
Adaptive Proton Therapy of Pediatric Head and Neck Cases Using MRI-Based Synthetic CTs: Initial Experience of the Prospective KiAPT Study

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Set-Up, Imaging, and Treatment Planning
2.2. Treatment, Verification Imaging, and Adaptation
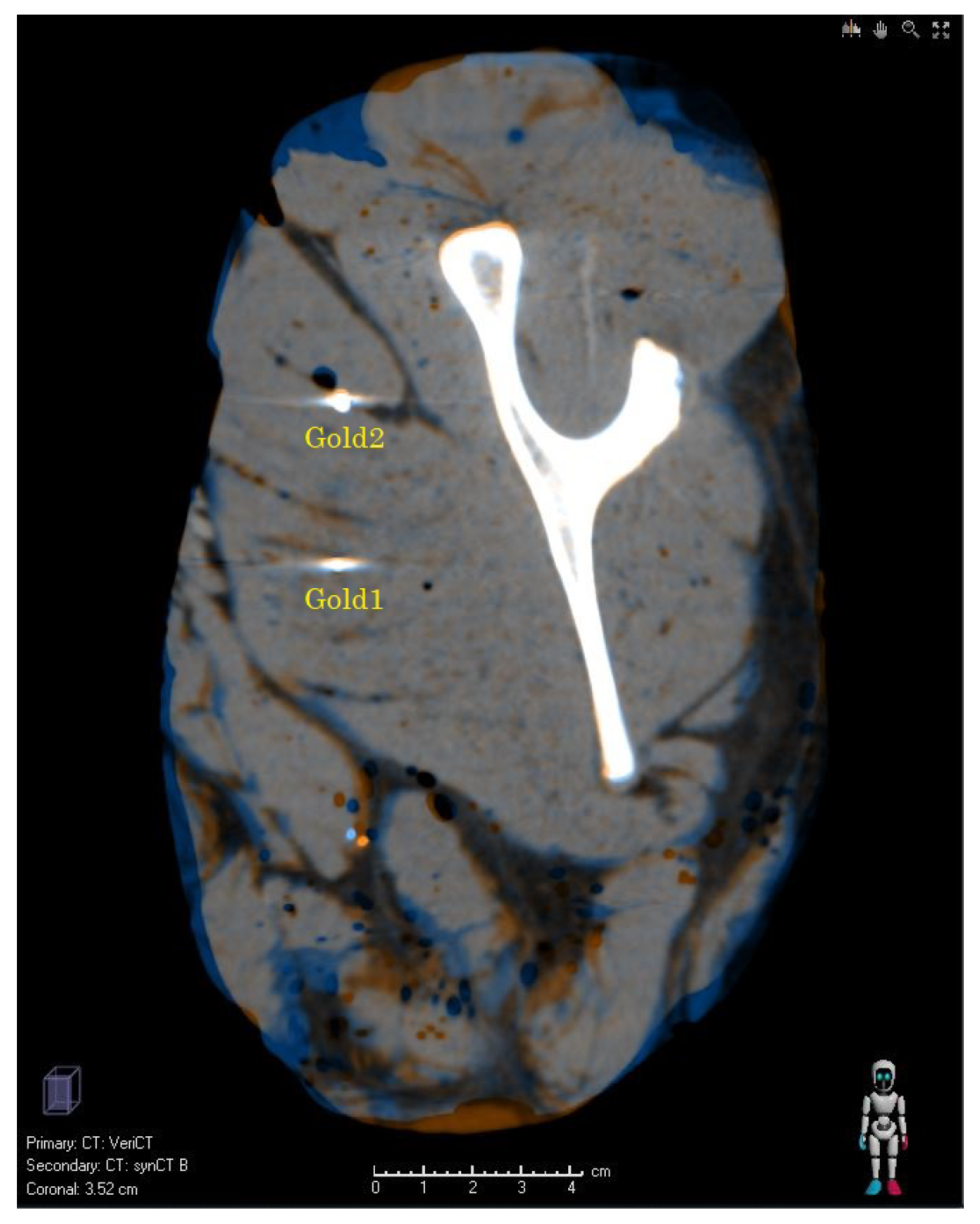
