
Predicting Immunotherapy Outcomes in Older Patients with Solid Tumors Using the LIPI Score
 , , ,
, , ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. LIPI Score
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Pretreatment LIPI Score
3.3. Clinical Profile According to the LIPI Score
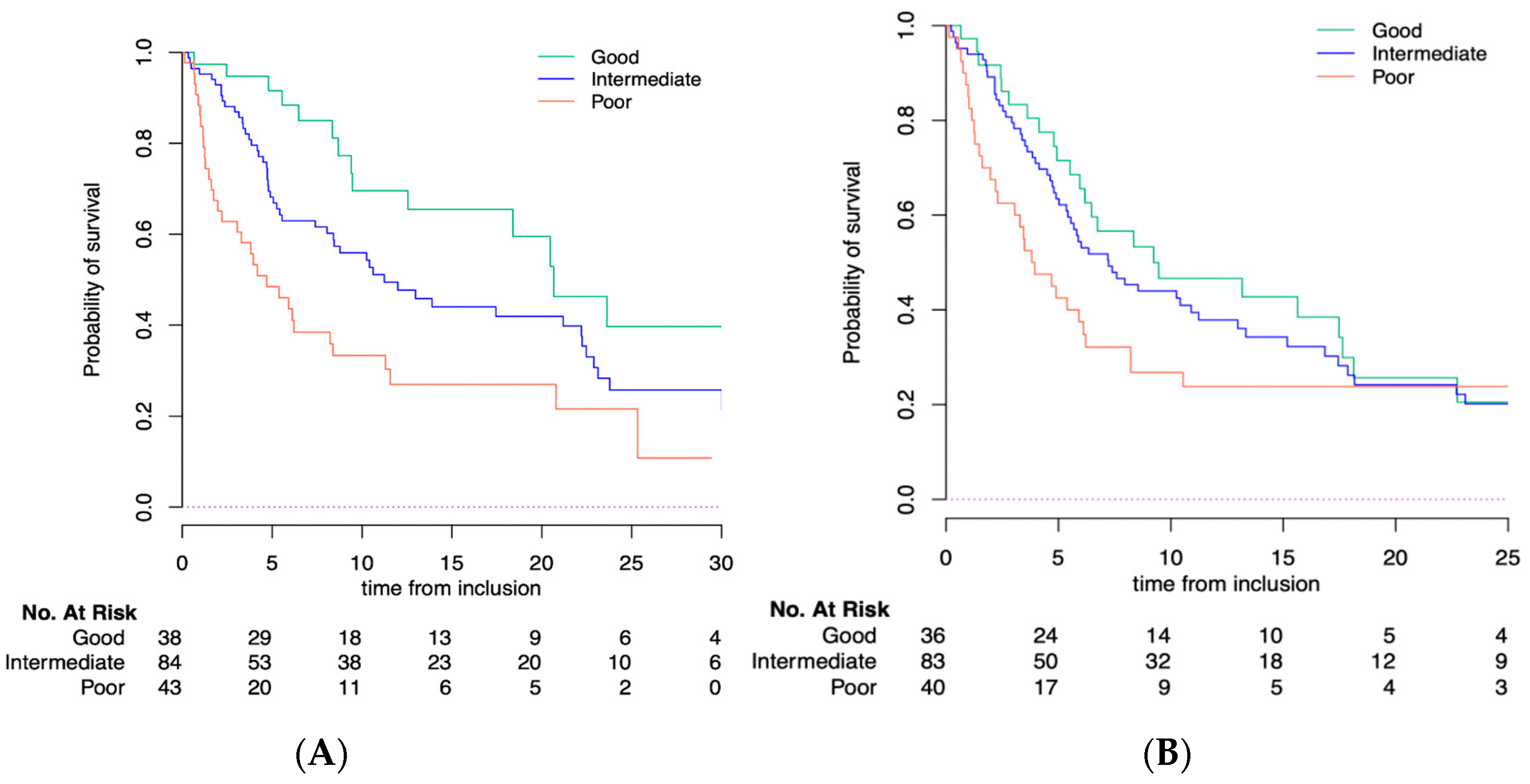
3.4. LIPI Is Correlated with ICB Outcomes
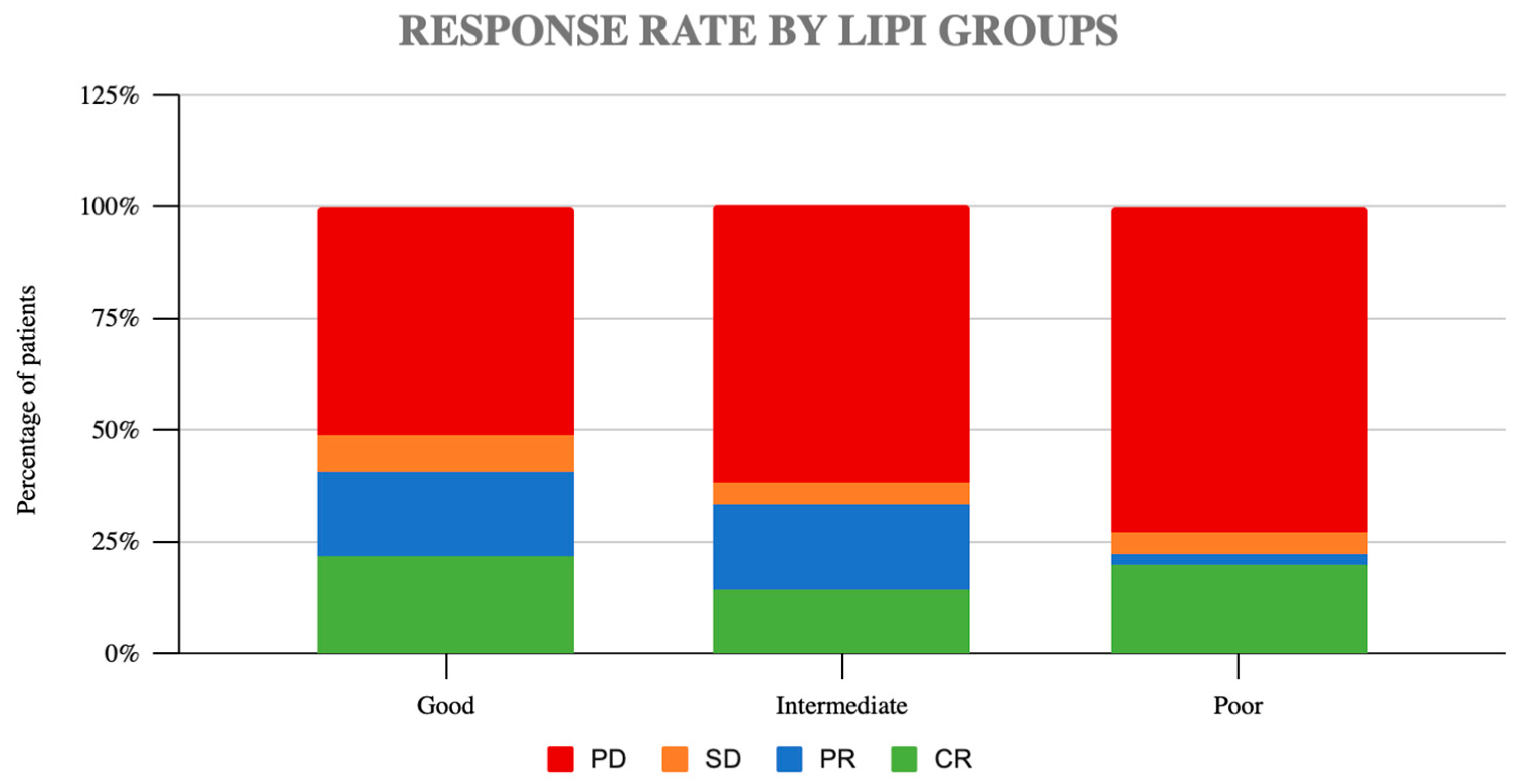
3.5. LIPI Is Correlated with ICB Response
3.6. Early Death and Response Rate
3.7. Pretreatment LIPI Score and Immune-Related Events (irAEs)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mok, T.S.; Wu, Y.L.; Kudaba, I.; Kowalski, D.M.; Cho, B.C.; Turna, H.Z.; Castro, G., Jr.; Srimuninnimit, V.; Laktionov, K.K.; Bondarenko, I.; et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): A randomised, open-label, controlled, phase 3 trial. Lancet 2019, 393, 1819–1830. [Google Scholar] [CrossRef]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motzer, R.J.; Escudier, B.; McDermott, D.F.; George, S.; Hammers, H.J.; Srinivas, S.; Tykodi, S.S.; Sosman, J.A.; Procopio, G.; Plimack, E.R.; et al. Nivolumab versus Everolimus in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2015, 373, 1803–1813. [Google Scholar] [CrossRef] [Green Version]
- Balar, A.V.; Galsky, M.D.; Rosenberg, J.E.; Powles, T.; Petrylak, D.P.; Bellmunt, J.; Loriot, Y.; Necchi, A.; Hoffman-Censits, J.; Perez-Gracia, J.L.; et al. Atezolizumab as first-line treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: A single-arm, multicentre, phase 2trial. Lancet 2017, 389, 67–76. [Google Scholar] [CrossRef] [Green Version]
- Robert, C.; Schachter, J.; Long, G.V.; Arance, A.; Grob, J.J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.; Lotem, M.; et al. Pembrolizumab versus Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2015, 372, 2521–2532. [Google Scholar] [CrossRef] [PubMed]
- Baldini, C.; Romano, P.M.; Voisin, A.-L.; Danlos, F.-X.; Champiat, S.; Laghouati, S.; Kfoury, M.; Vincent, H.; Postel-Vinay, S.; Varga, A.; et al. Impact of aging on immune-related adverse events generated by anti-programmed death (ligand)PD-(L)1 therapies. Eur. J. Cancer 2020, 129, 71–79. [Google Scholar] [CrossRef]
