
Impact of Change in Body Composition during Follow-Up on the Survival of GEP-NET

 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
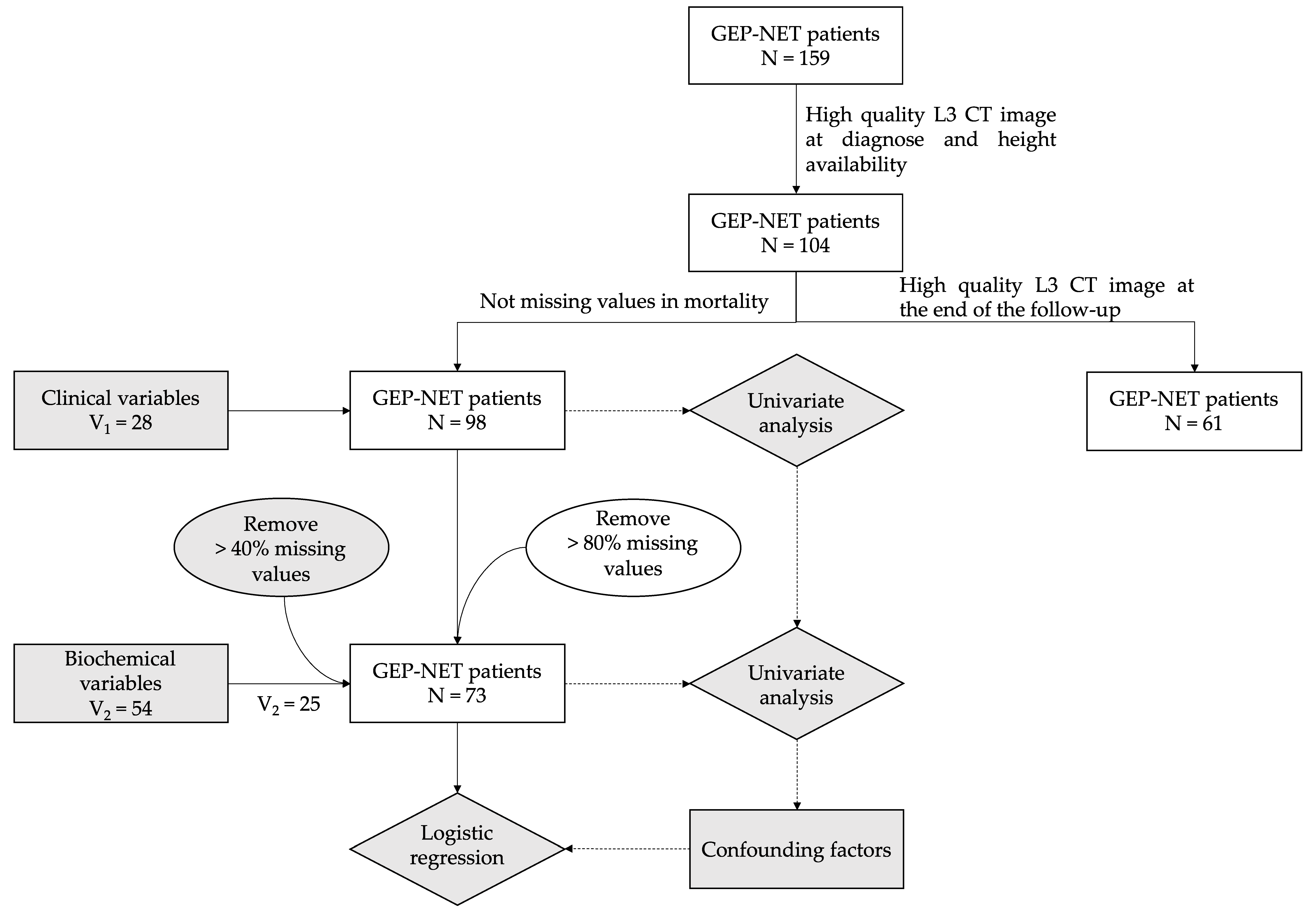
2.1. Recruitment and Variable Collection
2.2. Analysis of CT Images
2.3. Statistical Analysis
3. Results
3.1. Cohort Descriptaion
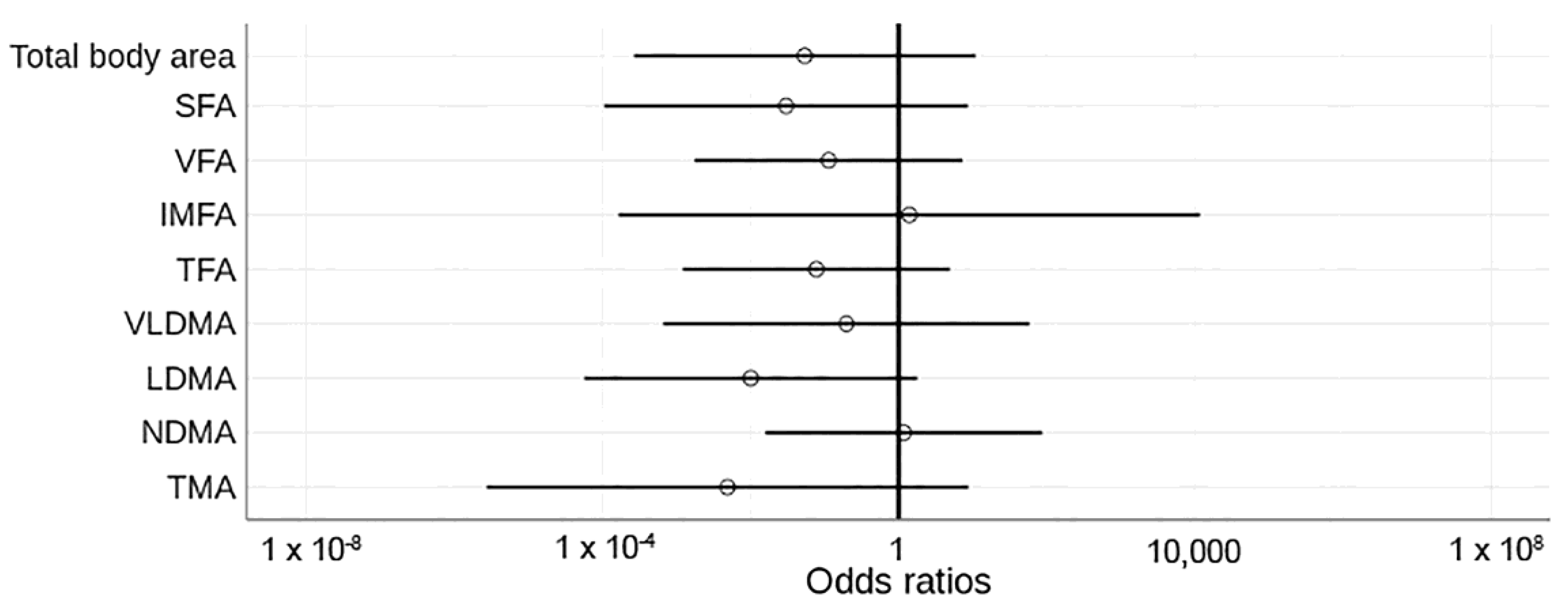
3.2. Variations of Body Composition, Clinical and Biochemical Profile in Relation with Mortality of the Disease
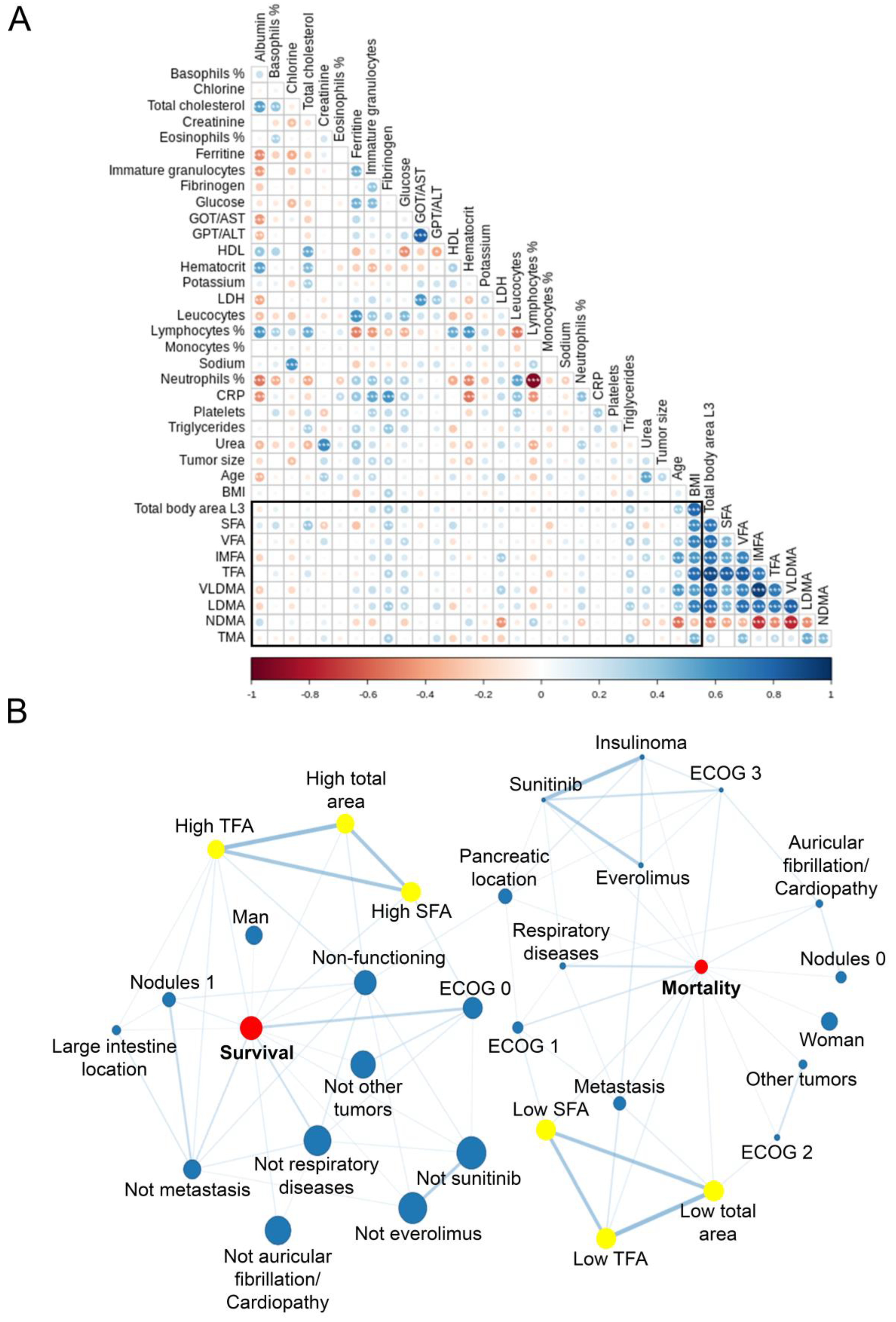
3.3. Correlations between Body Composition and Clinico-Biochemical Variable in Relation to Survival
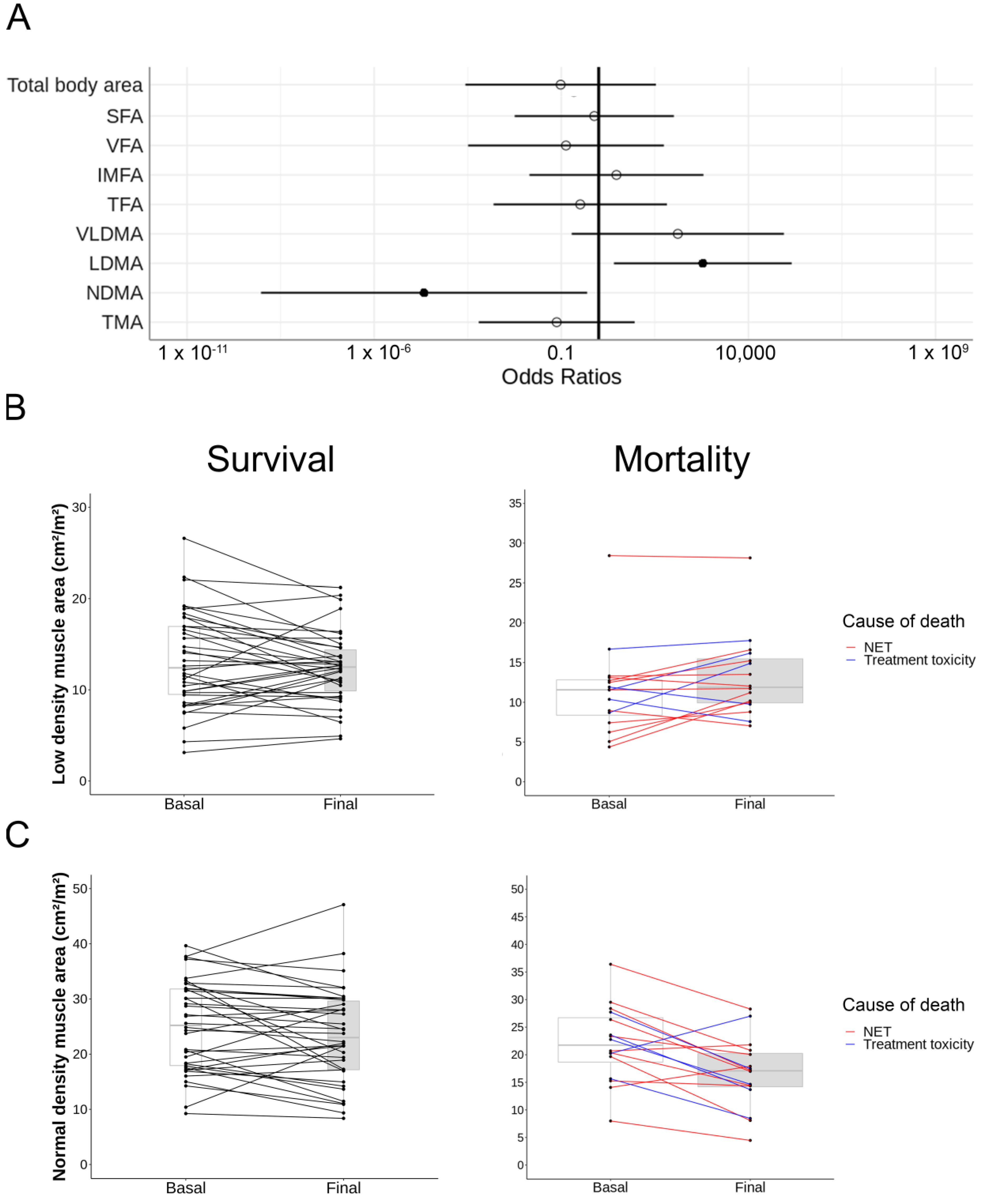
3.4. Body Composition Changes during Follow-Up Have an Impact on Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients With Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335. [Google Scholar] [CrossRef]
- Nuñez-Valdovinos, B.; Carmona-Bayonas, A.; Jimenez-Fonseca, P.; Capdevilla, J.; Castaño, Á.; Benavent, M.; Barrio, J.J.P.; Teule, A.; Alonso, V.; Custodio, A.; et al. Neuroendocrine Tumor Heterogeneity Adds Uncertainty to the World Health Organization 2010 Classification: Real-World Data from the Spanish Tumor Registry (R-GETNE). Oncologist 2018, 23, 422–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sampedro-Núñez, M.; Serrano-Somavilla, A.; Adrados, M.; Cameselle-Teijeiro, J.M.; Blanco-Carrera, C.; Cabezas-Agricola, J.M.; Martínez-Hernández, R.; Martín-Pérez, E.; de Nova, J.L.; Díaz, J.A.; et al. Analysis of expression of the PD-1/PD-L1 immune checkpoint system and its prognostic impact in gastroenteropancreatic neuroendocrine tumors. Sci. Rep. 2018, 8, 17812. [Google Scholar] [CrossRef] [Green Version]
- Carmona-Bayonas, A.; Jiménez-Fonseca, P.; Lamarca, Á.; Barriuso, J.; Castaño, Á.; Benavent, M.; Alonso, V.; del Riesco-Martínez, M.C.; Alonso-Gordoa, T.; Custodio, A.; et al. Prediction of Progression-Free Survival in Patients With Advanced, Well-Differentiated, Neuroendocrine Tumors Being Treated With a Somatostatin Analog: The GETNE-TRASGU Study. J. Clin. Oncol. 2019, 37, 2571–2580. [Google Scholar] [CrossRef]
- Lennon, H.; Sperrin, M.; Badrick, E.; Renehan, A.G. The Obesity Paradox in Cancer: A Review. Curr. Oncol. Rep. 2016, 18, 56. [Google Scholar] [CrossRef] [Green Version]
- Altieri, B.; Barrea, L.; Modica, R.; Muscogiuri, G.; Savastano, S.; Colao, A.; Faggiano, A. Nutrition and neuroendocrine tumors: An update of the literature. Rev. Endocr. Metab. Disord. 2018, 19, 159–167. [Google Scholar] [CrossRef]
- Laing, E.; Kiss, N.; Michael, M.; Krishnasamy, M. Nutritional Complications and the Management of Patients with Gastroenteropancreatic Neuroendocrine Tumors. Neuroendocrinology 2020, 110, 430–442. [Google Scholar] [CrossRef]
