
A Soft Label Deep Learning to Assist Breast Cancer Target Therapy and Thyroid Cancer Diagnosis
 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Related Works in Soft Label, Label Smoothing, and Segmentation Approaches
2.1. Soft Label Techniques
2.2. Label Smoothing Methods
2.3. Segmentation Approaches
3. Materials and Methods
3.1. Materials
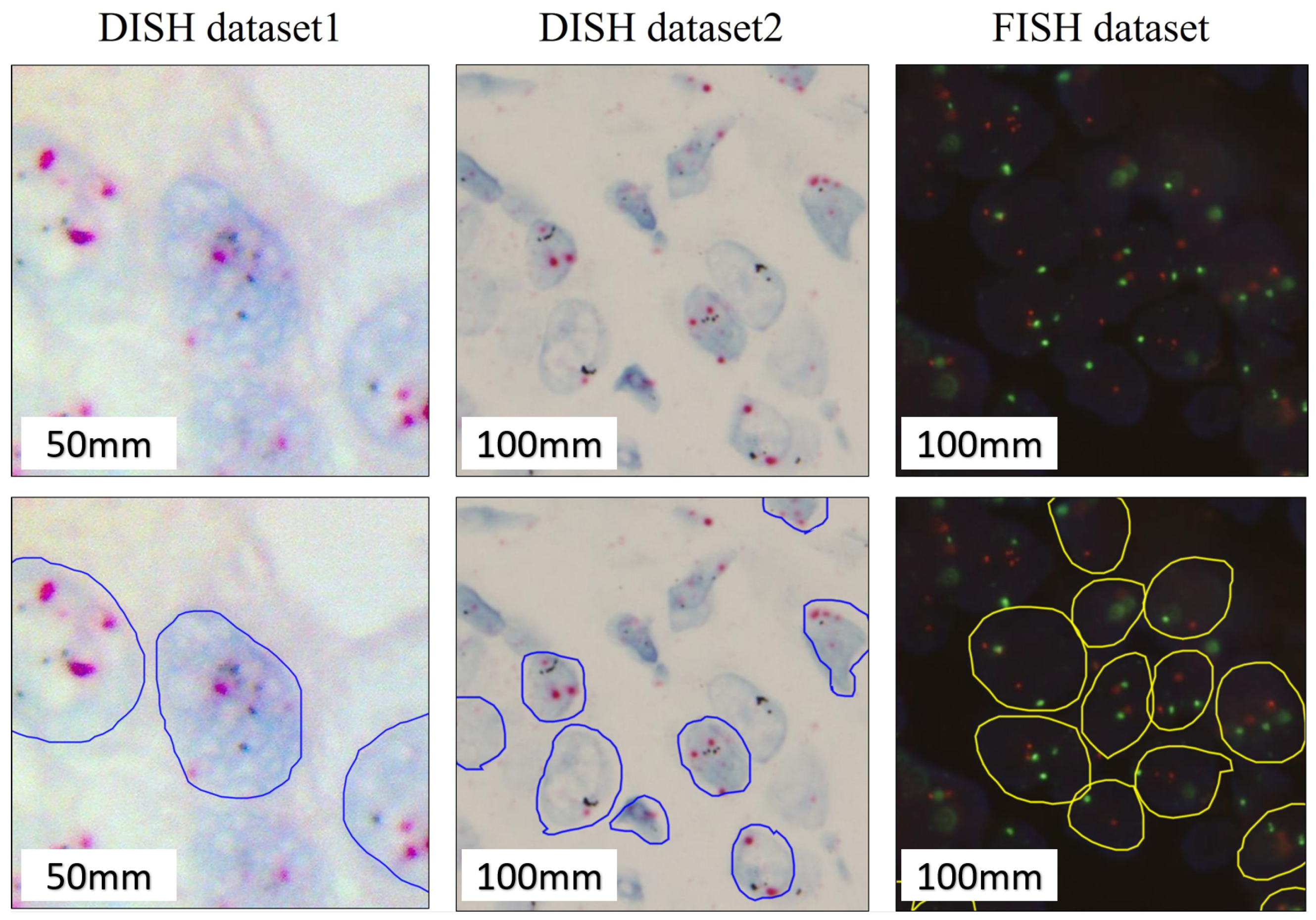
3.1.1. Fish Breast Dataset
3.1.2. Dish Breast Datasets
3.1.3. FNA and TP Thyroid Dataset
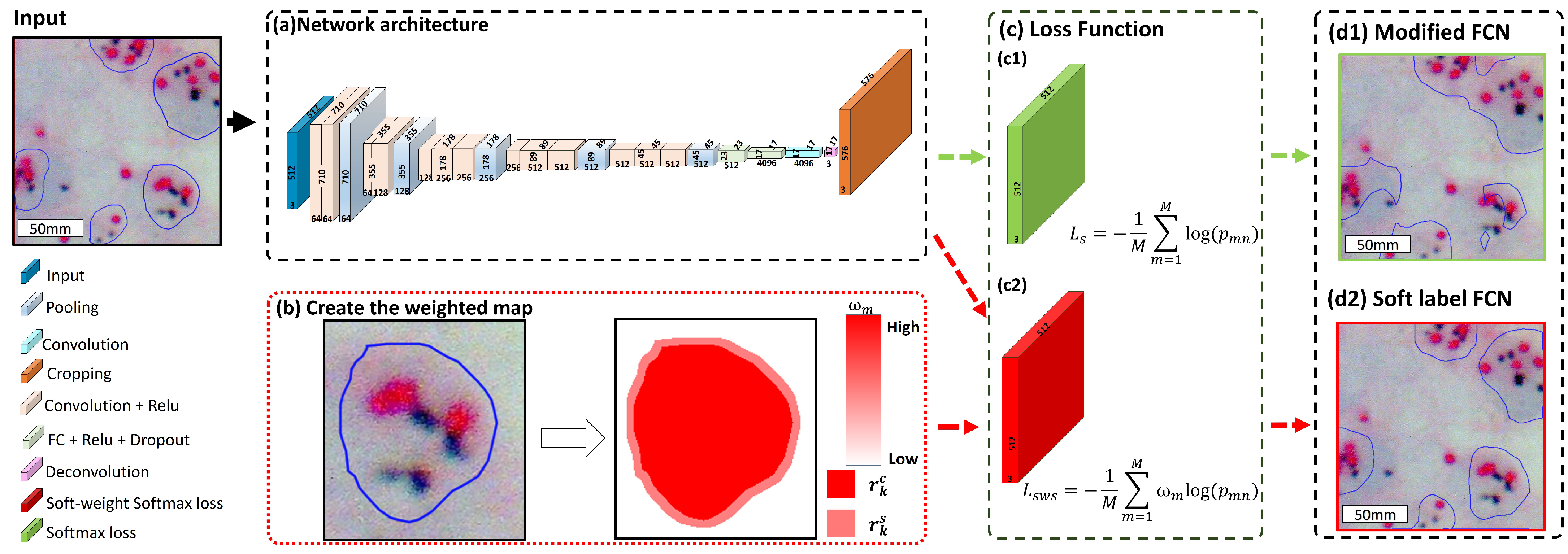
3.2. Proposed Method: Soft Label FCN
3.2.1. Soft Label Modeling
3.2.2. Soft Weight Softmax Loss Function
3.2.3. Proposed Soft-Labeled FCN Architecture
3.2.4. Implementation Details
4. Results
4.1. Evaluation Metrics
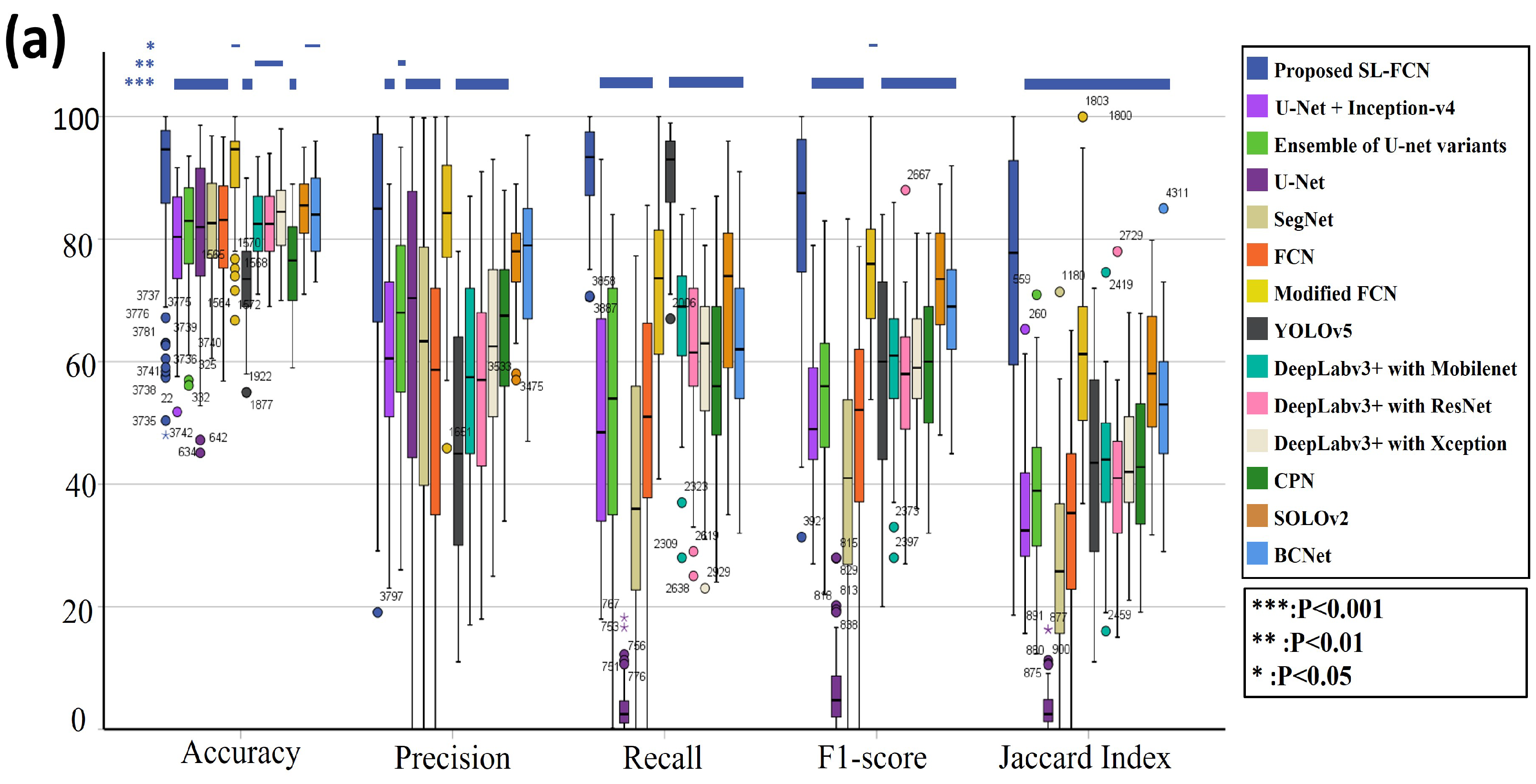
4.2. Quantitative Evaluation with Statistical Analysis in DISH Breast Dataset 1
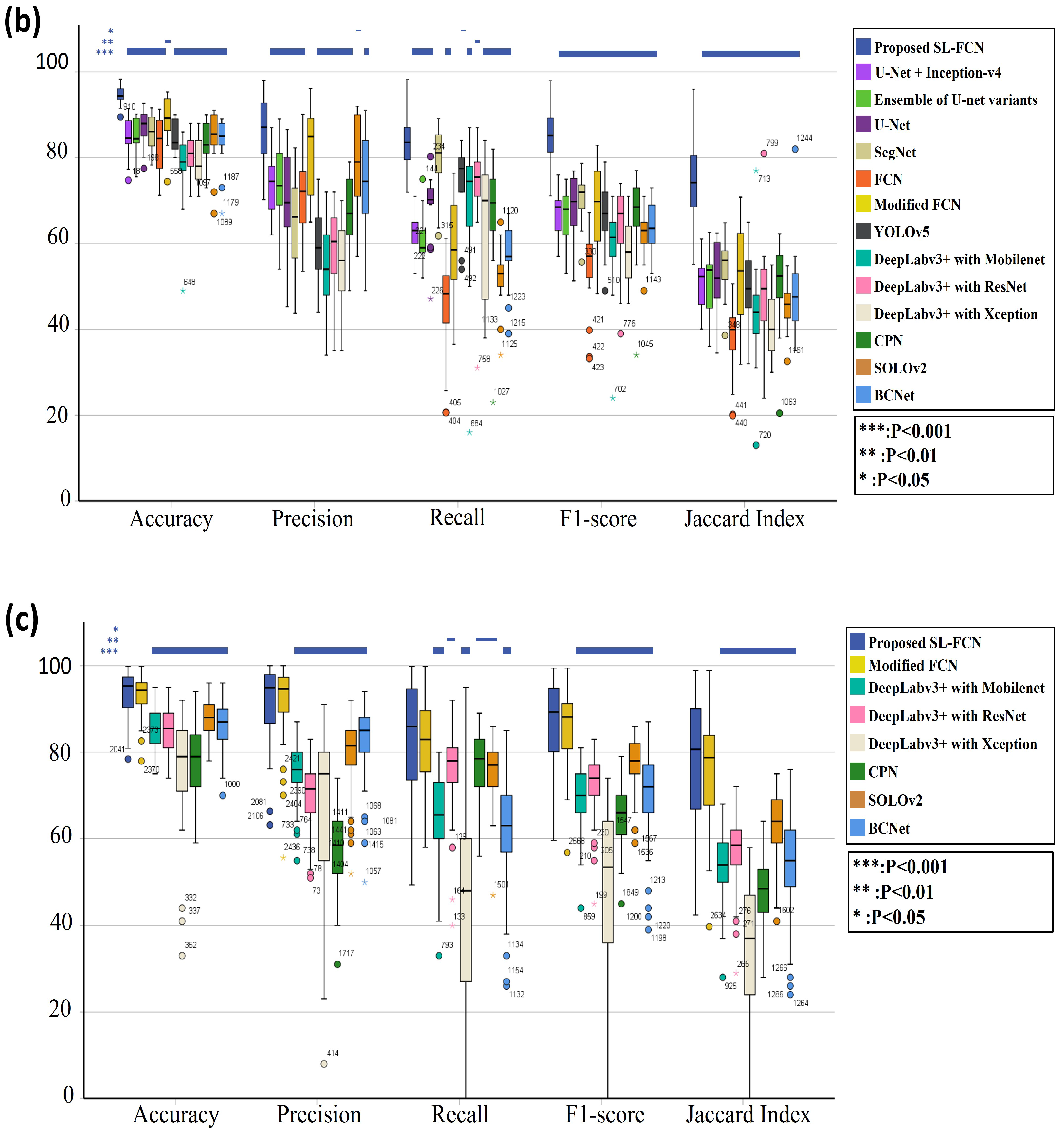
4.3. Quantitative Evaluation with Statistical Analysis in DISH Breast Dataset 2
4.4. Quantitative Evaluation with Statistical Analysis in the FISH Breast Dataset
4.5. Quantitative Evaluation with Statistical Analysis in the Thyroid Dataset
4.6. Ablation Study
5. Discussion and Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. Adv. Neural Inf. Process. Syst. 2012, 25, 84–90. [Google Scholar] [CrossRef] [Green Version]
- Falk, T.; Mai, D.; Bensch, R.; Çiçek, Ö.; Abdulkadir, A.; Marrakchi, Y.; Böhm, A.; Deubner, J.; Jäckel, Z.; Seiwald, K.; et al. U-Net: Deep learning for cell counting, detection, and morphometry. Nat. Methods 2019, 16, 67–70. [Google Scholar] [CrossRef]
- Wang, C.W.; Huang, S.C.; Lee, Y.C.; Shen, Y.J.; Meng, S.I.; Gaol, J.L. Deep learning for bone marrow cell detection and classification on whole-slide images. Med. Image Anal. 2022, 75, 102270. [Google Scholar] [CrossRef]
- Redmon, J.; Farhadi, A. YOLO9000: Better, faster, stronger. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 7263–7271. [Google Scholar]
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; Van Der Laak, J.A.; Van Ginneken, B.; Sánchez, C.I. A survey on deep learning in medical image analysis. Med. Image Anal. 2017, 42, 60–88. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.J.; Chao, T.K.; Khalil, M.A.; Lee, Y.C.; Hong, D.Z.; Wu, J.J.; Wang, C.W. Deep Learning Fast Screening Approach on Cytological Whole Slides for Thyroid Cancer Diagnosis. Cancers 2021, 13, 3891. [Google Scholar] [CrossRef]
- Wang, C.W.; Liou, Y.A.; Lin, Y.J.; Chang, C.C.; Chu, P.H.; Lee, Y.C.; Wang, C.H.; Chao, T.K. Artificial intelligence-assisted fast screening cervical high grade squamous intraepithelial lesion and squamous cell carcinoma diagnosis and treatment planning. Sci. Rep. 2021, 11, 16244. [Google Scholar] [CrossRef]
- Khalil, M.A.; Lee, Y.C.; Lien, H.C.; Jeng, Y.M.; Wang, C.W. Fast Segmentation of Metastatic Foci in H&E Whole-Slide Images for Breast Cancer Diagnosis. Diagnostics 2022, 12, 990. [Google Scholar]
- Wang, C.W.; Khalil, M.A.; Lin, Y.J.; Lee, Y.C.; Huang, T.W.; Chao, T.K. Deep Learning Using Endobronchial-Ultrasound-Guided Transbronchial Needle Aspiration Image to Improve the Overall Diagnostic Yield of Sampling Mediastinal Lymphadenopathy. Diagnostics 2022, 12, 2234. [Google Scholar] [CrossRef]