- Nishijima, T.F.; Muss, H.B.; Shachar, S.S.; Moschos, S.J. Comparison of efficacy of immune checkpoint inhibitors (ICIs) between younger and older patients: A systematic review and meta-analysis. Cancer Treat. Rev. 2016, 45, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Champiat, S.; Dercle, L.; Ammari, S.; Massard, C.; Hollebecque, A.; Postel-Vinay, S.; Chaput, N.; Eggermont, A.; Marabelle, A.; Soria, J.C.; et al. Hyperprogressive Disease Is a New Pattern of Progression in Cancer Patients Treated by Anti-PD-1/PD-L1. Clin. Cancer Res. 2017, 23, 1920–1928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.Y.; Kronbichler, A.; Eisenhut, M.; Hong, S.H.; van der Vliet, H.J.; Kang, J.; Shin, J.I.; Gamerith, G. Tumor Mutational Burden and Efficacy of Immune Checkpoint Inhibitors: A Systematic Review and Meta-Analysis. Cancers 2019, 11, 1798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ready, N.; Hellmann, M.D.; Awad, M.M.; Otterson, G.A.; Gutierrez, M.; Gainor, J.F.; Borghaei, H.; Jolivet, J.; Horn, L.; Mates, M.; et al. First-Line Nivolumab Plus Ipilimumab in Advanced Non-Small-Cell Lung Cancer (CheckMate 568): Outcomes by Programmed Death Ligand 1 and Tumor Mutational Burden as Biomarkers. J. Clin. Oncol. 2019, 37, 992–1000. [Google Scholar] [CrossRef] [PubMed]
- Le, D.T.; Uram, J.N.; Wang, H.; Bartlett, B.R.; Kemberling, H.; Eyring, A.D.; Skora, A.D.; Luber, B.S.; Azad, N.S.; Laheru, D.; et al. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N. Engl. J. Med. 2015, 372, 2509–2520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charrier, M.; Mezquita, L.; Lueza, B.; Dupraz, L.; Planchard, D.; Remon, J.; Caramella, C.; Cassard, L.; Boselli, L.; Reiners, K.; et al. Circulating innate immune markers and outcomes in treatment-naïve advanced non-small cell lung cancer patients. Eur. J. Cancer 2019, 108, 88–96. [Google Scholar] [CrossRef]
- Benitez, J.C.; Recondo, G.; Rassy, E.; Mezquita, L. The LIPI score and inflammatory biomarkers for selection of patients with solid tumors treated with checkpoint inhibitors. Q. J. Nucl. Med. Mol. Imaging 2020, 64, 162–174. [Google Scholar] [CrossRef]
- Mezquita, L.; Auclin, E.; Ferrara, R.; Charrier, M.; Remon, J.; Planchard, D.; Ponce, S.; Ares, L.P.; Leroy, L.; Audigier-Valette, C.; et al. Association of the Lung Immune Prognostic Index with Immune Checkpoint Inhibitor Outcomes in Patients with Advanced Non-Small Cell Lung Cancer. JAMA Oncol. 2018, 4, 351–357. [Google Scholar] [CrossRef]