- Davis, M.P.; Panikkar, R. Sarcopenia associated with chemotherapy and targeted agents for cancer therapy. Ann. Palliat. Med. 2019, 8, 86–101. [Google Scholar] [CrossRef]
- Meza-Valderrama, D.; Marco, E.; Dávalos-Yerovi, V.; Muns, M.D.; Tejero-Sánchez, M.; Duarte, E.; Sánchez-Rodríguez, D. Sarcopenia, Malnutrition, and Cachexia: Adapting Definitions and Terminology of Nutritional Disorders in Older People with Cancer. Nutrients 2021, 13, 761. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.; Birdsell, L.; MacDonald, N.; Reiman, T.; Clandinin, M.T.; Murphy, L.J.M.; Ghosh, S.; Sawyer, M.B.; Baracos, V.E. Cancer Cachexia in the Age of Obesity: Skeletal Muscle Depletion Is a Powerful Prognostic Factor, Independent of Body Mass Index. J. Clin. Oncol. 2013, 31, 1539–1547. [Google Scholar] [CrossRef]
- Bauer, J.M.; Cruz-Jentoft, A.J.; Fielding, R.A.; Kanis, J.A.; Reginster, J.-Y.; Bruyère, O.; Cesari, M.; Chapurlat, R.; Al-Daghri, N.; Dennison, E.; et al. Is There Enough Evidence for Osteosarcopenic Obesity as a Distinct Entity? A Critical Literature Review. Calcif. Tissue Int. 2019, 105, 109–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- di Filippo, L.; de Lorenzo, R.; Giustina, A.; Rovere-Querini, P.; Conte, C. Vitamin D in Osteosarcopenic Obesity. Nutrients 2022, 14, 1816. [Google Scholar] [CrossRef] [PubMed]
- Ticinesi, A.; Meschi, T.; Narici, M.V.; Lauretani, F.; Maggio, M. Muscle Ultrasound and Sarcopenia in Older Individuals: A Clinical Perspective. J. Am. Med. Dir. Assoc. 2017, 18, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Barbosa-Silva, M.C.G.; Barros, A.J. Bioelectrical impedance analysis in clinical practice: A new perspective on its use beyond body composition equations. Curr. Opin. Clin. Nutr. Metab. Care 2005, 8, 311–317. [Google Scholar] [CrossRef]
- Qureshi, S.A.; Burch, N.; Druce, M.; Hattersley, J.G.; Khan, S.; Gopalakrishnan, K.; Darby, C.; Wong, J.L.H.; Davies, L.; Fletcher, S.; et al. Screening for malnutrition in patients with gastro-entero-pancreatic neuroendocrine tumours: A cross-sectional study. BMJ Open 2016, 6, e010765. [Google Scholar] [CrossRef]
- Malietzis, G.; Aziz, O.; Bagnall, N.M.; Johns, N.; Fearon, K.C.; Jenkins, J.T. The role of body composition evaluation by computerized tomography in determining colorectal cancer treatment outcomes: A systematic review. Eur. J. Surg. Oncol. 2015, 41, 186–196. [Google Scholar] [CrossRef]
- Dam, T.T.; Peters, K.W.; Fragala, M.; Cawthon, P.M.; Harris, T.B.; McLean, R.; Shardell, M.; Alley, D.E.; Kenny, A.; Ferrucci, L.; et al. An Evidence-Based Comparison of Operational Criteria for the Presence of Sarcopenia. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2014, 69, 584–590. [Google Scholar] [CrossRef]