- Wang, C.W.; Lee, Y.C.; Chang, C.C.; Lin, Y.J.; Liou, Y.A.; Hsu, P.C.; Chang, C.C.; Sai, A.K.O.; Wang, C.H.; Chao, T.K. A Weakly Supervised Deep Learning Method for Guiding Ovarian Cancer Treatment and Identifying an Effective Biomarker. Cancers 2022, 14, 1651. [Google Scholar] [CrossRef]
- Wang, C.W.; Chang, C.C.; Lee, Y.C.; Lin, Y.J.; Lo, S.C.; Hsu, P.C.; Liou, Y.A.; Wang, C.H.; Chao, T.K. Weakly supervised deep learning for prediction of treatment effectiveness on ovarian cancer from histopathology images. Comput. Med. Imaging Graph. 2022, 99, 102093. [Google Scholar] [CrossRef]
- Araújo, T.; Aresta, G.; Castro, E.; Rouco, J.; Aguiar, P.; Eloy, C.; Polónia, A.; Campilho, A. Classification of breast cancer histology images using convolutional neural networks. PLoS ONE 2017, 12, e0177544. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Gown, A.M.; Goldstein, L.C.; Barry, T.S.; Kussick, S.J.; Kandalaft, P.L.; Kim, P.M.; Tse, C.C. High concordance between immunohistochemistry and fluorescence in situ hybridization testing for HER2 status in breast cancer requires a normalized IHC scoring system. Mod. Pathol. 2008, 21, 1271–1277. [Google Scholar] [CrossRef] [Green Version]
- Jelovac, D.; Emens, L.A. HER2-directed therapy for metastatic breast cancer. Oncol. Williston Park 2013, 27, 166–175. [Google Scholar]
- Vogel, C.L.; Cobleigh, M.A.; Tripathy, D.; Gutheil, J.C.; Harris, L.N.; Fehrenbacher, L.; Slamon, D.J.; Murphy, M.; Novotny, W.F.; Burchmore, M.; et al. Efficacy and safety of trastuzumab as a single agent in first-line treatment of HER2-overexpressing metastatic breast cancer. J. Clin. Oncol. 2002, 20, 719–726. [Google Scholar] [CrossRef]
- Piccart-Gebhart, M.J.; Procter, M.; Leyland-Jones, B.; Goldhirsch, A.; Untch, M.; Smith, I.; Gianni, L.; Baselga, J.; Bell, R.; Jackisch, C.; et al. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N. Engl. J. Med. 2005, 353, 1659–1672. [Google Scholar] [CrossRef] [Green Version]
- Kaufman, B.; Trudeau, M.; Awada, A.; Blackwell, K.; Bachelot, T.; Salazar, V.; DeSilvio, M.; Westlund, R.; Zaks, T.; Spector, N.; et al. Lapatinib monotherapy in patients with HER2-overexpressing relapsed or refractory inflammatory breast cancer: Final results and survival of the expanded HER2+ cohort in EGF103009, a phase II study. Lancet Oncol. 2009, 10, 581–588. [Google Scholar] [CrossRef]
- Emde, A.; Köstler, W.J.; Yarden, Y.; Association of Radiotherapy and Oncology of the Mediterranean arEa (AROME). Therapeutic strategies and mechanisms of tumorigenesis of HER2-overexpressing breast cancer. Crit. Rev. Oncol. Hematol. 2012, 84 (Suppl. 1), e49–e57. [Google Scholar] [CrossRef] [Green Version]
- Hilal, T.; Romond, E.H. ERBB2 (HER2) testing in breast cancer. JAMA 2016, 315, 1280–1281. [Google Scholar] [CrossRef]
- Kunte, S.; Abraham, J.; Montero, A.J. Novel HER2–targeted therapies for HER2–positive metastatic breast cancer. Cancer 2020, 126, 4278–4288. [Google Scholar] [CrossRef]