- Le Burel, S.; Champiat, S.; Mateus, C.; Marabelle, A.; Michot, J.M.; Robert, C.; Belkhir, R.; Soria, J.C.; Laghouati, S.; Voisin, A.L.; et al. Prevalence of immune-related systemic adverse events in patienttreated with anti-Programmed cell Death 1/anti-Programmed cell Death-Ligand 1 agents: A single-centre pharmacovigilance database analysis. Eur. J. Cancer 2017, 82, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Seymour, L.; Bogaerts, J.; Perrone, A.; Ford, R.; Schwartz, L.H.; Mandrekar, S.; Lin, N.U.; Litière, S.; Dancey, J.; Chen, A.; et al. iRECIST: Guidelines for response criteria for use in trials testing immunotherapeutics. Lancet Oncol. 2017, 18, e143–e152. [Google Scholar] [CrossRef] [Green Version]
- Varga, A.; Bernard-Tessier, A.; Auclin, E.; Pérez, L.M.; Baldini, C.; Planchard, D.; Marabelle, A.; Hollebecque, A.; Besse, B.; Massard, C. Applicability of the lung immune prognostic index (LIPI) in patients with metastatic solid tumors when treated with immune checkpoint inhibitors (ICI) in early clinical trials. Ann. Oncol. 2019, 30, i2. [Google Scholar] [CrossRef]
- Riudavets, M.; Auclin, E.; Mezquita, L. Host circulating biomarkers for immune-checkpoint inhibitors: Single-agent and combinations. Future Oncol. 2020, 16, 1665–1668. [Google Scholar] [CrossRef] [PubMed]
- Recondo, G.; Mezquita, L. Clinical efficacy, predictive biomarkers and response patterns of immunotherapy combinations for patients with cancer. Future Oncol. 2020, 16, 1659–1664. [Google Scholar] [CrossRef]
- Schernberg, A.; Mezquita, L.; Boros, A.; Botticella, A.; Caramella, C.; Besse, B.; Escande, A.; Planchard, D.; Le Péchoux, C.; Deutsch, E. Neutrophilia as prognostic biomarker in locally advanced stage III lung cancer. PLoS ONE 2018, 13, e0204490. [Google Scholar] [CrossRef] [PubMed]
- MacGregor, R.R.; Shalit, M. Neutrophil function in healthy elderly subjects. J. Gerontol. 1990, 45, M55–M60. [Google Scholar] [CrossRef] [PubMed]
- Butcher, S.K.; Chahal, H.; Nayak, L.; Sinclair, A.; Henriquez, N.V.; Sapey, E.; O’Mahony, D.; Lord, J.M. Senescence in innate immune responses: Reduced neutrophil phagocytic capacity and CD16 expression in elderly humans. J. Leukoc. Biol. 2001, 70, 881–886. [Google Scholar] [CrossRef]
