
Modifiers of and Disparities in Palliative and Supportive Care Timing and Utilization among Neurosurgical Patients with Malignant Central Nervous System Tumors

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
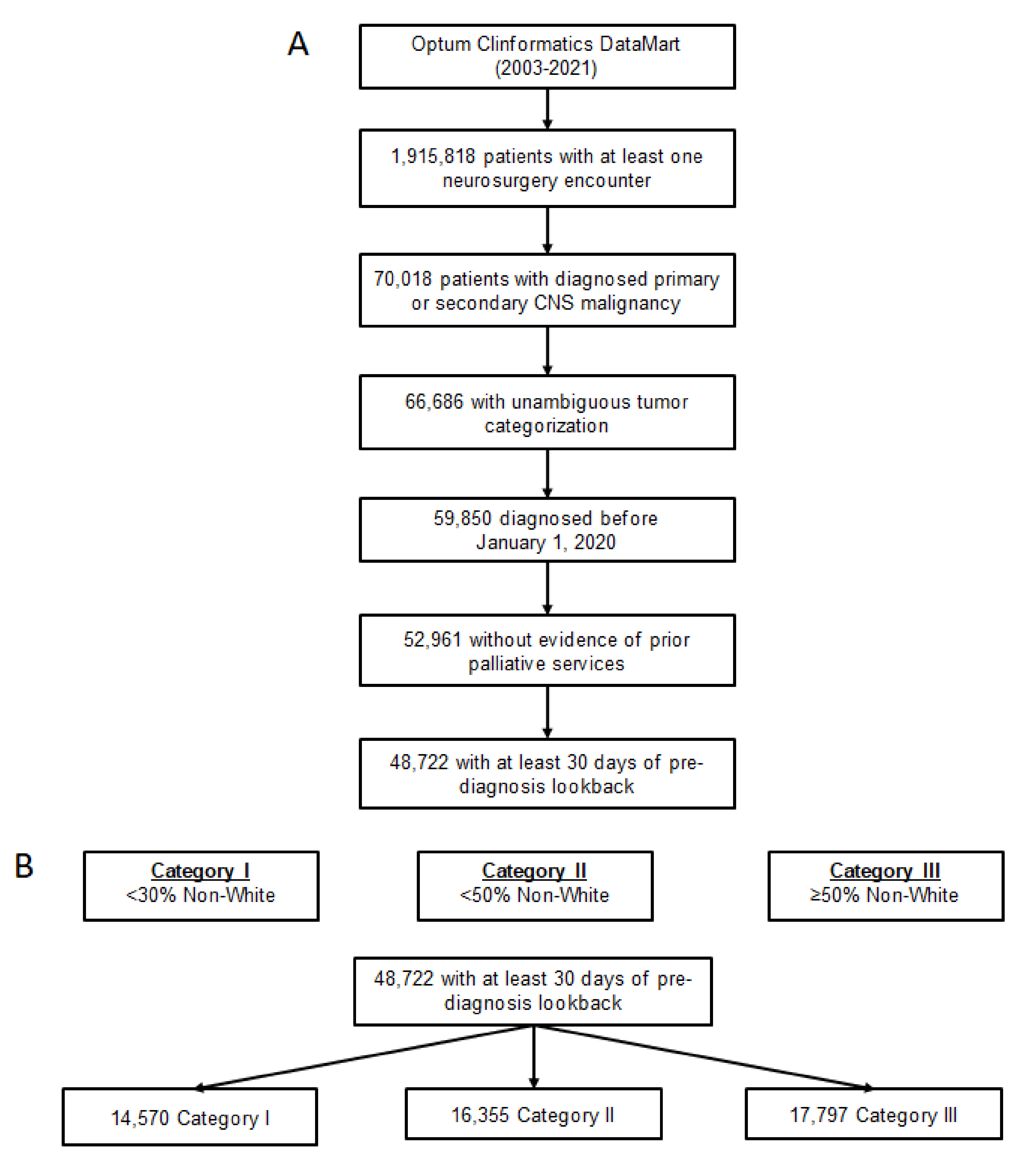
2.2. Cohort Design
2.3. Statistical Analysis
3. Results
4. Discussion
4.1. Racial Disparities in Treatment and Surgical Outcomes
4.2. Racial Disparities in Palliative and Supportive Care
4.3. Provider Influences on Quality of Healthcare for Minority Groups
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| American Society of Clinical Oncology (ASCO) |
| Central nervous system (CNS) |
| Current Procedural Terminology (CPT) |
| Exclusive Provider Organization (EPO) |
| Glioblastoma (GBM) |
| Health Maintenance Organization (HMO) |
| Indemnity (IND) |
| International Classification of Diseases (ICD) system |
| Other (OTH) |
| Palliative care (PC) |
| Point-of-service (POS) |
| Provider patient racial diversity index (provider pRDI) |
References
- World Health Organization. Palliative Care; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Toor, H.; Barrett, R.; Myers, J.; Parry, N. Implementing a Novel Interprofessional Caregiver Support Clinic: A Palliative Medicine and Social Work Collaboration. Am. J. Hosp. Palliat. Med. 2021, 10499091211051669. [Google Scholar] [CrossRef] [PubMed]
- Bekelman, D.B.; Johnson-Koenke, R.; Bowles, D.W.; Fischer, S.M. Improving Early Palliative Care with a Scalable, Stepped Peer Navigator and Social Work Intervention: A Single-Arm Clinical Trial. J. Palliat. Med. 2018, 21, 1011–1016. [Google Scholar] [CrossRef] [PubMed]
- Moncho, M.E.I.; Palomar-Abril, V.; Soria-Comes, T. Palliative Care Unit at Home: Impact on Quality of Life in Cancer Patients at the End of Life in a Rural Environment. Am. J. Hosp. Palliat. Med. 2021, 39, 529–532. [Google Scholar] [CrossRef] [PubMed]
- Chini, C.; Bascialla, L.; Giaquinto, A.; Magni, E.; Gobba, S.M.; Proserpio, I.; Suter, M.B.; Nigro, O.; Tinelli, G.; Pinotti, G. Homcology: Home chemotherapy delivery in a simultaneous care project for frail advanced cancer patients. Support. Care Cancer 2020, 29, 917–923. [Google Scholar] [CrossRef]
- Ferrell, B.R.; Temel, J.S.; Temin, S.; Alesi, E.R.; Balboni, T.A.; Basch, E.M.; Firn, J.I.; Paice, J.A.; Peppercorn, J.M.; Phillips, T.; et al. Integration of Palliative Care Into Standard Oncology Care: American Society of Clinical Oncology Clinical Practice Guideline Update. J. Clin. Oncol. 2017, 35, 96–112. [Google Scholar] [CrossRef] [Green Version]
- Stupp, R.; Taillibert, S.; Kanner, A.A.; Kesari, S.; Steinberg, D.M.; Toms, S.A.; Taylor, L.P.; Lieberman, F.; Silvani, A.; Fink, K.L.; et al. Maintenance Therapy With Tumor-Treating Fields Plus Temozolomide vs Temozolomide Alone for Glioblastoma. JAMA 2015, 314, 2535–2543. [Google Scholar] [CrossRef]
- Stupp, R.; Taillibert, S.; Kanner, A.A.; Read, W.; Steinberg, D.M.; Lhermitte, B.; Toms, S.; Idbaih, A.; Ahluwalia, M.S.; Fink, K.; et al. Effect of Tumor-Treating Fields Plus Maintenance Temozolomide vs Maintenance Temozolomide Alone on Survival in Patients With Glioblastoma. JAMA 2017, 318, 2306–2316. [Google Scholar] [CrossRef] [Green Version]