- Press, M.F.; Seoane, J.A.; Curtis, C.; Quinaux, E.; Guzman, R.; Sauter, G.; Eiermann, W.; Mackey, J.R.; Robert, N.; Pienkowski, T.; et al. Assessment of ERBB2/HER2 status in HER2-equivocal breast cancers by FISH and 2013/2014 ASCO-CAP guidelines. JAMA Oncol. 2019, 5, 366–375. [Google Scholar] [CrossRef] [Green Version]
- Agersborg, S.; Mixon, C.; Nguyen, T.; Aithal, S.; Sudarsanam, S.; Blocker, F.; Weiss, L.; Gasparini, R.; Jiang, S.; Chen, W.; et al. Immunohistochemistry and alternative FISH testing in breast cancer with HER2 equivocal amplification. Breast Cancer Res. Treat. 2018, 170, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Edelweiss, M.; Sebastiao, A.P.M.; Oen, H.; Kracun, M.; Serrette, R.; Ross, D.S. HER2 assessment by bright-field dual in situ hybridization in cell blocks of recurrent and metastatic breast carcinoma. Cancer Cytopathol. 2019, 127, 684–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Troxell, M.; Sibley, R.K.; West, R.B.; Bean, G.R.; Allison, K.H. HER2 dual in situ hybridization: Correlations and cautions. Arch. Pathol. Lab. Med. 2020, 144, 1525–1534. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.H.; Wang, K.; Lin, D.Y.; Xu, J.; Chen, J.; Long, X.Y.; Ge, Y.; Luo, X.L.; Zhang, K.P.; Liu, Y.H.; et al. Impact of the updated 2018 ASCO/CAP guidelines on HER2 FISH testing in invasive breast cancer: A retrospective study of HER2 fish results of 2233 cases. Breast Cancer Res. Treat. 2019, 175, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Slamon, D.J.; Leyland-Jones, B.; Shak, S.; Fuchs, H.; Paton, V.; Bajamonde, A.; Fleming, T.; Eiermann, W.; Wolter, J.; Pegram, M.; et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N. Engl. J. Med. 2001, 344, 783–792. [Google Scholar] [CrossRef]
- Burstein, H.J.; Harris, L.N.; Marcom, P.K.; Lambert-Falls, R.; Havlin, K.; Overmoyer, B.; Friedlander Jr, R.J.; Gargiulo, J.; Strenger, R.; Vogel, C.L.; et al. Trastuzumab and vinorelbine as first-line therapy for HER2-overexpressing metastatic breast cancer: Multicenter phase II trial with clinical outcomes, analysis of serum tumor markers as predictive factors, and cardiac surveillance algorithm. J. Clin. Oncol. 2003, 21, 2889–2895. [Google Scholar] [CrossRef]
- Yu, K.H.; Beam, A.L.; Kohane, I.S. Artificial intelligence in healthcare. Nat. Biomed. Eng. 2018, 2, 719–731. [Google Scholar] [CrossRef]
- Zakrzewski, F.; de Back, W.; Weigert, M.; Wenke, T.; Zeugner, S.; Mantey, R.; Sperling, C.; Friedrich, K.; Roeder, I.; Aust, D.; et al. Automated detection of the HER2 gene amplification status in Fluorescence in situ hybridization images for the diagnostics of cancer tissues. Sci. Rep. 2019, 9, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Bera, K.; Schalper, K.A.; Rimm, D.L.; Velcheti, V.; Madabhushi, A. Artificial intelligence in digital pathology—New tools for diagnosis and precision oncology. Nat. Rev. Clin. Oncol. 2019, 16, 703–715. [Google Scholar] [CrossRef]