- Magombedze, G.; Reddy PB, J.; Eda, S.; Ganusov, V.V. Cellular and population plasticity of helper CD4(+) T cell responses. Front. Physiol. 2013, 4, 206. [Google Scholar] [CrossRef] [Green Version]
- Franceschi, C.; Campisi, J. Chronic inflammation (inflammaging) and its potential contribution to age-associated diseases. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69 (Suppl. 1), S4–S9. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, A.; Stockwell, P.A.; Rodger, E.J.; Duncan, E.J.; Parry, M.F.; Weeks, R.J.; Morison, I.M. Genome-wide DNA methylation map of human neutrophils reveals widespread inter-individual epigenetic variation. Sci. Rep. 2015, 5, 17328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.; Ge, B.; Casale, F.P.; Vasquez, L.; Kwan, T.; Garrido-Martín, D.; Watt, S.; Yan, Y.; Kundu, K.; Ecker, S.; et al. Genetic Drivers of Epigenetic and Transcriptional Variation in Human Immune Cells. Cell 2016, 167, 1398–1414.e24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ecker, S.; Chen, L.; Pancaldi, V.; Bagger, F.O.; Fernández, J.M.; Carrillo de Santa Pau, E.; Juan, D.; Mann, A.L.; Watt, S.; Casale, F.P.; et al. Genome-wide analysis of differential transcriptional and epigenetic variability across human immune cell types. Genome Biol. 2017, 18, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanc-Durand, F.; Auclin, E.; Planchard, D.; Aix, S.P.; Hendriks, L.; Sullivan, I.; Saravia, D.; Routy, B.; Castro, R.L.; Pilotto, S.; et al. Association of lung immune prognostic index (LIPI) with survival of first line immune checkpoint inhibitors single agent or in combination with chemotherapy in untreated advanced NSCLC patients. Ann. Oncol. 2019, 30, xi5. [Google Scholar] [CrossRef]
- Ferrara, R.; Mezquita, L.; Texier, M.; Lahmar, J.; Audigier-Valette, C.; Tessonnier, L.; Mazieres, J.; Zalcman, G.; Brosseau, S.; Le Moulec, S.; et al. Hyperprogressive Disease in Patients with Advanced Non-Small Cell Lung Cancer Treated with PD-1/PD-L1 Inhibitors or with Single-Agent Chemotherapy. JAMA Oncol. 2018, 4, 1543–1552. [Google Scholar] [CrossRef] [PubMed]