- Nabors, L.B.; Portnow, J.; Ahluwalia, M.; Baehring, J.; Brem, H.; Brem, S.; Butowski, N.; Campian, J.L.; Clark, S.W.; Fabiano, A.J.; et al. Central Nervous System Cancers, Version 3.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2020, 18, 1537–1570. [Google Scholar] [CrossRef]
- Corbett, K.; Sharma, A.; Pond, G.R.; Brastianos, P.K.; Das, S.; Sahgal, A.; Jerzak, K.J. Central Nervous System–Specific Outcomes of Phase 3 Randomized Clinical Trials in Patients with Advanced Breast Cancer, Lung Cancer, and Melanoma. JAMA Oncol. 2021, 7, 1062. [Google Scholar] [CrossRef]
- Zeng, C.; Wen, W.; Morgans, A.K.; Pao, W.; Shu, X.-O.; Zheng, W. Disparities by Race, Age, and Sex in the Improvement of Survival for Major Cancers. JAMA Oncol. 2015, 1, 88–96. [Google Scholar] [CrossRef]
- Vlacich, G.; Samson, P.P.; Perkins, S.M.; Roach, M.C.; Parikh, P.J.; Bradley, J.D.; Lockhart, A.C.; Puri, V.; Meyers, B.F.; Kozower, B.; et al. Treatment utilization and outcomes in elderly patients with locally advanced esophageal carcinoma: A review of the National Cancer Database. Cancer Med. 2017, 6, 2886–2896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, A.P.; Nguyen, D.-D.; Meirkhanov, A.; Golshan, M.; Melnitchouk, N.; Lipsitz, S.R.; Kilbridge, K.L.; Kibel, A.S.; Cooper, Z.; Weissman, J.; et al. Association of Care at Minority-Serving vs Non-Minority-Serving Hospitals With Use of Palliative Care Among Racial/Ethnic Minorities with Metastatic Cancer in the United States. JAMA Netw. Open 2019, 2, e187633. [Google Scholar] [CrossRef] [PubMed]
- Elixhauser, A.; Steiner, C.; Harris, D.R.; Coffey, R.M. Comorbidity Measures for Use with Administrative Data. Med. Care 1998, 36, 8–27. [Google Scholar] [CrossRef] [PubMed]
- Goyal, A.; Zreik, J.; Brown, D.A.; Kerezoudis, P.; Habermann, E.B.; Chaichana, K.L.; Chen, C.C.; Bydon, M.; Parney, I.F. Disparities in access to surgery for glioblastoma multiforme at high-volume Commission on Cancer–accredited hospitals in the United States. J. Neurosurg. 2021, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Hodges, T.R.; Labak, C.M.; Mahajan, U.V.; Wright, C.H.; Wright, J.; Cioffi, G.; Gittleman, H.; Herring, E.Z.; Zhou, X.; Duncan, K.; et al. Impact of race on care, readmissions, and survival for patients with glioblastoma: An analysis of the National Cancer Database. Neuro-Oncol. Adv. 2021, 3, vdab040. [Google Scholar] [CrossRef] [PubMed]
- Ramos, R.D.L.G.; Benton, J.A.; Gelfand, Y.; Echt, M.; Rodriguez, J.V.F.; Yanamadala, V.; Yassari, R. Racial disparities in clinical presentation, type of intervention, and in-hospital outcomes of patients with metastatic spine disease: An analysis of 145,809 admissions in the United States. Cancer Epidemiol. 2020, 68, 101792. [Google Scholar] [CrossRef] [PubMed]
- Chiu, R.G.; Murphy, B.E.; Zhu, A.; Mehta, A.I. Racial and Ethnic Disparities in the Inpatient Management of Primary Spinal Cord Tumors. World Neurosurg. 2020, 140, e175–e184. [Google Scholar] [CrossRef]
- Kim, E.; McClelland, I.S.; Jaboin, J.J.; Attia, A. Disparities in Patterns of Conventional Versus Stereotactic Body Radiotherapy in the Treatment of Spine Metastasis in the United States. J. Palliat. Care 2020, 36, 130–134. [Google Scholar] [CrossRef]
