
Clinical Indications for Treatment with Multi-Kinase Inhibitors in Patients with Radioiodine-Refractory Differentiated Thyroid Cancer


Abstract
:Simple Summary
Abstract
1. Introduction
2. Controversy over the Optimal Timing for Starting MKIs
3. Recommendation of Each Guideline for Starting MKIs
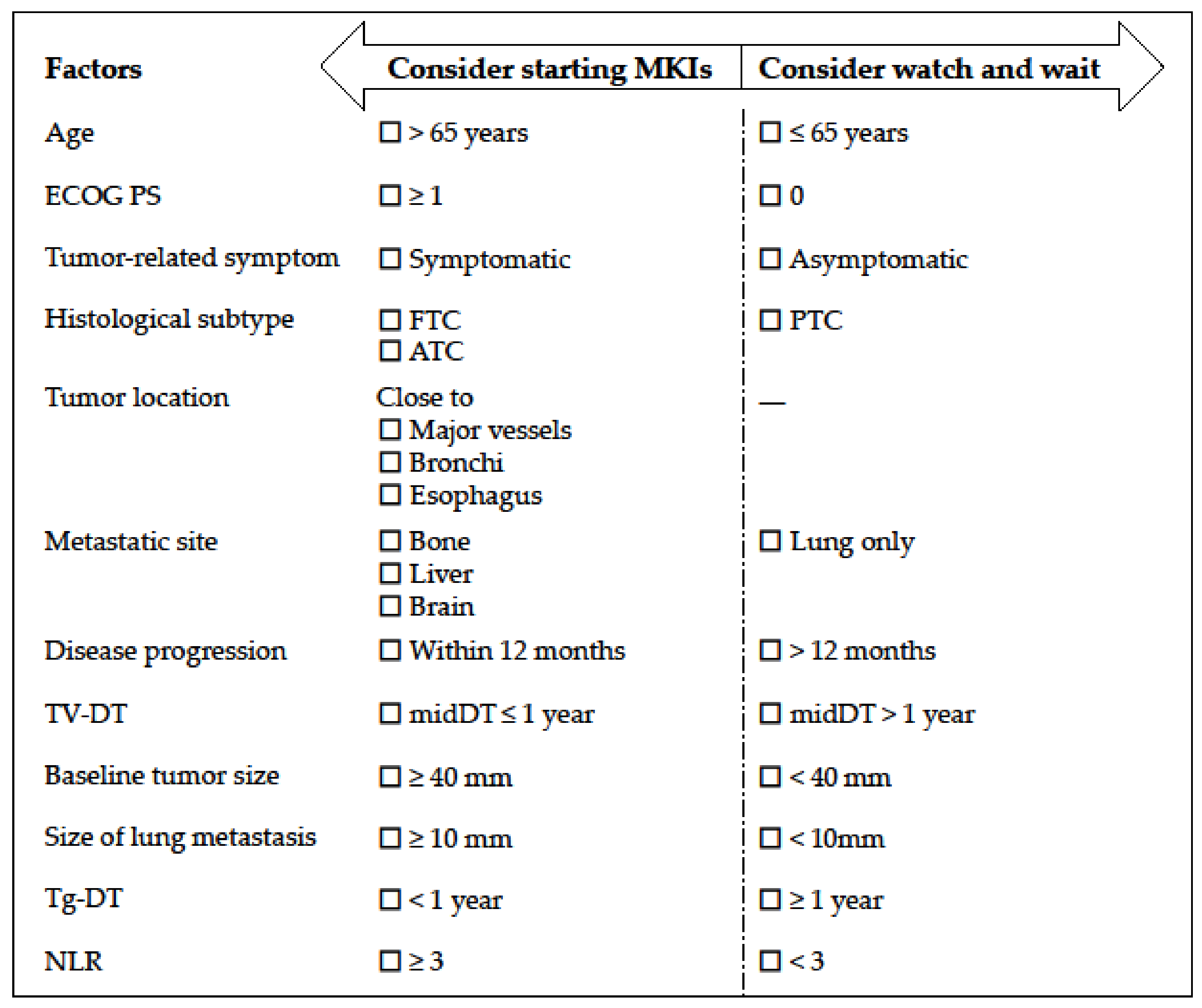
4. Possible Indications for Starting MKIs
4.1. Disease Progression
4.2. Age
4.3. Sex
4.4. Histological Subtypes
4.5. Tumor Location
4.6. Metastatic Sites
4.7. Thyroglobulin and Thyroglobulin Doubling Time
4.8. Tumor Volume Doubling Time
4.9. Tumor-Related Symptoms
4.10. Tumor Burden
4.11. Neutrophil-to-Lymphocyte Ratio
4.12. Genetic Landscape
5. Perspectives in the Era of Specific Treatment
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Antonelli, A.; La Motta, C. Novel therapeutic clues in thyroid carcinomas: The role of targeting cancer stem cells. Med. Res. Rev. 2017, 37, 1299–1317. [Google Scholar] [CrossRef] [PubMed]
- Global Burden of Disease Cancer Collaboration; Fitzmaurice, C.; Dicker, D.; Pain, A.; Hamavid, H.; Moradi-Lakeh, M.; MacIntyre, M.F.; Allen, C.; Hansen, G.; Woodbrook, R.; et al. The Global Burden of Cancer 2013. JAMA Oncol. 2015, 1, 505–527. [Google Scholar] [CrossRef] [PubMed]
- Hay, I.D.; Grant, C.S.; van Heerden, J.A.; Goellner, J.R.; Ebersold, J.R.; Bergstralh, E.J. Papillary thyroid microcarcinoma: A study of 535 cases observed in a 50-year period. Surgery 1992, 112, 1139–1147. [Google Scholar] [PubMed]
- Ringel, M.D.; Ladenson, P.W. Controversies in the follow-up and management of well-differentiated thyroid cancer. Endocr. Relat. Cancer 2004, 11, 97–116. [Google Scholar] [CrossRef] [Green Version]
- Noguchi, S.; Yamashita, H.; Murakami, N.; Nakayama, I.; Toda, M.; Kawamoto, H. Small carcinomas of the thyroid. A long-term follow-up of 867 patients. Arch. Surg. 1996, 131, 187–191. [Google Scholar] [CrossRef]
- Davies, L.; Welch, H.G. Increasing incidence of thyroid cancer in the United States, 1973–2002. JAMA 2006, 295, 2164–2167. [Google Scholar] [CrossRef] [Green Version]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Jonklaas, J.; Sarlis, N.J.; Litofsky, D.; Ain, K.B.; Bigos, S.T.; Brierley, J.D.; Cooper, D.S.; Haugen, B.R.; Ladenson, P.W.; Magner, J.; et al. Outcomes of patients with differentiated thyroid carcinoma following initial therapy. Thyroid 2006, 16, 1229–1242. [Google Scholar] [CrossRef]
- Sciuto, R.; Romano, L.; Rea, S.; Marandino, F.; Sperduti, I.; Maini, C.L. Natural history and clinical outcome of differentiated thyroid carcinoma: A retrospective analysis of 1503 patients treated at a single institution. Ann. Oncol. 2009, 20, 1728–1735. [Google Scholar] [CrossRef]
- Gruber, J.J.; Colevas, A.D. Differentiated thyroid cancer: Focus on emerging treatments for radioactive iodine-refractory patients. Oncologist 2015, 20, 113–126. [Google Scholar] [CrossRef] [Green Version]
- Mazzaferri, E.L.; Kloos, R.T. Clinical review 128: Current approaches to primary therapy for papillary and follicular thyroid cancer. J. Clin. Endocrinol. Metab. 2001, 86, 1447–1463. [Google Scholar] [CrossRef]
- Schlumberger, M.J.; Filetti, S.; Hay, I.D. Nontoxic goiter and thyroid neoplasia. In Williams’ Textbook of Endocrinology, 10th ed.; Larsen, R.P., Kronenberg, H.M., Melmed, S., Polonsky, K.S., Eds.; WB Saunders Company: Philadelphia, PA, USA, 2003; pp. 457–490. [Google Scholar]
- Maxon, H.R., 3rd; Smith, H.S. Radioiodine-131 in the diagnosis and treatment of metastatic well differentiated thyroid cancer. Endocrinol. Metab. Clin. N. Am. 1990, 19, 685–718. [Google Scholar] [CrossRef]
- Robbins, R.J.; Schlumberger, M.J. The evolving role of 131I for the treatment of differentiated thyroid carcinoma. J. Nucl. Med. 2005, 46 (Suppl. 1), 28S–37S. [Google Scholar]