- Kas, B.; Talbot, H.; Ferrara, R.; Richard, C.; Lamarque, J.-P.; Pitre-Champagnat, S.; Planchard, D.; Balleyguier, C.; Besse, B.; Mezquita, L.; et al. Clarification of Definitions of Hyperprogressive Disease during Immunotherapy for Non-Small Cell Lung Cancer. JAMA Oncol. 2020, 6, 1039–1046. [Google Scholar] [CrossRef]
- Kim, Y.; Kim, C.H.; Lee, H.Y.; Lee, S.-H.; Kim, H.S.; Lee, S.; Cha, H.; Hong, S.; Kim, K.; Seo, S.W.; et al. Comprehensive Clinical and Genetic Characterization of Hyperprogression Based on Volumetry in Advanced Non-Small Cell Lung Cancer Treated with Immune Checkpoint Inhibitor. J. Thorac. Oncol. 2019, 14, 1608–1618. [Google Scholar] [CrossRef]
- Mezquita, L.; Preeshagul, I.; Auclin, E.; Saravia, D.; Hendriks, L.; Rizvi, H.; Park, W.; Nadal, E.; Martin-Romano, P.; Ruffinelli, J.C.; et al. Predicting immunotherapy outcomes under therapy in patients with advanced NSCLC using dNLR and its early dynamics. Eur. J. Cancer 2021, 151, 211–220. [Google Scholar] [CrossRef]
- Gomes, F.; Lorigan, P.; Woolley, S.; Foden, P.; Burns, K.; Yorke, J.; Blackhall, F. A prospective cohort study on the safety of checkpoint inhibitors in older cancer patients—The ELDERS study. ESMO Open 2021, 6, 100042. [Google Scholar] [CrossRef]
- Soubeyran, P.; Bellera, C.; Goyard, J.; Heitz, D.; Curé, H.; Rousselot, H.; Albrand, G.; Servent, V.; Jean, O.S.; Van Praagh, I.; et al. Screening for vulnerability in older cancer patients: The ONCODAGE Prospective Multicenter Cohort Study. PLoS ONE 2014, 9, e115060. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
|
Overall Population, n = 191 (100%) | LIPI Good n = 38 (23%) | Intermediate LIPI n = 84 (51%) | Poor LIPI n = 43 (26%) | |
|---|---|---|---|---|
| Age | ||||
| median, range | 77 (70–93) | 78 (70–91) | 78 (70–93) | 76 (70–89) |
| Gender | ||||
| Female | 74 (39%) | 20 (52%) | 28 (33%) | 16 (37%) |
| Male | 117 (61%) | 18 (47%) | 56 (67%) | 27 (62%) |
| Cancer type | ||||
| Melanoma | 127 (66.5%) | 31(81.5%) | 58 (69%) | 31(72%) |
| Merkel cell | 2 (1%) | 0 (0%) | 2 (2.3%) | 0 (0%) |
| NSCLC | 29 (15%) | 4 (10.5%) | 10 (11.9%) | 7 (16.2%) |
| SCLC | 22 (11,5%) | 0 (0%) | 10 (11.9%) | 3 (6.9%) |
| Urothelial | 7 (3.6%) | 2 (5%) | 1 (1%) | 2 (4.6%) |
| HNSCC | 1 (0.5%) | 1 (2.6%) | 0 (0%) | 0 (0%) |