- Muhlestein, W.E.; Akagi, D.S.; Chotai, S.; Chambless, L.B. The Impact of Race on Discharge Disposition and Length of Hospitalization After Craniotomy for Brain Tumor. World Neurosurg. 2017, 104, 24–38. [Google Scholar] [CrossRef]
- Hung, B.; Pennington, Z.; Hersh, A.M.; Schilling, A.; Ehresman, J.; Patel, J.; Antar, A.; Porras, J.L.; Elsamadicy, A.A.; Sciubba, D.M. Impact of race on nonroutine discharge, length of stay, and postoperative complications after surgery for spinal metastases. J. Neurosurg. Spine 2022, 36, 678–685. [Google Scholar] [CrossRef]
- Mazor, M.B.; Li, L.; Morillo, J.; Allen, O.S.; Wisnivesky, J.P.; Smith, C.B. Disparities in Supportive Care Needs Over Time Between Racial and Ethnic Minority and Non-Minority Patients With Advanced Lung Cancer. J. Pain Symptom Manag. 2022, 63, 563–571. [Google Scholar] [CrossRef] [PubMed]
- LoPresti, M.A.; Dement, F.; Gold, H.T. End-of-Life Care for People With Cancer From Ethnic Minority Groups. Am. J. Hosp. Palliat. Med. 2014, 33, 291–305. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.K.; Earle, C.C.; McCarthy, E.P. Racial and Ethnic Differences in End-of-Life Care in Fee-for-Service Medicare Beneficiaries with Advanced Cancer. J. Am. Geriatr. Soc. 2008, 57, 153–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reyes-Gibby, C.C.; Anderson, K.O.; Shete, S.; Bruera, E.; Yennurajalingam, S. Early referral to supportive care specialists for symptom burden in lung cancer patients. Cancer 2011, 118, 856–863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubens, M.; Ramamoorthy, V.; Saxena, A.; McGranaghan, P.; Bhatt, C.; Das, S.; Shehadeh, N.; Veledar, E.; Viamonte-Ros, A.; Odia, Y.; et al. Inpatient Palliative Care Use Among Critically III Brain Metastasis Patients in the United States. Am. J. Clin. Oncol. 2020, 43, 806–812. [Google Scholar] [CrossRef]
- Xu, G.; Fields, S.K.; Laine, C.; Veloski, J.J.; Barzansky, B.; Martini, C.J. The relationship between the race/ethnicity of generalist physicians and their care for underserved populations. Am. J. Public Health 1997, 87, 817–822. [Google Scholar] [CrossRef] [Green Version]
- Diamond, L.; Izquierdo, K.; Canfield, D.; Matsoukas, K.; Gany, F. A Systematic Review of the Impact of Patient–Physician Non-English Language Concordance on Quality of Care and Outcomes. J. Gen. Intern. Med. 2019, 34, 1591–1606. [Google Scholar] [CrossRef]
- Schouten, B.C.; Meeuwesen, L.; Schouten, B.C.; Meeuwesen, L. Cultural differences in medical communication: A review of the literature. Patient Educ. Couns. 2006, 64, 21–34. [Google Scholar] [CrossRef]
- Ibrahim, S.A.; Whittle, J.; Bean-Mayberry, B.; Kelley, M.E.; Good, C.; Conigliaro, J. Racial/Ethnic Variations in Physician Recommendations for Cardiac Revascularization. Am. J. Public Health 2003, 93, 1689–1693. [Google Scholar] [CrossRef]
- Haider, A.H.; Schneider, E.B.; Sriram, N.; Dossick, D.S.; Scott, V.K.; Swoboda, S.M.; Losonczy, L.; Haut, E.R.; Efron, D.T.; Pronovost, P.J.; et al. Unconscious Race and Social Class Bias Among Acute Care Surgical Clinicians and Clinical Treatment Decisions. JAMA Surg. 2015, 150, 457–464. [Google Scholar] [CrossRef]
- Saha, S.; Komaromy, M.; Koepsell, T.D.; Bindman, A.B. Patient-Physician Racial Concordance and the Perceived Quality and Use of Health Care. Arch. Intern. Med. 1999, 159, 997–1004. [Google Scholar] [CrossRef] [PubMed]
