
The Role of Human Chorionic Gonadotropin Beta (hCGβ) in HPV-Positive and HPV-Negative Oropharyngeal Squamous Cell Carcinoma

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. S-hCGβ Determination
2.3. Tumor Slides
2.4. hCGβ Immunohistochemistry
2.5. Data Analysis
3. Results
3.1. Clinical Characteristics and S-hCGβ
3.2. Clinical Characteristics and hCGβ IHC
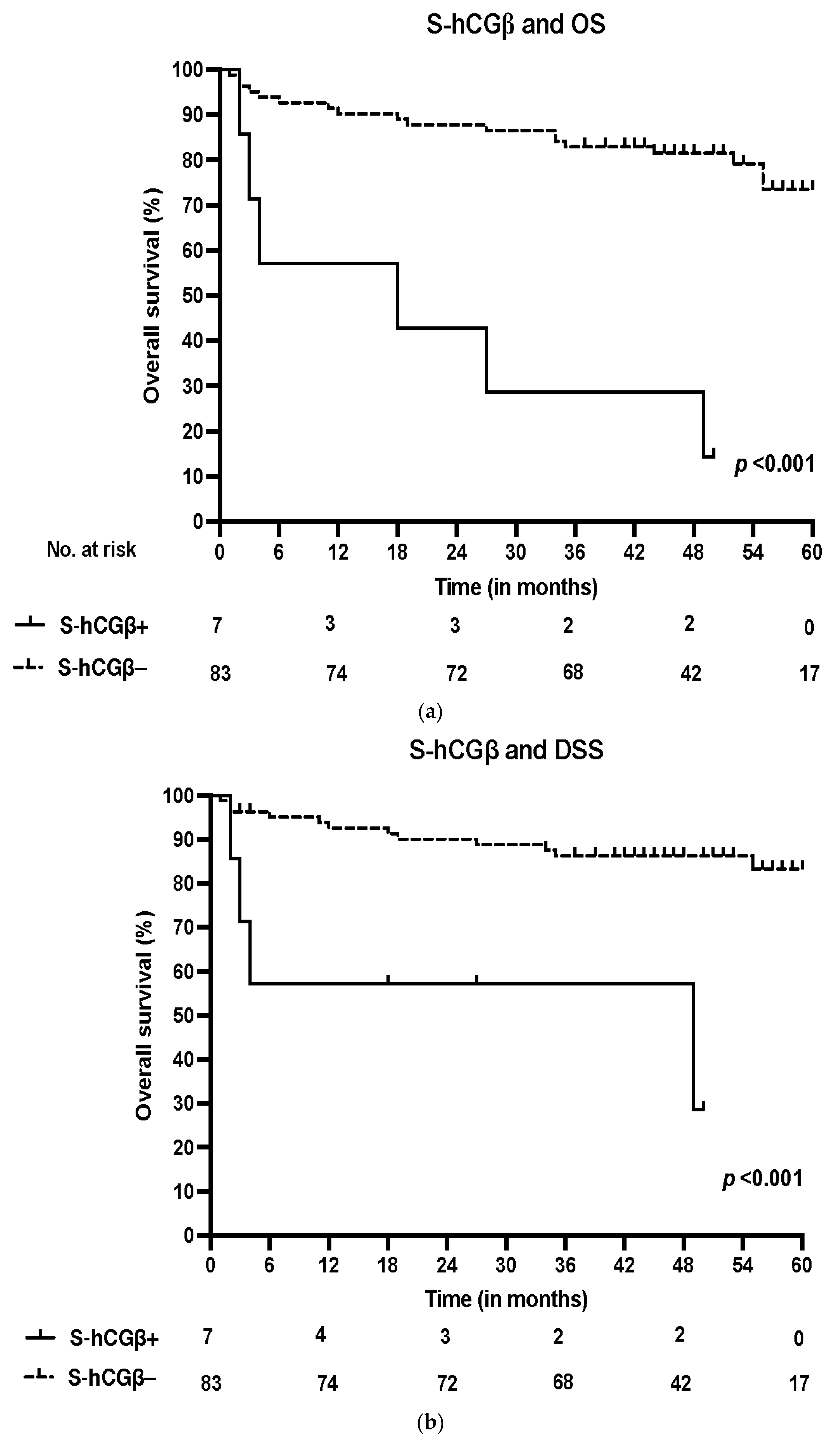
3.3. Survival and S-hCGβ
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ernster, J.A.; Sciotto, C.G.; O’Brien, M.M.; Finch, J.L.; Robinson, L.J.; Willson, T.; Mathews, M. Rising incidence of oropharyngeal cancer and the role of oncogenic human papilloma virus. Laryngoscope 2007, 117, 2115–2128. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Berman, T.A.; Schiller, J.T. Human papillomavirus in cervical cancer and oropharyngeal cancer: One cause, two diseases. Cancer 2017, 123, 2219–2229. [Google Scholar] [CrossRef]
- Gillison, M.L.; Koch, W.M.; Capone, R.B.; Spafford, M.; Westra, W.H.; Wu, L.; Zahurak, M.L.; Daniel, R.W.; Viglione, M.; Symer, D.E.; et al. Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. J. Natl. Cancer Inst. 2000, 92, 709–720. [Google Scholar] [CrossRef]
- Lewis, J.S. Chapter 10: Malignant Neoplasms of the Oropharynx. In Head and Neck Pathology, 3rd ed.; Thompson, L.D.R., Bishop, J.A., Eds.; Elsevier: Philadelphia, PA, USA, 2019; pp. 230–240.e1. [Google Scholar]
- Allen, C.T.; Lewis, J.S., Jr.; El-Mofty, S.K.; Haughey, B.H.; Nussenbaum, B. Human papillomavirus and oropharynx cancer: Biology, detection and clinical implications. Laryngoscope 2010, 120, 1756–1772. [Google Scholar] [CrossRef]
- Li, Y.; Jiang, B.; Huang, M.; Wang, G.; Bai, Y.; Huang, W. Retrospective study of the clinicopathological characteristics and prognosis of elderly patients with oropharyngeal squamous cell carcinoma. J. Int. Med. Res. 2021, 49, 3000605211016662. [Google Scholar] [CrossRef]
- Haughey, B.H.; Sinha, P. Prognostic factors and survival unique to surgically treated p16+ oropharyngeal cancer. Laryngoscope 2012, 122 (Suppl. S2), S13–S33. [Google Scholar] [CrossRef]
- Mann, K.; Saller, B.; Hoermann, R. Clinical use of HCG and hCG beta determinations. Scand. J. Clin. Lab. Investig. Suppl. 1993, 216, 97–104. [Google Scholar] [CrossRef]
- Cole, L.A. Biological functions of hCG and hCG-related molecules. Reprod. Biol. Endocrinol. 2010, 8, 102. [Google Scholar] [CrossRef] [Green Version]
- Stenman, U.H.; Tiitinen, A.; Alfthan, H.; Valmu, L. The classification, functions and clinical use of different isoforms of HCG. Hum. Reprod. Update 2006, 12, 769–784. [Google Scholar] [CrossRef]