| Main sites of metastasis | ||||
| Skin | 37 (19.3%) | 7 (18.4%) | 19 (22.6%) | 7 (16.2%) |
| Lymph nodes | 84 (43.9%) | 14 (36.8%) | 38 (45.2%) | 25 (58.1%) |
| Lung | 71 (37%) | 11 (28.9%) | 28 (33.3%) | 23 (53.4%) |
| Liver | 37 (19.3%) | 4 (15.5%) | 14 (16.6%) | 12 (27.9%) |
| Bones | 49 (25.6%) | 8 (21%) | 18 (21.4%) | 12 (27.9%) |
| Adrenal glands | 20 (10.4%) | 3 (7.8%) | 8 (9.5%) | 3 (6.9%) |
| Kidney | 6 (3%) | 0 (0%) | 2 (2.3%) | 1 (2.3%) |
| Spleen | 8 (4%) | 4 (10.5%) | 3 (3.5%) | 1 (2.3%) |
| Gastrointestinal | 11 (5.7%) | 3 (7.8%) | 3 (3.5%) | 3 (6.9%) |
| Brain | 37 (19.3%) | 2 (5.2%) | 17 (20.2%) | 14 (32%) |
| Thyroid | 2 (1%) | 0 (0%) | 2 (2.3%) | 0 (0%) |
| Pancreas | 1 (0.5%) | 0 (0%) | 1 (1%) | 0 (0%) |
| Performance status ECOG | ||||
| 0–1 | 160 (84.2%) | 38 (100%) | 73 (88%) | 32 (74%) |
| ≥2 | 30 (15.7%) | 0(0%) | 10 (12%) | 11 (25.5%) |
| Missing | 1 (0.5%) | 0 (0%) | 1 (0.5%) | 0 (0%) |
| Line of treatment | ||||
| ≤2 | 170 (89%) | 36 (95%) | 79 (94%) | 33 (77%) |
| >2 | 21(11%) | 2 (5%) | 5 (6%) | 10 (23%) |
| Missing | 0 | 0 | 0 | 0 |
| Type of immunotherapy | ||||
| Anti PD1 | 182 (95.2%) | 36 (94.7%) | 81 (96.4%) | 41(95.3%) |
| Anti PD(L)1 | 9 (4.7%) | 2 (5.2%) | 3 (3.5%) | 2 (4.6%) |
| Types of anti PD(L)1 | ||||
| Avelumab | 2 (1%) | 0 (0%) | 2 (2.3%) | 0 (0%) |
| Atezolizumab | 7 (3.6%) | 2 (5.2%) | 1(1.1%) | 2 (4.6%) |
| Pembrolizumab | 114 (59.6%) | 29 (76.3%) | 50 (59.5%) | 28 (65%) |
| Nivolumab | 68 (35.6%) | 7(18.4%) | 31 (36.9%) | 13 (30.2%) |
| Steroids at baseline | ||||
| Dose >20 mg (prednisone equivalent) | 25 (13.3%) | 2 (5.2%) | 11(13.2%) | 8 (18.6%) |
| Multivariate Analysis | PFS | OS | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Gender | ||||||
| Male | 1.201 | 0.78–1.83 | 0.401 | 1.392 | 0.87–2.22 | 0.164 |
| Histology | ||||||
| NSCLC | 1.81 | 1.08–3.04 | 0.05 | 1.70 | 0.97–2.95 | 0.06 |
| Urothelial | 2.27 | 0.66–7.77 | 0.05 | 2.47 | 0.62–9.77 | 0.19 |
| Other | 3.47 | 0.81–14.75 | 0.05 | 4.52 | 0.58–34.71 | 0.14 |
| Main sites of metastasis | ||||||
| Lung | 1.09 | 0.72–1.65 | 0.66 | 1.174 | 0.75–1.83 | 0.48 |
| Liver | 1.50 | 0.90–2.52 | 0.11 | 1.55 | 0.90–2.66 | 0.10 |
| Bone | 1.23 | 0.74–2.05 | 0.40 | 1.12 | 0.65–1.91 | 0.66 |
| Adrenal glands | 1.90 | 1.01–3.54 | 0.04 | 2.64 | 1.40–4.95 | 0.003 |