- Chu, M.P.; Li, Y.; Ghosh, S.; Sass, S.; Smylie, M.; Walker, J.; Sawyer, M.B. Body composition is prognostic and predictive of ipilimumab activity in metastatic melanoma. J. Cachexia Sarcopenia Muscle 2020, 11, 748–755. [Google Scholar] [CrossRef]
- Aleixo, G.F.P.; Shachar, S.S.; Nyrop, K.A.; Muss, H.B.; Malpica, L.; Williams, G.R. Myosteatosis and prognosis in cancer: Systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2020, 145, 102839. [Google Scholar] [CrossRef]
- Kikut, J.; Jasińska, A.; Pobłocki, J.; Brodowski, J.; Małgorzata, S. Assessment and State of Nutrition of Patients with Gastroenteropancreatic Neuroendocrine Neoplasms. Nutrients 2020, 12, 1961. [Google Scholar] [CrossRef]
- Daly, L.E.; Power, D.G.; O’Reilly, Á.; Donnellan, P.; Cushen, S.J.; O’Sullivan, K.; Twomey, M.; Woodlock, D.P.; Redmond, H.P.; Ryan, A.M. The impact of body composition parameters on ipilimumab toxicity and survival in patients with metastatic melanoma. Br. J. Cancer 2017, 116, 310–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Findlay, M.; White, K.; Brown, C.; Bauer, J.D. Nutritional status and skeletal muscle status in patients with head and neck cancer: Impact on outcomes. J. Cachexia Sarcopenia Muscle 2021, 12, 2187–2198. [Google Scholar] [CrossRef] [PubMed]
- Falconi, M.; Eriksson, B.; Kaltsas, G.; Bartsch, D.K.; Capdevila, J.; Caplin, M.; Kos-Kudla, B.; Kwekkeboom, D.; Rindi, G.; Klöppel, G.; et al. ENETS Consensus Guidelines Update for the Management of Patients with Functional Pancreatic Neuroendocrine Tumors and Non-Functional Pancreatic Neuroendocrine Tumors. Neuroendocrinology 2016, 103, 153–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavel, M.; de Herder, W.W. ENETS Consensus Guidelines for the Standards of Care in Neuroendocrine Tumors. Neuroendocrinology 2017, 105, 193–195. [Google Scholar] [CrossRef] [Green Version]
- Rueden, C.T.; Schindelin, J.; Hiner, M.C.; DeZonia, B.E.; Walter, A.E.; Arena, E.T.; Eliceiri, K.W. ImageJ2: ImageJ for the next generation of scientific image data. BMC Bioinform. 2017, 18, 529. [Google Scholar] [CrossRef] [Green Version]
- Gomez-Perez, S.; McKeever, L.; Sheean, P. Tutorial: A Step-by-Step Guide (Version 2.0) for Measuring Abdominal Circumference and Skeletal Muscle From a Single Cross-Sectional Computed-Tomography Image Using the National Institutes of Health ImageJ. J. Parenter. Enter. Nutr. 2020, 44, 419–424. [Google Scholar] [CrossRef]
