
Improving Risk Assessment for Metastatic Disease in Endometrioid Endometrial Cancer Patients Using Molecular and Clinical Features: An NRG Oncology/Gynecologic Oncology Group Study


 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Characteristics
2.2. Transcript Expression Data
2.3. Transcript Selection and Classifier Development
2.4. Relationships with Cancer Biomarkers and Functional Pathway Analysis
2.5. Exploring the Prognostic Relationship between MS7 and Clinical Outcome
3. Results
3.1. Selecting Transcripts Associated with Metastasis
3.2. Developing a Transcript-Based Classifier of Metastasis
3.3. Evaluating a Transcript-Based Classifier of Metastasis with Other Features
3.4. Developing and Evaluating Diagnostic Models of Metastasis
3.5. Evaluating the Biologic Plausibility of the MS7 Classifier of Metastasis
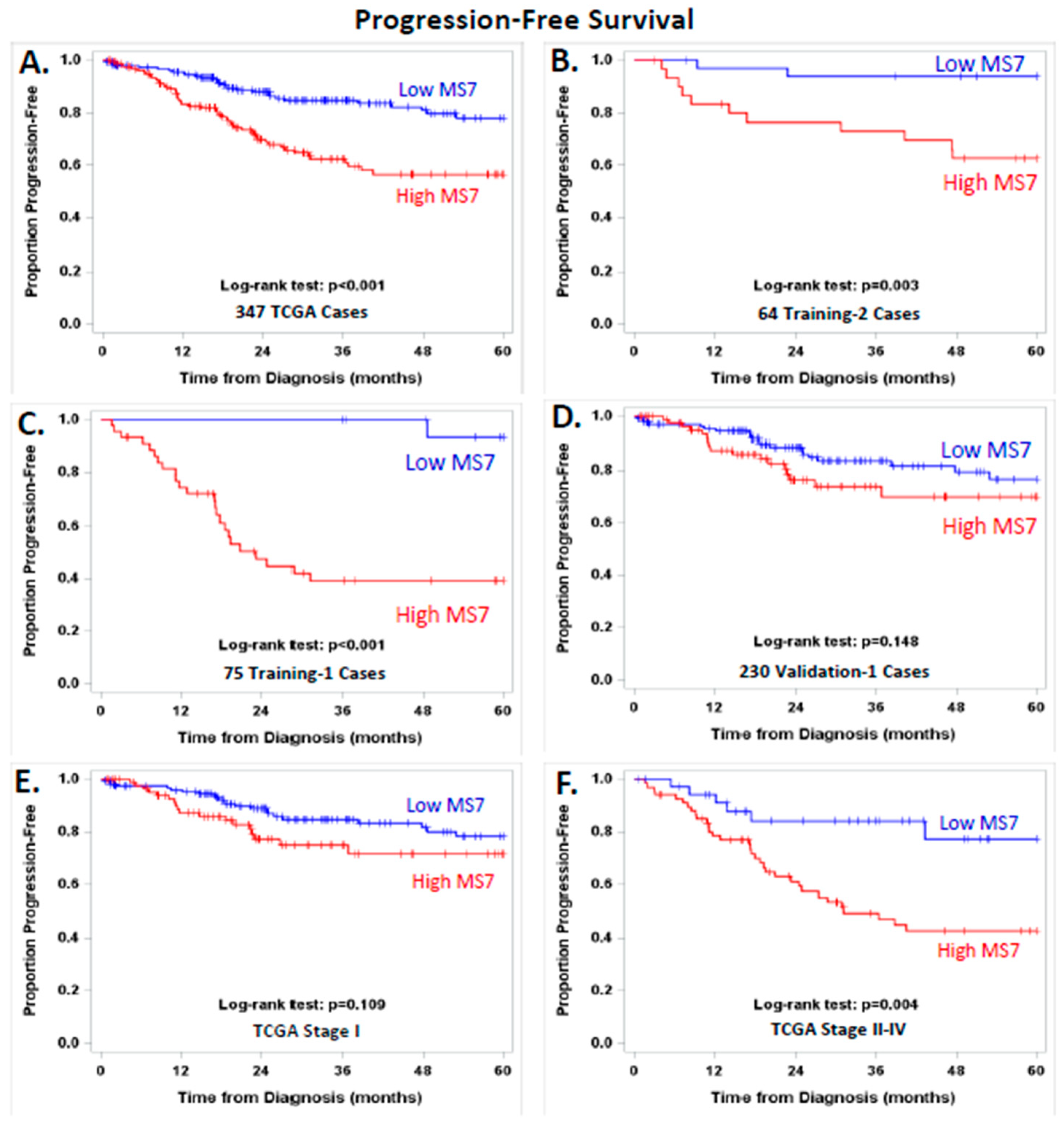
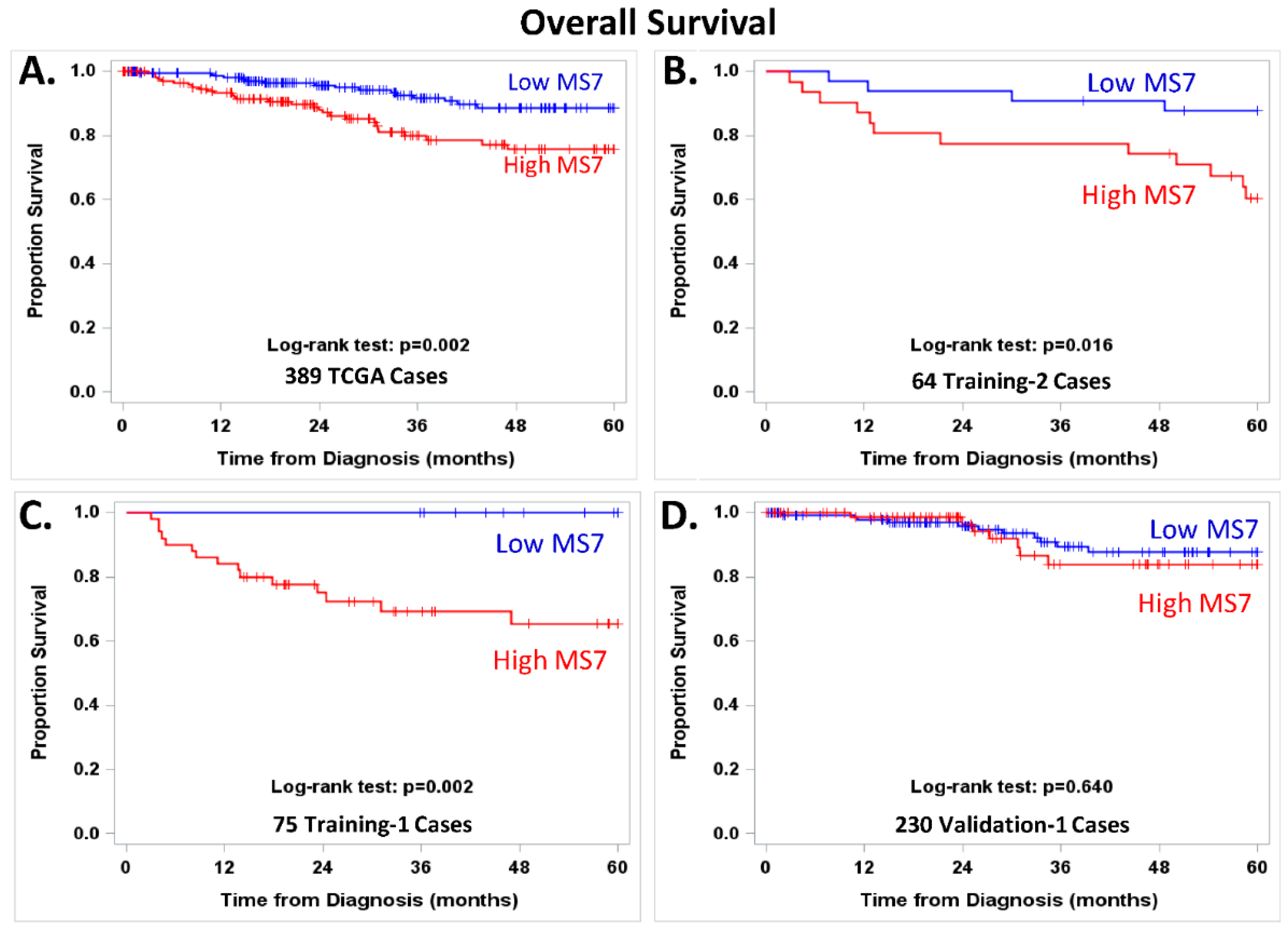
3.6. Exploring the Potential Prognostic Value of MS7
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- McMeekin, D.S.; Yashar, C.; Campos, S.M.; Zaino, R.J. Principles and Practices of Gynecologic Oncology; Limmincott Williams and Wilkins: Philadelphia, PA, USA, 2013; p. 1118. [Google Scholar]
- Mariani, A.; Webb, M.J.; Keeney, G.L.; Lesnick, T.G.; Podratz, K.C. Surgical stage I endometrial cancer: Predictors of distant failure and death. Gynecol. Oncol. 2002, 87, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Akbayir, O.; Goksedef, B.P.C.; Numanoglu, C.; Çorbacioğlu, A.; Ulker, V.; Akyol, A.; Güraslan, H.; Cetin, A.; Gulkilik, A. Immediate colposcopic evaluation in postmenopausal women with low-grade squamous intraepithelial lesion cytology. Acta Obstet. Gynecol. Scand. 2012, 91, 1109–1113. [Google Scholar] [CrossRef] [PubMed]
- Luomaranta, A.; Leminen, A.; Loukovaara, M. Prediction of lymph node and distant metastasis in patients with endometrial carcinoma: A new model based on demographics, biochemical factors, and tumor histology. Gynecol. Oncol. 2013, 129, 28–32. [Google Scholar] [CrossRef]
- Koskas, M.; Genin, A.S.; Graesslin, O.; Barranger, E.; Haddad, B.; Darai, E.; Rouzier, R. Evaluation of a method of predicting lymph node metastasis in endometrial cancer based on five pre-operative characteristics. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 172, 115–119. [Google Scholar] [CrossRef]
- AlHilli, M.; Podratz, K.; Dowdy, S.; Bakkum-Gamez, J.; Weaver, A.; McGree, M.; Keeney, G.; Cliby, W.; Mariani, A. Risk-scoring system for the individualized prediction of lymphatic dissemination in patients with endometrioid endometrial cancer. Gynecol. Oncol. 2013, 131, 103–108. [Google Scholar] [CrossRef]
- Koskas, M.; Bassot, K.; Graesslin, O.; Aristizabal, P.; Barranger, E.; Clavel-Chapelon, F.; Haddad, B.; Luton, D.; Darai, E.; Rouzier, R. Impact of lymphovascular space invasion on a nomogram for predicting lymph node metastasis in endometrial cancer. Gynecol. Oncol. 2013, 129, 292–297. [Google Scholar] [CrossRef]
- Lee, J.-Y.; Jung, D.-C.; Park, S.-H.; Lim, M.-C.; Seo, S.-S.; Park, S.-Y.; Kang, S. Preoperative prediction model of lymph node metastasis in endometrial cancer. Int. J. Gynecol. Cancer 2010, 20, 1350–1355. [Google Scholar] [CrossRef]