- Szegedy, C.; Ioffe, S.; Vanhoucke, V.; Alemi, A.A. Inception-v4, inception-resnet and the impact of residual connections on learning. In Proceedings of the Thirty-First AAAI Conference on Artificial Intelligence, San Francisco, CA, USA, 4–9 February 2017. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 26 June–1 July 2016; pp. 770–778. [Google Scholar]
- Badrinarayanan, V.; Kendall, A.; Cipolla, R. Segnet: A deep convolutional encoder-decoder architecture for image segmentation. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 39, 2481–2495. [Google Scholar] [CrossRef] [PubMed]
- Jubayer, F.; Soeb, J.A.; Mojumder, A.N.; Paul, M.K.; Barua, P.; Kayshar, S.; Akter, S.S.; Rahman, M.; Islam, A. Detection of mold on the food surface using YOLOv5. Curr. Res. Food Sci. 2021, 4, 724–728. [Google Scholar] [CrossRef]
- Shelhamer, E.; Long, J.; Darrell, T. Fully convolutional networks for semantic segmentation. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 39, 640–651. [Google Scholar] [CrossRef] [PubMed]
- Upschulte, E.; Harmeling, S.; Amunts, K.; Dickscheid, T. Contour Proposal Networks for Biomedical Instance Segmentation. Med. Image Anal. 2022, 77, 102371. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Zhang, R.; Kong, T.; Li, L.; Shen, C. Solov2: Dynamic and fast instance segmentation. Adv. Neural Inf. Process. Syst. 2020, 33, 17721–17732. [Google Scholar]
- Ke, L.; Tai, Y.W.; Tang, C.K. Deep Occlusion-Aware Instance Segmentation with Overlapping BiLayers. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR), Nashville, TN, USA, 20–25 June 2021; pp. 4019–4028. [Google Scholar]
- Chen, L.C.; Zhu, Y.; Papandreou, G.; Schroff, F.; Adam, H. Encoder-decoder with atrous separable convolution for semantic image segmentation. In Proceedings of the European conference on Computer Vision (ECCV), Munich, Germany, 8–14 September 2018; pp. 801–818. [Google Scholar]
- Howard, A.G.; Zhu, M.; Chen, B.; Kalenichenko, D.; Wang, W.; Weyand, T.; Andreetto, M.; Adam, H. Mobilenets: Efficient convolutional neural networks for mobile vision applications. arXiv 2017, arXiv:1704.04861. [Google Scholar]
- Chollet, F. Xception: Deep learning with depthwise separable convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 1251–1258. [Google Scholar]
- Wang, L.; Zhang, L.; Zhu, M.; Qi, X.; Yi, Z. Automatic diagnosis for thyroid nodules in ultrasound images by deep neural networks. Med. Image Anal. 2020, 61, 101665. [Google Scholar] [CrossRef]
- Dov, D.; Kovalsky, S.Z.; Assaad, S.; Cohen, J.; Range, D.E.; Pendse, A.A.; Henao, R.; Carin, L. Weakly supervised instance learning for thyroid malignancy prediction from whole slide cytopathology images. Med. Image Anal. 2021, 67, 101814. [Google Scholar] [CrossRef]
- Gros, C.; Lemay, A.; Cohen-Adad, J. SoftSeg: Advantages of soft versus binary training for image segmentation. Med. Image Anal. 2021, 71, 102038. [Google Scholar] [CrossRef]
- Müller, R.; Kornblith, S.; Hinton, G. When Does Label Smoothing Help? In Proceedings of the 33rd International Conference on Neural Information Processing Systems, Vancouver, BC, Canada, 8–14 December 2019; Curran Associates Inc.: Red Hook, NY, USA, 2019. [Google Scholar]