- Doorenbos, A.Z.; Morris, A.M.; Haozous, E.A.; Harris, H.; Flum, D.R. ReCAP: Assessing Cultural Competence Among Oncology Surgeons. J. Oncol. Pract. 2016, 12, 61–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thai, A.A.; Tacey, M.; Byrne, A.; White, S.; Yoong, J. Exploring disparities in receipt of adjuvant chemotherapy in culturally and linguistically diverse groups: An Australian centre’s experience. Intern. Med. J. 2017, 48, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Hasnain-Wynia, R.; Baker, D.W.; Nerenz, D.; Feinglass, J.; Beal, A.C.; Landrum, M.B.; Behal, R.; Weissman, J.S. Disparities in Health Care Are Driven by Where Minority Patients Seek Care. Arch. Intern. Med. 2007, 167, 1233–1239. [Google Scholar] [CrossRef]
- Lu, P.W.; Scully, R.E.; Fields, A.C.; Welten, V.M.; Lipsitz, S.R.; Trinh, Q.-D.; Haider, A.; Weissman, J.S.; Freund, K.M.; Melnitchouk, N. Racial Disparities in Treatment for Rectal Cancer at Minority-Serving Hospitals. J. Gastrointest. Surg. 2020, 25, 1847–1856. [Google Scholar] [CrossRef]
- Bevilacqua, G.; Bolcato, M.; Rodriguez, D.; Aprile, A. Shared care plan: An extraordinary tool for the personalisation of medicine and respect for self-determination. Acta Biomed. 2021, 92, e2021001. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Unmatched Cohort Characteristics | ||||||||
|---|---|---|---|---|---|---|---|---|
| Characteristic | Category 1 (N = 14,570) | Category 2 (N = 16,355) | Category 3 (N = 17,797) | SMD (0 vs. 1) | SMD (0 vs. 1) | |||
| N | % | N | % | N | % | |||
| Year of Diagnosis | 2013.77 | 4.77% | 2011.01 | 4.47% | 2011.83 | 4.52% | 0.597 | 0.417 |
| Age at Diagnosis (years) | 61.31 | 16.2% | 58.56 | 21.16% | 60.83 | 14.83% | 0.146 | 0.031 |
| Sex | 0.044 | 0.075 | ||||||
| Female (ref) | 7146 | 49% | 8385 | 51.3% | 9399 | 52.8% | ||
| Male | 7424 | 51% | 7970 | 48.7% | 8398 | 47.2% | ||
| Race | 0.105 | 0.582 | ||||||
| White (ref) | 12,635 | 86.7% | 14,671 | 89.7% | 11,156 | 62.7% | ||
| Asian | 284 | 1.9% | 249 | 1.5% | 874 | 4.9% | ||
| Black | 806 | 5.5% | 812 | 5% | 3453 | 19.4% | ||
| Hispanic | 845 | 5.8% | 623 | 3.8% | 2314 | 13% | ||
| Tumor Type | 0.498 | 0.564 | ||||||
| Primary (ref) | 10,128 | 69.5% | 7466 | 45.6% | 7574 | 42.6% | ||
| Secondary | 4442 | 30.5% | 8889 | 54.4% | 10,223 | 57.4% | ||
| Insurance Plan | 0.48 | 0.203 | ||||||
| HMO | 3668 | 25.2% | 3136 | 19.2% | 4205 | 23.6% | ||
| EPO | 602 | 4.1% | 1208 | 7.4% | 1351 | 7.6% | ||
| IND | 295 | 2% | 461 | 2.8% | 336 | 1.9% | ||
| OTH | 4213 | 28.9% | 2175 | 13.3% | 4155 | 23.3% | ||
| POS | 4549 | 31.2% | 7568 | 46.3% | 5767 | 32.4% | ||
| PPO | 1243 | 8.5% | 1807 | 11% | 1983 | 11.1% | ||
| Received Surgery Post-Diagnosis | 9271 | 63.6% | 10,540 | 64.4% | 11,861 | 66.6% | 0.017 | 0.063 |
| Comorbidities | ||||||||
| Congestive Heart Failure | 116 | 0.8% | 104 | 0.6% | 175 | 1% | 0.019 | 0.02 |
| Cardiac Arrhythmia | 342 | 2.3% | 323 | 2% | 404 | 2.3% | 0.026 | 0.005 |
| Valvular Disease | 119 | 0.8% | 110 | 0.7% | 160 | 0.9% | 0.017 | 0.009 |
| Pulmonary Circulation Disorders | 56 | 0.4% | 34 | 0.2% | 62 | 0.3% | 0.032 | 0.006 |
| Peripheral Vascular Disorders | 168 | 1.2% | 140 | 0.9% | 227 | 1.3% | 0.03 | 0.011 |