- Kang, S.; Kang, W.D.; Chung, H.H.; Jeong, D.H.; Seo, S.-S.; Lee, J.-M.; Lee, J.-K.; Kim, J.-W.; Kim, S.-M.; Park, S.-Y.; et al. Preoperative identification of a low-risk group for lymph node metastasis in endometrial cancer: A Korean gynecologic oncology group study. J. Clin. Oncol. 2012, 30, 1329–1334. [Google Scholar] [CrossRef]
- Kang, S.; Lee, J.-M.; Lee, J.-K.; Kim, J.W.; Cho, C.-H.; Kim, S.-M.; Park, S.-Y.; Park, C.-Y.; Kim, K.-T. How low is low enough? Evaluation of various risk-assessment models for lymph node metastasis in endometrial cancer: A Korean multicenter study. J. Gynecol. Oncol. 2012, 23, 251–256. [Google Scholar] [CrossRef]
- Milam, M.R.; Java, J.; Walker, J.L.; Metzinger, D.S.; Parker, L.P.; Coleman, R.L. Nodal metastasis risk in endometrioid endometrial cancer. Obstet. Gynecol. 2012, 119, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Ballester, M.; Canlorbe, G.; Cortez, A.; Gonin, J.; Laas, E.; Bendifallah, S.; Graesslin, O.; Daraï, E. Histological and immunohistochemical profiles predict lymph node status in women with low-intermediate risk endometrial cancer. Gynecol. Oncol. 2013, 130, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Bendifallah, S.; Canlorbe, G.; Collinet, P.; Arsene, E.; Huguet, F.; Coutant, C.; Hudry, D.; Graesslin, O.; Raimond, E.; Touboul, C.; et al. Just how accurate are the major risk stratification systems for early-stage endometrial cancer? Br. J. Cancer 2015, 112, 793–801. [Google Scholar] [CrossRef]
- Tuomi, T.; Pasanen, A.; Luomaranta, A.; Leminen, A.; Butzow, R.; Loukovaara, M. Risk-stratification of endometrial carcinomas revisited: A combined preoperative and intraoperative scoring system for a reliable prediction of an advanced disease. Gynecol. Oncol. 2015, 137, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Ytre-Hauge, S.; Husby, J.A.; Magnussen, I.J.; Werner, H.M.; Salvesen, O.; Bjørge, L.; Trovik, J.; Stefansson, I.M.; Salvesen, H.B.; Haldorsen, I.S. Preoperative tumor size at MRI predicts deep myometrial invasion, lymph node metastases, and patient outcome in endometrial carcinomas. Int. J. Gynecol. Cancer 2015, 25, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Cox Bauer, C.M.; Greer, D.M.; Kram, J.J.F.; Kamelle, S.A. Tumor diameter as a predictor of lymphatic dissemination in endometrioid endometrial cancer. Gynecol. Oncol. 2016, 141, 199–205. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research Network; Kandoth, C.; Schultz, N.; Cherniack, A.D.; Akbani, R.; Liu, Y.; Shen, H.; Robertson, A.G.; Pashtan, I.; Shen, R.; et al. Integrated genomic characterization of endometrial carcinoma. Nature 2013, 497, 67–73. [Google Scholar] [CrossRef]
- Morice, P.; Leary, A.; Creutzberg, C.; Abu-Rustum, N.; Darai, E. Endometrial cancer. Lancet 2016, 387, 1094–1108. [Google Scholar] [CrossRef]
- Bidus, M.A.; Risinger, J.I.; Chandramouli, G.V.; Dainty, L.A.; Litzi, T.J.; Berchuck, A.; Barrett, J.C.; Maxwell, G.L. Prediction of lymph node metastasis in patients with endometrioid endometrial cancer using expression microarray. Clin. Cancer Res. 2006, 12, 83–88. [Google Scholar] [CrossRef]
