
Efficacy of Neoadjuvant Targeted Therapy for Borderline Resectable III B-D or IV Stage BRAF V600 Mutation-Positive Melanoma

 ,
,  , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Clinical Data
2.2. Statistical Analysis
3. Results
3.1. Neoadjuvant Treatment and Surgery
3.2. Neoadjuvant Treatment Safety
3.3. Treatment after Surgery
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cardoso, F.; Paluch-Shimon, S.; Senkus, E.; Curigliano, G.; Aapro, M.S.; Andre, F.; Barrios, C.H.; Bergh, J.; Bhattacharyya, G.S.; Biganzoli, L.; et al. 5th ESO-ESMO international consensus guidelines for advanced breast cancer (ABC 5). Ann. Oncol. 2020, 31, 1623–1649. [Google Scholar] [CrossRef]
- Glynne-Jones, R.; Wyrwicz, L.; Tiret, E.; Brown, G.; Rodel, C.; Cervantes, A.; Arnold, D.; ESMO Guidelines Committee. Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv263. [Google Scholar] [CrossRef]
- Lordick, F.; Mariette, C.; Haustermans, K.; Obermannova, R.; Arnold, D.; ESMO Guidelines Committee. Oesophageal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, v50–v57. [Google Scholar] [CrossRef]
- Smyth, E.C.; Verheij, M.; Allum, W.; Cunningham, D.; Cervantes, A.; Arnold, D.; ESMO Guidelines Committee. Gastric cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, v38–v49. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.T.; Zackrisson, S.; Senkus, E.; ESMO Guidelines Committee. Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019, 30, 1674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gronchi, A.; Miah, A.B.; Dei Tos, A.P.; Abecassis, N.; Bajpai, J.; Bauer, S.; Biagini, R.; Bielack, S.; Blay, J.Y.; Bolle, S.; et al. Soft tissue and visceral sarcomas: ESMO-EURACAN-GENTURIS Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2021, 32, 1348–1365. [Google Scholar] [CrossRef] [PubMed]
- Michielin, O.; van Akkooi, A.C.J.; Ascierto, P.A.; Dummer, R.; Keilholz, U.; The ESMO Guidelines Committee. Cutaneous melanoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-updagger. Ann. Oncol. 2019, 30, 1884–1901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rutkowski, P.; Wysocki, P.J.; Nasierowska-Guttmejer, A.; Jeziorski, A.; Wysocki, W.M.; Kalinka, E.; Świtaj, T.; Kozak, K.; Kamińska-Winciorek, G.; Czarnecka, A.M.; et al. Czerniak skóry. Onkol. W Prakt. Klin. -Eduk. 2020, 6, 225–245. [Google Scholar]