- Kats, E.; Goldberger, J.; Greenspan, H. A soft STAPLE algorithm combined with anatomical knowledge. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Shenzhen, China, 13–17 October 2019; Springer: Berlin/Heidelberg, Germany, 2019; pp. 510–517. [Google Scholar]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. In Proceedings of the Medical Image Computing and Computer-Assisted Intervention—MICCAI 2015, Munich, Germany, 5–9 October 2015; Navab, N., Hornegger, J., Wells, W.M., Frangi, A.F., Eds.; Springer International Publishing: Cham, Switzerland, 2015; pp. 234–241. [Google Scholar]
- Zhang, C.B.; Jiang, P.T.; Hou, Q.; Wei, Y.; Han, Q.; Li, Z.; Cheng, M.M. Delving deep into label smoothing. IEEE Trans. Image Process. 2021, 30, 5984–5996. [Google Scholar] [CrossRef]
- Van Engelen, A.; Niessen, W.; Klein, S.; Verhagen, H.; Groen, H.; Wentzel, J.; Lugt, A.; de Bruijne, M. Supervised in-vivo plaque characterization incorporating class label uncertainty. In Proceedings of the 2012 9th IEEE International Symposium on Biomedical Imaging (ISBI), Barcelona, Spain, 2–5 May 2012. [Google Scholar] [CrossRef]
- de Weert, T.T.; Ouhlous, M.; Meijering, E.; Zondervan, P.E.; Hendriks, J.M.; van Sambeek, M.R.; Dippel, D.W.; van der Lugt, A. In vivo characterization and quantification of atherosclerotic carotid plaque components with multidetector computed tomography and histopathological correlation. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 2366–2372. [Google Scholar] [CrossRef] [PubMed]
- Qi, L.; Wang, L.; Huo, J.; Shi, Y.; Gao, Y. Progressive Cross-Camera Soft-Label Learning for Semi-Supervised Person Re-Identification. IEEE Trans. Circuits Syst. Video Technol. 2020, 30, 2815–2829. [Google Scholar] [CrossRef] [Green Version]
- Warfield, S.; Zou, K.; Wells, W. Simultaneous truth and performance level estimation (STAPLE): An algorithm for the validation of image segmentation. IEEE Trans. Med. Imaging 2004, 23, 903–921. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Wei, D.; Cao, S.; Ma, K.; Wang, L.; Zheng, Y. Superpixel-Guided Label Softening for Medical Image Segmentation; Springer: Cham, Switzerland, 2020. [Google Scholar]
- Pham, H.H.; Le, T.T.; Tran, D.Q.; Ngo, D.T.; Nguyen, H.Q. Interpreting chest X-rays via CNNs that exploit hierarchical disease dependencies and uncertainty labels. Neurocomputing 2021, 437, 186–194. [Google Scholar] [CrossRef]
- Zhao, H.H.; Rosin, P.L.; Lai, Y.K.; Wang, Y.N. Automatic semantic style transfer using deep convolutional neural networks and soft masks. Vis. Comput. 2020, 36, 1307–1324. [Google Scholar] [CrossRef] [Green Version]
- Chorowski, J.; Jaitly, N. Towards better decoding and language model integration in sequence to sequence models. arXiv 2016, arXiv:1612.02695. [Google Scholar]
- Vaswani, A.; Shazeer, N.; Parmar, N.; Uszkoreit, J.; Jones, L.; Gomez, A.N.; Kaiser, Ł.; Polosukhin, I. Attention is all you need. Adv. Neural Inf. Process. Syst. 2017, 30, 6000–6010. [Google Scholar]
- Kuijf, H.J.; Bennink, E. Grand Challenge on MR Brain Segmentation at MICCAI 2018. Available online: https://mrbrains18.isi.uu.nl (accessed on 1 August 2022).
