
Circulating Tumor DNA-Based Disease Monitoring of Patients with Locally Advanced Esophageal Cancer
 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
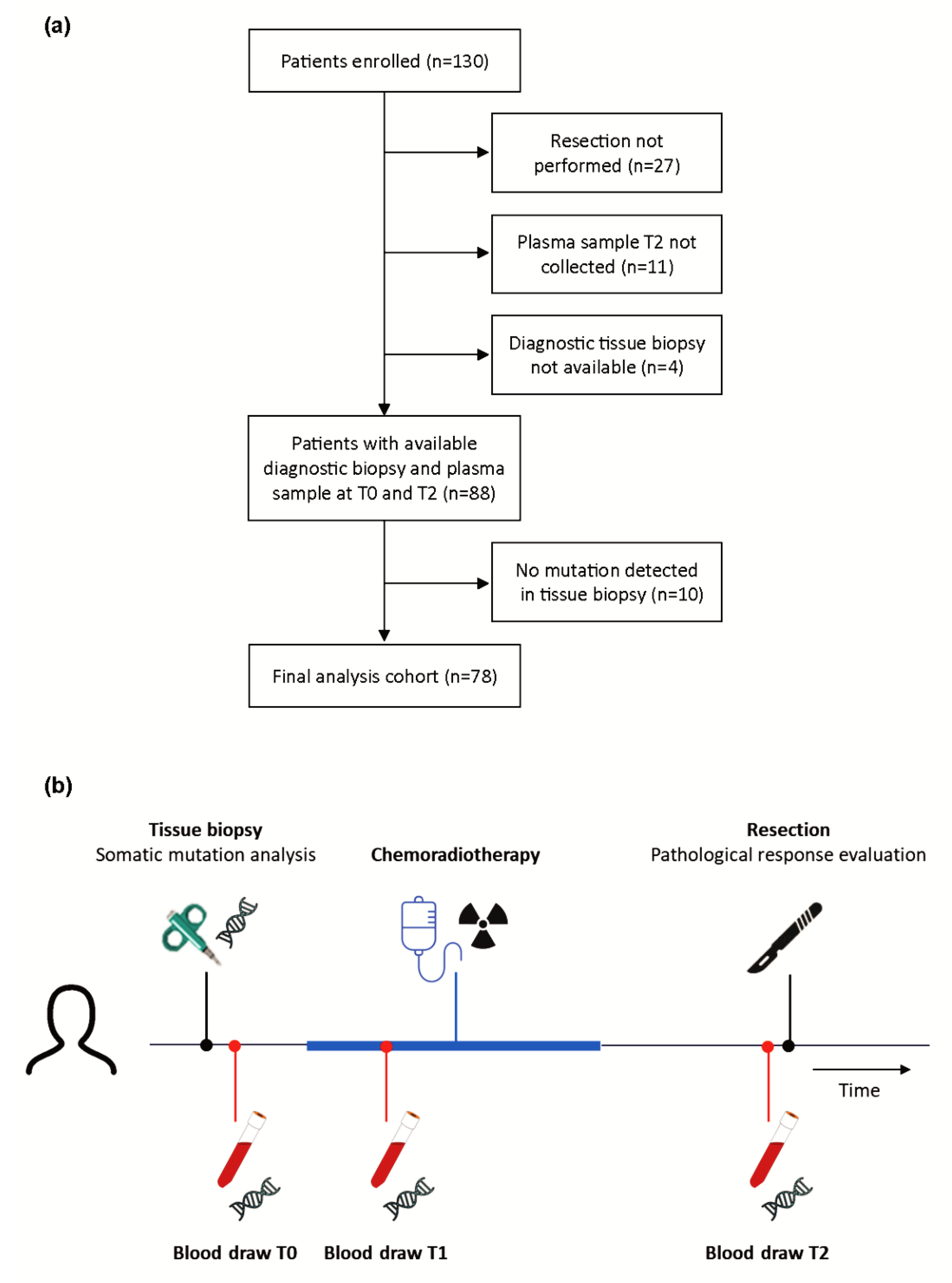
2.1. Patient and Sample Collection
2.2. Tumor Tissue Analysis
2.3. Plasma Analysis
2.4. Data Evaluation
3. Results
3.1. Patient Characteristics
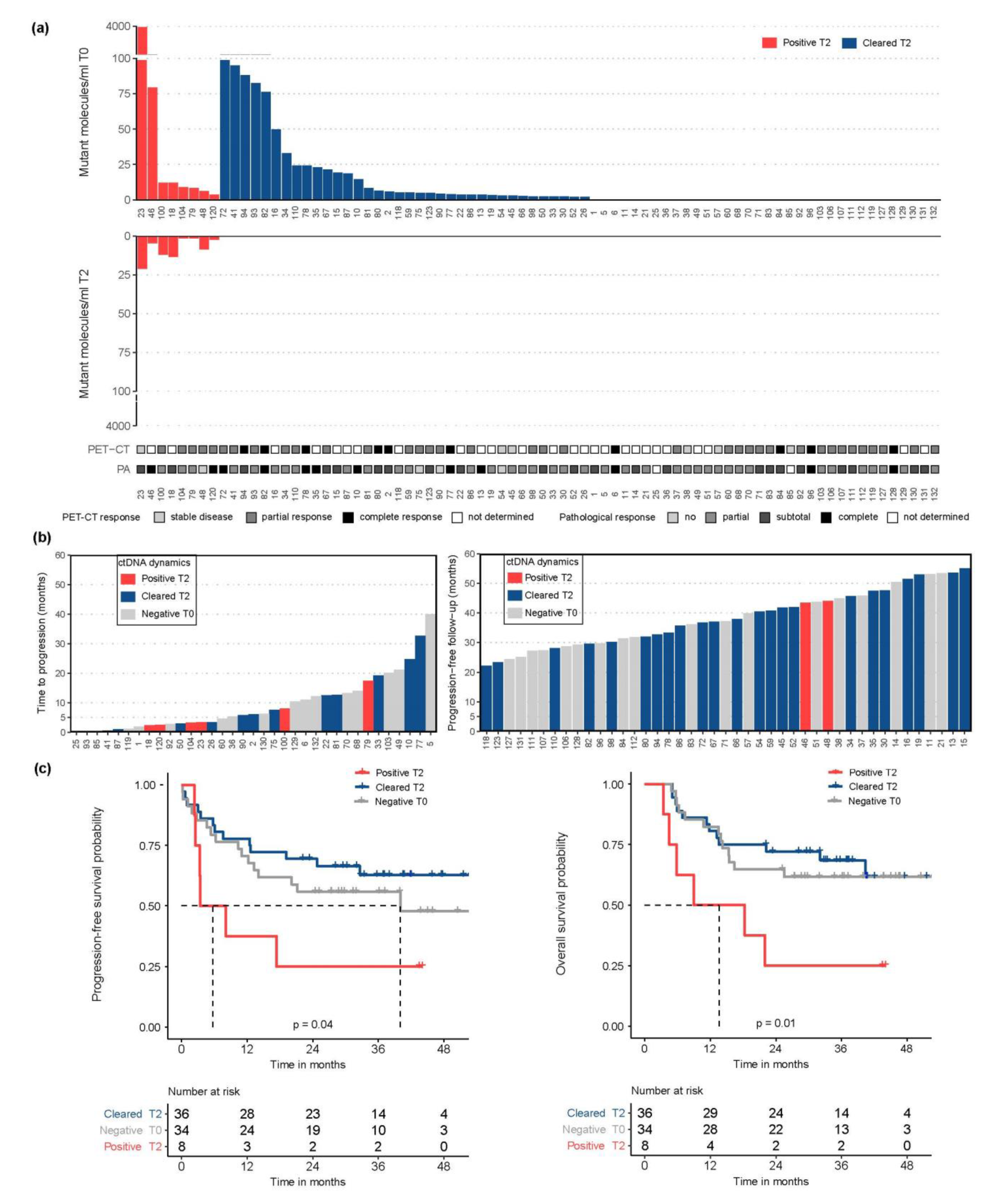
3.2. ctDNA Detection Pre-CRT Was Associated with Tumor Burden
3.3. Preoperative ctDNA Detection Was Associated with Higher Risk of Recurrence
3.4. ctDNA Dynamics during CRT Was Not Associated with Response
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Van Hagen, P.; Hulshof, M.C.; van Lanschot, J.J.; Steyerberg, E.W.; van Berge Henegouwen, M.I.; Wijnhoven, B.P.; Richel, D.J.; Nieuwenhuijzen, G.A.; Hospers, G.A.; Bonenkamp, J.J.; et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N. Engl. J. Med. 2012, 366, 2074–2084. [Google Scholar] [CrossRef] [PubMed]
- Noordman, B.J.; Shapiro, J.; Spaander, M.C.; Krishnadath, K.K.; van Laarhoven, H.W.; van Berge Henegouwen, M.I.; Nieuwenhuijzen, G.A.; van Hillegersberg, R.; Sosef, M.N.; Steyerberg, E.W.; et al. Accuracy of Detecting Residual Disease After Cross Neoadjuvant Chemoradiotherapy for Esophageal Cancer (preSANO Trial): Rationale and Protocol. JMIR Res. Protoc. 2015, 4, e79. [Google Scholar] [CrossRef] [PubMed]
- Levinsky, N.C.; Wima, K.; Morris, M.C.; Ahmad, S.A.; Shah, S.A.; Starnes, S.L.; Van Haren, R.M. Outcome of delayed versus timely esophagectomy after chemoradiation for esophageal adenocarcinoma. J. Thorac. Cardiovasc. Surg. 2020, 159, 2555–2566. [Google Scholar] [CrossRef] [PubMed]
- Seely, A.J.; Ivanovic, J.; Threader, J.; Al-Hussaini, A.; Al-Shehab, D.; Ramsay, T.; Gilbert, S.; Maziak, D.E.; Shamji, F.M.; Sundaresan, R.S. Systematic classification of morbidity and mortality after thoracic surgery. Ann. Thorac. Surg. 2010, 90, 936–942; discussion 942. [Google Scholar] [CrossRef]
- Shapiro, J.; van Lanschot, J.J.B.; Hulshof, M.; van Hagen, P.; van Berge Henegouwen, M.I.; Wijnhoven, B.P.L.; van Laarhoven, H.W.M.; Nieuwenhuijzen, G.A.P.; Hospers, G.A.P.; Bonenkamp, J.J.; et al. Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): Long-term results of a randomised controlled trial. Lancet Oncol. 2015, 16, 1090–1098. [Google Scholar] [CrossRef]