- Long, D.E.; Tezanos, A.G.V.; Wise, J.N.; Kern, P.A.; Bamman, M.M.; Peterson, C.A.; Dennis, R.A. A guide for using NIH Image J for single slice cross-sectional area and composition analysis of the thigh from computed tomography. PLoS ONE 2019, 14, e0211629. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Escobar, M.; Martinez-Uribe, L. Network Coincidence Analysis: The netCoin R Package. J. Stat. Softw. 2020, 93, 1–32. [Google Scholar] [CrossRef]
- Wang, J.; Xue, Z.; Lu, J.; He, Q.; Zheng, Z.; Xu, B.; Wie, J.; Li, P.; Xu, Y.; Lin, J.; et al. Effect of sarcopenia on short- and long-term outcomes in patients with gastric neuroendocrine neoplasms after radical gastrectomy: Results from a large, two-institution series. BMC Cancer 2020, 20, 1002. [Google Scholar] [CrossRef]
- Ranallo, N.; Iamurri, A.P.; Foca, F.; Liverani, C.; de Vita, A.; Mercatali, L.; Calabrese, C.; Spadazzi, C.; Fabbri, C.; Cavaliere, D.; et al. Prognostic and Predictive Role of Body Composition in Metastatic Neuroendocrine Tumor Patients Treated with Everolimus: A Real-World Data Analysis. Cancers 2022, 14, 3231. [Google Scholar] [CrossRef]
- Herrera-Martínez, Y.; Teomiro, C.A.; Idougourram, S.L.; Puertas, M.J.M.; Continente, A.C.; Blanch, R.S.; Castaño, J.P.; Moreno, M.Á.G.; Gahete, M.D.; Luque, R.M.; et al. Sarcopenia and Ghrelin System in the Clinical Outcome and Prognosis of Gastroenteropancreatic Neuroendocrine Neoplasms. Cancers 2021, 14, 111. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.L.; Clarke, S.J.; Engel, A.; Diakos, C.I.; Pavlakis, N.; Roach, P.J.; Bailey, D.L.; Bauer, J.; Findlay, M. Computed tomography (CT)-defined sarcopenia and myosteatosis are prevalent in patients with neuroendocrine neoplasms (NENs) treated with peptide receptor radionuclide therapy (PRRT). Eur. J. Clin. Nutr. 2022, 76, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Jeffery, E.; Lee, Y.C.G.; Newton, R.U.; Lyons-Wall, P.; McVeigh, J.; Fitzgerald, D.B.; Straker, L.; Peddle-Mclntyre, C.J. Changes in body composition in patients with malignant pleural mesothelioma and the relationship with activity levels and dietary intake. Eur. J. Clin. Nutr. 2022, 76, 979–986. [Google Scholar] [CrossRef]
- Borre, M.; Dam, G.A.; Knudsen, A.W.; Grønbaek, H. Nutritional status and nutritional risk in patients with neuroendocrine tumors. Scand. J. Gastroenterol. 2018, 53, 284–292. [Google Scholar] [CrossRef]
- Baracos, V.E.; Martin, L.; Korc, M.; Guttridge, D.C.; Fearon, K.C.H. Cancer-associated cachexia. Nat. Rev. Dis. Primers 2018, 4, 17105. [Google Scholar] [CrossRef]
- Murphy, K.T. The pathogenesis and treatment of cardiac atrophy in cancer cachexia. Am. J. Physiol. Heart Circulat. Physiol. 2016, 310, H466–H477. [Google Scholar] [CrossRef]