| Brain | 1.29 | 0.78–2.11 | 0.31 | 1.18 | 0.70–1.99 | 0.52 |
| Immunotherapy line | ||||||
| >Second line | 0.967 | 0.48–1.93 | 0.92 | 0.549 | 0.26–1.16 | 0.116 |
| Concomitant Steroids dose prednisone equivalent | ||||||
| 2.39 | 1.32–4.32 | 0.004 | 2.637 | 1.44–4.80 | 0.002 | |
| PS | ||||||
| ≥2 | 2.012 | 1.05–3.84 | 0.035 | 1.728 | 0.87–3.41 | 0.115 |
| Albumin | ||||||
| Low | 1.652 | 0.95–2.86 | 0.073 | 2.394 | 1.35–4.22 | 0.003 |
| LIPI score | ||||||
| Intermediate | 0.865 | 0.52–1.42 | 0.36 | 1.391 | 0.77–2.50 | 0.008 |
| Poor | 1.224 | 0.66–2.24 | 2.77 | 1.37–5.59 | ||
|
Overall Population n = 191 (100%) |
LIPI Good n = 38 (23%) |
Intermediate LIPI n = 84 (51%) |
Poor LIPI n = 43 (26%) | |
|---|---|---|---|---|
| irAES | 63 (32.9%) | 17 (44%) | 26 (30.9%) | 13 (30.2%) |
| Median Grade CTCAE | 2.43 | 2.47 | 2.42 | 2.46 |
| Types irAEs | ||||
| Skin | 29 (15%) | 5 (13%) | 14 (16%) | 6 (14%) |
| Lung | 5 (2.6%) | 1 (2.6%) | 4 (4.7%) | 0 (0%) |
| Liver | 6 (3%) | 3 (7.8%) | 3 (3.5%) | 0 (0%) |
| GI | 6 (3%) | 2 (5.2%) | 1 (1%) | 1 (2%) |
| Thyroid | 17 (8.9%) | 5 (13%) | 8 (9%) | 2 (4.6%) |
| Pancreas | 3 (1.5%) | 2 (5.2%) | 1 (1%) | 0 (0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pierro, M.; Baldini, C.; Auclin, E.; Vincent, H.; Varga, A.; Martin Romano, P.; Vuagnat, P.; Besse, B.; Planchard, D.; Hollebecque, A.; et al. Predicting Immunotherapy Outcomes in Older Patients with Solid Tumors Using the LIPI Score. Cancers 2022, 14, 5078. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14205078
Pierro M, Baldini C, Auclin E, Vincent H, Varga A, Martin Romano P, Vuagnat P, Besse B, Planchard D, Hollebecque A, et al. Predicting Immunotherapy Outcomes in Older Patients with Solid Tumors Using the LIPI Score. Cancers. 2022; 14(20):5078. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14205078
Chicago/Turabian StylePierro, Monica, Capucine Baldini, Edouard Auclin, Hélène Vincent, Andreea Varga, Patricia Martin Romano, Perrine Vuagnat, Benjamin Besse, David Planchard, Antoine Hollebecque, and et al. 2022. "Predicting Immunotherapy Outcomes in Older Patients with Solid Tumors Using the LIPI Score" Cancers 14, no. 20: 5078. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14205078