- Krizhevsky, A.; Nair, V.; Hinton, G. CIFAR-100 (Canadian Institute for Advanced Research). Available online: https://cs.toronto.edu/~kriz/cifar.html (accessed on 1 August 2022).
- Shen, J.; Li, T.; Hu, C.; He, H.; Jiang, D.; Liu, J. An Augmented Cell Segmentation in Fluorescent in Situ Hybridization Images. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 6306–6309. [Google Scholar]
- Shen, J.; Li, T.; Hu, C.; He, H.; Liu, J. Automatic cell segmentation using mini-u-net on fluorescence in situ hybridization images. In Proceedings of the Medical Imaging 2019: Computer-Aided Diagnosis, SPIE, San Diego, CA, USA, 13 March 2019; Volume 10950, pp. 721–727. [Google Scholar]
- Ljosa, V.; Sokolnicki, K.L.; Carpenter, A.E. Annotated high-throughput microscopy image sets for validation. Nat. Methods 2012, 9, 637. [Google Scholar] [CrossRef] [Green Version]
- Lin, T.Y.; Maire, M.; Belongie, S.; Hays, J.; Perona, P.; Ramanan, D.; Dollár, P.; Zitnick, C.L. Microsoft coco: Common objects in context. In Proceedings of the European Conference on Computer Vision, Zurich, Switzerland, 6–12 September 2014; Springer: Berlin/Heidelberg, Germany, 2014; pp. 740–755. [Google Scholar]
- Cordts, M.; Omran, M.; Ramos, S.; Rehfeld, T.; Enzweiler, M.; Benenson, R.; Franke, U.; Roth, S.; Schiele, B. The cityscapes dataset for semantic urban scene understanding. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 3213–3223. [Google Scholar]
- Wolff, A.C.; Hammond, M.E.H.; Schwartz, J.N.; Hagerty, K.L.; Allred, D.C.; Cote, R.J.; Dowsett, M.; Fitzgibbons, P.L.; Hanna, W.M.; Langer, A.; et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. Arch. Pathol. Lab. Med. 2007, 131, 18–43. [Google Scholar] [CrossRef]
- Slamon, D.J.; Clark, G.M.; Wong, S.G.; Levin, W.J.; Ullrich, A.; McGuire, W.L. Human breast cancer: Correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science 1987, 235, 177–182. [Google Scholar] [CrossRef] [Green Version]
- Meric-Bernstam, F.; Johnson, A.M.; Dumbrava, E.E.I.; Raghav, K.; Balaji, K.; Bhatt, M.; Murthy, R.K.; Rodon, J.; Piha-Paul, S.A. Advances in HER2-targeted therapy: Novel agents and opportunities beyond breast and gastric cancer. Clin. Cancer Res. 2019, 25, 2033–2041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dagrada, G.P.; Mezzelani, A.; Alasio, L.; Ruggeri, M.; Romanò, R.; Pierotti, M.A.; Pilotti, S. HER-2/neu assessment in primary chemotherapy treated breast carcinoma: No evidence of gene profile changing. Breast Cancer Res. Treat. 2003, 80, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Lear-Kaul, K.C.; Yoon, H.R.; Kleinschmidt-DeMasters, B.K.; McGavran, L.; Singh, M. Her-2/neu status in breast cancer metastases to the central nervous system. Arch. Pathol. Lab. Med. 2003, 127, 1451–1457. [Google Scholar] [CrossRef] [PubMed]
- Durbecq, V.; Di Leo, A.; Cardoso, F.; Rouas, G.; Leroy, J.Y.; Piccart, M.; Larsimont, D. Comparison of topoisomerase-IIalpha gene status between primary breast cancer and corresponding distant metastatic sites. Breast Cancer Res. Treat. 2003, 77, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Bowles, E.J.A.; Wellman, R.; Feigelson, H.S.; Onitilo, A.A.; Freedman, A.N.; Delate, T.; Allen, L.A.; Nekhlyudov, L.; Goddard, K.A.; Davis, R.L.; et al. Risk of heart failure in breast cancer patients after anthracycline and trastuzumab treatment: A retrospective cohort study. J. Natl. Cancer Inst. 2012, 104, 1293–1305. [Google Scholar] [CrossRef]
- Mohan, N.; Jiang, J.; Dokmanovic, M.; Wu, W.J. Trastuzumab-mediated cardiotoxicity: Current understanding, challenges, and frontiers. Antib. Ther. 2018, 1, 13–17. [Google Scholar] [CrossRef]
- Zhu, X.; Verma, S. Targeted therapy in her2-positive metastatic breast cancer: A review of the literature. Curr. Oncol. 2015, 22, 19–28. [Google Scholar] [CrossRef] [Green Version]