- Fearon, K.C.H.; Glass, D.J.; Guttridge, D.C. Cancer Cachexia: Mediators, Signaling, and Metabolic Pathways. Cell Metab. 2012, 16, 153–166. [Google Scholar] [CrossRef] [Green Version]
- Wen, Y.; Yang, J.; Han, X. Fibrinogen-to-Albumin Ratio is Associated with All-Cause Mortality in Cancer Patients. Int. J. Gen. Med. 2021, 14, 4867–4875. [Google Scholar] [CrossRef]
- Wu, J.; You, K.; Chen, C.; Zhong, H.; Jiang, Y.; Mo, H.; Song, J.; Qiu, X.; Liu, Y. High Pretreatment LDH Predicts Poor Prognosis in Hypopharyngeal Cancer. Front. Oncol. 2021, 11, 641682. [Google Scholar] [CrossRef]
- Dai, T.; Peng, L.; Lin, G.; Li, Y.; Yao, J.; Deng, Y.; Li, H.; Wang, G.; Liu, W.; Yang, Y.; et al. Preoperative elevated plasma fibrinogen level predicts tumor recurrence and poor prognosis in patients with hepatocellular carcinoma. J. Gastrointest. Oncol. 2019, 10, 1049–1063. [Google Scholar] [CrossRef]
- Muscaritoli, M.; Arends, J.; Bachmann, P.; Baraos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN practical guideline: Clinical Nutrition in cancer. Clin. Nutr. 2021, 40, 2898–2913. [Google Scholar] [CrossRef] [PubMed]
- García-Almeida, J.; García-García, C.; Vegas-Aguilar, I.M.; Pomar, M.D.B.; Cornejo-Pareja, I.M.; Medina, B.F.; de Román, D.A.; Guerrero, D.B.; Lesmes, I.B.; Madueño, F.J.T. Nutritional ultrasound®: Conceptualisation, technical considerations and standardisation. Endocrinol. Diabetes Nutr. 2022; in press. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Overall N = 98 |
|---|---|
| Age (years), mean (SD) | 63.34 (15.74) |
| Sex (M/F), N (%) | 50 (51.02%)/48 (48.98%) |
| Tumor location, N (%) | Small intestine: 34 (40.00%) Pancreas: 37 (38.95%) Large intestine: 19 (20.00%) Undefined: 1 (1.05%) |
| Exitus, N (%) | 33 (33.67%) |
| BMI (kg/m2), mean (SD) | 25.55 (4.60) |
| Total area (cm2/m2), mean (SD) | 262.09 (64.20) |
| Subcutaneous fat area (cm2/m2), mean (SD) | 66.92 (32.88) |
| Visceral fat area (cm2/m2), mean (SD) | 61.35 (38.86) |
| Intermuscular fat area (cm2/m2), mean (SD) | 5.58 (3.83) |
| Total fat area (cm2/m2), mean (SD) | 133.84 (59.29) |
| VLD muscle area (cm2/m2), mean (SD) | 4.86 (2.74) |
| LD muscle area (cm2/m2), mean (SD) | 13.23 (5.33) |
| ND muscle area (cm2/m2), mean (SD) | 23.76 (8.00) |
| Total muscle area (cm2/m2), mean (SD) | 42.36 (7.56) |
| Variable | Overall (N = 98) | Survival (N = 65) | Mortality (N = 33) | p Value |
|---|---|---|---|---|
| General clinical variables at diagnose | ||||
| Age * | 63.41 (15.80) | 60.58 (15.63) | 68.97 (14.82) | 0.01 |
| Female | 51 (52.04%) | 37 (56.92%) | 14 (42.42%) | 0.25 |
| Never smoked | 49 (57.65%) | 35 (64.91%) | 14 (51.85%) | 0.55 |
| Currently smoking | 17 (20.00%) | 11 (19.30%) | 6 (22.22%) | |