2.3. Image Processing
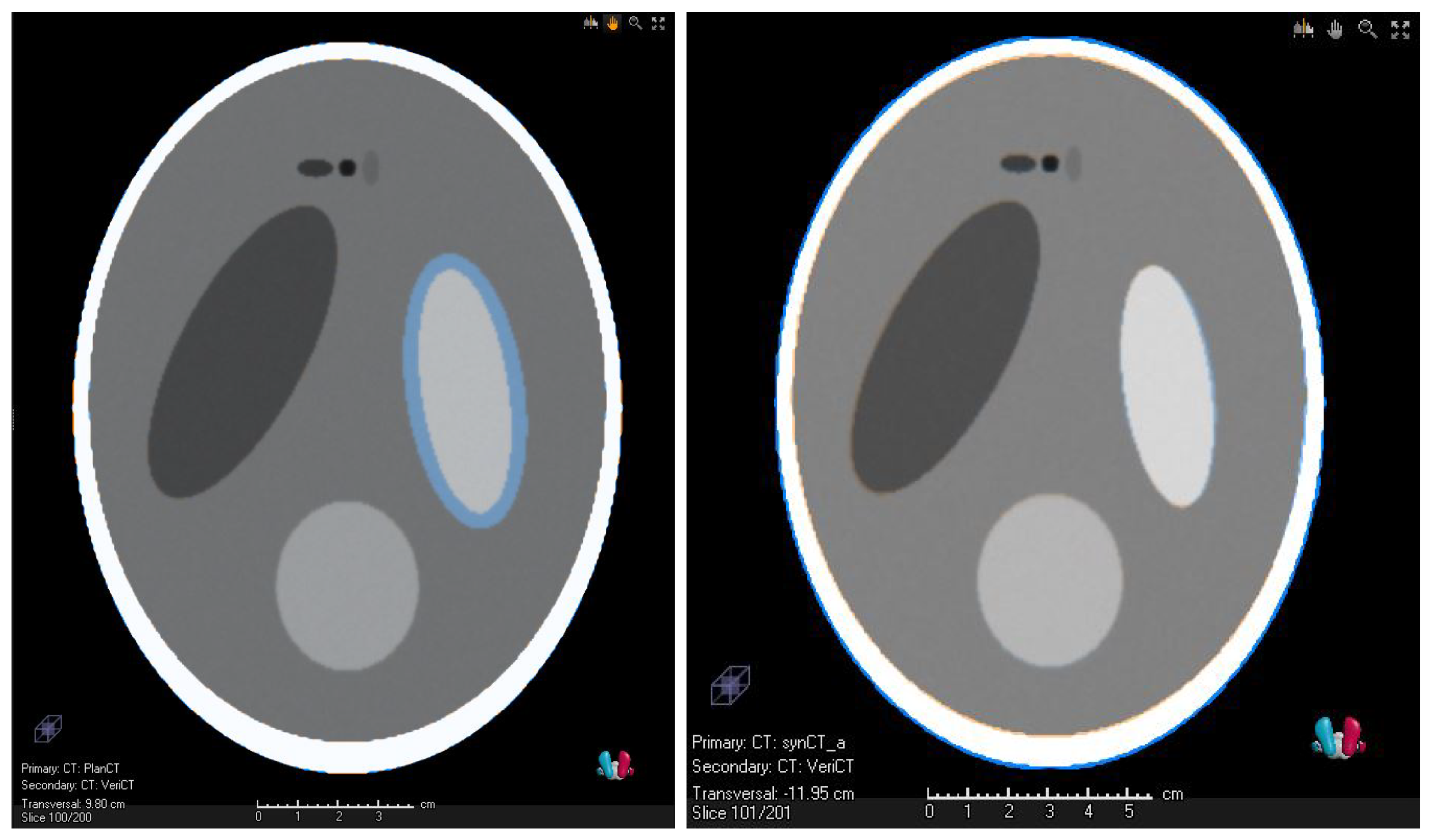
2.4. Validation of the Synthetic CTs—Methods
- A mathematical Shepp–Logan-type phantom. The similarity of the vCT and the sCT was also evaluated with the TRE (<3 mm) and additionally with the Dice similarity coefficient (DSC) (>0.85) criterion [30].