- Durante, C.; Haddy, N.; Baudin, E.; Leboulleux, S.; Hartl, D.; Travagli, J.P.; Caillou, B.; Ricard, M.; Lumbroso, J.D.; De Vathaire, F.; et al. Long-term outcome of 444 patients with distant metastases from papillary and follicular thyroid carcinoma: Benefits and limits of radioiodine therapy. J. Clin. Endocrinol. Metab. 2006, 91, 2892–2899. [Google Scholar] [CrossRef]
- Durante, C.; Montesano, T.; Torlontano, M.; Attard, M.; Monzani, F.; Tumino, S.; Costante, G.; Meringolo, D.; Bruno, R.; Trulli, F.; et al. Papillary thyroid cancer: Time course of recurrences during postsurgery surveillance. J. Clin. Endocrinol. Metab. 2013, 98, 636–642. [Google Scholar] [CrossRef] [Green Version]
- D’Agostino, M.; Sponziello, M.; Puppin, C.; Celano, M.; Maggisano, V.; Baldan, F.; Biffoni, M.; Bulotta, S.; Durante, C.; Filetti, S.; et al. Different expression of TSH receptor and NIS genes in thyroid cancer: Role of epigenetics. J. Mol. Endocrinol. 2014, 52, 121–131. [Google Scholar] [CrossRef] [Green Version]
- Wilhelm, S.M.; Carter, C.; Tang, L.; Wilkie, D.; McNabola, A.; Rong, H.; Chen, C.; Zhang, X.; Vincent, P.; McHugh, M.; et al. BAY 43-9006 exhibits broad spectrum oral antitumor activity and targets the RAF/MEK/ERK pathway and receptor tyrosine kinases involved in tumor progression and angiogenesis. Cancer Res. 2004, 64, 7099–7109. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.S.; Adnane, J.; Trail, P.A.; Levy, J.; Henderson, A.; Xue, D.; Bortolon, E.; Ichetovkin, M.; Chen, C.; McNabola, A.; et al. Sorafenib (BAY 43-9006) inhibits tumor growth and vascularization and induces tumor apoptosis and hypoxia in RCC xenograft models. Cancer Chemother. Pharmacol. 2007, 59, 561–574. [Google Scholar] [CrossRef]
- Brose, M.S.; Nutting, C.M.; Jarzab, B.; Elisei, R.; Siena, S.; Bastholt, L.; de la Fouchardiere, C.; Pacini, F.; Paschke, R.; Shong, Y.K.; et al. Sorafenib in radioactive iodine-refractory, locally advanced or metastatic differentiated thyroid cancer: A randomised, double-blind, phase 3 trial. Lancet 2014, 384, 319–328. [Google Scholar] [CrossRef] [Green Version]
- Matsui, J.; Funahashi, Y.; Uenaka, T.; Watanabe, T.; Tsuruoka, A.; Asada, M. Multi-kinase inhibitor E7080 suppresses lymph node and lung metastases of human mammary breast tumor MDA-MB-231 via inhibition of vascular endothelial growth factor-receptor (VEGF-R) 2 and VEGF-R3 kinase. Clin. Cancer Res. 2008, 14, 5459–5465. [Google Scholar] [CrossRef] [Green Version]
- Matsui, J.; Yamamoto, Y.; Funahashi, Y.; Tsuruoka, A.; Watanabe, T.; Wakabayashi, T.; Uenaka, T.; Asada, M. E7080, a novel inhibitor that targets multiple kinases, has potent antitumor activities against stem cell factor producing human small cell lung cancer H146, based on angiogenesis inhibition. Int. J. Cancer 2008, 122, 664–671. [Google Scholar] [CrossRef]
- Okamoto, K.; Kodama, K.; Takase, K.; Sugi, N.H.; Yamamoto, Y.; Iwata, M.; Tsuruoka, A. Antitumor activities of the targeted multi-tyrosine kinase inhibitor lenvatinib (E7080) against RET gene fusion-driven tumor models. Cancer Lett. 2013, 340, 97–103. [Google Scholar] [CrossRef] [Green Version]
- Schlumberger, M.; Tahara, M.; Wirth, L.J.; Robinson, B.; Brose, M.S.; Elisei, R.; Habra, M.A.; Newbold, K.; Shah, M.H.; Hoff, A.O.; et al. Lenvatinib versus placebo in radioiodine-refractory thyroid cancer. N. Engl. J. Med. 2015, 372, 621–630. [Google Scholar] [CrossRef] [Green Version]
- NCCN Clinical Practice Guidelines in Oncology, Thyroid Carcinoma Version 3. 2020. Available online: https://www.nccn.org/professionals/physician_gls/pdf/thyroid.pdf (accessed on 11 March 2021).