- Bateman, N.W.; Dubil, E.A.; Wang, G.; Hood, B.L.; Oliver, J.M.; Litzi, T.A.; Gist, G.D.; Mitchell, D.A.; Blanton, B.; Phippen, N.T.; et al. Race-specific molecular alterations correlate with differential outcomes for black and white endometrioid endometrial cancer patients. Cancer 2017, 123, 4004–4012. [Google Scholar] [CrossRef]
- Risinger, J.I.; Allard, J.; Chandran, U.; Day, R.; Chandramouli, G.V.R.; Miller, C.; Zahn, C.; Oliver, J.; Litzi, T.; Marcus, C.; et al. Gene expression analysis of early stage endometrial cancers reveals unique transcripts associated with grade and histology but not depth of invasion. Front. Oncol. 2013, 3, 139. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, G.L.; Allard, J.; Gadisetti, C.V.; Litzi, T.; Casablanca, Y.; Chandran, U.; Darcy, K.M.; Levine, D.A.; Berchuck, A.; Hamilton, C.A.; et al. Transcript expression in endometrial cancers from Black and White patients. Gynecol. Oncol. 2013, 130, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Kohler, M.F.; Carney, P.; Dodge, R.; Soper, J.T.; Clarke-Pearson, D.L.; Marks, J.R.; Berchuck, A. p53 overexpression in advanced-stage endometrial adenocarcinoma. Am. J. Obstet. Gynecol. 1996, 175, 1246–1252. [Google Scholar] [CrossRef]
- Trovik, J.; Wik, E.; Werner, H.M.; Krakstad, C.; Helland, H.; Vandenput, I.; Njølstad, T.; Stefansson, I.M.; Marcickiewicz, J.; Tingulstad, S.; et al. Hormone receptor loss in endometrial carcinoma curettage predicts lymph node metastasis and poor outcome in prospective multicentre trial. Eur. J. Cancer 2013, 49, 3431–3441. [Google Scholar] [CrossRef] [PubMed]
- Ohkouchi, T.; Sakuragi, N.; Watari, H.; Nomura, E.; Todo, Y.; Yamada, H.; Fujimoto, S. Prognostic significance of Bcl-2, p53 overexpression, and lymph node metastasis in surgically staged endometrial carcinoma. Am. J. Obstet. Gynecol. 2002, 187, 353–359. [Google Scholar] [CrossRef]
- Mariani, A.; Sebo, T.J.; Katzmann, J.A.; Roche, P.C.; Keeney, G.L.; Lesnick, T.G.; Podratz, K.C. Endometrial cancer: Can nodal status be predicted with curettage? Gynecol. Oncol. 2005, 96, 594–600. [Google Scholar] [CrossRef]
- Engelsen, I.B.; Stefansson, I.; Akslen, L.A.; Salvesen, H.B. Pathologic expression of p53 or p16 in preoperative curettage specimens identifies high-risk endometrial carcinomas. Am. J. Obstet. Gynecol. 2006, 195, 979–986. [Google Scholar] [CrossRef]
- Kang, S.; Thompson, Z.; McClung, E.C.; Abdallah, R.; Lee, J.K.; Bosquet, J.G.; Wenham, R.M.; Chon, H.S. Gene Expression Signature-Based Prediction of Lymph Node Metastasis in Patients With Endometrioid Endometrial Cancer. Int. J. Gynecol. Cancer 2018, 28, 260–266. [Google Scholar] [CrossRef]
- Pasanen, A.; Loukovaara, M.; Tuomi, T.; Butzow, R. Preoperative Risk Stratification of Endometrial Carcinoma: L1CAM as a Biomarker. Int. J. Gynecol. Cancer 2017, 27, 1318–1324. [Google Scholar] [CrossRef]
- Korkmaz, V.; Meydanli, M.M.; Yalçın, I.; Sarı, M.E.; Sahin, H.; Kocaman, E.; Haberal, A.; Dursun, P.; Güngör, T.; Ayhan, A. Comparison of three different risk-stratification models for predicting lymph node involvement in endometrioid endometrial cancer clinically confined to the uterus. J. Gynecol. Oncol. 2017, 28, e78. [Google Scholar] [CrossRef]