| Non currently smoking | 19 (22.35%) | 11 (19.30%) | 7 (25.93%) | |
| Weight + | 70.53 (16.71) | 74.49 (19.19) | 64.69 (9.97) | 0.02 |
| BMI + | 25.85 (4.65) | 26.64 (5.16) | 24.31 (2.96) | 0.01 |
| Tumor clinical variables | ||||
| Grade (G) | <0.01 | |||
| 0 | 2 (2.56%) | 1 (1.49%) | 1 (4.76%) | |
| 1 | 37 (47.44%) | 33 (49.25%) | 4 (19.05%) | |
| 2 | 26 (33.33%) | 20 (29.85%) | 6 (28.57%) | |
| 3 | 11 (14.10%) | 3 (4.48%) | 8 (38.09%) | |
| 4 | 2 (2.56%) | 0 | 2 (2.52%) | |
| ECOG 0 | 57 (60.00%) | 48 (77.42%) | 9 (27.27%) | <0.01 |
| ECOG 1 | 27 (28.42%) | 11 (17.74%) | 16 (48.48%) | |
| ECOG 2 | 8 (8.42%) | 3 (4.84%) | 5 (15.15%) | |
| ECOG 3 | 3 (3.16%) | 0 | 3 (9.09%) | |
| Carcinoid Syndrome | 19 (20.21%) | 11 (17.19%) | 8 (26.67%) | 0.19 |
| Gastrinoma | 3 (3.19%) | 2 (3.12%) | 1 (3.33%) | |
| Insulinoma | 4 (4.26%) | 1 (1.56%) | 3 (10.00%) | |
| Tumor size (mm) * | 40.25 (43.05) | 28. 94 (30.72) | 62.88 (54.48) | 0.01 |
| Functioning | 9 (11.39%) | 5 (9.80%) | 4 (14.29%) | 0.82 |
| Residual tumor: | 0.04 | |||
| 0 | 45 (48.91%) | 37 (57.81%) | 8 (28.57%) | |
| 1 | 37 (40.22%) | 21 (32.82%) | 16 (57.14%) | |
| NA | 10 (10.87%) | 6 (9.38%) | 4 (14.29%) | |
| Location of primary tumor: | 0.23 | |||
| Small intestine | 39 (41.05%) | 27 (41.54%) | 12 (40.00%) | |
| Pancreatic | 36 (37.89%) | 21 (32.31%) | 15 (50.00%) | |
| Large intestine | 19 (20.00%) | 16 (24.62%) | 3 (10.00%) | |
| Undefined | 1 (1.05%) | 1 (1.54%) | 0 | |
| Nodules | 0.12 | |||
| 0 | 23 (27.38%) | 13 (20%) | 10 (30.303%) | |
| 1 | 31 (36.9%) | 26 (40%) | 5 (15.152%) | |
| 2 | 21 (25%) | 15 (23.077%) | 6 (18.182%) | |
| 3 | 8 (9.52%) | 5 (7.692%) | 3 (9.091%) | |
| Nx | 1 (1.19%) | 0 (0%) | 1 (3.03%) | |
| Unknown | 10 (11.9%) | 5 (7.692%) | 5 (15.152%) | 0.01 |
| No metastasis | 45 (60.81%) | 38 (71.70%) | 7 (33.33%) | |
| Metastasis | 29 (39.19%) | 15 (28.30%) | 14 (66/67%) | |
| Incidental NET | 50 (52.63%) | 33 (51.56%) | 17 (54.84%) | 0.94 |
| Body composition in L3 CT images | ||||
| Body area + | 262.05 (64.24) | 269.19 (66.28) | 247.99 (58.43) | 0.11 |
| SFA + | 66.59 (33.12) | 72.25 (35.25) | 55.45 (25.44) | 0.01 |
| VFA * | 61.55 (38.72) | 64.34 (36.95) | 56.06 (42.03) | 0.15 |
| TFA + | 133.76 (59.36) | 142.03 (58.94) | 117.47 (57.62) | 0.05 |
| IMFA * | 5.61 (3.82) | 5.44 (4.12) | 5.95 (3.17) | 0.24 |
| VLDMA * | 4.88 (2.73) | 4.72 (2.65) | 5.20 (2.89) | 0.49 |
| LDMA + | 13.27 (5.29) | 13.55 (5.26) | 12.71 (5.39) | 0.46 |
| NDMA + | 23.67 (8.02) | 25.15 (8.17) | 20.76 (6.96) | 0.01 |
| TMA * | 42.33 (7.59) | 43.93 (7.37) | 39.18 (7.11) | <0.01 |
| Drugs–Treatment | ||||
| Metformin | 17 (19.10%) | 13 (21.67%) | 4 (13.79%) | 0.25 |