- Kim, H.; Park, S.Y.; Jung, J.; Kim, J.H.; Hahn, S.Y.; Shin, J.H.; Oh, Y.L.; Chung, M.K.; Kim, H.I.; Kim, S.W.; et al. Improved survival after early detection of asymptomatic distant metastasis in patients with thyroid cancer. Sci. Rep. 2019, 9, 18745. [Google Scholar] [CrossRef]
- Schlumberger, M.; Jarzab, B.; Elisei, R.; Siena, S.; Bastholt, L.; de la Fouchardiere, C.; Pacini, F.; Paschke, R.; Worden, F.; Bockisch, A.; et al. Phase III randomized, double-blinded, placebo controlled trial of sorafenib in locally advanced or metastatic patients with radioactive iodine (RAI)-refractory differentiated thyroid cancer (DTC)—Exploratory analyses of patientreported outcomes. In Proceedings of the 83rd Annual Meeting of the American Thyroid Association, San Juan, Puerto Rico, 16–20 October 2013. [Google Scholar]
- Nervo, A.; Ragni, A.; Piovesan, A.; Marica, V.; Migliore, E.; Gallo, M.; Arvat, E. Quality of life during treatment with lenvatinib for thyroid cancer: The patients’ perspective beyond the medical evaluation. Eur. Thyroid J. 2021, 10, 65–71. [Google Scholar]
- Giani, C.; Valerio, L.; Bongiovanni, A.; Durante, C.; Grani, G.; Ibrahim, T.; Mariotti, S.; Massa, M.; Pani, F.; Pellegriti, G.; et al. Safety and quality-of-life data from an Italian expanded access program of lenvatinib for treatment of thyroid cancer. Thyroid 2021, 31, 224–232. [Google Scholar] [CrossRef]
- Dadu, R.; Cabanillas, M.E. Optimizing therapy for radioactive iodine-refractory differentiated thyroid cancer: Current state of the art and future directions. Minerva Endocrinol. 2012, 37, 335–356. [Google Scholar]
- Schutz, F.A.; Je, Y.; Richards, C.J.; Choueiri, T.K. Meta-analysis of randomized controlled trials for the incidence and risk of treatment-related mortality in patients with cancer treated with vascular endothelial growth factor tyrosine kinase inhibitors. J. Clin. Oncol. 2012, 30, 871–877. [Google Scholar] [CrossRef]
- Zettinig, G.; Fueger, B.J.; Passler, C.; Kaserer, K.; Pirich, C.; Dudczak, R.; Niederle, B. Long-term follow-up of patients with bone metastases from differentiated thyroid carcinoma—Surgery or conventional therapy? Clin. Endocrinol. 2002, 56, 377–382. [Google Scholar] [CrossRef]
- Chiu, A.C.; Delpassand, E.S.; Sherman, S.I. Prognosis and treatment of brain metastases in thyroid carcinoma. J. Clin. Endocrinol. Metab. 1997, 82, 3637–3642. [Google Scholar] [CrossRef]
- Henriques de Figueiredo, B.; Godbert, Y.; Soubeyran, I.; Carrat, X.; Lagarde, P.; Cazeau, A.L.; Italiano, A.; Sargos, P.; Kantor, G.; Loiseau, H.; et al. Brain metastases from thyroid carcinoma: A retrospective study of 21 patients. Thyroid 2014, 24, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filetti, S.; Durante, C.; Hartl, D.; Leboulleux, S.; Locati, L.D.; Newbold, K.; Papotti, M.G.; Berruti, A.; ESMO Guidelines Committee. Thyroid cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann. Oncol. 2019, 30, 1856–1883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fugazzola, L.; Elisei, R.; Fuhrer, D.; Jarzab, B.; Leboulleux, S.; Newbold, K.; Smit, J. 2019 European Thyroid Association Guidelines for the treatment and follow-up of advanced radioiodine-refractory thyroid cancer. Eur. Thyroid J. 2019, 8, 227–245. [Google Scholar] [CrossRef]
- Ito, Y.; Onoda, N.; Okamoto, T. The revised clinical practice guidelines on the management of thyroid tumors by the Japan Associations of Endocrine Surgeons: Core questions and recommendations for treatments of thyroid cancer. Endocr. J. 2020, 67, 669–717. [Google Scholar] [CrossRef] [Green Version]
- Gild, M.L.; Tsang, V.H.M.; Clifton-Bligh, R.J.; Robinson, B.G. Multikinase inhibitors in thyroid cancer: Timing of targeted therapy. Nat. Rev. Endocrinol. 2021, 17, 225–234. [Google Scholar] [CrossRef]
- Brose, M.S.; Smit, J.; Lin, C.C.; Pitoia, F.; Fellous, M.; DeSanctis, Y.; Schlumberger, M.; Tori, M.; Sugitani, I. Timing of multikinase inhibitor initiation in differentiated thyroid cancer. Endocr. Relat. Cancer 2017, 24, 237–242. [Google Scholar] [CrossRef] [Green Version]
- Brose, M.S.; Smit, J.; Lin, C.C.; Tori, M.; Bowels, D.W.; Worden, F.; Shen, D.H.; Huang, S.; Alevizaki, M.; Peeters, R.P.; et al. Final analysis of RIFTOS MKI, a global, non-interventional study assessing the use of multikinase inhibitors (MKIs) for the treatment of patients with asymptomatic radioactive iodine-refractory differentiated thyroid cancer (RAI-R DTC). Ann. Oncol. 2020, 31 (Suppl 4), S1087. [Google Scholar] [CrossRef]
- Brose, M.S.; Worden, F.P.; Newbold, K.L.; Guo, M.; Hurria, A. Effect of age on the efficacy and safety of lenvatinib in radioiodine-refractory differentiated thyroid cancer in the phase III SELECT trial. J. Clin. Oncol. 2017, 35, 2692–2699. [Google Scholar] [CrossRef]
- Gianoukakis, A.G.; Dutcus, C.E.; Batty, N.; Guo, M.; Baig, M. Prolonged duration of response in lenvatinib responders with thyroid cancer. Endocr. Relat. Cancer 2018, 25, 699–704. [Google Scholar] [CrossRef]
- Brose, M.S.; Schlumbeger, M.; Jeffers, M.; Kappeler, C.; Meinhardt, G.; Peña, C.E.A. Analysis of biomarkers and association with clinical outcomes in patients with differentiated thyroid cancer: Subanalysis of the sorafenib phase III DECISION trial. Clin. Cancer Res. 2019, 25, 7370–7380. [Google Scholar] [CrossRef] [Green Version]