| Hypertension Uncomplicated | 1487 | 10.2% | 1356 | 8.3% | 2159 | 12.1% | 0.066 | 0.061 |
| Hypertension Complicated | 88 | 0.6% | 110 | 0.7% | 196 | 1.1% | 0.009 | 0.054 |
| Paralysis | 42 | 0.3% | 29 | 0.2% | 50 | 0.3% | 0.023 | 0.001 |
| Chronic Pulmonary Disease | 511 | 3.5% | 603 | 3.7% | 759 | 4.3% | 0.01 | 0.039 |
| Diabetes Uncomplicated | 605 | 4.2% | 598 | 3.7% | 1032 | 5.8% | 0.026 | 0.076 |
| Diabetes Complicated | 186 | 1.3% | 110 | 0.7% | 264 | 1.5% | 0.062 | 0.018 |
| Hypothyroidism | 380 | 2.6% | 356 | 2.2% | 445 | 2.5% | 0.028 | 0.007 |
| Renal Failure | 144 | 1% | 107 | 0.7% | 212 | 1.2% | 0.037 | 0.02 |
| Liver Disease | 91 | 0.6% | 125 | 0.8% | 163 | 0.9% | 0.017 | 0.033 |
| Peptic Ulcer Disease excluding bleeding | 16 | 0.1% | 13 | 0.1% | 28 | 0.2% | 0.01 | 0.013 |
| AIDS/HIV | 7 | 0% | 11 | 0.1% | 34 | 0.2% | 0.008 | 0.041 |
| Rheumatoid Arthritis/Collagen | 131 | 0.9% | 128 | 0.8% | 165 | 0.9% | 0.013 | 0.003 |
| Coagulopathy | 50 | 0.3% | 70 | 0.4% | 81 | 0.5% | 0.014 | 0.018 |
| Obesity | 176 | 1.2% | 113 | 0.7% | 170 | 1% | 0.053 | 0.024 |
| Weight Loss | 35 | 0.2% | 71 | 0.4% | 92 | 0.5% | 0.033 | 0.045 |
| Fluid and Electrolyte Disorders | 137 | 0.9% | 175 | 1.1% | 242 | 1.4% | 0.013 | 0.039 |
| Blood Loss Anemia | 10 | 0.1% | 17 | 0.1% | 31 | 0.2% | 0.012 | 0.03 |
| Deficiency Anemia | 150 | 1% | 185 | 1.1% | 233 | 1.3% | 0.01 | 0.026 |
| Alcohol Abuse | 25 | 0.2% | 31 | 0.2% | 33 | 0.2% | 0.004 | 0.003 |
| Drug Abuse | 24 | 0.2% | 19 | 0.1% | 32 | 0.2% | 0.013 | 0.004 |
| Psychoses | 58 | 0.4% | 32 | 0.2% | 56 | 0.3% | 0.037 | 0.014 |
| Depression | 387 | 2.7% | 375 | 2.3% | 396 | 2.2% | 0.023 | 0.028 |
| Matched Cohort Characteristics | ||||||||
| Characteristic | Category 1 (N = 7504) | Category 2 (N = 7504) | Category 3 (N = 7504) | SMD (0 vs. 1) | SMD (0 vs. 1) | |||
| N | % | N | % | N | % | |||
| Year of Diagnosis | 2011.19 | 4.55% | 2010.99 | 4.62% | 2011.36 | 4.52% | 0.043 | 0.037 |
| Age at Diagnosis (years) | 62.52 | 15.22% | 62.36 | 15.1% | 61.71 | 15.42% | 0.01 | 0.052 |
| Sex | 0.055 | 0.019 | ||||||
| Female (ref) | 3756 | 50.1% | 3961 | 52.8% | 3826 | 51% | ||
| Male | 3748 | 49.9% | 3543 | 47.2% | 3678 | 49% | ||
| Race | <0.001 | <0.001 | ||||||
| White (ref) | 7093 | 94.5% | 7093 | 94.5% | 7093 | 94.5% | ||
| Asian | 78 | 1% | 78 | 1% | 78 | 1% | ||
| Black | 189 | 2.5% | 189 | 2.5% | 189 | 2.5% | ||
| Hispanic | 144 | 1.9% | 144 | 1.9% | 144 | 1.9% | ||
| Tumor Type | 0.062 | 0.069 | ||||||
| Primary (ref) | 3470 | 46.2% | 3237 | 43.1% | 3213 | 42.8% | ||
| Secondary | 4034 | 53.8% | 4267 | 56.9% | 4291 | 57.2% | ||
| Insurance Plan | <0.001 | <0.001 | ||||||
| HMO | 2302 | 30.7% | 2302 | 30.7% | 2302 | 30.7% | ||
| EPO | 277 | 3.7% | 277 | 3.7% | 277 | 3.7% | ||
| IND | 213 | 2.8% | 213 | 2.8% | 213 | 2.8% | ||
| OTH | 1702 | 22.7% | 1702 | 22.7% | 1702 | 22.7% | ||
| POS | 2247 | 29.9% | 2247 | 29.9% | 2247 | 29.9% | ||
| PPO | 763 | 10.2% | 763 | 10.2% | 763 | 10.2% | ||
| Received Surgery Post-DX | 4548 | 60.6% | 4742 | 63.2% | 5129 | 68.4% | 0.053 | 0.162 |
| Comorbidities | ||||||||
| Congestive Heart Failure | 62 | 0.8% | 64 | 0.9% | 88 | 1.2% | 0.003 | 0.035 |
| Cardiac Arrhythmia | 173 | 2.3% | 205 | 2.7% | 222 | 3% | 0.027 | 0.041 |