- Wan, J.C.M.; Massie, C.; Garcia-Corbacho, J.; Mouliere, F.; Brenton, J.D.; Caldas, C.; Pacey, S.; Baird, R.; Rosenfeld, N. Liquid biopsies come of age: Towards implementation of circulating tumour DNA. Nat. Rev. Cancer 2017, 17, 223–238. [Google Scholar] [CrossRef]
- Heitzer, E.; Haque, I.S.; Roberts, C.E.S.; Speicher, M.R. Current and future perspectives of liquid biopsies in genomics-driven oncology. Nat. Rev. Genet. 2019, 20, 71–88. [Google Scholar] [CrossRef]
- Abbosh, C.; Birkbak, N.J.; Wilson, G.A.; Jamal-Hanjani, M.; Constantin, T.; Salari, R.; Le Quesne, J.; Moore, D.A.; Veeriah, S.; Rosenthal, R.; et al. Phylogenetic ctDNA analysis depicts early-stage lung cancer evolution. Nature 2017, 545, 446–451. [Google Scholar] [CrossRef]
- Tie, J.; Wang, Y.; Tomasetti, C.; Li, L.; Springer, S.; Kinde, I.; Silliman, N.; Tacey, M.; Wong, H.L.; Christie, M.; et al. Circulating tumor DNA analysis detects minimal residual disease and predicts recurrence in patients with stage II colon cancer. Sci. Transl. Med. 2016, 8, 346ra92. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Murillas, I.; Schiavon, G.; Weigelt, B.; Ng, C.; Hrebien, S.; Cutts, R.J.; Cheang, M.; Osin, P.; Nerurkar, A.; Kozarewa, I.; et al. Mutation tracking in circulating tumor DNA predicts relapse in early breast cancer. Sci. Transl. Med. 2015, 7, 302ra133. [Google Scholar] [CrossRef] [PubMed]
- Ko, J.M.Y.; Ng, H.Y.; Lam, K.O.; Chiu, K.W.H.; Kwong, D.L.W.; Lo, A.W.I.; Wong, J.C.; Lin, R.C.W.; Fong, H.C.H.; Li, J.Y.K.; et al. Liquid Biopsy Serial Monitoring of Treatment Responses and Relapse in Advanced Esophageal Squamous Cell Carcinoma. Cancers 2020, 12, 1352. [Google Scholar] [CrossRef] [PubMed]
- Maron, S.B.; Chase, L.M.; Lomnicki, S.; Kochanny, S.; Moore, K.L.; Joshi, S.S.; Landron, S.; Johnson, J.; Kiedrowski, L.A.; Nagy, R.J.; et al. Circulating Tumor DNA Sequencing Analysis of Gastroesophageal Adenocarcinoma. Clin. Cancer Res. 2019, 25, 7098–7112. [Google Scholar] [CrossRef] [PubMed]