- Marcillac, I.; Troalen, F.; Bidart, J.M.; Ghillani, P.; Ribrag, V.; Escudier, B.; Malassagne, B.; Droz, J.P.; Lhommé, C.; Rougier, P.; et al. Free human chorionic gonadotropin beta subunit in gonadal and nongonadal neoplasms. Cancer Res. 1992, 52, 3901–3907. [Google Scholar]
- Gehring, C.; Siepmann, T.; Heidegger, H.; Jeschke, U. The controversial role of human chorionic gonadotropin in the development of breast cancer and other types of tumors. Breast 2016, 26, 135–140. [Google Scholar] [CrossRef]
- Lyytinen, I.; Lempinen, M.; Nordin, A.; Mäkisalo, H.; Stenman, U.H.; Isoniemi, H. Prognostic significance of tumor-associated trypsin inhibitor (TATI) and human chorionic gonadotropin-β (hCGβ) in patients with hepatocellular carcinoma. Scand. J. Gastroenterol. 2013, 48, 1066–1073. [Google Scholar] [CrossRef]
- Stenman, U.H.; Alfthan, H.; Hotakainen, K. Human chorionic gonadotropin in cancer. Clin. Biochem. 2004, 37, 549–561. [Google Scholar] [CrossRef]
- Hedström, J.; Grenman, R.; Ramsay, H.; Finne, P.; Lundin, J.; Haglund, C.; Alfthan, H.; Stenman, U.H. Concentration of free hCGbeta subunit in serum as a prognostic marker for squamous-cell carcinoma of the oral cavity and oropharynx. Int. J. Cancer 1999, 84, 525–528. [Google Scholar] [CrossRef]
- Bhalang, K.; Kafrawy, A.H.; Miles, D.A. Immunohistochemical study of the expression of human chorionic gonadotropin-beta in oral squamous cell carcinoma. Cancer 1999, 85, 757–762. [Google Scholar] [CrossRef]
- Meda, S.; Reginald, B.A.; Reddy, B.S. Immunohistochemical study of the expression of human chorionic gonadotropin-β in salivary gland tumors. Cancer Res. Ther. 2018, 14, 952–956. [Google Scholar]
- Carpén, T.; Sjöblom, A.; Lundberg, M.; Haglund, C.; Markkola, A.; Syrjänen, S.; Tarkkanen, J.; Mäkitie, A.; Hagström, J.; Mattila, P. Presenting symptoms and clinical findings in HPV-positive and HPV-negative oropharyngeal cancer patients. Acta Oto-Laryngol. 2018, 138, 513–518. [Google Scholar] [CrossRef] [Green Version]
- Sjöblom, A.; Stenman, U.H.; Hagström, J.; Jouhi, L.; Haglund, C.; Syrjänen, S.; Mattila, P.; Mäkitie, A.; Carpén, T. Tumor-Associated Trypsin Inhibitor (TATI) as a Biomarker of Poor Prognosis in Oropharyngeal Squamous Cell Carcinoma Irrespective of HPV Status. Cancers 2021, 13, 2811. [Google Scholar] [CrossRef]
- Alfthan, H.; Haglund, C.; Dabek, J.; Stenman, U.H. Concentrations of human choriogonadotropin, its beta-subunit, and the core fragment of the beta-subunit in serum and urine of men and nonpregnant women. Clin. Chem. 1992, 38, 1981–1987. [Google Scholar] [CrossRef]
- Vartiainen, J.; Lehtovirta, P.; Finne, P.; Stenman, U.H.; Alfthan, H. Preoperative serum concentration of hCGbeta as a prognostic factor in ovarian cancer. Int. J. Cancer 2001, 95, 313–316. [Google Scholar]