- Boyraz, G.; Atalay, F.O.; Salman, M.C.; Usubutun, A.; Erturk, A.; Gultekin, M.; Ozgul, N.; Yuce, K. Comparison of Mayo and Milwaukee Risk Stratification Models for Predicting Lymph Node Metastasis in Endometrial Cancer. Int. J. Gynecol. Cancer 2018, 28, 869–874. [Google Scholar] [CrossRef] [PubMed]
- Doghri, R.; Chaabouni, S.; Houcine, Y.; Charfi, L.; Boujelbene, N.; Driss, M.; Mrad, K. Evaluation of tumor-free distance and depth of myometrial invasion as prognostic factors in endometrial cancer. Mol. Clin. Oncol. 2018, 9, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Momtahan, M.; Hosseini, M.; Robati, M.; Najib, F. Predictive Value of Kanagawa Cancer Center Scoring System for Lymph Node Metastasis and Need for Lymphadenectomy in Patients with Endometrial Cancer: A Validation Study. Int. J. Gynecol. Cancer 2018, 28, 1290–1296. [Google Scholar] [CrossRef] [PubMed]
- Wakayama, A.; Kudaka, W.; Matsumoto, H.; Aoyama, H.; Ooyama, T.; Taira, Y.; Arakaki, Y.; Shimoji, Y.; Nakasone, T.; Nishihira, K.; et al. Lymphatic vessel involvement is predictive for lymph node metastasis and an important prognostic factor in endometrial cancer. Int. J. Clin. Oncol. 2018, 23, 532–538. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Ma, X.; Wang, Y.; Liu, Y.; Liu, C. Comparison of Different Scoring Systems in the Assessment of Estrogen Receptor Status for Predicting Prognosis in Endometrial Cancer. Int. J. Gynecol. Pathol. 2019, 38, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Jiang, T.; Huang, L.; Zhang, S. Preoperative serum CA125: A useful marker for surgical management of endometrial cancer. BMC Cancer 2015, 15, 396. [Google Scholar] [CrossRef]
- Son, J.-H.; Kong, T.-W.; Kim, S.H.; Paek, J.; Chang, S.-J.; Lee, E.J.; Ryu, H.-S. Prediction of lymph node metastasis in patients with apparent early endometrial cancer. Obstet. Gynecol. Sci. 2015, 58, 385–390. [Google Scholar] [CrossRef]
- Imai, K.; Kato, H.; Katayama, K.; Nakanishi, K.; Kawano, A.; Iura, A.; Konnai, K.; Onose, R.; Hirahara, F.; Miyagi, E. A preoperative risk-scoring system to predict lymph node metastasis in endometrial cancer and stratify patients for lymphadenectomy. Gynecol. Oncol. 2016, 142, 273–277. [Google Scholar] [CrossRef]
- Koskas, M.; Uzan, J.; Vanderstraeten, A.; Vergote, I.; Amant, F. External validation of non-imaging models for predicting distant metastasis in patients with endometrial cancer. Gynecol. Oncol. 2016, 142, 83–88. [Google Scholar] [CrossRef]
- Lee, J.; Kong, T.W.; Paek, J.; Chang, S.J.; Ryu, H.S. Predicting Model of Lymph Node Metastasis Using Preoperative Tumor Grade, Transvaginal Ultrasound, and Serum CA-125 Level in Patients with Endometrial Cancer. Int. J. Gynecol. Cancer 2016, 26, 1630–1635. [Google Scholar] [CrossRef]
- Yang, B.; Shan, B.; Xue, X.; Wang, H.; Shan, W.; Ning, C.; Zhou, Q.; Chen, X.; Luo, X. Predicting Lymph Node Metastasis in Endometrial Cancer Using Serum CA125 Combined with Immunohistochemical Markers PR and Ki67, and a Comparison with Other Prediction Models. PLoS ONE 2016, 11, e0155145. [Google Scholar] [CrossRef]