- Kato, S.; Okamura, R.; Baumgartner, J.M.; Patel, H.; Leichman, L.; Kelly, K.; Sicklick, J.K.; Fanta, P.T.; Lippman, S.M.; Kurzrock, R. Analysis of Circulating Tumor DNA and Clinical Correlates in Patients with Esophageal, Gastroesophageal Junction, and Gastric Adenocarcinoma. Clin. Cancer Res. 2018, 24, 6248–6256. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, S.; Ichikawa, D.; Hirajima, S.; Takeshita, H.; Shiozaki, A.; Fujiwara, H.; Kawaguchi, T.; Miyamae, M.; Konishi, H.; Kubota, T.; et al. Clinical impact of predicting CCND1 amplification using plasma DNA in superficial esophageal squamous cell carcinoma. Dig. Dis. Sci. 2014, 59, 1152–1159. [Google Scholar] [CrossRef]
- Andolfo, I.; Petrosino, G.; Vecchione, L.; De Antonellis, P.; Capasso, M.; Montanaro, D.; Gemei, M.; Troncone, G.; Iolascon, A.; Orditura, M.; et al. Detection of erbB2 copy number variations in plasma of patients with esophageal carcinoma. BMC Cancer 2011, 11, 126. [Google Scholar] [CrossRef]
- Boldrin, E.; Curtarello, M.; Fassan, M.; Rugge, M.; Realdon, S.; Alfieri, R.; Amadori, A.; Saggioro, D. Allelic Imbalance Analysis in Liquid Biopsy to Monitor Locally Advanced Esophageal Cancer Patients During Treatment. Front. Oncol. 2020, 10, 1320. [Google Scholar] [CrossRef]
- Luo, H.; Li, H.; Hu, Z.; Wu, H.; Liu, C.; Li, Y.; Zhang, X.; Lin, P.; Hou, Q.; Ding, G.; et al. Noninvasive diagnosis and monitoring of mutations by deep sequencing of circulating tumor DNA in esophageal squamous cell carcinoma. Biochem. Biophys. Res. Commun. 2016, 471, 596–602. [Google Scholar] [CrossRef]
- Ueda, M.; Iguchi, T.; Masuda, T.; Nakahara, Y.; Hirata, H.; Uchi, R.; Niida, A.; Momose, K.; Sakimura, S.; Chiba, K.; et al. Somatic mutations in plasma cell-free DNA are diagnostic markers for esophageal squamous cell carcinoma recurrence. Oncotarget 2016, 7, 62280–62291. [Google Scholar] [CrossRef]
- Azad, T.D.; Chaudhuri, A.A.; Fang, P.; Qiao, Y.; Esfahani, M.S.; Chabon, J.J.; Hamilton, E.G.; Yang, Y.D.; Lovejoy, A.; Newman, A.M.; et al. Circulating Tumor DNA Analysis for Detection of Minimal Residual Disease After Chemoradiotherapy for Localized Esophageal Cancer. Gastroenterology 2020, 158, 494–505.e6. [Google Scholar] [CrossRef]
- Ococks, E.; Frankell, A.M.; Masque Soler, N.; Grehan, N.; Northrop, A.; Coles, H.; Redmond, A.M.; Devonshire, G.; Weaver, J.M.J.; Hughes, C.; et al. Longitudinal tracking of 97 esophageal adenocarcinomas using liquid biopsy sampling. Ann. Oncol. 2021, 32, 522–532. [Google Scholar] [CrossRef] [PubMed]