| Valvular Disease | 51 | 0.7% | 59 | 0.8% | 84 | 1.1% | 0.012 | 0.047 |
| Pulmonary Circulation Disorders | 29 | 0.4% | 17 | 0.2% | 31 | 0.4% | 0.029 | 0.004 |
| Peripheral Vascular Disorders | 101 | 1.3% | 90 | 1.2% | 119 | 1.6% | 0.013 | 0.02 |
| Hypertension Uncomplicated | 759 | 10.1% | 760 | 10.1% | 1063 | 14.2% | <0.001 | 0.124 |
| Hypertension Complicated | 53 | 0.7% | 72 | 1% | 84 | 1.1% | 0.028 | 0.043 |
| Paralysis | 20 | 0.3% | 17 | 0.2% | 27 | 0.4% | 0.008 | 0.017 |
| Chronic Pulmonary Disease | 320 | 4.3% | 369 | 4.9% | 392 | 5.2% | 0.031 | 0.045 |
| Diabetes Uncomplicated | 326 | 4.3% | 355 | 4.7% | 518 | 6.9% | 0.019 | 0.111 |
| Diabetes Complicated | 60 | 0.8% | 68 | 0.9% | 112 | 1.5% | 0.012 | 0.065 |
| Hypothyroidism | 186 | 2.5% | 210 | 2.8% | 210 | 2.8% | 0.02 | 0.02 |
| Renal Failure | 75 | 1% | 59 | 0.8% | 97 | 1.3% | 0.023 | 0.028 |
| Liver Disease | 54 | 0.7% | 74 | 1% | 81 | 1.1% | 0.029 | 0.038 |
| Peptic Ulcer Disease excluding bleeding | 9 | 0.1% | 8 | 0.1% | 17 | 0.2% | 0.004 | 0.026 |
| AIDS/HIV | 3 | 0% | 6 | 0.1% | 19 | 0.3% | 0.016 | 0.056 |
| Rheumatoid Arthritis/Collagen | 59 | 0.8% | 63 | 0.8% | 83 | 1.1% | 0.006 | 0.033 |
| Coagulopathy | 33 | 0.4% | 34 | 0.5% | 53 | 0.7% | 0.002 | 0.035 |
| Obesity | 51 | 0.7% | 57 | 0.8% | 76 | 1% | 0.009 | 0.036 |
| Weight Loss | 31 | 0.4% | 38 | 0.5% | 43 | 0.6% | 0.014 | 0.023 |
| Fluid and Electrolyte Disorders | 86 | 1.1% | 105 | 1.4% | 131 | 1.7% | 0.023 | 0.05 |
| Blood Loss Anemia | 8 | 0.1% | 11 | 0.1% | 16 | 0.2% | 0.011 | 0.027 |
| Deficiency Anemia | 87 | 1.2% | 117 | 1.6% | 101 | 1.3% | 0.035 | 0.017 |
| Alcohol Abuse | 13 | 0.2% | 23 | 0.3% | 19 | 0.3% | 0.027 | 0.017 |
| Drug Abuse | 6 | 0.1% | 8 | 0.1% | 14 | 0.2% | 0.009 | 0.029 |
| Psychoses | 17 | 0.2% | 25 | 0.3% | 31 | 0.4% | 0.02 | 0.033 |
| Depression | 186 | 2.5% | 228 | 3% | 222 | 3% | 0.034 | 0.03 |
| Characteristic | Palliative Care | Home Health Services | Social Worker Services | |||
|---|---|---|---|---|---|---|
| OR | p-Value | OR | p-Value | OR | p-Value | |
| Year of Diagnosis | 1.027 | <0.001 | 0.935 | <0.001 | 1.029 | <0.001 |
| Age at Diagnosis (years) | 1.011 | <0.001 | 1.005 | <0.001 | 0.983 | <0.001 |
| Sex | ||||||
| Female (ref) | ||||||
| Male | 0.971 | 0.178 | 0.981 | 0.389 | 0.850 | <0.001 |
| Race | ||||||
| White (ref) | ||||||
| Asian | 0.881 | 0.053 | 0.842 | 0.013 | 0.599 | <0.001 |
| Black | 1.031 | 0.396 | 0.981 | 0.612 | 0.756 | <0.001 |
| Hispanic | 0.882 | 0.003 | 0.900 | 0.016 | 0.819 | 0.003 |
| Tumor Type | ||||||
| Primary (ref) | ||||||
| Secondary | 1.678 | <0.001 | 1.398 | <0.001 | 0.737 | <0.001 |
| Insurance Plan | ||||||
| HMO | ||||||
| EPO | 1.587 | <0.001 | 1.401 | <0.001 | 1.109 | 0.185 |
| IND | 0.274 | <0.001 | 0.299 | <0.001 | 2.166 | <0.001 |
| OTH | 2.197 | <0.001 | 0.391 | <0.001 | 0.822 | 0.003 |
| POS | 1.744 | <0.001 | 1.582 | <0.001 | 1.239 | <0.001 |
| PPO | 1.656 | <0.001 | 0.863 | <0.001 | 1.013 | 0.856 |
| Received Surgery Post-Diagnosis | 1.772 | <0.001 | 2.263 | <0.001 | 1.458 | <0.001 |
| Provider pRDI Category | ||||||
| I | ||||||
| II | 1.347 | <0.001 | 1.268 | <0.001 | 1.335 | <0.001 |
| III | 1.478 | <0.001 | 1.556 | <0.001 | 1.498 | <0.001 |
| Comorbidities | ||||||