- Dowsett, M.; Bartlett, J.; Ellis, I.; Salter, J.; Hills, M.; Mallon, E.; Watters, A.; Cooke, T.; Paish, C.; Wencyk, P.; et al. Correlation between immunohistochemistry (HercepTest) and fluorescence in situ hybridization (FISH) for HER-2 in 426 breast carcinomas from 37 centres. J. Pathol. J. Pathol. Soc. Great Br. Irel. 2003, 199, 418–423. [Google Scholar]
- Borley, A.; Mercer, T.; Morgan, M.; Dutton, P.; Barrett-Lee, P.; Brunelli, M.; Jasani, B. Impact of HER2 copy number in IHC2+/FISH-amplified breast cancer on outcome of adjuvant trastuzumab treatment in a large UK cancer network. Br. J. Cancer 2014, 110, 2139–2143. [Google Scholar] [CrossRef] [Green Version]
- Nishimura, R.; Okamoto, N.; Satou, M.; Kojima, K.; Tanaka, S.; Yamashita, N. Bright-field HER2 dual in situ hybridization (DISH) assay on breast cancer cell blocks: A comparative study with histological sections. Breast Cancer 2016, 23, 917–921. [Google Scholar] [CrossRef] [Green Version]
- Hartman, A.K.; Gorman, B.K.; Chakraborty, S.; Mody, D.R.; Schwartz, M.R. Determination of HER2/neu status: A pilot study comparing HER2/neu dual in situ hybridization DNA probe cocktail assay performed on cell blocks to immunohistochemisty and fluorescence in situ hybridization performed on histologic specimens. Arch. Pathol. Lab. Med. 2014, 138, 553–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bejnordi, B.E.; Veta, M.; Van Diest, P.J.; Van Ginneken, B.; Karssemeijer, N.; Litjens, G.; Van Der Laak, J.A.; Hermsen, M.; Manson, Q.F.; Balkenhol, M.; et al. Diagnostic assessment of deep learning algorithms for detection of lymph node metastases in women with breast cancer. JAMA 2017, 318, 2199–2210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, C.; Xu, H.; Xu, J.; Gilmore, H.; Mandal, M.; Madabhushi, A. Multi-Pass Adaptive Voting for nuclei detection in histopathological images. Sci. Rep. 2016, 6, 33985. [Google Scholar] [CrossRef] [PubMed]
- Sornapudi, S.; Stanley, R.J.; Stoecker, W.V.; Almubarak, H.; Long, R.; Antani, S.; Thoma, G.; Zuna, R.; Frazier, S.R. Deep learning nuclei detection in digitized histology images by superpixels. J. Pathol. Inform. 2018, 9, 5. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Cruz-Roa, A.; Basavanhally, A.; Gilmore, H.; Shih, N.; Feldman, M.; Tomaszewski, J.; Gonzalez, F.; Madabhushi, A. Mitosis detection in breast cancer pathology images by combining handcrafted and convolutional neural network features. J. Med. Imaging Bellingham 2014, 1, 034003. [Google Scholar] [CrossRef]
- Pardo, E.; Morgado, J.M.T.; Malpica, N. Semantic segmentation of mFISH images using convolutional networks. Cytom. Part A 2018, 93, 620–627. [Google Scholar] [CrossRef]
- Höfener, H.; Homeyer, A.; Förster, M.; Drieschner, N.; Schildhaus, H.U.; Hahn, H.K. Automated density-based counting of FISH amplification signals for HER2 status assessment. Comput. Methods Programs Biomed. 2019, 173, 77–85. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dataset | Overall Magnification | Size (Pixels) | Slides | |
|---|---|---|---|---|
| DISH breast dataset1 | 1200× | 1600 × 1200 | Total | 210 |
| Training | 148 (70%) | |||
| Testing | 62 (30%) | |||
| DISH breast dataset2 | 600× | 1360 × 1024 | Total | 60 |
| Training | 42 (70%) | |||
| Testing | 18 (30%) | |||
| FISH breast dataset | 600× | 1360 × 1024 | Total | 200 |
| Training | 134 (67%) | |||
| Testing | 66 (33%) | |||
| FNA and TP thyroid dataset | 200× | 77,338 × 37,285 (WSI) | Total | 131 |
| Training | 28 (21%) | |||
| Testing | 103 (79%) | |||
| Layer | Features (Train) | Features (Inference) | Kernel Size | Stride |
|---|---|---|---|---|
| Input | - | - | ||
| 1 | ||||