- Brooks, R.A.; Tritchler, D.S.; Darcy, K.M.; Lankes, H.A.; Salani, R.; Sperduto, P.; Guntupalli, S.; DiSilvestro, P.; Kesterson, J.; Olawaiye, A.B.; et al. GOG 8020/210: Risk stratification of lymph node metastasis, disease progression and survival using single nucleotide polymorphisms in endometrial cancer: An NRG oncology/gynecologic oncology group study. Gynecol. Oncol. 2019, 153, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Bendifallah, S.; Canlorbe, G.; Raimond, E.; Bazire, L.; Huguet, F.; Graesslin, O.; Rouzier, R.; Darai, E.; Ballester, M. An external validation study of nomograms designed to predict isolated loco-regional and distant endometrial cancer recurrences: How applicable are they? Br. J. Cancer 2013, 109, 1498–1503. [Google Scholar] [CrossRef] [PubMed]
- Carney, M.E.; Lancaster, J.M.; Ford, C.; Tsodikov, A.; Wiggins, C.L. A population-based study of patterns of care for ovarian cancer: Who is seen by a gynecologic oncologist and who is not? Gynecol. Oncol. 2002, 84, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.K.; Sherman, A.E.; Kapp, D.S.; Zhang, R.; Osann, K.E.; Maxwell, L.; Chen, L.-M.; Deshmukh, H. Influence of gynecologic oncologists on the survival of patients with endometrial cancer. J. Clin. Oncol. 2011, 29, 832–838. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, A.; Huvila, J.; Thompson, E.F.; Leung, S.; Chiu, D.; Lum, A.; McConechy, M.; Grondin, K.; Aguirre-Hernandez, R.; Salvador, S.; et al. Variation in practice in endometrial cancer and potential for improved care and equity through molecular classification. Gynecol. Oncol. 2022, 165, 201–214. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, G.L.; Secord, A.A.; Powell, M.A. The ProMisE of uniform care for endometrial cancer patients. Gynecol. Oncol. 2022, 165, 199–200. [Google Scholar] [CrossRef]
- Havrilesky, L.J.; Maxwell, G.L.; Chan, J.K.; Myers, E.R. Cost effectiveness of a test to detect metastases for endometrial cancer. Gynecol. Oncol. 2009, 112, 526–530. [Google Scholar] [CrossRef]
- Liu, Q.R.; Lu, L.; Zhu, X.G.; Gong, J.P.; Shaham, Y.; Uhl, G.R. Rodent BDNF genes, novel promoters, novel splice variants, and regulation by cocaine. Brain Res. 2006, 1067, 1–12. [Google Scholar] [CrossRef]
- Pruunsild, P.; Kazantseva, A.; Aid, T.; Palm, K.; Timmusk, T. Dissecting the human BDNF locus: Bidirectional transcription, complex splicing, and multiple promoters. Genomics 2007, 90, 397–406. [Google Scholar] [CrossRef]
- Thiele, C.J.; Li, Z.; McKee, A.E. On Trk—The TrkB signal transduction pathway is an increasingly important target in cancer biology. Clin. Cancer Res. 2009, 15, 5962–5967. [Google Scholar] [CrossRef] [PubMed]
- Cornelio, D.B.; DE Farias, C.B.; Prusch, D.S.; Heinen, T.E.; DOS Santos, R.P.; Abujamra, A.L.; Schwartsmann, G.; Roesler, R. Influence of GRPR and BDNF/TrkB signaling on the viability of breast and gynecologic cancer cells. Mol. Clin. Oncol. 2013, 1, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Bao, W.; Qiu, H.; Yang, T.; Luo, X.; Zhang, H.; Wan, X. Upregulation of TrkB promotes epithelial-mesenchymal transition and anoikis resistance in endometrial carcinoma. PLoS ONE 2013, 8, e70616. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Alconada, L.; Eritja, N.; Muinelo-Romay, L.; Barbazan, J.; Lopez-Lopez, R.; Matias-Guiu, X.; Gil-Moreno, A.; Dolcet, X.; Abal, M. ETV5 transcription program links BDNF and promotion of EMT at invasive front of endometrial carcinomas. Carcinogenesis 2014, 35, 2679–2686. [Google Scholar] [CrossRef] [PubMed]