- Cabalag, C.S.; Yates, M.; Corrales, M.B.; Yeh, P.; Wong, S.Q.; Zhang, B.Z.; Fujihara, K.M.; Chong, L.; Hii, M.W.; Dawson, S.-J.; et al. Potential Clinical Utility of a Targeted Circulating Tumor DNA Assay in Esophageal Adenocarcinoma. Ann. Surg. 2022, 276, e120–e126. [Google Scholar] [CrossRef] [PubMed]
- Bonazzi, V.F.; Aoude, L.G.; Brosda, S.; Lonie, J.M.; Patel, K.; Bradford, J.J.; Koufariotis, L.T.; Wood, S.; Smithers, B.M.; Waddell, N.; et al. ctDNA as a biomarker of progression in oesophageal adenocarcinoma. ESMO Open 2022, 7, 100452. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Yao, Q.; Jin, H. Plasma Circulating Tumor DNA Sequencing Predicts Minimal Residual Disease in Resectable Esophageal Squamous Cell Carcinoma. Front. Oncol. 2021, 11, 616209. [Google Scholar] [CrossRef]
- Burnet, N.G.; Thomas, S.J.; Burton, K.E.; Jefferies, S.J. Defining the tumour and target volumes for radiotherapy. Cancer Imaging 2004, 4, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Mandard, A.M.; Dalibard, F.; Mandard, J.C.; Marnay, J.; Henry-Amar, M.; Petiot, J.F.; Roussel, A.; Jacob, J.H.; Segol, P.; Samama, G.; et al. Pathologic assessment of tumor regression after preoperative chemoradiotherapy of esophageal carcinoma. Clinicopathologic correlations. Cancer 1994, 73, 2680–2686. [Google Scholar] [CrossRef]
- Eijkelenboom, A.; Kamping, E.J.; Kastner-van Raaij, A.W.; Hendriks-Cornelissen, S.J.; Neveling, K.; Kuiper, R.P.; Hoischen, A.; Nelen, M.R.; Ligtenberg, M.J.; Tops, B.B. Reliable Next-Generation Sequencing of Formalin-Fixed, Paraffin-Embedded Tissue Using Single Molecule Tags. J. Mol. Diagn. 2016, 18, 851–863. [Google Scholar] [CrossRef]
- De Voer, R.M.; Diets, I.J.; van der Post, R.S.; Weren, R.D.A.; Kamping, E.J.; de Bitter, T.J.J.; Elze, L.; Verhoeven, R.H.A.; Vink-Borger, E.; Eijkelenboom, A.; et al. Clinical, Pathology, Genetic, and Molecular Features of Colorectal Tumors in Adolescents and Adults 25 Years or Younger. Clin. Gastroenterol. Hepatol. 2021, 19, 1642–1651.e8. [Google Scholar] [CrossRef]