- Rutkowski, P.; Wysocki, P.J.; Nasierowska-Guttmejer, A.; Jeziorski, A.; Wysocki, W.M.; Kalinka, E.; Świtaj, T.; Kozak, K.; Kamińska-Winciorek, G.; Czarnecka, A.M.; et al. Cutaneous melanoma. Oncol. Clin. Pract. 2020, 16, 163–182. [Google Scholar] [CrossRef]
- Blankenstein, S.A.; Rohaan, M.W.; Klop, W.M.C.; van der Hiel, B.; van de Wiel, B.A.; Lahaye, M.J.; Adriaansz, S.; Sikorska, K.; van Tinteren, H.; Sari, A.; et al. Neoadjuvant Cytoreductive Treatment with BRAF/MEK Inhibition of prior Unresectable Regionally Advanced Melanoma to Allow Complete Surgical Resection, REDUCTOR: A Prospective, Single Arm, Open-label Phase II Trial. Ann. Surg. 2021, 274, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Ługowska, I.; Szkultecka Dębek, M.; Sozańska-Solak, A.; Ziobro, M.; Wysocki, P.J.; Barszcz, E.; Jakubczyk, M.; Niewada, M.; Rutkowski, P. Stage III/IV Melanoma in Poland: Epidemiology, standard of care and treatment related costs. J. Health Policy Outcomes Res. 2012, 2, 41–47. [Google Scholar] [CrossRef]
- Borgstein, P.J.; Meijer, S.; van Diest, P.J. Are locoregional cutaneous metastases in melanoma predictable? Ann. Surg. Oncol. 1999, 6, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Perez, M.C.; Tanabe, K.K.; Ariyan, C.E.; Miura, J.T.; Mutabdzic, D.; Farma, J.M.; Zager, J.S. Local and Recurrent Regional Metastases of Melanoma. Cutan. Melanoma 2019, 705–737. [Google Scholar] [CrossRef] [Green Version]
- Nan Tie, E.; Lai-Kwon, J.E.; Gyorki, D.E. Systemic therapies for unresectable locoregional melanoma: A significant area of need. Melanoma Manag. 2019, 6, MMT25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eroglu, Z.; Eatrides, J.; Naqvi, S.M.H.; Kim, Y.; Rich, J.; Babacan, N.A.; Brohl, A.S.; Markowitz, J.; Sarnaik, A.; Zager, J.; et al. Neoadjuvant BRAF-targeted therapy in regionally advanced and oligometastatic melanoma. Pigment. Cell Melanoma Res. 2020, 33, 86–95. [Google Scholar] [CrossRef]
- Koyanagi, K.; O’Day, S.J.; Gonzalez, R.; Lewis, K.; Robinson, W.A.; Amatruda, T.T.; Wang, H.J.; Elashoff, R.M.; Takeuchi, H.; Umetani, N.; et al. Serial monitoring of circulating melanoma cells during neoadjuvant biochemotherapy for stage III melanoma: Outcome prediction in a multicenter trial. J. Clin. Oncol. 2005, 23, 8057–8064. [Google Scholar] [CrossRef] [Green Version]
- Pierard, G.E.; Pierard-Franchimont, C.; Reginster, M.A.; Quatresooz, P. Smouldering malignant melanoma and metastatic dormancy: An update and review. Derm. Res. Pract. 2012, 2012, 461278. [Google Scholar] [CrossRef] [Green Version]