| Somatostatin Analogues | 32 (32.65%) | 20 (30.77%) | 12 (36.36%) | 0.74 |
| Everolimus | 6 (6.12%) | 2 (3.08%) | 4 (12.12%) | 0.19 |
| Sunitinib | 2 (2.04%) | 0 | 2 (6.06%) | 0.21 |
| Radionuclides | 8 (8.16%) | 5 (7.69%) | 3 (9.09%) | 1.000 |
| Other diseases at diagnosis | ||||
| Arterial hypertension | 47 (51.65%) | 30 (50.00%) | 17 (54.84%) | 0.83 |
| Diabetes Mellitus | 34 (35.05%) | 23 (35.38%) | 11 (34.38%) | 0.77 |
| Other tumors | 18 (19.78%) | 8 (13.33%) | 10 (32.26%) | 0.06 |
| Atrial fibrillation/Cardiopathy | 13 (14.29%) | 5 (8.33%) | 8 (25.81%) | 0.05 |
| Cardiovascular disease | 13 (14.29%) | 6 (10.00%) | 7 (22.58%) | 0.19 |
| Respiratory disease | 10 (11.11%) | 1 (1.69%) | 9 (29.03%) | <0.01 |
| Reuma | 11 (12.22%) | 6 (10.17%) | 5 (16.13%) | 0.55 |
| Infectious disease | 3 (3.33%) | 2 (3.39%) | 1 (3.23%) | 0.77 |
| Autoimmune disease | 9 (10.00%) | 5 (8.47%) | 4 (12.90%) | 0.62 |
| Biochemical variables at diagnosis | ||||
| Albumin * | 3.98 (0.61) | 4.09 (0.58) | 3.71 (0.61) | 0.02 |
| Fibrinogen + | 537.37 (155.60) | 551.67 (154.64) | 504.26 (156.86) | 0.28 |
| Glucose * | 117.37 (30.44) | 116.98 (31.43) | 118.26 (28.74) | 0.86 |
| Urea * | 37.85 (13.77) | 34.49 (11.00) | 45.21 (16.44) | 0.01 |
| Creatinine * | 0.90 (0.39) | 0.84 (0.25) | 1.04 (0.59) | 0.06 |
| Sodium + | 139.85 (2.24) | 140.03 (1.86) | 139.47 (2.92) | 0.43 |
| Potassium + | 4.28 (0.32) | 4.27 (0.27) | 4.29 (0.41) | 0.91 |
| GOT/AST * | 31.74 (36.72) | 22.94 (6.78) | 52.85 (63.05) | 0.04 |
| GPT/ALT * | 32.86 (31.05) | 28.64 (19.26) | 42.97 (48.26) | 0.52 |
| LDH * | 206.04 (79.70) | 182.53 (39.31) | 255.55 (115.35) | 0.02 |
| Cholesterol + | 167.30 (46.66) | 172.08 (46.89) | 156.33 (45.38) | 0.21 |
| HDL + | 44.22 (14.91) | 45.04 (15.71) | 42.70 (13.68) | 0.62 |
| Triglycerides * | 128.01 (71.10) | 135.78 (82.20) | 110.90 (31.96) | 0.52 |
| Ferritine * | 256.66 (509.75) | 155.67 (139.52) | 416.13 (795.94) | 0.14 |
| CRP * | 3.60 (3.91) | 3.50 (3.93) | 3.83 (3.97) | 0.56 |
| Hematocrit + | 4.32 (0.67) | 4.41 (0.63) | 4.14 (0.73) | 0.15 |
| Leucocytes * | 8.87 (3.11) | 8.79 (2.79) | 9.06 (3.82) | 0.46 |
| Lymphocytes (%) + | 20.49 (9.82) | 21.30 (9.38) | 18.62 (10.76) | 0.33 |
| Monocytes (%) + | 8.11 (2.20) | 8.02 (1.98) | 8.33 (2.68) | 0.64 |
| Neutrophils (%) + | 67.28 (10.52) | 66.96 (9.52) | 68.01 (12.74) | 0.74 |
| Immature granulocytes (%) * | 0.42 (0.34) | 0.43 (0.38) | 0.41 (0.22) | 0.66 |
| Eosinophils (%) * | 2.16 (1.43) | 2.10 (1.39) | 2.31 (1.55) | 0.54 |
| Basophils (%) * | 0.42 (0.23) | 0.43 (0.23) | 0.40 (0.21) | 0.50 |
| Platelets * | 257.30 (96.34) | 264.74 (99.90) | 240.29 (87.54) | 0.27 |