- Louhimo, J.; Kokkola, A.; Alfthan, H.; Stenman, U.H.; Haglund, C. Preoperative hCGbeta and CA 72-4 are prognostic factors in gastric cancer. Int. J. Cancer 2004, 111, 929–933. [Google Scholar] [CrossRef]
- Louhimo, J.; Nordling, S.; Alfthan, H.; von Boguslawski, K.; Stenman, U.H.; Haglund, C. Specific staining of human chorionic gonadotropin beta in benign and malignant gastrointestinal tissues with monoclonal antibodies. Histopathology 2001, 38, 418–424. [Google Scholar] [CrossRef]
- Hotakainen, K.; Ljungberg, B.; Haglund, C.; Nordling, S.; Paju, A.; Stenman, U.H. Expression of the free beta-subunit of human chorionic gonadotropin in renal cell carcinoma: Prognostic study on tissue and serum. Int. J. Cancer 2003, 104, 631–635. [Google Scholar] [CrossRef]
- Stewart, J.A.; Koistinen, R.; Lempiäinen, A.; Hotakainen, K.; Salminen, U.S.; Vakkuri, A.; Wennervirta, J.; Stenman, U.H.; Koistinen, H. Dramatic increase in serum trypsinogens, SPINK1 and hCGβ in aortic surgery patients after hypothermic circulatory arrest. Scand. J. Clin. Lab. Investig. 2020, 80, 640–643. [Google Scholar] [CrossRef]
- Braunstein, G.D. False-positive serum human chorionic gonadotropin results: Causes, characteristics, and recognition. Am. J. Obstet. Gynecol. 2002, 187, 217–224. [Google Scholar] [CrossRef]
- Wu, W.; Gao, H.; Li, X.; Peng, S.; Yu, J.; Liu, N.; Zhan, G.; Zhu, Y.; Wang, K.; Guo, X. β-hCG promotes epithelial ovarian cancer metastasis through ERK/MMP2 signaling pathway. Cell Cycle 2019, 18, 46–59. [Google Scholar] [CrossRef]
- Li, D.; Wen, X.; Ghali, L.; Al-Shalabi, F.M.; Docherty, S.M.; Purkis, P.; Iles, R.K. hCG beta expression by cervical squamous carcinoma—In vivo histological association with tumour invasion and apoptosis. Histopathology 2008, 53, 147–155. [Google Scholar] [CrossRef]
- Acevedo, H.F.; Krichevsky, A.; Campbell-Acevedo, E.A.; Galyon, J.C.; Buffo, M.J.; Hartsock, R.J. Expression of membrane-associated human chorionic gonadotropin, its subunits, and fragments by cultured human cancer cells. Cancer 1992, 69, 1829–1842. [Google Scholar] [CrossRef]
- Gillott, D.J.; Iles, R.K.; Chard, T. The effects of beta-human chorionic gonadotrophin on the in vitro growth of bladder cancer cell lines. Br. J. Cancer 1996, 3, 323–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Been, M.J.; Watkins, J.; Manz, R.M.; Gentry, L.R.; Leverson, G.E.; Harari, P.M.; Hartig, G.K. Tumor volume as a prognostic factor in oropharyngeal squamous cell carcinoma treated with primary radiotherapy. Laryngoscope 2008, 118, 1377–1382. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, J.P.; Mallick, I.; Bhutani, R.; Ghosh-Laskar, S.; Gupta, T.; Budrukkar, A.; Murthy, V.; Sengar, M.; Dinshaw, K.A. Prognostic factors in oropharyngeal cancer—Analysis of 627 cases receiving definitive radiotherapy. Acta Oncol. 2009, 48, 1026–1033. [Google Scholar] [CrossRef] [PubMed]
