in Hyperthermia for Deep-seated Intrathoracic Tumors Using an 8 MHz RF Capacitive Heating Device. Therm. Med. 1999, 15, 15–19. [Google Scholar] [CrossRef] [Green Version]
- Modeling for Device Design and Personalized Treatment Planning. Sim4Life by ZMT. 2014. Available online: http://www.zurichmedtech.com/applications/thermal-therapies/ (accessed on 27 January 2017).
- Pennes, H.H. Analysis of Tissue and Arterial Blood Temperatures in the Resting Human Forearm. J. Appl. Physiol. 1998, 85, 5–34. [Google Scholar] [CrossRef]
- Paulides, M.M.; Stauffer, P.R.; Neufeld, E.; Maccarini, P.F.; Kyriakou, A.; Canters, R.A.; Diederich, C.J.; Bakker, J.F.; Van Rhoon, G.C. Simulation techniques in hyperthermia treatment planning. Int. J. Hyperth. 2013, 29, 346–357. [Google Scholar] [CrossRef]
- Tomimatsu, A.; Kosaka, K.; Kusano, S.; Ostapenko, V.V.; Imada, H.; Nomoto, S.; Terashima, H. Refinement of Circulating Liquid of Overlay Bolus in Hyperthermia Using an 8MHz RF Capacitive Heating Device. Therm. Med. 1999, 15, 71–77. [Google Scholar] [CrossRef]
- Karasawa, K.; Muta, N.; Nakagawa, K.; Hasezawa, K.; Terahara, A.; Onogi, Y.; Sakata, K.-I.; Aoki, Y.; Sasaki, Y.; Akanuma, A. Thermoradiotherapy in the treatment of locally advanced nonsmall cell lung cancer. Int. J. Radiat. Oncol. 1994, 30, 1171–1177. [Google Scholar] [CrossRef]
- Kato, H.; Hyodo, K.; Akasaka, N.; Nishimura, K.; Kasai, T.; Uchida, N.; Sugimura, K. Optimization of bolus for capacitive type heating. Therm. Med. 1997, 13, 10–17. [Google Scholar] [CrossRef] [Green Version]
- Tomura, K.; Ohguri, T.; Mulder, H.T.; Murakami, M.; Nakahara, S.; Yahara, K.; Korogi, Y. The usefulness of mobile insulator sheets for the optimisation of deep heating area for regional hyperthermia using a capacitively coupled heating method: Phantom, simulation and clinical prospective studies. Int. J. Hyperth. 2017, 34, 1092–1103. [Google Scholar] [CrossRef] [Green Version]
- Ohguri, T.; Imada, H.; Yahara, K.; Morioka, T.; Nakano, K.; Terashima, H.; Korogi, Y. Radiotherapy With 8-MHz Radiofrequency-Capacitive Regional Hyperthermia for Stage III Non–Small-Cell Lung Cancer: The Radiofrequency-Output Power Correlates With the Intraesophageal Temperature and Clinical Outcomes. Int. J. Radiat. Oncol. 2009, 73, 128–135. [Google Scholar] [CrossRef]
- Ohguri, T.; Yahara, K.; Moon, S.D.; Yamaguchi, S.; Imada, H.; Terashima, H.; Korogi, Y. Deep regional hyperthermia for the whole thoracic region using 8 MHz radiofrequency-capacitive heating device: Relationship between the radiofrequency-output power and the intra-oesophageal temperature and predictive factors for a good heating in 59 patients. Int. J. Hyperth. 2011, 27, 20–26. [Google Scholar] [CrossRef]
- Crezee, J.; Bennis, M.; Gavazzi, S.; Stalpers, L.; Van Lier, A.; Kok, H.P. Development of electrical properties tomography for hyperthermia treatment planning. In Proceedings of the 2017 First IEEE MTT-S International Microwave Bio Conference (IMBIOC), Gothenburg, Sweden, 15–17 May 2017. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Materials | Electric Conductivity (S/m) | Relative Permittivity | Mass Density (kg/m3) |
|---|---|---|---|
| Muscle | 0.61 | 203 | 1090 |
| Fat | 0.05 | 33 | 911 |
| Bone | 0.04 | 43 | 1908 |
| Regular boluses | |||
| 5% NaCl at 10 °C | 6.31 | 82 | 1000 |
| Overlay boluses | |||
| 0.1% NaCl at 5 °C | 0.11 | 85 | 1000 |
| 0.5% NaCl at 5 °C | 0.57 | 85 | 1000 |
| 1% NaCl at 5 °C | 1.10 | 85 | 1000 |
| 5% NaCl at 5 °C | 5.58 | 84 | 1000 |
| IGC bolus | |||
| 5% NaCl at 10 °C | 6.31 | 82 | 1000 |
| Materials | Specific Heat Capacity (J/kg K) | Thermal Conductivity (W/m K) | Heat Generation Rate (W/kg) | Perfusion Rate (mL/min kg) |
|---|---|---|---|---|
| Muscle | 3421 | 0.49 | 0.91 | 36.7 |
| Fat | 2348 | 0.21 | 0.51 | 32.7 |
| Bone | 1312 | 0.32 | 0.15 | 10.0 |
| IGC bolus | 4180 | 6 | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ohguri, T.; Kuroda, K.; Yahara, K.; Nakahara, S.; Kakinouchi, S.; Itamura, H.; Morisaki, T.; Korogi, Y. Optimization of the Clinical Setting Using Numerical Simulations of the Electromagnetic Field in an Obese Patient Model for Deep Regional Hyperthermia of an 8 MHz Radiofrequency Capacitively Coupled Device in the Pelvis. Cancers 2021, 13, 979. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13050979
Ohguri T, Kuroda K, Yahara K, Nakahara S, Kakinouchi S, Itamura H, Morisaki T, Korogi Y. Optimization of the Clinical Setting Using Numerical Simulations of the Electromagnetic Field in an Obese Patient Model for Deep Regional Hyperthermia of an 8 MHz Radiofrequency Capacitively Coupled Device in the Pelvis. Cancers. 2021; 13(5):979. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13050979
Chicago/Turabian StyleOhguri, Takayuki, Kagayaki Kuroda, Katsuya Yahara, Sota Nakahara, Sho Kakinouchi, Hirohide Itamura, Takahiro Morisaki, and Yukunori Korogi. 2021. "Optimization of the Clinical Setting Using Numerical Simulations of the Electromagnetic Field in an Obese Patient Model for Deep Regional Hyperthermia of an 8 MHz Radiofrequency Capacitively Coupled Device in the Pelvis" Cancers 13, no. 5: 979. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13050979