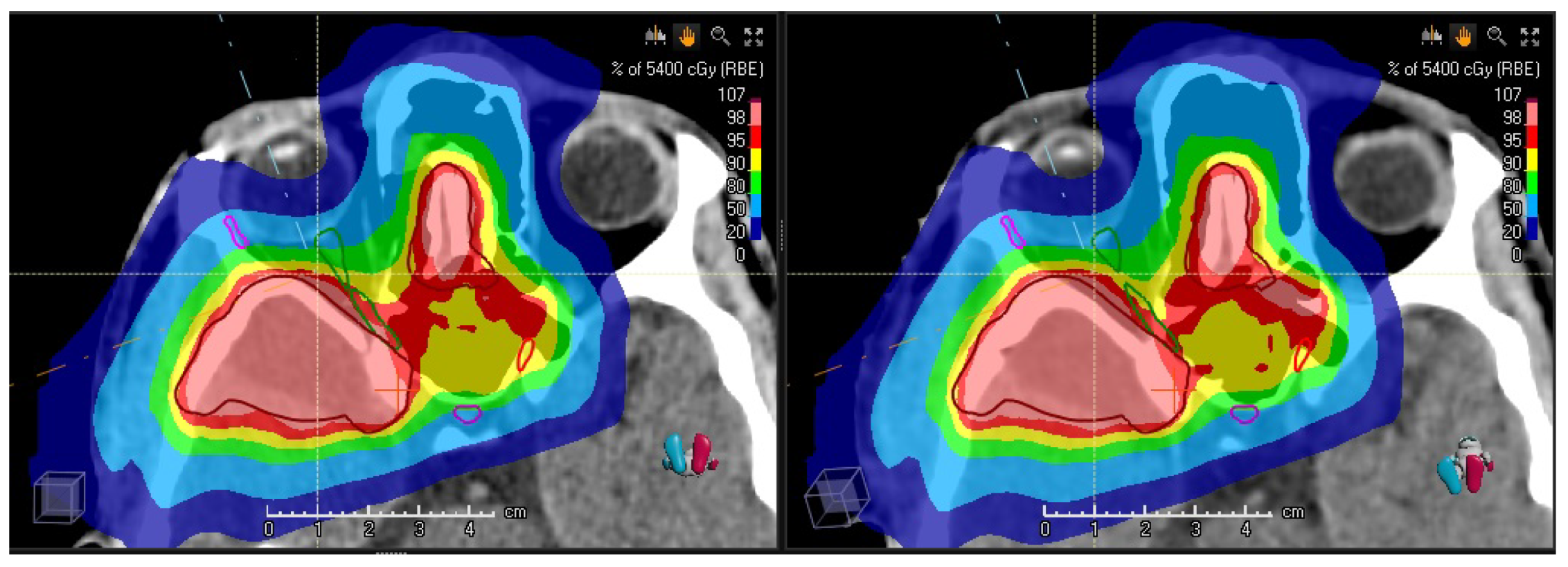
- A clinical case with a full set of planning/verification CT and MRI. A dosimetric comparison was performed.
3. Results
3.1. Validation of the Synthetic CTs—Results
3.2. Preliminary Results of the Clinical Study
4. Discussion
4.1. Clinical Impact
4.2. Comparison with Previous Studies
4.3. Validation of the Method and Technical Considerations and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| sCT | synthetic CT |
| vCT | verification CT |
| DIR | deformable image registration |
| TRE | target registration error |
| IMPT | intensity-modulated PT |
| IMRT | intensity-modulated RT |
| ROI | region of interest |
| MRI | magnetic resonance imaging |
| DSC | Dice similarity coefficient |
| DVF | deformation vector field |
| OAR | organ-at-risk |
| OARs | organs-at-risk |
| PBS | pencil beam scanning |
| PT | proton therapy |
| RT | Radiation therapy |
| ART | adaptive photon therapy |
| APT | adaptive proton therapy |
| TPS | treatment planning system |
Appendix A. Details of the Shepp–Logan Phantoms

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Soft Tissue | CT | MRT |
|---|---|---|
| Air | −1000 | 0 |
| Skin | −100 | 5500 |
| Bone | 1000 | 800 |
| Brain, gray matter | 0–25 | 1500–2300 |
| Brain, white matter | 25–50 | 2900–3600 |
| Tumor | 50 | 3600 |
| Craniospinal fluid | −5 | 1000 |
References
- Armoogum, K.S.; Thorp, N. Dosimetric Comparison and Potential for Improved Clinical Outcomes of Paediatric CNS Patients Treated with Protons or IMRT. Cancers 2015, 7, 706–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leiser, D.; Calaminus, G.; Malyapa, R.; Bojaxhiu, B.; Albertini, F.; Kliebsch, U.; Mikroutsikos, L.; Morach, P.; Bolsi, A.; Walser, M.; et al. Tumour control and Quality of Life in children with rhabdomyosarcoma treated with pencil beam scanning proton therapy. Radiother. Oncol. 2016, 120, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Albright, J.T.; Topham, A.K.; Reilly, J.S. Pediatric Head and Neck Malignancies: US Incidence and Trends Over 2 Decades. Arch. Otolaryngol.–Head Neck Surg. 2002, 128, 655–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fagerström Kristensen, I.; Nilsson, K.; Nilsson, P. Comparative Proton and Photon Treatment Planning in Pediatric Patients with Various Diagnoses. Int. J. Part. Ther. 2015, 2, 367–375. [Google Scholar] [CrossRef]
- van der Laan, H.P.; van de Water, T.A.; van Herpt, H.E.; Christianen, M.E.M.C.; Bijl, H.P.; Korevaar, E.W.; Rasch, C.R.; van ‘T Veld, A.A.; van der Schaaf, A.; Schilstra, C.; et al. The potential of intensity-modulated proton radiotherapy to reduce swallowing dysfunction in the treatment of head and neck cancer: A planning comparative study. Acta Oncol. 2013, 52, 561–569. [Google Scholar] [CrossRef]
- Eaton, B.R.; Esiashvili, N.; Kim, S.; Patterson, B.; Weyman, E.A.; Thornton, L.T.; Mazewski, C.; MacDonald, T.J.; Ebb, D.; MacDonald, S.M.; et al. Endocrine outcomes with proton and photon radiotherapy for standard risk medulloblastoma. Neuro-Oncology 2015, 18, 881–887. [Google Scholar] [CrossRef] [Green Version]
- Beetz, I.; Schilstra, C.; van der Schaaf, A.; van den Heuvel, E.R.; Doornaert, P.; van Luijk, P.; Vissink, A.; van der Laan, B.F.; Leemans, C.R.; Bijl, H.P.; et al. NTCP models for patient-rated xerostomia and sticky saliva after treatment with intensity modulated radiotherapy for head and neck cancer: The role of dosimetric and clinical factors. Radiother. Oncol. 2012, 105, 101–106. [Google Scholar] [CrossRef] [Green Version]