- Balch, C.M.; Gershenwald, J.E.; Soong, S.J.; Thompson, J.F.; Atkins, M.B.; Byrd, D.R.; Buzaid, A.C.; Cochran, A.J.; Coit, D.G.; Ding, S.; et al. Final version of 2009 AJCC melanoma staging and classification. J. Clin. Oncol. 2009, 27, 6199–6206. [Google Scholar] [CrossRef] [Green Version]
- Gershenwald, J.E.; Scolyer, R.A.; Hess, K.R.; Sondak, V.K.; Long, G.V.; Ross, M.I.; Lazar, A.J.; Faries, M.B.; Kirkwood, J.M.; McArthur, G.A.; et al. Melanoma staging: Evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 472–492. [Google Scholar] [CrossRef] [Green Version]
- Teterycz, P.; Ługowska, I.; Koseła-Paterczyk, H.; Rutkowski, P. Comparison of seventh and eighth edition of AJCC staging system in melanomas at locoregional stage. World J. Surg. Oncol. 2019, 17, 129. [Google Scholar] [CrossRef] [PubMed]
- Garbe, C.; Keim, U.; Suciu, S.; Amaral, T.; Eigentler, T.K.; Gesierich, A.; Hauschild, A.; Heinzerling, L.; Kiecker, F.; Schadendorf, D.; et al. Prognosis of Patients With Stage III Melanoma According to American Joint Committee on Cancer Version 8: A Reassessment on the Basis of 3 Independent Stage III Melanoma Cohorts. J. Clin. Oncol. 2020, 38, 2543–2551. [Google Scholar] [CrossRef]
- Dong, X.D.; Tyler, D.; Johnson, J.L.; DeMatos, P.; Seigler, H.F. Analysis of prognosis and disease progression after local recurrence of melanoma. Cancer 2000, 88, 1063–1071. [Google Scholar] [CrossRef]
- Long, G.V.; Hauschild, A.; Santinami, M.; Atkinson, V.; Mandalà, M.; Chiarion-Sileni, V.; Larkin, J.; Nyakas, M.; Dutriaux, C.; Haydon, A.; et al. Adjuvant Dabrafenib plus Trametinib in Stage III BRAF-Mutated Melanoma. N. Engl. J. Med. 2017, 377, 1813–1823. [Google Scholar] [CrossRef] [Green Version]
- Dummer, R.; Hauschild, A.; Santinami, M.; Atkinson, V.; Mandala, M.; Kirkwood, J.M.; Chiarion Sileni, V.; Larkin, J.; Nyakas, M.; Dutriaux, C.; et al. Five-Year Analysis of Adjuvant Dabrafenib plus Trametinib in Stage III Melanoma. N. Engl. J. Med. 2020, 383, 1139–1148. [Google Scholar] [CrossRef]
- Christofyllakis, K.; Pföhler, C.; Bewarder, M.; Müller, C.S.L.; Thurner, L.; Rixecker, T.; Vogt, T.; Stilgenbauer, S.; Yordanova, K.; Kaddu-Mulindwa, D. Adjuvant Therapy of High-Risk (Stages IIC–IV) Malignant Melanoma in the Post Interferon-Alpha Era: A Systematic Review and Meta-Analysis. Front. Oncol. 2021, 10, 3481. [Google Scholar] [CrossRef]