- Monajemi, H.; Fontijn, R.D.; Pannekoek, H.; Horrevoets, A.J. The apolipoprotein L gene cluster has emerged recently in evolution and is expressed in human vascular tissue. Genomics 2002, 79, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.E.; Malik, H.S. The apolipoprotein L family of programmed cell death and immunity genes rapidly evolved in primates at discrete sites of host-pathogen interactions. Genome Res. 2009, 19, 850–858. [Google Scholar] [CrossRef]
- Caudell, D.; Zhang, Z.; Chung, Y.J.; Aplan, P.D. Expression of a CALM-AF10 fusion gene leads to Hoxa cluster overexpression and acute leukemia in transgenic mice. Cancer Res. 2007, 67, 8022–8031. [Google Scholar] [CrossRef]
- Xia, H.; Winokur, S.T.; Kuo, W.L.; Altherr, M.R.; Bredt, D.S. Actinin-associated LIM protein: Identification of a domain interaction between PDZ and spectrin-like repeat motifs. J. Cell Biol. 1997, 139, 507–515. [Google Scholar] [CrossRef]
- Klaavuniemi, T.; Alho, N.; Hotulainen, P.; Kelloniemi, A.; Havukainen, H.; Permi, P.; Mattila, S.; Ylänne, J. Characterization of the interaction between Actinin-Associated LIM Protein (ALP) and the rod domain of alpha-actinin. BMC Cell Biol. 2009, 10, 22. [Google Scholar] [CrossRef]
- Ohsawa, N.; Koebis, M.; Suo, S.; Nishino, I.; Ishiura, S. Alternative splicing of PDLIM3/ALP, for alpha-actinin-associated LIM protein 3, is aberrant in persons with myotonic dystrophy. Biochem. Biophys. Res. Commun. 2011, 409, 64–69. [Google Scholar] [CrossRef]
- Shou, Y.; Robinson, D.M.; Amakye, D.D.; Rose, K.L.; Cho, Y.-J.; Ligon, K.L.; Sharp, T.; Haider, A.S.; Bandaru, R.; Ando, Y.; et al. A five-gene hedgehog signature developed as a patient preselection tool for hedgehog inhibitor therapy in medulloblastoma. Clin. Cancer Res. 2015, 21, 585–593. [Google Scholar] [CrossRef] [PubMed]
- Cazalla, D.; Newton, K.; Caceres, J.F. A novel SR-related protein is required for the second step of Pre-mRNA splicing. Mol. Cell Biol. 2005, 25, 2969–2980. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Li, W.; Qiu, W.; Ren, W.; Li, Q.; Han, B.; Zhou, L.; Cheng, L.; Zhang, H.; Ye, Q. RSRC1 SUMOylation enhances SUMOylation and inhibits transcriptional activity of estrogen receptor beta. FEBS Lett. 2015, 589, 1476–1484. [Google Scholar] [CrossRef] [PubMed]
- Tompkins, V.S.; Hagen, J.; Frazier, A.A.; Lushnikova, T.; Fitzgerald, M.P.; di Tommaso, A.; Ladeveze, V.; Domann, F.E.; Eischen, C.M.; Quelle, D.E. A novel nuclear interactor of ARF and MDM2 (NIAM) that maintains chromosomal stability. J. Biol. Chem. 2007, 282, 1322–1333. [Google Scholar] [CrossRef] [PubMed]
- Reed, S.M.; Hagen, J.; Tompkins, V.S.; Thies, K.; Quelle, F.W.; Quelle, D.E. Nuclear interactor of ARF and Mdm2 regulates multiple pathways to activate p53. Cell Cycle 2014, 13, 1288–1298. [Google Scholar] [CrossRef] [PubMed]