- Steeghs, E.M.P.; Kroeze, L.I.; Tops, B.B.J.; van Kempen, L.C.; Ter Elst, A.; Kastner-van Raaij, A.W.M.; Hendriks-Cornelissen, S.J.B.; Hermsen, M.J.W.; Jansen, E.A.M.; Nederlof, P.M.; et al. Comprehensive routine diagnostic screening to identify predictive mutations, gene amplifications, and microsatellite instability in FFPE tumor material. BMC Cancer 2020, 20, 291. [Google Scholar] [CrossRef]
- Cancer Genome Atlas, N. Comprehensive molecular characterization of human colon and rectal cancer. Nature 2012, 487, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Research Network; Analysis Working Group: Asan University; BC Cancer Agency; Brigham and Women’s Hospital; Broad Institute; Brown University; Case Western Reserve University; Dana-Farber Cancer Institute; Duke University; Greater Poland Cancer Centre; et al. Integrated genomic characterization of oesophageal carcinoma. Nature 2017, 541, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Durbin, R. Fast and accurate short read alignment with Burrows-Wheeler transform. Bioinformatics 2009, 25, 1754–1760. [Google Scholar] [CrossRef] [PubMed]
- Kelly, R.J.; Ajani, J.A.; Kuzdzal, J.; Zander, T.; Van Cutsem, E.; Piessen, G.; Mendez, G.; Feliciano, J.; Motoyama, S.; Lievre, A.; et al. Adjuvant Nivolumab in Resected Esophageal or Gastroesophageal Junction Cancer. N. Engl. J. Med. 2021, 384, 1191–1203. [Google Scholar] [CrossRef]
- Egyud, M.; Tejani, M.; Pennathur, A.; Luketich, J.; Sridhar, P.; Yamada, E.; Stahlberg, A.; Filges, S.; Krzyzanowski, P.; Jackson, J.; et al. Detection of Circulating Tumor DNA in Plasma: A Potential Biomarker for Esophageal Adenocarcinoma. Ann. Thorac. Surg. 2019, 108, 343–349. [Google Scholar] [CrossRef]
- Bettegowda, C.; Sausen, M.; Leary, R.J.; Kinde, I.; Wang, Y.; Agrawal, N.; Bartlett, B.R.; Wang, H.; Luber, B.; Alani, R.M.; et al. Detection of circulating tumor DNA in early- and late-stage human malignancies. Sci. Transl. Med. 2014, 6, 224ra24. [Google Scholar] [CrossRef]
- Vidal, J.; Casadevall, D.; Bellosillo, B.; Pericay, C.; Garcia-Carbonero, R.; Losa, F.; Layos, L.; Alonso, V.; Capdevila, J.; Gallego, J.; et al. Clinical Impact of Presurgery Circulating Tumor DNA after Total Neoadjuvant Treatment in Locally Advanced Rectal Cancer: A Biomarker Study from the GEMCAD 1402 Trial. Clin. Cancer Res. 2021, 27, 2890–2898. [Google Scholar] [CrossRef]