| Congestive Heart Failure | 0.827 | 0.131 | 1.042 | 0.765 | 0.587 | 0.055 |
| Cardiac Arrhythmia | 0.951 | 0.505 | 0.881 | 0.153 | 0.840 | 0.249 |
| Valvular Disease | 1.000 | 0.999 | 1.360 | 0.019 | 1.476 | 0.056 |
| Pulmonary Circulation Disorders | 0.874 | 0.481 | 0.763 | 0.234 | 1.802 | 0.033 |
| Peripheral Vascular Disorders | 0.947 | 0.591 | 0.739 | 0.020 | 0.751 | 0.201 |
| Hypertension Uncomplicated | 0.964 | 0.344 | 0.987 | 0.763 | 0.816 | 0.005 |
| Hypertension Complicated | 1.065 | 0.613 | 0.842 | 0.262 | 0.583 | 0.058 |
| Paralysis | 0.906 | 0.672 | 1.426 | 0.112 | 1.452 | 0.207 |
| Chronic Pulmonary Disease | 1.011 | 0.851 | 1.003 | 0.957 | 0.861 | 0.164 |
| Diabetes Uncomplicated | 1.093 | 0.095 | 1.150 | 0.020 | 1.302 | 0.004 |
| Diabetes Complicated | 1.172 | 0.103 | 0.881 | 0.318 | 1.330 | 0.093 |
| Hypothyroidism | 1.066 | 0.353 | 1.075 | 0.346 | 1.093 | 0.438 |
| Renal Failure | 0.970 | 0.794 | 0.947 | 0.702 | 1.230 | 0.338 |
| Liver Disease | 1.127 | 0.301 | 1.210 | 0.122 | 0.800 | 0.315 |
| Peptic Ulcer Disease excluding bleeding | 1.692 | 0.063 | 1.132 | 0.709 | 1.388 | 0.506 |
| AIDS/HIV | 0.950 | 0.879 | 1.540 | 0.164 | 0.833 | 0.762 |
| Rheumatoid Arthritis/Collagen | 0.976 | 0.829 | 1.327 | 0.016 | 1.126 | 0.515 |
| Coagulopathy | 1.113 | 0.509 | 1.380 | 0.056 | 1.197 | 0.522 |
| Obesity | 0.989 | 0.918 | 1.019 | 0.885 | 1.437 | 0.026 |
| Weight Loss | 1.186 | 0.292 | 1.533 | 0.010 | 0.763 | 0.403 |
| Fluid and Electrolyte Disorders | 0.957 | 0.671 | 0.946 | 0.630 | 1.021 | 0.907 |
| Blood Loss Anemia | 0.640 | 0.154 | 0.913 | 0.787 | 0.453 | 0.280 |
| Deficiency Anemia | 1.009 | 0.923 | 1.180 | 0.137 | 0.945 | 0.753 |
| Alcohol Abuse | 0.736 | 0.238 | 0.891 | 0.672 | 0.830 | 0.649 |
| Drug Abuse | 0.981 | 0.945 | 1.077 | 0.803 | 0.469 | 0.152 |
| Psychoses | 1.331 | 0.131 | 0.744 | 0.244 | 2.712 | <0.001 |
| Depression | 1.118 | 0.112 | 1.142 | 0.072 | 2.775 | <0.001 |
| Characteristic | Palliative Care | Home Health Services | Social Worker Services | |||
|---|---|---|---|---|---|---|
| B | p-Value | B | p-Value | B | p-Value | |
| Year of Diagnosis | −6.284 | 0.328 | −50.284 | 0.018 | −1.836 | 0.618 |
| Age at Diagnosis (years) | 6.053 | <0.001 | −3.555 | 0.537 | 1.07 | 0.283 |
| Sex | ||||||
| Female (ref) | ||||||
| Male | −208.974 | <0.001 | −136.668 | 0.432 | −20.919 | 0.487 |
| Race | ||||||
| White (ref) | ||||||
| Asian | −71.749 | 0.648 | −513.737 | 0.324 | 169.436 | 0.060 |
| Black | 104.263 | 0.242 | −434.966 | 0.141 | −87.706 | 0.086 |
| Hispanic | 83.091 | 0.407 | −545.657 | 0.101 | −51.849 | 0.367 |
| Tumor Type | ||||||
| Primary (ref) | ||||||
| Secondary | −177.758 | 0.001 | −419.209 | 0.023 | −39.836 | 0.213 |
| Insurance Plan | ||||||
| HMO | ||||||
| EPO | −533.252 | <0.001 | −140.992 | 0.720 | −185.904 | 0.006 |
| IND | −1095.737 | <0.001 | −935.989 | 0.124 | −238.122 | 0.024 |
| OTH | 1439.161 | <0.001 | −641.019 | 0.026 | −265.996 | <0.001 |
| POS | −563.782 | <0.001 | 55.797 | 0.823 | −163.057 | <0.001 |
| PPO | 279.395 | 0.004 | −540.616 | 0.096 | −220.862 | <0.001 |
| Received Surgery Post-Diagnosis | 636.44 | <0.001 | 829.55 | <0.001 | −24.814 | 0.433 |
| Provider pRDI Category | ||||||
| I | ||||||
| II | 276.364 | <0.001 | 97.673 | 0.675 | 19.296 | 0.632 |