- Butler, S.A.; Iles, R.K. The free monomeric beta subunit of human chorionic gonadotrophin (hCG beta) and the recently identified homodimeric beta-beta subunit (hCG beta beta) both have autocrine growth effects. Tumor Biol. 2004, 25, 18–23. [Google Scholar] [CrossRef]
- Hirata, F.; Axelrod, J. Phospholipid methylation and biological signal transmission. Science 1980, 209, 1082–1090. [Google Scholar] [CrossRef]
- Abramovitch, R.; Tavor, E.; Jacob-Hirsch, J.; Zeira, E.; Amariglio, N.; Pappo, O.; Rechavi, G.; Galun, E.; Honigman, A. A pivotal role of cyclic AMP-responsive element binding protein in tumor progression. Cancer Res. 2004, 64, 1338–1346. [Google Scholar] [CrossRef] [Green Version]
- Simpson, B.J.; Ramage, A.D.; Hulme, M.J.; Burns, D.J.; Katsaros, D.; Langdon, S.P.; Miller, W.R. Cyclic adenosine 3′,5′-monophosphate-binding proteins in human ovarian cancer: Correlations with clinicopathological features. Clin. Cancer Res. 1996, 2, 201–206. [Google Scholar]
- Tiwari, R.; Manzar, N.; Bhatia, V.; Yadav, A.; Nengroo, M.A.; Datta, D.; Carskadon, S.; Gupta, N.; Sigouros, M.; Khani, F.; et al. Androgen deprivation upregulates SPINK1 expression and potentiates cellular plasticity in prostate cancer. Nat. Commun. 2020, 11, 384. [Google Scholar] [CrossRef] [Green Version]
- Liu, N.; Peng, S.M.; Zhan, G.X.; Yu, J.; Wu, W.M.; Gao, H.; Li, X.F.; Guo, X.Q. Human chorionic gonadotropin β regulates epithelial-mesenchymal transition and metastasis in human ovarian cancer. Oncol. Rep. 2017, 38, 1464–1472. [Google Scholar] [CrossRef] [Green Version]
- Singh, P.; Chalertpet, K.; Sukbhattee, J.; Wongmanee, N.; Suwannakart, P.; Yanatatsaneejit, P. Association between promoter methylation and gene expression of CGB3 and NOP56 in HPV-infected cervical cancer cells. Biomed. Rep. 2022, 16, 1. [Google Scholar] [CrossRef]
- Handwerger, S.; Wilson, S.P.; Tyrey, L.; Conn, P.M. Biochemical evidence that human placental lactogen and human chorionic gonadotropin are not stored in cytoplasmic secretion granules. Biol. Reprod. 1987, 37, 28–32. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variable. | S-hCGβ+ | % | S-hCGβ− | % | p-Value | Missing/% |
|---|---|---|---|---|---|---|
| Number of patients | 7 | 7.8 | 83 | 92.2 | ||
| Mean age at diagnosis | 64.5 | 61.4 | 0.156 | |||
| Gender | ||||||
| Male | 5 | 70.6 | 61 | 92.4 | ||
| Female | 2 | 8.3 | 22 | 91.7 | 0.906 | |
| Smoking | ||||||
| Non-smoker | 1 | 3.6 | 27 | 96.4 | ||
| Ex-smoker | 2 | 6.7 | 28 | 93.3 | ||