- Boniface, C.; Deig, C.; Halsey, C.; Kelley, T.; Heskett, M.B.; Thomas, C.R., Jr.; Spellman, P.T.; Nabavizadeh, N. The Feasibility of Patient-Specific Circulating Tumor DNA Monitoring throughout Multi-Modality Therapy for Locally Advanced Esophageal and Rectal Cancer: A Potential Biomarker for Early Detection of Subclinical Disease. Diagnostics 2021, 11, 73. [Google Scholar] [CrossRef]
- Borggreve, A.S.; Mook, S.; Verheij, M.; Mul, V.E.M.; Bergman, J.J.; Bartels-Rutten, A.; Ter Beek, L.C.; Beets-Tan, R.G.H.; Bennink, R.J.; van Berge Henegouwen, M.I.; et al. Preoperative image-guided identification of response to neoadjuvant chemoradiotherapy in esophageal cancer (PRIDE): A multicenter observational study. BMC Cancer 2018, 18, 1006. [Google Scholar] [CrossRef]
- Murugaesu, N.; Wilson, G.A.; Birkbak, N.J.; Watkins, T.B.K.; McGranahan, N.; Kumar, S.; Abbassi-Ghadi, N.; Salm, M.; Mitter, R.; Horswell, S.; et al. Tracking the Genomic Evolution of Esophageal Adenocarcinoma through Neoadjuvant Chemotherapy. Cancer Discov. 2015, 5, 821–831. [Google Scholar] [CrossRef] [Green Version]
- Killcoyne, S.; Gregson, E.; Wedge, D.C.; Woodcock, D.J.; Eldridge, M.D.; de la Rue, R.; Miremadi, A.; Abbas, S.; Blasko, A.; Kosmidou, C.; et al. Genomic copy number predicts esophageal cancer years before transformation. Nat. Med. 2020, 26, 1726–1732. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Clinicopathological Characteristics | All Patients (n = 78) | ctDNA Pre-CRT (T0) (n = 78) | ctDNA Preoperative (T2) (n = 78) | |||||
|---|---|---|---|---|---|---|---|---|
| Negative | Positive | p-Value | Negative | Positive | p-Value | |||
| Age, median (range) | 67 (50–82) | 68 (50–82) | 65 (52–80) | 0.27 | 67 (50–82) | 64 (54–80) | 0.42 | |
| Gender, n (%) | Male | 60 (77) | 24 (40) | 36 (60) | 0.29 | 55 (92) | 5 (8) | 0.38 |
| Female | 18 (23) | 10 (56) | 8 (44) | 15 (83) | 3 (17) | |||
| ASA score, n (%) | I | 9 (12) | 5 (56) | 4 (44) | 0.76 | 9 (100) | 0 (0) | 0.65 |
| II | 46 (59) | 19 (41) | 27 (59) | 40 (87) | 6 (13) | |||
| III | 23 (30) | 10 (44) | 13 (57) | 21 (91) | 2 (9) | |||
| cTNM stage (7th edition), n (%) | IB (cT2N0) | 6 (8) | 5 (83) | 1 (17) | 0.05 | 6 (100) | 0 (0) | 0.38 |
| IIA (cT3N0) | 20 (26) | 9 (45) | 11 (55) | 18 (90) | 2 (10) | |||