- Kramer, A.; Green, J.; Pollard, J., Jr.; Tugendreich, S. Causal analysis approaches in Ingenuity Pathway Analysis. Bioinformatics 2014, 30, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Vilgelm, A.; Lian, Z.; Wang, H.; Beauparlant, S.L.; Klein-Szanto, A.; Ellenson, L.H.; Di Cristofano, A. Akt-mediated phosphorylation and activation of estrogen receptor alpha is required for endometrial neoplastic transformation in Pten+/− mice. Cancer Res. 2006, 66, 3375–3380. [Google Scholar] [CrossRef]
- Shah, Y.M.; Rowan, B.G. The Src kinase pathway promotes tamoxifen agonist action in Ishikawa endometrial cells through phosphorylation-dependent stabilization of estrogen receptor (alpha) promoter interaction and elevated steroid receptor coactivator 1 activity. Mol. Endocrinol. 2005, 19, 732–748. [Google Scholar] [CrossRef]
- Powell, S.N.; Kachnic, L.A. Roles of BRCA1 and BRCA2 in homologous recombination, DNA replication fidelity and the cellular response to ionizing radiation. Oncogene 2003, 22, 5784–5791. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| RNA Sequencing Data | Affymetrix Microarray Data | ||||
|---|---|---|---|---|---|
| Training-1 | Validation-1 | Exploratory | Training-2 | Validation-2 | |
| Median Age in Years | 61 | 63 | 62 | 61.8 | - |
| [Interquartile Range] | [55.0–67.0] | [55.0–71.0] | [55.0–70.0] | [56.5–72.8] | |
| <60 | 32 (42.7) | 86 (37.9) | 154 (39.9) | 27 (42.2) | - |
| ≥60 | 43 (57.3) | 141 (62.1) | 232 (60.1) | 37 (57.8) | - |
| Unknown | - | 18 | 3 | - | 81 |
| Tumor Grade | |||||
| 1 (G1) | 13 (17.3) | 65 (26.5) | 93 (23.9) | 12 (18.7) | 26 (32.1) |
| 2 (G2) | 14 (18.7) | 77 (31.4) | 106 (27.3) | 15 (23.4) | 33 (40.7) |
| 3 (G3) | 48 (64.0) | 103 (42.0) | 190 (48.8) | 37 (57.8) | 22 (27.2) |
| Stage | |||||
| IA | 24 (32.0) | 163 (66.5) | 185 (47.6) | 18 (28.1) | 53 (65.4) |
| IB | 5 (6.7) | 70 (28.6) | 91 (23.4) | 13 (20.3) | 16 (19.8) |
| II | - | - | 31 (8.0) | - | - |
| III/IIIA/IIIB | - | - | 31 (8.0) | - | - |
| IIIC | 33 (44.0) | 10 (4.1) | 37 (9.5) | 22 (34.4) | 9 (11.1) |
| IV | 13 (17.3) | 2 (0.8) | 14 (3.6) | 11 (17.2) | 3 (3.7) |
| Myometrial Invasion | |||||
| <50% | 43 (59.7) | 166 (69.8) | 245 (70.2) | 27 (42.2) | 56 (69.1) |
| ≥>50% | 29 (40.3) | 72 (30.3) | 104 (29.8) | 37 (57.8) | 25 (30.9) |
| Unknown | 3 | 7 | 40 | - | - |
| Metastasis Status | |||||
| Uterine-Confined Disease | 29 (38.7) | 233 (95.1) | 276 (71.0) | 31 (48.4) | 69 (85.2) |
| Other Metastatic State | - | - | 62 (15.9) | ||
| Nodal/Distant Metastasis | 46 (61.3) | 12 (4.9) | 51 (13.1) | 33 (51.6) | 12 (14.8) |
| Source | |||||
| TCGA | 75 | 230 | 389 | - | - |
| GOG | - | - | - | 64 | - |
| GYN-COE | - | 15 | - | - | 81 |
| Cohort | Prediction Model ^ | AUC | 95% CI |
|---|---|---|---|
| Training-1 | MS7 Score | 0.89 | 0.80–0.98 |
| G3 (yes/no) | 0.66 | 0.55–0.77 | |
| MI (yes/no) | 0.69 | 0.59–0.80 | |
| MS7 Score + G3 (yes/no) | 0.89 | 0.80–0.98 | |
| MS7 Score + MI (yes/no) | 0.92 | 0.85–0.99 | |
| MS7 Score + MI (yes/no) + G3 (yes/no) | 0.92 | 0.85–0.99 | |
| Validation-1 | MS7 | 0.75 | 0.60–0.91 |