- Christianen, M.E.; Schilstra, C.; Beetz, I.; Muijs, C.T.; Chouvalova, O.; Burlage, F.R.; Doornaert, P.; Koken, P.W.; Leemans, C.R.; Rinkel, R.N.; et al. Predictive modelling for swallowing dysfunction after primary (chemo)radiation: Results of a prospective observational study. Radiother. Oncol. 2012, 105, 107–114. [Google Scholar] [CrossRef] [Green Version]
- Constine, L.; Ronckers, C.; Hua, C.H.; Olch, A.; Kremer, L.; Jackson, A.; Bentzen, S. Pediatric Normal Tissue Effects in the Clinic (PENTEC): An International Collaboration to Analyse Normal Tissue Radiation Dose–Volume Response Relationships for Paediatric Cancer Patients. Clin. Oncol. 2019, 31, 199–207. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, D.L.; Garden, A.S.; Thomas, J.; Chen, Y.; Zhang, Y.; Lewin, J.; Chambers, M.S.; Dong, L. Adaptive Radiotherapy for Head-and-Neck Cancer: Initial Clinical Outcomes From a Prospective Trial. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, 986–993. [Google Scholar] [CrossRef] [Green Version]
- Paganetti, H.; Botas, P.; Sharp, G.C.; Winey, B. Adaptive proton therapy. Phys. Med. Biol. 2021, 66, 22TR01. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.M.; Daly, M.E.; Cui, J.; Mathai, M.; Benedict, S.; Purdy, J.A. Clinical outcomes among patients with head and neck cancer treated by intensity-modulated radiotherapy with and without adaptive replanning. Head Neck 2014, 36, 1541–1546. [Google Scholar] [CrossRef] [PubMed]
- Surucu, M.; Shah, K.K.; Roeske, J.C.; Choi, M.; Small Jr, W.; Emami, B. Adaptive radiotherapy for head and neck cancer: Implications for clinical and dosimetry outcomes. Technol. Cancer Res. Treat. 2017, 16, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Morgan, H.E.; Sher, D.J. Adaptive radiotherapy for head and neck cancer. Cancers Head Neck 2020, 5, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Ramaekers, B.L.; Pijls-Johannesma, M.; Joore, M.A.; Van Den Ende, P.; Langendijk, J.A.; Lambin, P.; Kessels, A.G.; Grutters, J.P. Systematic review and meta-analysis of radiotherapy in various head and neck cancers: Comparing photons, carbon-ions and protons. Cancer Treat. Rev. 2011, 37, 185–201. [Google Scholar] [CrossRef] [PubMed]
- Sio, T.T.; Lin, H.K.; Shi, Q.; Gunn, G.B.; Cleeland, C.S.; Lee, J.J.; Hernandez, M.; Blanchard, P.; Thaker, N.G.; Phan, J.; et al. Intensity modulated proton therapy versus intensity modulated photon radiation therapy for oropharyngeal cancer: First comparative results of patient-reported outcomes. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 1107–1114. [Google Scholar] [CrossRef] [Green Version]
- Placidi, L.; Bolsi, A.; Lomax, A.J.; Schneider, R.A.; Malyapa, R.; Weber, D.C.; Albertini, F. Effect of Anatomic Changes on Pencil Beam Scanned Proton Dose Distributions for Cranial and Extracranial Tumors. Int. J. Radiat. Oncol. Biol. Phys. 2017, 97, 616–623. [Google Scholar] [CrossRef]
- Minatogawa, H.; Yasuda, K.; Dekura, Y.; Takao, S.; Matsuura, T.; Yoshimura, T.; Suzuki, R.; Yokota, I.; Fujima, N.; Onimaru, R.; et al. Potential benefits of adaptive intensity-modulated proton therapy in nasopharyngeal carcinomas. J. Appl. Clin. Med. Phys. 2021, 22, 174–183. [Google Scholar] [CrossRef]