- Owen, C.; Palmieri, D.; Guminski, A.; Carlino, M.S.; Menzies, A.M.; Long, G.V. Management of melanoma recurrence following adjuvant anti-PD1 therapy. Ann. Oncol. 2018, 29, viii446–viii447. [Google Scholar] [CrossRef]
- Bhave, P.; Pallan, L.; Long, G.V.; Menzies, A.M.; Atkinson, V.; Cohen, J.V.; Sullivan, R.J.; Chiarion-Sileni, V.; Nyakas, M.; Kahler, K.; et al. Melanoma recurrence patterns and management after adjuvant targeted therapy: A multicentre analysis. Br. J. Cancer 2021, 124, 574–580. [Google Scholar] [CrossRef]
- Amaria, R.N.; Prieto, P.A.; Tetzlaff, M.T.; Reuben, A.; Andrews, M.C.; Ross, M.I.; Glitza, I.C.; Cormier, J.; Hwu, W.J.; Tawbi, H.A.; et al. Neoadjuvant plus adjuvant dabrafenib and trametinib versus standard of care in patients with high-risk, surgically resectable melanoma: A single-centre, open-label, randomised, phase 2 trial. Lancet Oncol. 2018, 19, 181–193. [Google Scholar] [CrossRef]
- Zippel, D.; Markel, G.; Shapira-Frommer, R.; Ben-Betzalel, G.; Goitein, D.; Ben-Ami, E.; Nissan, A.; Schachter, J.; Schneebaum, S. Perioperative BRAF inhibitors in locally advanced stage III melanoma. J. Surg. Oncol. 2017, 116, 856–861. [Google Scholar] [CrossRef] [PubMed]
- Long, G.V.; Saw, R.P.M.; Lo, S.; Nieweg, O.E.; Shannon, K.F.; Gonzalez, M.; Guminski, A.; Lee, J.H.; Lee, H.; Ferguson, P.M.; et al. Neoadjuvant dabrafenib combined with trametinib for resectable, stage IIIB-C, BRAF(V600) mutation-positive melanoma (NeoCombi): A single-arm, open-label, single-centre, phase 2 trial. Lancet Oncol. 2019, 20, 961–971. [Google Scholar] [CrossRef]
- Villani, A.; Scalvenzi, M.; Fabbrocini, G.; Ocampo-Candiani, J.; Ocampo-Garza, S.S. Looking into a Better Future: Novel Therapies for Metastatic Melanoma. Dermatol. Ther. 2021, 11, 751–767. [Google Scholar] [CrossRef]
- Huang, A.C.; Orlowski, R.J.; Xu, X.; Mick, R.; George, S.M.; Yan, P.K.; Manne, S.; Kraya, A.A.; Wubbenhorst, B.; Dorfman, L.; et al. A single dose of neoadjuvant PD-1 blockade predicts clinical outcomes in resectable melanoma. Nat. Med. 2019, 25, 454–461. [Google Scholar] [CrossRef]
- Jakub, J.W.; Racz, J.M.; Hieken, T.J.; Gonzalez, A.B.; Kottschade, L.A.; Markovic, S.N.; Yan, Y.; Block, M.S. Neoadjuvant systemic therapy for regionally advanced melanoma. J. Surg. Oncol. 2018, 117, 1164–1169. [Google Scholar] [CrossRef]