- Tahara, M.; Schlumberger, M.; Elisei, R.; Habra, M.A.; Kiyota, N.; Paschke, R.; Dutcus, C.E.; Hihara, T.; McGrath, S.; Matijevic, M.; et al. Exploratory analysis of biomarkers associated with clinical outcomes from the study of lenvatinib in differentiated cancer of the thyroid. Eur. J. Cancer 2017, 75, 213–221. [Google Scholar] [CrossRef] [Green Version]
- Sabra, M.M.; Sherman, E.; Tuttle, R.M. Prolongation of tumour volume doubling time (midDT) is associated with improvement in disease-specific survival in patients with rapidly progressive radioactive iodine refractory differentiated thyroid cancer selected for molecular targeted therapy. Clin. Endocrinol. 2019, 90, 617–622. [Google Scholar] [CrossRef]
- Kim, M.J.; Kim, S.M.; Lee, E.K.; Hwangbo, Y.; Lee, Y.J.; Cho, S.W.; Park, D.J.; Lee, Y.; Park, Y.J. Tumor doubling time predicts response to sorafenib in radioactive iodine-refractory differentiated thyroid cancer. Endocr. J. 2019, 66, 597–604. [Google Scholar] [CrossRef] [Green Version]
- Schlumberger, M.; Elisei, R.; Pacini, F.; Jarzab, B.; Giannetta, L.; Bastholt, L.; De la Fouchardiere, C.; Paschke, R.; Worden, F.; Shong, Y.; et al. Prognostic and predictive factors correlated with treatment outcomes for radioactive iodine-refractory differentiated thyroid cancer (RAI-rDTC) patients receiving sorafenib or placebo in the phase III DECISION trial. Thyroid 2014, 24 (Suppl. 1), A–6. [Google Scholar]
- Suzuki, C.; Kiyota, N.; Imamura, Y.; Goto, H.; Suto, H.; Chayahara, N.; Toyoda, M.; Ito, Y.; Miya, A.; Miyauchi, A.; et al. Exploratory analysis of prognostic factors for lenvatinib in radioiodine-refractory differentiated thyroid cancer. Head Neck 2019, 41, 3023–3032. [Google Scholar] [CrossRef]
- Haddad, R.I.; Schlumberger, M.; Wirth, L.J.; Sherman, E.J.; Shah, M.H.; Robinson, B.; Dutcus, C.E.; Teng, A.; Gianoukakis, A.G.; Sherman, S.I. Incidence and timing of common adverse events in Lenvatinib-treated patients from the SELECT trial and their association with survival outcomes. Endocrine 2017, 56, 121–128. [Google Scholar] [CrossRef] [Green Version]
- Kiyota, N.; Tahara, M.; Robinson, B.; Schlumberger, M.; Sherman, S.; Leboulleux, S.; Lee, E.K.; Suzuki, T.; Ren, M.; Fushimi, K.; et al. Impact of baseline tumor size on overall survival in patients with RR-DTC treated with lenvatinib (SELECT). In Proceedings of the 2021 the Japanese Society of Medical Oncology Annual Meeting, Virtual Congress, 18–21 February 2021. [Google Scholar]
- Fukuda, N.; Toda, K.; Ohmoto, A.; Wang, X.; Hayashi, N.; Urasaki, T.; Sato, Y.; Nakano, K.; Ono, M.; Tomomatsu, J.; et al. Baseline tumour size as a prognostic factor for radioiodine-refractory differentiated thyroid cancer treated with lenvatinib. Anticancer Res. 2021, 41, 1683–1691. [Google Scholar] [CrossRef]
- Tahara, M.; Kiyota, N.; Hoff, A.O.; Badiu, C.; Owonikoko, T.K.; Dutcus, C.E.; Suzuki, T.; Ren, M.; Wirth, L.J. Impact of lung metastases on overall survival in the phase 3 SELECT study of lenvatinib in patients with radioiodine-refractory differentiated thyroid cancer. Eur. J. Cancer 2021, 147, 51–57. [Google Scholar] [CrossRef]
- Fukuda, N.; Wang, X.; Ohmoto, A.; Urasaki, T.; Sato, Y.; Nakano, K.; Nishizawa, M.; Yunokawa, M.; Ono, M.; Tomomatsu, J.; et al. Sequential analysis of neutrophil-to-lymphocyte ratio for differentiated thyroid cancer patients treated with lenvatinib. In Vivo 2020, 34, 709–714. [Google Scholar] [CrossRef] [Green Version]
- Taylor, M.H.; Takahashi, S.; Capdevila, J.; Tahara, M.; Leboulleux, S.; Kiyota, N.; Dutcus, C.E.; Xie, R.; Robinson, B.; Sherman, S.I.; et al. Correlation of performance status and neutrophil-lymphocyte ratio with efficacy in radioiodine-refractory differentiated thyroid cancer treated with lenvatinib. Thyroid 2021. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Tahara, M. Management of recurrent or metastatic thyroid cancer. ESMO Open 2018, 3 (Suppl. 1), e000359. [Google Scholar] [CrossRef] [Green Version]
- Orosco, R.K.; Hussain, T.; Brumund, K.T.; Oh, D.K.; Chang, D.C.; Bouvet, M. Analysis of age and disease status as predictors of thyroid cancer-specific mortality using the Surveillance, Epidemiology, and End Results database. Thyroid 2015, 25, 125–132. [Google Scholar] [CrossRef] [Green Version]
- Oyer, S.L.; Smith, V.A.; Lentsch, E.J. Reevaluating the prognostic significance of age in differentiated thyroid cancer. Otolaryngol. Head Neck Surg. 2012, 147, 221–226. [Google Scholar] [CrossRef]
- Gilliland, F.D.; Hunt, W.C.; Morris, D.M.; Key, C.R. Prognostic factors for thyroid carcinoma. A population-based study of 15,698 cases from the Surveillance, Epidemiology and End Results (SEER) program 1973–1991. Cancer 1997, 79, 564–573. [Google Scholar] [CrossRef]
- Siegel, R.; Naishadham, D.; Jemal, A. Cancer statistics, 2012. CA Cancer J. Clin. 2012, 62, 10–29. [Google Scholar] [CrossRef] [Green Version]
- Rahbari, R.; Zhang, L.; Kebebew, E. Thyroid cancer gender disparity. Future Oncol. 2010, 6, 1771–1779. [Google Scholar] [CrossRef] [Green Version]