| G3 (yes/no) | 0.67 | 0.54–0.81 | |
| MI (yes/no) | 0.72 | 0.58–0.86 | |
| MS7 + G3 (yes/no) | 0.76 | 0.59–0.92 | |
| MS7 + MI (yes/no) | 0.81 | 0.71–0.92 | |
| MS7 + MI (yes/no) + G3 (yes/no) | 0.83 | 0.72–0.94 | |
| Training-2 | MS7 | 0.89 | 0.81–0.97 |
| G3 (yes/no) | 0.56 | 0.44–0.68 | |
| MI (yes/no) | 0.65 | 0.54–0.77 | |
| MS7 + G3 (yes/no) | 0.90 | 0.82–0.98 | |
| MS7 + MI (yes/no) | 0.91 | 0.84–0.98 | |
| MS7 + MI (yes/no) + G3 (yes/no) | 0.92 | 0.86–0.99 | |
| Validation-2 | MS7 | 0.74 | 0.59–0.90 |
| G3 | 0.73 | 0.59–0.88 | |
| MI | 0.76 | 0.62–0.90 | |
| MS7 + G3 (yes/no) | 0.80 | 0.66–0.94 | |
| MS7 + MI (yes/no) | 0.86 | 0.77–0.96 | |
| MS7 + MI (yes/no) + G3 (yes/no) | 0.87 | 0.78–0.97 |
| Predictive Accuracy | RNA Sequencing Data | Affymetrix Microarray Data | Merged Data | |
|---|---|---|---|---|
| Validation-1 [N = 245] | Validation-2 [N = 81] | Validation 1 + 2 [N = 326] | ||
| MS7 | SN; 95% CI | 0.83; 0.52–0.98 | 0.75; 0.43–0.95 | 0.79; 0.58–0.93 |
| SP; 95% CI | 0.61; 0.55–0.68 | 0.64; 0.51–0.75 | 0.62; 0.56–0.67 | |
| PPV; 95% CI | 0.28; 0.21–0.33 | 0.27; 0.18–0.37 | 0.27; 0.22–0.32 | |
| NPV; 95% CI | 0.95; 0.85–1.00 | 0.93; 0.87–1.00 | 0.94; 0.90–0.98 | |
| MS7 + Grade 3 † | SN; 95% CI | 0.92; 0.62–1.00 | 0.83; 0.52–0.98 | 0.88; 0.68–0.97 |
| SP; 95% CI | 0.42; 0.36–0.49 | 0.55; 0.43–0.67 | 0.45; 0.40–0.51 | |
| PPV; 95% CI | 0.22; 0.18–0.25 | 0.25; 0.18–0.32 | 0.22; 0.19–0.25 | |
| NPV; 95% CI | 0.97; 0.90–1.00 | 0.95; 0.88–1.00 | 0.95; 0.90–1.00 | |
| MS7 + MI ‡ | SN; 95% CI | 1.00; 0.72–1.00 | 1.00; 0.74–1.00 | 1.00; 0.85–1.00 |
| SP; 95% CI | 0.48; 0.41–0.55 | 0.52; 0.40–0.64 | 0.49; 0.43–0.55 | |
| PPV; 95% CI | 0.25; 0.23–0.28 | 0.27; 0.23–0.33 | 0.26; 0.24–0.28 | |
| NPV; 95% CI | 1.00; 1.00–1.00 | 1.00; 1.00–1.00 | 1.00; 1.00–1.00 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casablanca, Y.; Wang, G.; Lankes, H.A.; Tian, C.; Bateman, N.W.; Miller, C.R.; Chappell, N.P.; Havrilesky, L.J.; Wallace, A.H.; Ramirez, N.C.; et al. Improving Risk Assessment for Metastatic Disease in Endometrioid Endometrial Cancer Patients Using Molecular and Clinical Features: An NRG Oncology/Gynecologic Oncology Group Study. Cancers 2022, 14, 4070. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14174070
Casablanca Y, Wang G, Lankes HA, Tian C, Bateman NW, Miller CR, Chappell NP, Havrilesky LJ, Wallace AH, Ramirez NC, et al. Improving Risk Assessment for Metastatic Disease in Endometrioid Endometrial Cancer Patients Using Molecular and Clinical Features: An NRG Oncology/Gynecologic Oncology Group Study. Cancers. 2022; 14(17):4070. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14174070
Chicago/Turabian StyleCasablanca, Yovanni, Guisong Wang, Heather A. Lankes, Chunqiao Tian, Nicholas W. Bateman, Caela R. Miller, Nicole P. Chappell, Laura J. Havrilesky, Amy Hooks Wallace, Nilsa C. Ramirez, and et al. 2022. "Improving Risk Assessment for Metastatic Disease in Endometrioid Endometrial Cancer Patients Using Molecular and Clinical Features: An NRG Oncology/Gynecologic Oncology Group Study" Cancers 14, no. 17: 4070. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14174070