- Fadaki, N.; Cardona-Huerta, S.; Martineau, L.; Thummala, S.; Cheng, S.T.; Bunker, S.R.; Garcia-Kennedy, R.; Wang, W.; Minor, D.; Kashani-Sabet, M.; et al. Inoperable bulky melanoma responds to neoadjuvant therapy with vemurafenib. BMJ Case Rep. 2012, 2012, bcr2012007034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koers, K.; Francken, A.B.; Haanen, J.B.; Woerdeman, L.A.; van der Hage, J.A. Vemurafenib as neoadjuvant treatment for unresectable regional metastatic melanoma. J. Clin. Oncol. 2013, 31, e251–e253. [Google Scholar] [CrossRef] [PubMed]
- Menzies, A.M.; Amaria, R.N.; Rozeman, E.A.; Huang, A.C.; Tetzlaff, M.T.; van de Wiel, B.A.; Lo, S.; Tarhini, A.A.; Burton, E.M.; Pennington, T.E.; et al. Pathological response and survival with neoadjuvant therapy in melanoma: A pooled analysis from the International Neoadjuvant Melanoma Consortium (INMC). Nat. Med. 2021, 27, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Boulva, K.; Apte, S.; Yu, A.; Tran, A.; Shorr, R.; Song, X.; Ong, M.; Nessim, C. Contemporary Neoadjuvant Therapies for High-Risk Melanoma: A Systematic Review. Cancers 2021, 13, 1905. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.Y.; Lowe, M. Neoadjuvant Treatments for Advanced Resectable Melanoma. J. Surg. Oncol. 2019, 119, 216–221. [Google Scholar] [CrossRef]
- Selli, C.; Sims, A.H. Neoadjuvant Therapy for Breast Cancer as a Model for Translational Research. Breast Cancer 2019, 13. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | Mean (Median) | SD | Range | |
|---|---|---|---|---|
| 50 (55) | 17.91 | 17–84 | ||
| LDH | 209 (180) | 78.84 | 128–513 | |
| NLR | 2.9 (2.4) | 0.78–0.73 | ||
| Gender | N | % | ||
| F | 26 | 56.5 | ||
| M | 20 | 43.5 | ||
| ECOG | 0 | 24 | 52.2 | |
| 1 | 21 | 45.7 | ||
| 2 | 1 | 2.2 | ||
| Melanoma | Skin | 36 | ||
| Mucosal | 2 | |||
| UPM | 8 | |||
| Primary tumor location | Head and neck | 4 | ||
| Upper and lower limb | 18 | |||
| Chest | 3 | |||
| Abdomen | 2 | |||
| Back | 9 | |||
| Genito-urinary | 2 | |||
| UPM | 8 | |||
| Primary tumor | T1 | 2 | ||
| T2 | 6 | |||
| T3 | 10 | |||
| T4 | 17 | |||
| Tx | 3 | |||
| UPM | 8 | |||
| Lymph nodes | N0 | 12 | ||
| N1a | 0 | |||
| N1b | 7 | |||
| N1c | 6 | |||
| N2a | 0 | |||
| N2b | 5 | |||
| N2c | 3 | |||
| N3a | 0 | |||
| N3b | 13 | |||
| N3c | 0 | |||
| Disease Location | Number of Patients | % of Patients |
|---|---|---|
| Localized disease | 8 | 17.4 |
| Skin metastases | 5 | 10.9 |
| Extra-regional nodes metastases | 5 | 10.9 |