- Laskar, S.; Pandit, P.; Mallik, S.; Tike, P.; Chaudhari, S.; Khanna, N.; Vora, T. Adaptive radiation therapy for pediatric head and neck malignancies: Dosimetric implications. Pract. Radiat. Oncol. 2015, 5, e87–e94. [Google Scholar] [CrossRef]
- Chin, S.; Eccles, C.L.; McWilliam, A.; Chuter, R.; Walker, E.; Whitehurst, P.; Berresford, J.; Van Herk, M.; Hoskin, P.J.; Choudhury, A. Magnetic resonance-guided radiation therapy: A review. J. Med. Imaging Radiat. Oncol. 2020, 64, 163–177. [Google Scholar] [CrossRef]
- Kraus, K.M.; Jäkel, O.; Niebuhr, N.I.; Pfaffenberger, A. Generation of synthetic CT data using patient specific daily MR image data and image registration. Phys. Med. Biol. 2017, 62, 1358–1377. [Google Scholar] [CrossRef] [PubMed]
- Bäumer, C.; Geismar, D.; Koska, B.; Kramer, P.; Lambert, J.; Lemke, M.; Plaude, S.; Pschichholz, L.; Qamhiyeh, S.; Schiemann, A.; et al. Comprehensive clinical commissioning and validation of the RayStation treatment planning system for proton therapy with active scanning and passive treatment techniques. Phys. Medica 2017, 43, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Wambersie, A. ICRU report 62, prescribing, recording and reporting photon beam therapy (supplement to ICRU Report 50). ICRU News, 1999. [Google Scholar]
- Anderton, J.; Moroz, V.; Marec-Bérard, P.; Gaspar, N.; Laurence, V.; Martín-Broto, J.; Sastre, A.; Gelderblom, H.; Owens, C.; Kaiser, S.; et al. International randomised controlled trial for the treatment of newly diagnosed EWING sarcoma family of tumours–EURO EWING 2012 Protocol. Trials 2020, 21, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behrends, C.; Haussmann, J.; Kramer, P.H.; Langendijk, J.A.; Gottschlag, H.; Geismar, D.; Budach, W.; Timmermann, B. Model-based comparison of organ at risk protection between VMAT and robustly optimised IMPT plans. Z. Für Med. Phys. 2021, 31, 5–15. [Google Scholar] [CrossRef]
- Acharya, S.; Wang, C.; Quesada, S.; Gargone, M.A.; Ates, O.; Uh, J.; Krasin, M.J.; Merchant, T.E.; ho Hua, C. Adaptive Proton Therapy for Pediatric Patients: Improving the Quality of the Delivered Plan With On-Treatment MRI. Int. J. Radiat. Oncol. Biol. Phys. 2021, 109, 242–251. [Google Scholar] [CrossRef]
- Heukelom, J.; Fuller, C.D. Head and Neck Cancer Adaptive Radiation Therapy (ART): Conceptual Considerations for the Informed Clinician. Semin. Radiat. Oncol. 2019, 29, 258–273. [Google Scholar] [CrossRef]
- Weistrand, O.; Svensson, S. The ANACONDA algorithm for deformable image registration in radiotherapy. Med. Phys. 2015, 42, 40–53. [Google Scholar] [CrossRef]
- Ger, R.B.; Yang, J.; Ding, Y.; Jacobsen, M.C.; Fuller, C.D.; Howell, R.M.; Li, H.; Jason Stafford, R.; Zhou, S.; Court, L.E. Accuracy of deformable image registration on magnetic resonance images in digital and physical phantoms. Med. Phys. 2017, 44, 5153–5161. [Google Scholar] [CrossRef]
- Brock, K.K.; Mutic, S.; McNutt, T.R.; Li, H.; Kessler, M.L. Use of image registration and fusion algorithms and techniques in radiotherapy: Report of the AAPM Radiation Therapy Committee Task Group No. 132. Med. Phys. 2017, 44, 43–76. [Google Scholar] [CrossRef] [Green Version]
- Bolan, P. 3D Shepp–Logan Phantom. 2020. Available online: https://www.mathworks.com/matlabcentral/fileexchange/9416-3d-shepp-logan-phantom (accessed on 30 August 2020).