- Kilfoy, B.A.; Devesa, S.S.; Ward, M.H.; Zhang, Y.; Rosenberg, P.S.; Holford, T.R.; Anderson, W.F. Gender is an age-specific effect modifier for papillary cancers of the thyroid gland. Cancer Epidemiol. Biomark. Prev. 2009, 18, 1092–1100. [Google Scholar] [CrossRef] [Green Version]
- Zahedi, A.; Bondaz, L.; Rajaraman, M.; Leslie, W.D.; Jefford, C.; Young, J.E.; Pathak, K.A.; Bureau, Y.; Rachinsky, I.; Badreddine, M.; et al. Risk for thyroid cancer recurrence is higher in men than in women independent of disease stage at presentation. Thyroid 2020, 30, 871–877. [Google Scholar] [CrossRef]
- Chow, S.M.; Law, S.C.; Au, S.K.; Leung, T.W.; Chan, P.T.; Mendenhall, W.M.; Lau, W.H. Differentiated thyroid carcinoma: Comparison between papillary and follicular carcinoma in a single institute. Head Neck 2002, 24, 670–677. [Google Scholar] [CrossRef] [PubMed]
- Madani, A.; Jozaghi, Y.; Tabah, R.; How, J.; Mitmaker, E. Rare metastases of well-differentiated thyroid cancers: A systematic review. Ann. Surg. Oncol. 2015, 22, 460–466. [Google Scholar] [CrossRef] [PubMed]
- Hundahl, S.A.; Fleming, I.D.; Fremgen, A.M.; Menck, H.R. A National Cancer Data Base report on 53,856 cases of thyroid carcinoma treated in the U.S., 1985–1995. Cancer 1998, 83, 2638–2648. [Google Scholar] [CrossRef]
- Elisei, R.; Schlumberger, M.; Tahara, M.; Robinson, B.; Brose, M.; Dutcus, C.; Zhu, J.; Newbold, K.; Kiyota, N.; Kim, S.-B.; et al. Subgroup analysis according to differentiated thyroid cancer histology in the phase 3 (SELECT) trial of lenvatinib. Oncol. Res. Treat. 2015, 38 (Suppl. 5), 25–26. [Google Scholar]
- Blevins, D.P.; Dadu, R.; Hu, M.; Baik, C.; Balachandran, D.; Ross, W.; Gunn, B.; Cabanillas, M.E. Aerodigestive fistula formation as a rare side effect of antiangiogenic tyrosine kinase inhibitor therapy for thyroid cancer. Thyroid 2014, 24, 918–922. [Google Scholar] [CrossRef] [Green Version]
- Staub, Y.; Nishiyama, A.; Suga, Y.; Fujita, M.; Matsushita, R.; Yano, S. Clinical characteristics associated with lenvatinib-induced fistula and tumor-related bleeding in patients with thyroid cancer. Anticancer Res. 2019, 39, 3871–3878. [Google Scholar] [CrossRef]
- Clark, J.R.; Lai, P.; Hall, F.; Borglund, A.; Eski, S.; Freeman, J.L. Variables predicting distant metastases in thyroid cancer. Laryngoscope 2005, 115, 661–667. [Google Scholar] [CrossRef]
- Benbassat, C.A.; Mechlis-Frish, S.; Hirsch, D. Clinicopathological characteristics and long-term outcome in patients with distant metastases from differentiated thyroid cancer. World J. Surg. 2006, 30, 1088–1095. [Google Scholar] [CrossRef]
- Schneider, T.C.; Abdulrahman, R.M.; Corssmit, E.P.; Morreau, H.; Smit, J.W.; Kapiteijn, E. Long-term analysis of the efficacy and tolerability of sorafenib in advanced radio-iodine refractory differentiated thyroid carcinoma: Final results of a phase II trial. Eur. J. Endocrinol. 2012, 167, 643–650. [Google Scholar] [CrossRef] [Green Version]
- Robinson, B.; Schlumberger, M.; Wirth, L.J.; Dutcus, C.E.; Song, J.; Taylor, M.H.; Kim, S.B.; Krzyzanowska, M.K.; Capdevila, J.; Sherman, S.I.; et al. Characterization of tumor size changes over time from the phase 3 study of lenvatinib in thyroid cancer. J. Clin. Endocrinol. Metab. 2016, 101, 4103–4109. [Google Scholar] [CrossRef] [Green Version]
- Citterio, C.E.; Targovnik, H.M.; Arvan, P. The role of thyroglobulin in thyroid hormonogenesis. Nat. Rev. Endocrinol. 2019, 15, 323–338. [Google Scholar] [CrossRef]
- Ringel, M.D.; Nabhan, F. Approach to follow-up of the patient with differentiated thyroid cancer and positive anti-thyroglobulin antibodies. J. Clin. Endocrinol. Metab. 2013, 98, 3104–3110. [Google Scholar] [CrossRef] [Green Version]
- Gibelli, B.; Tredici, P.; De Cicco, C.; Bodei, L.; Sandri, M.T.; Renne, G.; Bruschini, R.; Tradati, N. Preoperative determination of serum thyroglobulin to identify patients with differentiated thyroid cancer who may present recurrence without increased thyroglobulin. Acta Otorhinolaryngol. Ital. 2005, 25, 94–99. [Google Scholar]
- Frilling, A.; Görges, R.; Tecklenborg, K.; Gassmann, P.; Bockhorn, M.; Clausen, M.; Broelsch, C.E. Value of preoperative diagnostic modalities in patients with recurrent thyroid carcinoma. Surgery 2000, 128, 1067–1074. [Google Scholar] [CrossRef]
- Baloch, Z.; Carayon, P.; Conte-Devolx, B.; Demers, L.M.; Feldt-Rasmussen, U.; Henry, J.F.; LiVosli, V.A.; Niccoli-Sire, P.; John, R.; Ruf, J.; et al. Laboratory medicine practice guidelines. Laboratory support for the diagnosis and monitoring of thyroid disease. Thyroid 2003, 13, 3–126. [Google Scholar]
- Spencer, C.A.; Takeuchi, M.; Kazarosyan, M.; Wang, C.C.; Guttler, R.B.; Singer, P.A.; Fatemi, S.; LoPresti, J.S.; Nicoloff, J.T. Serum thyroglobulin autoantibodies: Prevalence, influence on serum thyroglobulin measurement, and prognostic significance in patients with differentiated thyroid carcinoma. J. Clin. Endocrinol. Metab. 1998, 83, 1121–1127. [Google Scholar] [CrossRef]
- Marotta, V.; Ramundo, V.; Camera, L.; Del Prete, M.; Fonti, R.; Esposito, R.; Palmieri, G.; Salvatore, M.; Vitale, M.; Colao, A.; et al. Sorafenib in advanced iodine-refractory differentiated thyroid cancer: Efficacy, safety and exploratory analysis of role of serum thyroglobulin and FDG-PET. Clin. Endocrinol. 2013, 78, 760–767. [Google Scholar] [CrossRef] [Green Version]