| Body Composition Measures | Status | Overall Mortality | p-Value * | Tumor-Cause Mortality | p-Value * |
|---|---|---|---|---|---|
| Total area (cm2/m2), mean (SD) | Survival | −0.88 (35.85) | 0.36 | 0.89 (37.01) | 0.44 |
| Mortality | −16.16 (50.37) | −1.90 (19.27) | |||
| Subcutaneous fat area (cm2/m2), mean (SD) | Survival | −0.47 (17.05) | 0.85 | 0.44 (17.75) | 0.32 |
| Mortality | −11.09 (25.49) | −10.46 (14.85) | |||
| Visceral fat area (cm2/m2), mean (SD) | Survival | −0.03 (21.23) | 0.56 | 0.74 (21.47) | 0.44 |
| Mortality | −10.97 (32.19) | −3.75 (20.96) | |||
| Intermuscular fat area (cm2/m2), mean (SD) | Survival | 1.06 (2.36) | 0.74 | 1.13 (2.37) | 0.76 |
| Mortality | 0.76 (2.91) | 1.04 (2.43) | |||
| Total fat area (cm2/m2), mean (SD) | Survival | 0.56 (35.39) | 0.68 | 2.32 (36.5) | 0.37 |
| Mortality | −21.30 (54.02) | −13.17 (30.40) | |||
| VLD muscle area (cm2/m2), mean (SD) | Survival | 0.16 (1.51) | 0.24 | 0.18 (1.50) | 0.10 |
| Mortality | 1.13 (2.41) | 1.63 (2.33) | |||
| LD muscle area (cm2/m2), mean (SD) | Survival | −0.92 (3.60) | 0.02 | −0.83 (3.59) | 0.03 |
| Mortality | 1.22 (3.54) | 1.89 (2.75) | |||
| ND muscle area (cm2/m2), mean (SD) | Survival | −1.61 (5.85) | 0.01 | −1.72 (5.81) | 0.05 |
| Mortality | −4.96 (5.07) | −5.25 (5.11) | |||
| Total muscle area (cm2/m2), mean (SD) | Survival | −2.43 (3.82) | 0.33 | −2.43 (3.77) | 0.72 |
| Mortality | −2.60 (5.72) | −3.15 (6.48) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sebastian-Valles, F.; Sánchez de la Blanca Carrero, N.; Rodríguez-Laval, V.; Martinez-Hernández, R.; Serrano-Somavilla, A.; Knott-Torcal, C.; Muñoz de Nova, J.L.; Martín-Pérez, E.; Marazuela, M.; Sampedro-Nuñez, M.A. Impact of Change in Body Composition during Follow-Up on the Survival of GEP-NET. Cancers 2022, 14, 5189. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14215189
Sebastian-Valles F, Sánchez de la Blanca Carrero N, Rodríguez-Laval V, Martinez-Hernández R, Serrano-Somavilla A, Knott-Torcal C, Muñoz de Nova JL, Martín-Pérez E, Marazuela M, Sampedro-Nuñez MA. Impact of Change in Body Composition during Follow-Up on the Survival of GEP-NET. Cancers. 2022; 14(21):5189. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14215189
Chicago/Turabian StyleSebastian-Valles, Fernando, Nuria Sánchez de la Blanca Carrero, Víctor Rodríguez-Laval, Rebeca Martinez-Hernández, Ana Serrano-Somavilla, Carolina Knott-Torcal, José Luis Muñoz de Nova, Elena Martín-Pérez, Mónica Marazuela, and Miguel Antonio Sampedro-Nuñez. 2022. "Impact of Change in Body Composition during Follow-Up on the Survival of GEP-NET" Cancers 14, no. 21: 5189. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14215189