- Pearce, M.S.; Salotti, J.A.; Little, M.P.; McHugh, K.; Lee, C.; Kim, K.P.; Howe, N.L.; Ronckers, C.M.; Rajaraman, P.; Craft, A.W.; et al. Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: A retrospective cohort study. Lancet 2012, 380, 499–505. [Google Scholar] [CrossRef] [Green Version]
- Korevaar, E.W.; Habraken, S.J.; Scandurra, D.; Kierkels, R.G.; Unipan, M.; Eenink, M.G.; Steenbakkers, R.J.; Peeters, S.G.; Zindler, J.D.; Hoogeman, M.; et al. Practical robustness evaluation in radiotherapy – A photon and proton-proof alternative to PTV-based plan evaluation. Radiother. Oncol. 2019, 141, 267–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simone, C.B., II; Ly, D.; Dan, T.D.; Ondos, J.; Ning, H.; Belard, A.; O’Connell, J.; Miller, R.W.; Simone, N.L. Comparison of intensity-modulated radiotherapy, adaptive radiotherapy, proton radiotherapy, and adaptive proton radiotherapy for treatment of locally advanced head and neck cancer. Radiother. Oncol. 2011, 101, 376–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volpe, S.; Bondiau, P.Y.; Claude, L.; Claren, A.; Padovani, L.; AlGhamdi, H.; Duhil De Benaze, G.; Opitz, L.; Baudin, G.; Dejean, C.; et al. Postsurgical geometrical variations of tumor bed and brainstem during photon and proton therapy for pediatric tumors of the posterior fossa: Dosimetric impact and predictive factors. Strahlenther. Und Onkol. 2021, 197, 1113–1123. [Google Scholar] [CrossRef] [PubMed]
- Hague, C.; Aznar, M.; Dong, L.; Fotouhi-Ghiam, A.; Lee, L.W.; Li, T.; Lin, A.; Lowe, M.; Lukens, J.N.; McPartlin, A.; et al. Inter-fraction robustness of intensity-modulated proton therapy in the post-operative treatment of oropharyngeal and oral cavity squamous cell carcinomas. Br. J. Radiol. 2020, 93, 20190638. [Google Scholar] [CrossRef] [PubMed]
- Vidal, M.; Moignier, C.; Patriarca, A.; Sotiropoulos, M.; Schneider, T.; De Marzi, L. Future technological developments in proton therapy—A predicted technological breakthrough. Cancer/Radiothérapie 2021, 25, 554–564. [Google Scholar] [CrossRef]
- Price, J.; Hall, E.; West, C.; Thomson, D. TORPEdO—A Phase III Trial of Intensity-modulated Proton Beam Therapy Versus Intensity-modulated Radiotherapy for Multi-toxicity Reduction in Oropharyngeal Cancer. Clin. Oncol. 2020, 32, 84–88. [Google Scholar] [CrossRef] [Green Version]
- Aly, F.; Miller, A.A.; Jameson, M.G.; Metcalfe, P.E. A prospective study of weekly intensity modulated radiation therapy plan adaptation for head and neck cancer: Improved target coverage and organ at risk sparing. Australas. Phys. Eng. Sci. Med. 2019, 42, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Rathod, H.; Mehta, M.; Kichloo, A.; Mankada, S.; Shah, R. Adaptive Radiotherapy in Orbital Rhabdomyosarcoma: A Case Report. J. Med. Sci. Clin. Res. 2020, 08, 439–442. [Google Scholar] [CrossRef]
- Shusharina, N.; Chan, A.; Adams, J.; Chen, G.; Sharp, G. Adaptive Proton Radiation Therapy for Base of Skull Tumors. Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, S803. [Google Scholar] [CrossRef]
- Lamiman, K.; Wong, K.K.; Tamrazi, B.; Nosrati, J.D.; Olch, A.; Chang, E.L.; Kiehna, E.N. A quantitative analysis of craniopharyngioma cyst expansion during and after radiation therapy and surgical implications. Neurosurg. Focus FOC 2016, 41, E15. [Google Scholar] [CrossRef] [Green Version]
- Ajithkumar, T.; Mazhari, A.L.; Stickan-Verfürth, M.; Kramer, P.H.; Fuentes, C.S.; Lambert, J.; Thomas, H.; Müller, H.; Fleischhack, G.; Timmermann, B. Proton Therapy for Craniopharyngioma—An Early Report from a Single European Centre. Clin. Oncol. 2018, 30, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Elter, A.; Dorsch, S.; Mann, P.; Runz, A.; Johnen, W.; Spindeldreier, C.K.; Klüter, S.; Karger, C.P. End-to-end test of an online adaptive treatment procedure in MR-guided radiotherapy using a phantom with anthropomorphic structures. Phys. Med. Biol. 2019, 64, 225003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meschini, G.; Vai, A.; Paganelli, C.; Molinelli, S.; Fontana, G.; Pella, A.; Preda, L.; Vitolo, V.; Valvo, F.; Ciocca, M.; et al. Virtual 4DCT from 4DMRI for the management of respiratory motion in carbon ion therapy of abdominal tumors. Med. Phys. 2020, 47, 909–916. [Google Scholar] [CrossRef] [PubMed]