- Werner, R.A.; Lückerath, K.; Schmid, J.S.; Higuchi, T.; Kreissl, M.C.; Grelle, I.; Reiners, C.; Buck, A.K.; Lapa, C. Thyroglobulin fluctuations in patients with iodine-refractory differentiated thyroid carcinoma on lenvatinib treatment—Initial experience. Sci. Rep. 2016, 6, 28081. [Google Scholar] [CrossRef] [Green Version]
- Bachelot, A.; Cailleux, A.F.; Klain, M.; Baudin, E.; Ricard, M.; Bellon, N.; Caillou, B.; Travagli, J.P.; Schlumberger, M. Relationship between tumor burden and serum thyroglobulin level in patients with papillary and follicular thyroid carcinoma. Thyroid 2002, 12, 707–711. [Google Scholar] [CrossRef]
- Miyauchi, A.; Kudo, T.; Miya, A.; Kobayashi, K.; Ito, Y.; Takamura, Y.; Higashiyama, T.; Fukushima, M.; Kihara, M.; Inoue, H.; et al. Prognostic impact of serum thyroglobulin doubling-time under thyrotropin suppression in patients with papillary thyroid carcinoma who underwent total thyroidectomy. Thyroid 2011, 21, 707–716. [Google Scholar] [CrossRef]
- Berdelou, A.; Borget, I.; Godbert, Y.; Nguyen, T.; Garcia, M.E.; Chougnet, C.N.; Ferru, A.; Buffet, C.; Chabre, O.; Huillard, O.; et al. Lenvatinib for the treatment of radioiodine-refractory thyroid cancer in real-life practice. Thyroid 2018, 28, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Masaki, C.; Sugino, K.; Saito, N.; Akaishi, J.; Hames, K.Y.; Tomoda, C.; Suzuki, A.; Matsuzu, K.; Uruno, T.; Ohkuwa, K.; et al. Efficacy and limitations of lenvatinib therapy for radioiodine-refractory differentiated thyroid cancer: Real-world experiences. Thyroid 2020, 30, 214–221. [Google Scholar] [CrossRef]
- Fukuda, N.; Toda, K.; Wang, X.; Ohmoto, A.; Hayashi, N.; Urasaki, T.; Sato, Y.; Nakano, K.; Ono, M.; Tomomatsu, J.; et al. Prognostic significance of 8 weeks’ relative dose intensity of lenvatinib in treatment of radioiodine-refractory differentiated thyroid cancer patients. Endocr. J. 2021. [Google Scholar] [CrossRef] [PubMed]
- Doubling Time, Doubling Rate & Progression Calculator. Available online: https://www.kuma-h.or.jp/english/about/doubling-time-progression-calculator/ (accessed on 13 March 2021).
- Sabra, M.M.; Sherman, E.J.; Tuttle, R.M. Tumor volume doubling time of pulmonary metastases predicts overall survival and can guide the initiation of multikinase inhibitor therapy in patients with metastatic, follicular cell-derived thyroid carcinoma. Cancer 2017, 123, 2955–2964. [Google Scholar] [CrossRef] [PubMed]
- Tuttle, R.M.; Brose, M.S.; Grande, E.; Kim, S.W.; Tahara, M.; Sabra, M.M. Novel concepts for initiating multitargeted kinase inhibitors in radioactive iodine refractory differentiated thyroid cancer. Best Pract. Res. Clin. Endocrinol. Metab. 2017, 31, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Kish, J.K.; Chatterjee, D.; Wan, Y.; Yu, H.T.; Liassou, D.; Feinberg, B.A. Lenvatinib and subsequent therapy for radioactive iodine-refractory differentiated thyroid cancer: A real-world study of clinical effectiveness in the United States. Adv. Ther. 2020, 37, 2841–2852. [Google Scholar] [CrossRef] [PubMed]
- Locati, L.D.; Piovesan, A.; Durante, C.; Bregni, M.; Castagna, M.G.; Zovato, S.; Giusti, M.; Ibrahim, T.; Puxeddu, E.; Fedele, G.; et al. Real-world efficacy and safety of lenvatinib: Data from a compassionate use in the treatment of radioactive iodine-refractory differentiated thyroid cancer patients in Italy. Eur. J. Cancer 2019, 118, 35–40. [Google Scholar] [CrossRef]
- Tran, B.; Roshan, D.; Abraham, E.; Wang, L.; Garibotto, N.; Wykes, J.; Campbell, P.; Ebrahimi, A. The prognostic impact of tumor size in papillary thyroid carcinoma is modified by age. Thyroid 2018, 28, 991–996. [Google Scholar] [CrossRef]
- Ito, Y.; Kihara, M.; Takamura, Y.; Kobayashi, K.; Miya, A.; Hirokawa, M.; Miyauchi, A. Prognosis and prognostic factors of papillary thyroid carcinoma in patients under 20 years. Endocr. J. 2012, 59, 539–545. [Google Scholar] [CrossRef] [Green Version]
- Jing, X.; Yang, F.; Shao, C.; Wei, K.; Xie, M.; Shen, H.; Shu, Y. Role of hypoxia in cancer therapy by regulating the tumor microenvironment. Mol. Cancer 2019, 18, 157. [Google Scholar] [CrossRef] [Green Version]
- Trédan, O.; Galmarini, C.M.; Patel, K.; Tannock, I.F. Drug resistance and the solid tumor microenvironment. J. Natl. Cancer Inst. 2007, 99, 1441–1454. [Google Scholar] [CrossRef] [Green Version]
- Hartwich, J.; Orr, W.S.; Ng, C.Y.; Spence, Y.; Morton, C.; Davidoff, A.M. HIF-1α activation mediates resistance to anti-angiogenic therapy in neuroblastoma xenografts. J. Pediatr. Surg. 2013, 48, 39–46. [Google Scholar] [CrossRef] [Green Version]
- Hu, Y.L.; Jahangiri, A.; De Lay, M.; Aghi, M.K. Hypoxia-induced tumor cell autophagy mediates resistance to anti-angiogenic therapy. Autophagy 2012, 8, 979–981. [Google Scholar] [CrossRef] [Green Version]
- Ahmadi, M.; Ahmadihosseini, Z.; Allison, S.J.; Begum, S.; Rockley, K.; Sadiq, M.; Chintamaneni, S.; Lokwani, R.; Hughes, N.; Phillips, R.M. Hypoxia modulates the activity of a series of clinically approved tyrosine kinase inhibitors. Br. J. Pharmacol. 2014, 171, 224–236. [Google Scholar] [CrossRef]
- Coussens, L.M.; Werb, Z. Inflammation and cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef]