| Regional nodes metastases | 14 | 30.4 |
| Recurrence after LND/SNLB | 11 | 23.9 |
| Primary tumor recurrence | 3 | 6.5 |
| Resection | N | % |
|---|---|---|
| Skin metastases resection | 7 | 15.2 |
| Extra-regional LND | 3 | 6.5 |
| Regional LND | 18 | 39.1 |
| Recurrence after LND/SNLB resection | 11 | 23.9 |
| Primary tumor scar recurrence resection | 7 | 15.2 |
| PFS | DFS | OS |
|---|---|---|
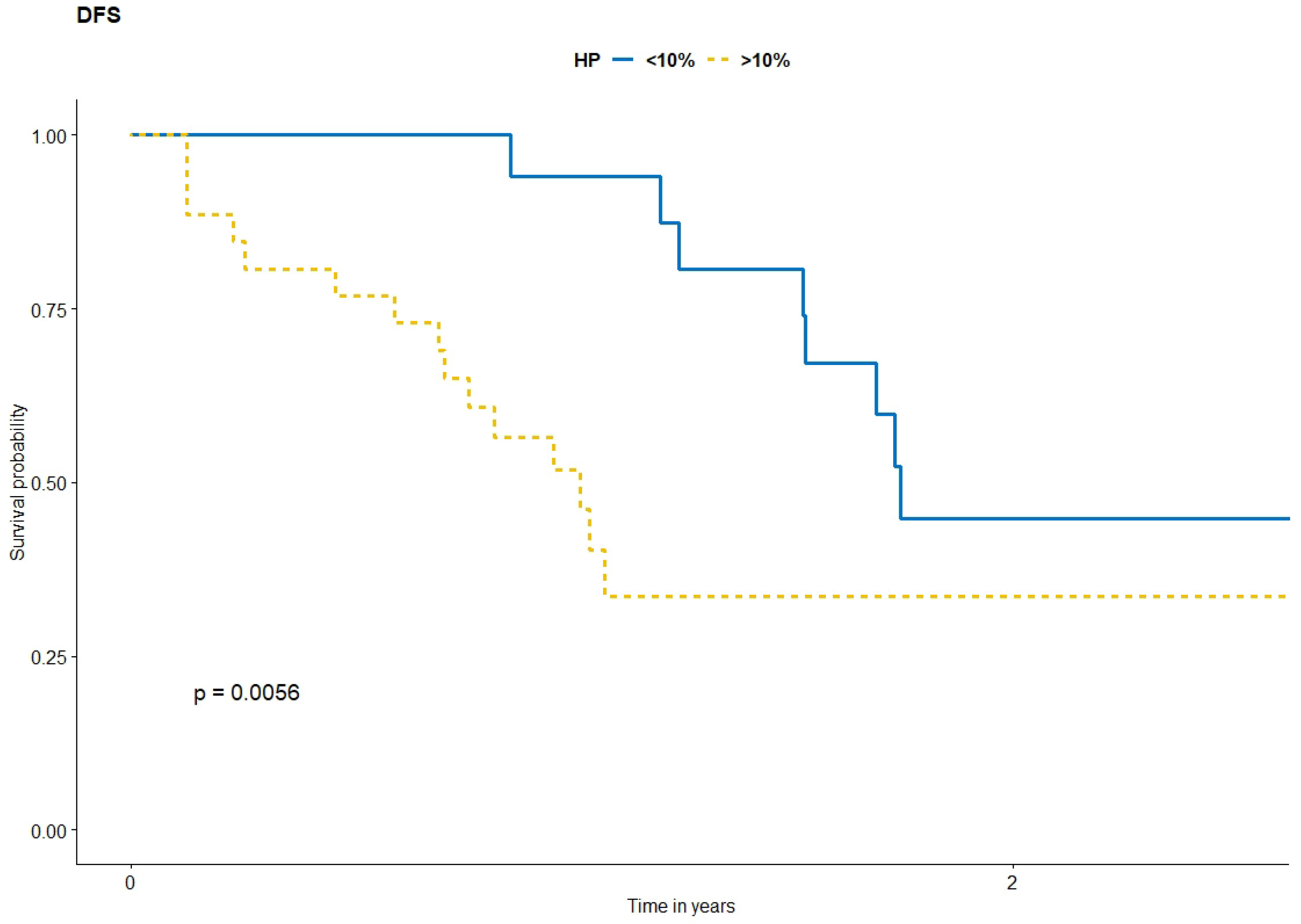
| <10% melanoma cells | <10% melanoma cells | <10% melanoma cells |
| 12m = 94.7% (95%CI 0.852–1.000) | 12m = 94.1% (95%CI 0.84–1) | 12m = 100% (95%CI 1.000–1) |
| 24m = 71.6% (95%CI 0.533–0.962) | 18m = 80.7% (95%CI 0.63–1) | 24m = 94.7% (95%CI 0.852–1) |
| 36m = 43.0% (95%CI 0.211–0.874) | 24m = 44.8% (95%CI 0.25–0.8) | 36m = 75.8% (95%CI 0.483–1) |
| >10% melanoma cells | >10% melanoma cells | >10% melanoma cells |
| 12m = 76.9% (95%CI 0.6232–0.949) | 12m = 51.8% (95%CI 0.35–0.76) | 12m = 84.6% (95%CI 0.718–0.997) |
| 24m = 41.3% (95%CI 0.2509–0.681) | 24m = 33.6% (95%CI 0.18–0.63) | 24m = 56.8% (95%CI 0.373–0.865) |
| 36m = 20.7% (95%CI 0.0474–0.902) | 36m = 33.6% (95%CI 0.18–0.63) | 36m = 56.8% (95%CI 0.373–0.865) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Czarnecka, A.M.; Ostaszewski, K.; Borkowska, A.; Szumera-Ciećkiewicz, A.; Kozak, K.; Świtaj, T.; Rogala, P.; Kalinowska, I.; Koseła-Paterczyk, H.; Zaborowski, K.; et al. Efficacy of Neoadjuvant Targeted Therapy for Borderline Resectable III B-D or IV Stage BRAF V600 Mutation-Positive Melanoma. Cancers 2022, 14, 110. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14010110
Czarnecka AM, Ostaszewski K, Borkowska A, Szumera-Ciećkiewicz A, Kozak K, Świtaj T, Rogala P, Kalinowska I, Koseła-Paterczyk H, Zaborowski K, et al. Efficacy of Neoadjuvant Targeted Therapy for Borderline Resectable III B-D or IV Stage BRAF V600 Mutation-Positive Melanoma. Cancers. 2022; 14(1):110. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14010110
Chicago/Turabian StyleCzarnecka, Anna M., Krzysztof Ostaszewski, Aneta Borkowska, Anna Szumera-Ciećkiewicz, Katarzyna Kozak, Tomasz Świtaj, Paweł Rogala, Iwona Kalinowska, Hanna Koseła-Paterczyk, Konrad Zaborowski, and et al. 2022. "Efficacy of Neoadjuvant Targeted Therapy for Borderline Resectable III B-D or IV Stage BRAF V600 Mutation-Positive Melanoma" Cancers 14, no. 1: 110. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14010110