| Current smoker | 4 | 12.5 | 28 | 87.5 | 0.554 | |
| Heavy alcohol use | ||||||
| Non-drinker | 2 | 4.7 | 41 | 95.3 | ||
| Ex-drinker | 1 | 10.0 | 9 | 90.0 | ||
| Current drinker | 3 | 14.3 | 18 | 85.7 | 0.383 | 16/17.8 |
| T class | ||||||
| T1–T2 | 3 | 5.2 | 55 | 94.8 | ||
| T3–T4 | 4 | 12.5 | 28 | 87.5 | 0.214 | |
| N class | ||||||
| N0–N1 | 5 | 6.8 | 69 | 93.2 | ||
| N2–N3 | 2 | 12.5 | 14 | 87.5 | 0.437 | |
| Stage | ||||||
| I–II | 2 | 3.2 | 61 | 96.8 | ||
| III–IV | 5 | 18.5 | 22 | 81.5 | 0.013 * | |
| Grade | ||||||
| I | 0 | 0.0 | 3 | 100.0 | ||
| II | 4 | 26.7 | 11 | 73.3 | ||
| III | 3 | 4.2 | 69 | 95.8 | 0.039 * | |
| Localization | ||||||
| Tonsil | 4 | 7.5 | 49 | 92.5 | ||
| Base of tongue | 1 | 4.5 | 21 | 95.5 | ||
| Soft palate | 0 | 0.0 | 10 | 100.0 | ||
| Posterior wall of oropharynx | 2 | 40.0 | 3 | 60.0 | 0.097 | |
| HPV | ||||||
| HPV+ | 2 | 3.8 | 51 | 96.2 | ||
| HPV− | 5 | 13.5 | 32 | 86.5 | 0.090 | |
| S-TATI | ||||||
| S-TATI+ | 4 | 19.0 | 17 | 81.0 | ||
| S-TATI- | 3 | 4.3 | 66 | 95.7 | 0.028 * |
| Variable | OS | DSS | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age at diagnosis | 1.08 | 1.03–1.14 | 0.003 * | 1.08 | 1.02–1.14 | 0.015 * |
| Smoking | 0.024 * | 0.183 | ||||
| Ex-smoker versus never smoker | 1.28 | 0.30–5.52 | 0.738 | 0.55 | 0.09–3.34 | 0.513 |
| Current smoker versus never smoker | 4.56 | 1.35–15.43 | 0.015 * | 2.45 | 0.64–9.37 | 0.192 |
| Stages III–IV versus Stages I–II | 1.67 | 0.68–4.10 | 0.267 | 1.93 | 0.60–6.20 | 0.267 |
| HPV− versus HPV+ | 1.13 | 0.40–3.22 | 0.818 | 1.02 | 0.26–3.93 | 0.980 |
| Ln(S-hCGβ) | 1.71 | 0.98–2.98 | 0.060 | 2.31 | 1.20–4.45 | 0.012 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sjöblom, A.; Carpén, T.; Stenman, U.-H.; Jouhi, L.; Haglund, C.; Syrjänen, S.; Mattila, P.; Mäkitie, A.; Hagström, J. The Role of Human Chorionic Gonadotropin Beta (hCGβ) in HPV-Positive and HPV-Negative Oropharyngeal Squamous Cell Carcinoma. Cancers 2022, 14, 2830. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14122830
Sjöblom A, Carpén T, Stenman U-H, Jouhi L, Haglund C, Syrjänen S, Mattila P, Mäkitie A, Hagström J. The Role of Human Chorionic Gonadotropin Beta (hCGβ) in HPV-Positive and HPV-Negative Oropharyngeal Squamous Cell Carcinoma. Cancers. 2022; 14(12):2830. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14122830
Chicago/Turabian StyleSjöblom, Anni, Timo Carpén, Ulf-Håkan Stenman, Lauri Jouhi, Caj Haglund, Stina Syrjänen, Petri Mattila, Antti Mäkitie, and Jaana Hagström. 2022. "The Role of Human Chorionic Gonadotropin Beta (hCGβ) in HPV-Positive and HPV-Negative Oropharyngeal Squamous Cell Carcinoma" Cancers 14, no. 12: 2830. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14122830