| III | 439.061 | <0.001 | 849.411 | <0.001 | 17.006 | 0.672 |
| Comorbidities | ||||||
| Congestive Heart Failure | −505.04 | 0.096 | −326.31 | 0.746 | −122.111 | 0.483 |
| Cardiac Arrhythmia | 125.699 | 0.500 | −84.224 | 0.891 | −33.675 | 0.752 |
| Valvular Disease | 220.38 | 0.464 | −172.757 | 0.863 | −42.285 | 0.806 |
| Pulmonary Circulation Disorders | −204.489 | 0.665 | −552.753 | 0.724 | −40.923 | 0.880 |
| Peripheral Vascular Disorders | 55.874 | 0.826 | −129.424 | 0.878 | 530.424 | <0.001 |
| Hypertension Uncomplicated | −51.218 | 0.595 | −18.985 | 0.953 | −102.452 | 0.063 |
| Hypertension Complicated | −214.48 | 0.499 | −124.797 | 0.906 | −152.06 | 0.403 |
| Paralysis | 788.05 | 0.134 | 629.979 | 0.717 | −118.86 | 0.693 |
| Chronic Pulmonary Disease | 259.933 | 0.063 | 283.419 | 0.541 | 36.887 | 0.646 |
| Diabetes Uncomplicated | 688.99 | <0.001 | 125.795 | 0.778 | −60.088 | 0.437 |
| Diabetes Complicated | 517.228 | 0.042 | −215.891 | 0.798 | 520.013 | <0.001 |
| Hypothyroidism | 243.271 | 0.159 | −187.655 | 0.743 | −79.269 | 0.424 |
| Renal Failure | −466.209 | 0.115 | 255.195 | 0.795 | −53.658 | 0.752 |
| Liver Disease | −257.867 | 0.390 | −450.065 | 0.650 | −116.873 | 0.496 |
| Peptic Ulcer Disease excluding bleeding | 377.287 | 0.623 | −1041.792 | 0.682 | 9.399 | 0.983 |
| AIDS/HIV | −297.161 | 0.710 | −1294.699 | 0.625 | −11.993 | 0.979 |
| Rheumatoid Arthritis/Collagen | 419.5 | 0.136 | 377.811 | 0.685 | 691.935 | <0.001 |
| Coagulopathy | 11.361 | 0.978 | 13257.089 | <0.001 | −24.972 | 0.916 |
| Obesity | −322.404 | 0.240 | −13.938 | 0.988 | 182.74 | 0.245 |
| Weight Loss | 748.606 | 0.072 | 31.574 | 0.982 | −73.72 | 0.757 |
| Fluid and Electrolyte Disorders | −191.583 | 0.455 | −999.169 | 0.239 | 7.816 | 0.958 |
| Blood Loss Anemia | −690.447 | 0.367 | −191.622 | 0.940 | −108.058 | 0.805 |
| Deficiency Anemia | 9.335 | 0.970 | −270.483 | 0.745 | −93.898 | 0.514 |
| Alcohol Abuse | −388.13 | 0.529 | −391.862 | 0.848 | 246.143 | 0.486 |
| Drug Abuse | 64.879 | 0.923 | −539.659 | 0.808 | −273.219 | 0.477 |
| Psychoses | 3.204 | 0.995 | −285.142 | 0.858 | 67.88 | 0.805 |
| Depression | −88.445 | 0.609 | −109.414 | 0.849 | 402.072 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jin, M.C.; Hsin, G.; Ratliff, J.; Thomas, R.; Zygourakis, C.C.; Li, G.; Wu, A. Modifiers of and Disparities in Palliative and Supportive Care Timing and Utilization among Neurosurgical Patients with Malignant Central Nervous System Tumors. Cancers 2022, 14, 2567. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102567
Jin MC, Hsin G, Ratliff J, Thomas R, Zygourakis CC, Li G, Wu A. Modifiers of and Disparities in Palliative and Supportive Care Timing and Utilization among Neurosurgical Patients with Malignant Central Nervous System Tumors. Cancers. 2022; 14(10):2567. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102567
Chicago/Turabian StyleJin, Michael Chuwei, Gary Hsin, John Ratliff, Reena Thomas, Corinna Clio Zygourakis, Gordon Li, and Adela Wu. 2022. "Modifiers of and Disparities in Palliative and Supportive Care Timing and Utilization among Neurosurgical Patients with Malignant Central Nervous System Tumors" Cancers 14, no. 10: 2567. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102567