- Wissmann, L.; Santelli, C.; Segars, W.P.; Kozerke, S. MRXCAT: Realistic numerical phantoms for cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2014, 16, 64. [Google Scholar] [CrossRef]
- Putz, F.; Mengling, V.; Perrin, R.; Masitho, S.; Weissmann, T.; Rösch, J.; Bäuerle, T.; Janka, R.; Cavallaro, A.; Uder, M.; et al. Magnetic resonance imaging for brain stereotactic radiotherapy. Strahlenther. Und Onkol. 2020, 196, 444–456. [Google Scholar] [CrossRef] [Green Version]
- Mengling, V.; Bert, C.; Perrin, R.; Masitho, S.; Weissmann, T.; Mansoorian, S.; Siavooshhaghighi, H.; Janka, R.; Doussin, S.; Habatsch, M.; et al. Implementation of a dedicated 1.5 T MR scanner for radiotherapy treatment planning featuring a novel high-channel coil setup for brain imaging in treatment position. Strahlenther. Und Onkol. 2021, 197, 246–256. [Google Scholar] [CrossRef]
- Stanescu, T.; Hans-Sonke, J.; Stavrev, P.; Fallone, B.G. 3T MR-based treatment planning for radiotherapy of brain lesions. Radiol. Oncol. 2006, 40, 125–132. [Google Scholar]
- Slagowski, J.; Ding, Y.; Wen, Z.; Fuller, C.; Chung, C.; Kadbi, M.; Ibbott, G.; Wang, J. Quantification of Geometric Distortion in Magnetic Resonance Imaging for Radiation Therapy Treatment Planning. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, e547. [Google Scholar] [CrossRef]
- Pappas, E.P.; Alshanqity, M.; Moutsatsos, A.; Lababidi, H.; Alsafi, K.; Georgiou, K.; Karaiskos, P.; Georgiou, E. MRI-Related Geometric Distortions in Stereotactic Radiotherapy Treatment Planning: Evaluation and Dosimetric Impact. Technol. Cancer Res. Treat. 2017, 16, 1120–1129. [Google Scholar] [CrossRef] [Green Version]
- Ulin, K.; Urie, M.M.; Cherlow, J.M. Results of a Multi-Institutional Benchmark Test for Cranial CT/MR Image Registration. Int. J. Radiat. Oncol. Biol. Phys. 2010, 77, 1584–1589. [Google Scholar] [CrossRef] [Green Version]
- Price, R.G.; Knight, R.A.; Hwang, K.P.; Bayram, E.; Nejad-Davarani, S.P.; Glide-Hurst, C.K. Optimization of a novel large field of view distortion phantom for MR-only treatment planning. J. Appl. Clin. Med. Phys. 2017, 18, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Handrack, J.; Bangert, M.; Möhler, C.; Bostel, T.; Greilich, S. Towards a generalised development of synthetic CT images and assessment of their dosimetric accuracy. Acta Oncol. 2020, 59, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Koivula, L.; Wee, L.; Korhonen, J. Feasibility of MRI-only treatment planning for proton therapy in brain and prostate cancers: Dose calculation accuracy in substitute CT images. Med. Phys. 2016, 43, 4634–4642. [Google Scholar] [CrossRef] [PubMed]
- Boye, D.; Lomax, T.; Knopf, A. Mapping motion from 4D-MRI to 3D-CT for use in 4D dose calculations: A technical feasibility study. Med. Phys. 2013, 40. [Google Scholar] [CrossRef] [PubMed]
- Dolde, K.; Naumann, P.; Dávid, C.; Gnirs, R.; Kachelrieß, M.; Lomax, A.J.; Saito, N.; Weber, D.C.; Pfaffenberger, A.; Zhang, Y. 4D dose calculation for pencil beam scanning proton therapy of pancreatic cancer using repeated 4DMRI datasets. Phys. Med. Biol. 2018, 63. [Google Scholar] [CrossRef] [PubMed]
- Neppl, S.; Landry, G.; Kurz, C.; Hansen, D.C.; Hoyle, B.; Stöcklein, S.; Seidensticker, M.; Weller, J.; Belka, C.; Parodi, K.; et al. Evaluation of proton and photon dose distributions recalculated on 2D and 3D Unet-generated pseudoCTs from T1-weighted MR head scans. Acta Oncol. 2019, 58, 1429–1434. [Google Scholar] [CrossRef] [PubMed]
- Spadea, M.F.; Pileggi, G.; Zaffino, P.; Salome, P.; Catana, C.; Izquierdo-Garcia, D.; Amato, F.; Seco, J. Deep Convolution Neural Network (DCNN) Multiplane Approach to Synthetic CT Generation From MR images—Application in Brain Proton Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, 495–503. [Google Scholar] [CrossRef]