| IIB (cT2N1) | 7 (9) | 2 (29) | 5 (71) | 7 (100) | 0 (0) | |||
| IIIA (cT2N2, cT3N1 or cT4N0) | 29 (37) | 15 (52) | 14 (48) | 27 (93) | 2 (7) | |||
| IIIB (cT3N2) | 16 (21) | 3 (19) | 13 (81) | 12 (75) | 4 (25) | |||
| Gross tumor volume (cm3), median (range) | 41 (7–174) | 32 (7–174) | 54 (14–117) | 0.02 | 39 (7–174) | 72 (40–88) | 0.04 | |
| Subtype, n (%) | Adenocarcinoma | 68 (87) | 32 (47) | 36 (53) | 0.29 | 62 (91) | 6 (9) | 0.40 |
| Squamous cell carcinoma | 7 (9) | 1 (14) | 6 (86) | 5 (71) | 2 (29) | |||
| Adenosquamous carcinoma | 2 (3) | 1 (50) | 1 (50) | 2 (100) | 0 (0) | |||
| Undifferentiated | 1 (1) | 0 (0) | 1 (100) | 1 (100) | 0 (0) | |||
| Differentiation, n (%) | Good-moderate | 38 (49) | 15 (40) | 23 (61) | 0.06 | 35 (92) | 3 (8) | 0.48 |
| Poor | 35 (45) | 19 (54) | 16 (46) | 31 (89) | 4 (11) | |||
| Not determined | 5 (6) | 0 (0) | 5 (100) | 4 (80) | 1 (20) | |||
| Follow-up progression free survival (months), median (range) | 28 (1–55) | 26 (1–53) | 30 (1–55) | 0.55 | 29 (1–55) | 6 (2–44) | 0.12 | |
| Follow-up overall survival (months), median (range) | 30 (3–55) | 29 (5–54) | 32 (3–55) | 0.90 | 32 (5–55) | 14 (3–44) | 0.07 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hofste, L.S.M.; Geerlings, M.J.; von Rhein, D.; Tolmeijer, S.H.; Weiss, M.M.; Gilissen, C.; Hofste, T.; Garms, L.M.; Janssen, M.J.R.; Rütten, H.; et al. Circulating Tumor DNA-Based Disease Monitoring of Patients with Locally Advanced Esophageal Cancer. Cancers 2022, 14, 4417. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14184417
Hofste LSM, Geerlings MJ, von Rhein D, Tolmeijer SH, Weiss MM, Gilissen C, Hofste T, Garms LM, Janssen MJR, Rütten H, et al. Circulating Tumor DNA-Based Disease Monitoring of Patients with Locally Advanced Esophageal Cancer. Cancers. 2022; 14(18):4417. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14184417
Chicago/Turabian StyleHofste, Lisa S. M., Maartje J. Geerlings, Daniel von Rhein, Sofie H. Tolmeijer, Marjan M. Weiss, Christian Gilissen, Tom Hofste, Linda M. Garms, Marcel J. R. Janssen, Heidi Rütten, and et al. 2022. "Circulating Tumor DNA-Based Disease Monitoring of Patients with Locally Advanced Esophageal Cancer" Cancers 14, no. 18: 4417. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14184417