- Templeton, A.J.; McNamara, M.G.; Šeruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocaña, A.; Leibowitz-Amit, R.; Sonpavde, G.; Knox, J.J.; Tran, B.; et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2014, 106, dju124. [Google Scholar] [CrossRef] [Green Version]
- Manatakis, D.K.; Tseleni-Balafouta, S.; Balalis, D.; Soulou, V.N.; Korkolis, D.P.; Sakorafas, G.H.; Plataniotis, G.; Gontikakis, E. Association of baseline neutrophil-to-lymphocyte ratio with clinicopathological characteristics of papillary thyroid carcinoma. Int. J. Endocrinol. 2017, 2017, 8471235. [Google Scholar] [CrossRef]
- Cho, J.S.; Park, M.H.; Ryu, Y.J.; Yoon, J.H. The neutrophil to lymphocyte ratio can discriminate anaplastic thyroid cancer against poorly or well differentiated cancer. Ann. Surg. Treat. Res. 2015, 88, 187–192. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, S.; Kiyota, N.; Yamazaki, T.; Chayahara, N.; Nakano, K.; Inagaki, L.; Toda, K.; Enokida, T.; Minami, H.; Imamura, Y.; et al. A Phase II study of the safety and efficacy of lenvatinib in patients with advanced thyroid cancer. Future Oncol. 2019, 15, 717–726. [Google Scholar] [CrossRef] [Green Version]
- Namba, H.; Nakashima, M.; Hayashi, T.; Hayashida, N.; Maeda, S.; Rogounovitch, T.I.; Ohtsuru, A.; Saenko, V.A.; Kanematsu, T.; Yamashita, S. Clinical implication of hot spot BRAF mutation, V599E, in papillary thyroid cancers. J. Clin. Endocrinol. Metab. 2003, 88, 4393–4397. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.H.; Kang, D.W.; Kim, S.H.; Seong, I.O.; Kang, D.Y. Mutations of the BRAF gene in papillary thyroid carcinoma in a Korean population. Yonsei Med. J. 2004, 45, 818–821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xing, M. BRAF mutation in thyroid cancer. Endocr. Relat. Cancer 2005, 12, 245–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Musholt, T.J.; Musholt, P.B.; Khaladj, N.; Schulz, D.; Scheumann, G.F.; Klempnauer, J. Prognostic significance of RET and NTRK1 rearrangements in sporadic papillary thyroid carcinoma. Surgery 2000, 128, 984–993. [Google Scholar] [CrossRef] [PubMed]
- Sugg, S.L.; Ezzat, S.; Zheng, L.; Freeman, J.L.; Rosen, I.B.; Asa, S.L. Oncogene profile of papillary thyroid carcinoma. Surgery 1999, 125, 46–52. [Google Scholar] [CrossRef]
- Lam, A.K.; Montone, K.T.; Nolan, K.A.; Livolsi, V.A. Ret oncogene activation in papillary thyroid carcinoma: Prevalence and implication on the histological parameters. Hum. Pathol. 1998, 29, 565–568. [Google Scholar] [CrossRef]
- Nakazawa, T.; Kondo, T.; Kobayashi, Y.; Takamura, N.; Murata, S.; Kameyama, K.; Muramatsu, A.; Ito, K.; Kobayashi, M.; Katoh, R. RET gene rearrangements (RET/PTC1 and RET/PTC3) in papillary thyroid carcinomas from an iodine-rich country (Japan). Cancer 2005, 104, 943–951. [Google Scholar] [CrossRef]
- Lemoine, N.R.; Mayall, E.S.; Wyllie, F.S.; Williams, E.D.; Goyns, M.; Stringer, B.; Wynford-Thomas, D. High frequency of ras oncogene activation in all stages of human thyroid tumorigenesis. Oncogene 1989, 4, 159–164. [Google Scholar]
- Namba, H.; Rubin, S.A.; Fagin, J.A. Point mutations of ras oncogenes are an early event in thyroid tumorigenesis. Mol. Endocrinol. 1990, 4, 1474–1479. [Google Scholar] [CrossRef] [Green Version]
- Rabes, H.M.; Demidchik, E.P.; Sidorow, J.D.; Lengfelder, E.; Beimfohr, C.; Hoelzel, D.; Klugbauer, S. Pattern of radiation-induced RET and NTRK1 rearrangements in 191 post-chernobyl papillary thyroid carcinomas: Biological, phenotypic, and clinical implications. Clin. Cancer Res. 2000, 6, 1093–1103. [Google Scholar]
- Basolo, F.; Pisaturo, F.; Pollina, L.E.; Fontanini, G.; Elisei, R.; Molinaro, E.; Iacconi, P.; Miccoli, P.; Pacini, F. N-ras mutation in poorly differentiated thyroid carcinomas: Correlation with bone metastases and inverse correlation to thyroglobulin expression. Thyroid 2000, 10, 19–23. [Google Scholar] [CrossRef]
- Brose, M.S.; Cabanillas, M.E.; Cohen, E.E.; Wirth, L.J.; Riehl, T.; Yue, H.; Sherman, S.I.; Sherman, E.J. Vemurafenib in patients with BRAF(V600E)-positive metastatic or unresectable papillary thyroid cancer refractory to radioactive iodine: A non-randomised, multicentre, open-label, phase 2 trial. Lancet Oncol. 2016, 17, 1272–1282. [Google Scholar] [CrossRef] [Green Version]
- Wirth, L.J.; Sherman, E.; Robinson, B.; Solomon, B.; Kang, H.; Lorch, J.; Worden, F.; Brose, M.; Patel, J.; Leboulleux, S.; et al. Efficacy of selpercatinib in RET-altered thyroid cancers. N. Engl. J. Med. 2020, 383, 825–835. [Google Scholar] [CrossRef]
- Drilon, A.; Laetsch, T.W.; Kummar, S.; DuBois, S.G.; Lassen, U.N.; Demetri, G.D.; Nathenson, M.; Doebele, R.C.; Farago, A.F.; Pappo, A.S.; et al. Efficacy of larotrectinib in TRK fusion-positive cancers in adults and children. N. Engl. J. Med. 2018, 378, 731–739. [Google Scholar] [CrossRef]
- Welsh, S.J.; Corrie, P.G. Management of BRAF and MEK inhibitor toxicities in patients with metastatic melanoma. Ther. Adv. Med. Oncol. 2015, 7, 122–136. [Google Scholar] [CrossRef] [Green Version]
- A Study of Selpercatinib (LY3527723) in Participants with RET-Mutant Medullary Thyroid Cancer (LIBRETTO-531). Available online: https://clinicaltrials.gov/ct2/show/NCT04211337 (accessed on 5 May 2021).