- Hoffmann, A.; Oborn, B.; Moteabbed, M.; Yan, S.; Bortfeld, T.; Knopf, A.; Fuchs, H.; Georg, D.; Seco, J.; Spadea, M.F.; et al. MR-guided proton therapy: A review and a preview. Radiat. Oncol. 2020, 15, 1–13. [Google Scholar] [CrossRef]
- Wang, C.; Uh, J.; Merchant, T.E.; Hua, C.h.; Acharya, S. Facilitating MR-Guided Adaptive Proton Therapy in Children Using Deep Learning-Based Synthetic CT. Int. J. Part. Ther. 2021, 8, 11–20. [Google Scholar] [CrossRef]
- Spadea, M.F.; Maspero, M.; Zaffino, P.; Seco, J. Deep learning based synthetic-CT generation in radiotherapy and PET: A review. Med. Phys. 2021, 48, 6537–6566. [Google Scholar] [CrossRef]
- Bäumer, C.; Bäcker, C.M.; Conti, M.; Fragoso Costa, P.; Herrmann, K.; Kazek, S.L.; Jentzen, W.; Panin, V.; Siegel, S.B.; Teimoorisichani, M.; et al. Can a ToF-PET photon attenuation reconstruction test stopping power estimations in proton therapy? A phantom study. Phys. Med. Biol. 2021, 66, 215010. [Google Scholar] [CrossRef] [PubMed]




| Quantity | ROI | Unit | rCT | vCT | sCT | Clinical Goal |
|---|---|---|---|---|---|---|
| PTV | % | 98.3 | 96.7 | 96.8 | 95.0 | |
| PTV | GyRBE | 55.7 | 55.7 | 55.8 | 57.8 | |
| PTV | GyRBE | 54.0 | 53.9 | 53.9 | ≈54 | |
| right optical nerve | GyRBE | 52.5 | 53.3 | 52.5 | 56.0 | |
| left optical nerve | GyRBE | 52.5 | 52.1 | 52.1 | 56.0 | |
| chiasm | GyRBE | 52.3 | 51.8 | 51.7 | 56.0 | |
| pituitary | GyRBE | 38.5 | 38.6 | 37.6 | 40 |
| Median Age (Range) | 6.9 Years (Range, 1.5–16 Years) |
|---|---|
| Gender | |
| Male | 6 pts (55%) |
| Female | 5 pts (45%) |
| Site | |
| Craniofacial | 7 pts (64%) |
| Base of skull | 2 pts (18%) |
| Other site | 2 pts (18%) |
| Histology | |
| Rabdomyosarcom | 8 pts ( 73%) |
| Other histotype | 3 pts ( 27%) |
| Treatment before PT | |
| Chemotherapy | 8 pts ( 73%) |
| Surgery | 6 pts ( 55%) |
| N Stage | |
| N0 | 10 pts (91%) |
| cN+ | 1 pt (9%) |
| Median prescribed dose (range) | 55.5 GyRBE (50–69.3 GyRBE) |
| OAR | Median Dose on Reference CT (Range) | Median Dose on sCT (Range) |
|---|---|---|
| (GyRBE) | (GyRBE) | |
| Spinal cord | ||
| 20.5 (0.06–48.7) | 24.8 (0.06–48.2) | |
| 22.7 (0.08–49.7 ) | 28.1 (0.07–49.2) | |
| Brainstem | ||
| 31.9 (0.5–54.3) | 31.8 (0.5–54.2) | |
| 34.8 (0.9–55.5) | 34.7 (0.9–55.4) | |
| Optic chiasm | ||
| 9.9 (0.4–54.7) | 9.4 (0.5–54.7) | |
| 8.9 (0.4–54.7) | 8.3 (0.4–54.6) | |
| Optic nerve (right) | ||
| 34.6 (1.9–55.4) | 34.7 (1.8–55.3) | |
| 33.3 (1.9–56.4) | 33.3 (1.8–56.5) | |
| Optic nerve (left) | ||
| 18 (0.1–53.3) | 17.9 (0.1–53.5) | |
| 18 (0.1–53.4) | 17.9 (0.1–53.5) | |
| Parotid gland (mean) | ||
| Right | 38.8 (0.2–51.7) | 38.7 (0.2–51.8) |
| Left | 0.9 (0–52.1) | 1.1 (0–52) |
| Submandibular gland (mean) | ||
| Right | 28.4 (0.04–57.2) | 29.1 (0.04–57.1) |
| Left | 5.2 (0–50.4) | 5.2 (0–50.4) |
| Cochlea | ||
| Right (mean) | 26.8 (0.9–59.7) | 26.6 (0.9–59.8) |
| Left (mean) | 1.3 (0–37.2) | 1.03 (0–36) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bäumer, C.; Frakulli, R.; Kohl, J.; Nagaraja, S.; Steinmeier, T.; Worawongsakul, R.; Timmermann, B. Adaptive Proton Therapy of Pediatric Head and Neck Cases Using MRI-Based Synthetic CTs: Initial Experience of the Prospective KiAPT Study. Cancers 2022, 14, 2616. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14112616
Bäumer C, Frakulli R, Kohl J, Nagaraja S, Steinmeier T, Worawongsakul R, Timmermann B. Adaptive Proton Therapy of Pediatric Head and Neck Cases Using MRI-Based Synthetic CTs: Initial Experience of the Prospective KiAPT Study. Cancers. 2022; 14(11):2616. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14112616
Chicago/Turabian StyleBäumer, Christian, Rezarta Frakulli, Jessica Kohl, Sindhu Nagaraja, Theresa Steinmeier, Rasin Worawongsakul, and Beate Timmermann. 2022. "Adaptive Proton Therapy of Pediatric Head and Neck Cases Using MRI-Based Synthetic CTs: Initial Experience of the Prospective KiAPT Study" Cancers 14, no. 11: 2616. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14112616