{kind=link}
| Trial Name | Decision [20] | Select [24] |
|---|---|---|
| Study design | Randomized controlled trial | Randomized controlled trial |
| No. of patients | 417 (Sorafenib 207, placebo 210) | 392 (Lenvatinib 261, placebo 131) |
| Eligibility criteria | Age ≥ 18 years Locally advanced or metastatic DTC Progression within 14 months RAI-refractory TSH < 0.5 mIU/L | Age ≥ 18 years Locally advanced or metastatic DTC Progression within 13 months RAI-refractory |
| Experimental arm | Sorafenib | Lenvatinib |
| Control arm | Placebo | Placebo |
| Primary endpoint | Progression-free survival | Progression-free survival |
| Patients’ characteristics | Male 52%, Female 48% PTC 57%, FTC 25%, PDTC 10%, others 9% Metastasis to lung 86%, LN 51%, bone 27%, liver 14% | Male 77%, Female 23% PTC 51%, FTC 37%, PDTC 12% Metastasis to lung 89%, bone 39% |
| Median PFS | 10.6 months vs. 5.8 months HR 0.59, 95% CI 0.45–0.76, p < 0.0001 | 18.3 months vs. 3.6 months HR 0.21; 99% CI 0.14–0.31, p < 0.001 |
| Overall response rate | 12.2% vs. 0.5%, p < 0.0001 | 64.8% vs. 1.5%, p < 0.001 |
| Overall survival | HR 0.80, 95% CI 0.54–1.19, p = 0.14 | HR 0.73, 95% CI 0.50–1.07, p = 0.10 |
| Parameter | Agent | Study Design | Results | Reference |
|---|---|---|---|---|
| Age | Lenvatinib | Prespecified subanalysis | Outcomes: OS (LEN vs. Pbo) Age ≤65 years: HR 0.98, 95% CI 0.58–1.66, p = 0.90 Age >65 years: HR 0.53, 95% CI 0.53–0.91, p = 0.01 | [42] |
| Sex | Lenvatinib | Prespecified subanalysis | Outcomes: PFS (LEN vs. Pbo) Male:
| [24] |
| Histological subtype | Lenvatinib | Prespecified subanalysis | Outcomes: OS (LEN vs. Pbo) Papillary: HR 0.73, 95% CI 0.50–1.07 Follicular: HR 0.41, 95% CI 0.18–0.97 | [24] |
| Liver metastasis | Lenvatinib | Prespecified subanalysis | Outcomes: Duration of response Liver metastasis (+) vs. (−): 15.7 months vs. 30.5 months | [43] |
| Brain metastasis | Lenvatinib | Prespecified subanalysis | Outcomes: Duration of response Brain metastasis (+) vs. (−): 9.3 months vs. 30.5 months | [43] |
| Baseline Tg level | Sorafenib | Post hoc | Outcomes: PFS (Tg high vs. Tg low) HR 2.03, 95% CI 1.52–2.71, p < 0.001 (Cut-off point: 1021 ng/mL) | [44] |
| Baseline Tg level | Lenvatinib | Exploratory analysis | Outcomes: PFS (Tg high vs. Tg low) Univariate p = 0.027, Multivariate p = 0.051 (Cut-off point: 1st quartile) | [45] |
| Tumor volume doubling time | Lenvatinib | Retrospective | Outcomes: MST
| [46] |
| Tumor volume doubling time | Sorafenib | Retrospective | Outcomes: PFS TV-DT ≤ 6 months: HR 2.70, 95% CI 1.33–5.45 TV-DT 6 months–1 year: HR 2.06, 95% CI 0.92–4.63 TV-DT 1–5 years: HR 1.35, 95% CI 0.69–2.63 TV-DT >5 years: Reference | [47] |
| Tumor-related symptoms | Sorafenib | Post hoc | Outcomes: PFS (SOR vs. Pbo) Asymptomatic:
| [48] |
| Tumor-related symptoms | Lenvatinib | Retrospective | Outcomes: PFS Symptomatic vs. asymptomatic: Relative risk 111.8, 95% CI 7.90–1581.3, p < 0.01 | [49] |
| ECOG PS | Lenvatinib | Post hoc | PS 0 vs. ≥1: Outcomes: PFS HR 0.51, 95% CI 0.34–0.76, p = 0.0008 Outcomes: OS HR 0.44, 95% CI 0.27–0.73, p = 0.001 | [50] |
| Baseline tumor size | Lenvatinib | Post hoc | Outcomes: OS Baseline tumor size >40 mm vs. ≤40 mm: 29.1 months vs. NR, HR 0.42, 95% CI 0.28–0.63 | [51] |
| Baseline tumor size | Lenvatinib | Retrospective | Baseline tumor size ≤42 mm vs. >42 mm Outcomes: PFS HR 3.37, 95% CI 1.26–9.02, p < 0.02 Outcomes: OS HR 4.14, 95% CI 1.42–12.11, p < 0.01 | [52] |
| Size of lung metastasis | Lenvatinib | Post hoc | Outcomes: OS (LEN vs. Pbo) Lung metastasis (any):
| [53] |
| Neutrophil-to-lymphocyte ratio | Lenvatinib | Retrospective | Outcomes: OS
| [54] |
| Neutrophil-to-lymphocyte ratio | Lenvatinib | Post hoc | NLR ≤ 3 vs. NLR > 3
| [55] |
| BRAF mutation | Sorafenib | Exploratory analysis | Outcomes: PFS
| [44] |
| BRAF mutation | Lenvatinib | Exploratory analysis | Outcomes: PFS
| [45] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fukuda, N.; Takahashi, S. Clinical Indications for Treatment with Multi-Kinase Inhibitors in Patients with Radioiodine-Refractory Differentiated Thyroid Cancer. Cancers 2021, 13, 2279. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13092279
Fukuda N, Takahashi S. Clinical Indications for Treatment with Multi-Kinase Inhibitors in Patients with Radioiodine-Refractory Differentiated Thyroid Cancer. Cancers. 2021; 13(9):2279. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13092279
Chicago/Turabian StyleFukuda, Naoki, and Shunji Takahashi. 2021. "Clinical Indications for Treatment with Multi-Kinase Inhibitors in Patients with Radioiodine-Refractory Differentiated Thyroid Cancer" Cancers 13, no. 9: 2279. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13092279