| 1 | ||||
| Pool1 | 2 | |||
| 1 | ||||
| 1 | ||||
| Pool2 | 1 | |||
| 1 | ||||
| 1 | ||||
| 1 | ||||
| Pool3 | 2 | |||
| 1 | ||||
| 1 | ||||
| 1 | ||||
| Pool4 | 2 | |||
| 1 | ||||
| 1 | ||||
| 1 | ||||
| Pool5 | 2 | |||
| 1 | ||||
| 1 | ||||
| Conv8 | 1 | |||
| Deconv8 | 32 | |||
| Cropping | - | - | ||
| Soft weight loss | - | - | ||
| Output | - | - |
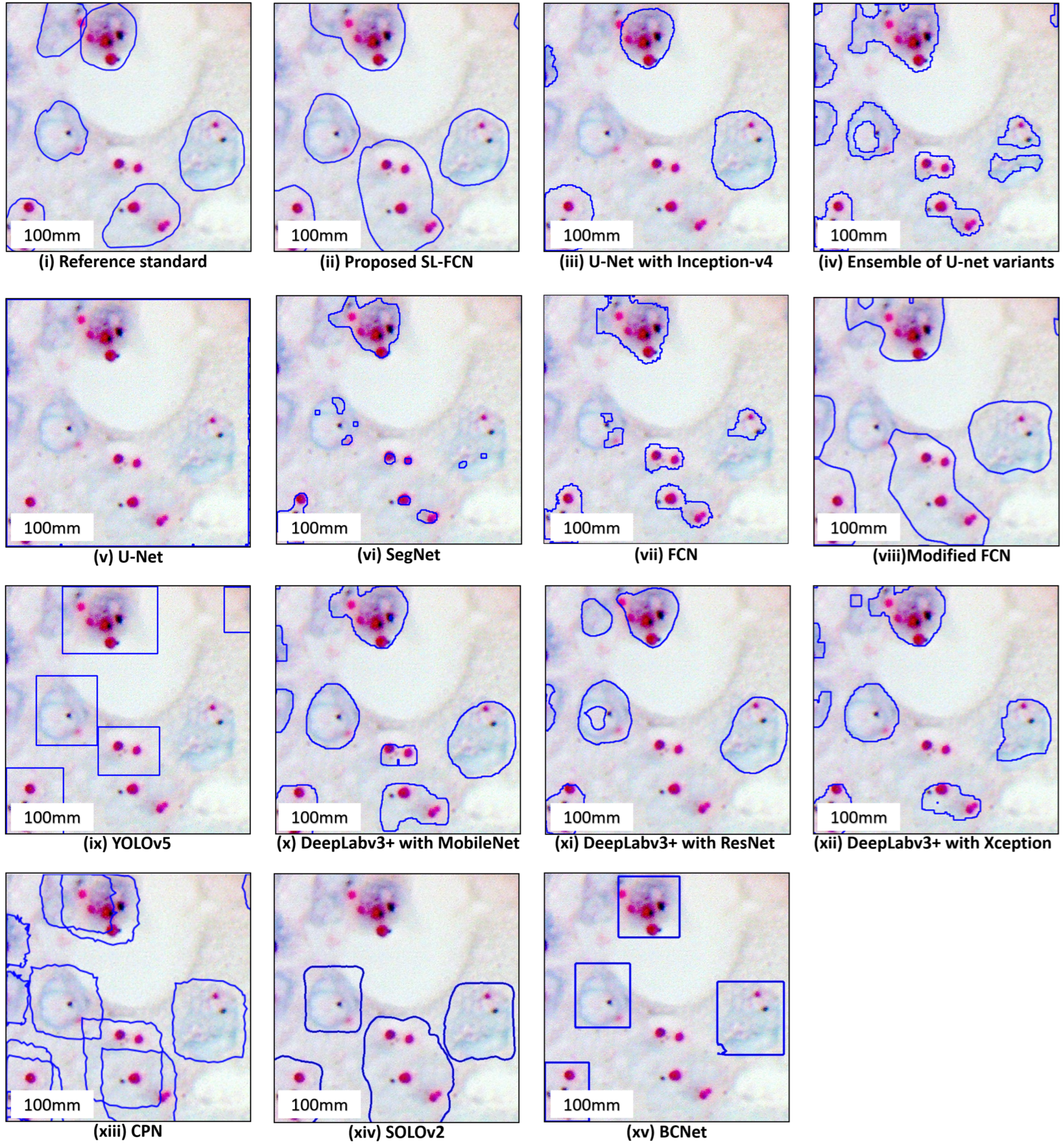
| (a) DISH Dataset 1 | ||||||
| Method | Accuracy | Precision | Recall | F1-Score | Jaccard Index | Rank F1-Score |
| Proposed soft label FCN | 87.77 ± 14.97% | 77.19 ± 23.41% | 91.20 ± 7.72% | 81.67 ± 17.76% | 72.40 ± 23.05% | 1 |
| U-Net [2] +InceptionV4 [32] | 78.74 ± 9.49% | 60.48 ± 15.70% | 50.67 ± 20.86% | 50.88 ± 12.65% | 35.10 ± 11.75% | 11 |
| Ensemble of U-Net variants | 80.71 ± 9.33% | 66.19 ± 17.36% | 52.88 ± 20.33% | 64.40 ± 12.98% | 38.44 ± 12.32% | 5 |
| U-Net [2] | 80.37 ± 13.38% | 63.48 ± 29.03% | 3.76 ± 3.86% | 6.76 ± 6.35% | 3.68 ± 3.59% | 14 |
| SegNet [34] | 81.89 ± 9.07% | 59.06 ± 25.21% | 37.38 ± 20.11% | 40.20 ± 18.27% | 26.78 ± 14.47% | 13 |
| Modified FCN [6,7,8,9,10,11] | 91.26 ± 7.56% | 83.12 ± 11.32% | 71.60 ± 15.38% | 75.79 ± 11.39% | 62.40 ± 15.43% | 2 |
| FCN [36] | 81.92 ± 9.43% | 51.47 ± 24.20% | 50.30 ± 19.18% | 48.75 ± 17.78% | 34.08 ± 15.45% | 12 |
| YOLOv5 [35] | 73.19 ± 7.58% | 46.38 ± 19.33% | 90.38 ± 7.75% | 58.22 ± 16.73% | 43.22 ± 16.29% | 9 |
| DeepLabv3+ [40] with MobileNet [41] | 82.76 ± 5.25% | 56.56 ± 17.83% | 66.74 ± 10.97% | 59.20 ± 11.01% | 42.43 ± 10.67% | 7 |
| DeepLabv3+ [40] with ResNet [33] | 82.45 ± 5.90% | 55.77 ± 16.42% | 62.48 ± 12.84% | 56.45 ± 11.39% | 39.66 ± 11.10% | 10 |
| DeepLabv3+ [40] with Xception [42] | 83.53 ± 5.81% | 61.74 ± 17.96% | 60.72 ± 11.98% | 58.93 ± 10.27% | 42.04 ± 10.26% | 8 |
| CPN [37] | 75.94 ± 7.55% | 65.94 ± 11.11% | 57.13 ± 17.11% | 59.37 ± 12.00% | 43.21 ± 12.06% | 6 |
| SOLOv2 [38] | 84.37 ± 6.34% | 76.82 ± 7.32% | 70.24 ± 15.33% | 72.34 ± 10.01% | 57.56 ± 11.79% | 3 |
| BCNet [39] | 83.71 ± 10.15% | 76.21 ± 12.40% | 62.34 ± 14.30% | 67.44 ± 11.08% | 51.91 ± 12.45% | 4 |
| (b) DISH Dataset 2 | ||||||
| Method | Accuracy | Precision | Recall | F1-Score | Jaccard Index | Rank F1-Score |
| Proposed soft label FCN | 94.64 ± 2.23% | 86.78 ± 8.16% | 83.78 ± 6.42% | 85.14 ± 6.61% | 74.67 ± 10.05% | 1 |
| U-Net [2] +InceptionV4 [32] | 84.92 ± 4.31% | 73.5 ± 8.11% | 65.5 ± 4.54% | 67.33 ± 5.23% | 50.97 ± 5.92% | 5 |
| Ensemble of U-net variants | 84.81 ± 4.38% | 74.38 ± 9.55% | 61.27 ± 5.81% | 66.88 ± 5.84% | 51.69 ± 6.95% | 6 |
| U-Net [2] | 86.89 ± 4.25% | 70.39 ± 10.89% | 69.09 ± 7.45% | 69.12 ± 6.92% | 52.97 ± 7.77% | 3 |
| SegNet [34] | 86.17 ± 3.92% | 65.70 ± 10.84% | 79.00 ± 8.45% | 70.73 ± 5.67% | 54.99 ± 6.59% | 2 |
| FCN [36] | 83.75 ± 5.89% | 72.55 ± 10.05% | 45.70 ± 12.25% | 54.22 ± 9.77% | 37.75 ± 8.71% | 14 |
| Modified FCN [6,7,8,9,10,11] | 89.04 ± 5.26% | 82.12 ± 9.48% | 59.41 ± 11.96% | 68.29 ± 9.98% | 52.68 ± 11.51% | 4 |
| YOLOv5 [35] | 84.66 ± 3.39% | 59.77 ± 9.05% | 75.05 ± 8.24% | 66.38 ± 8.03% | 49.61 ± 8.92% | 7 |
| DeepLabv3+ [40] with MobileNet [41] | 77.33 ± 8.51% | 55.06 ± 9.59% | 69.50 ± 16.74% | 59.78 ± 10.57% | 44.00 ± 12.18% | 12 |
| DeepLabv3+ [40] with ResNet [33] | 80.88 ± 4.56% | 59.00 ± 9.15% | 73.27 ± 11.80% | 64.16 ± 9.19% | 48.55 ± 11.99% | 9 |
| DeepLabv3+ [40] with Xception [42] | 78.72 ± 5.15% | 56.00 ± 9.34% | 63.61 ± 14.76% | 57.88 ± 7.68% | 40.66 ± 7.65% | 13 |
| CPN [37] | 83.61 ± 5.23% | 67.39 ± 8.02% | 67.22 ± 13.21% | 66.33 ± 10.09% | 50.33 ± 10.06% | 8 |
| SOLOv2 [38] | 84.78 ± 6.47% | 79.11 ± 10.24% | 52.44 ± 7.21% | 62.22 ± 5.35% | 45.34 ± 5.45% | 11 |
| BCNet [39] | 83.72 ± 5.74% | 73.61 ± 11.42% | 57.06 ± 7.18% | 63.50 ± 6.40% | 48.50 ± 10.85% | 10 |
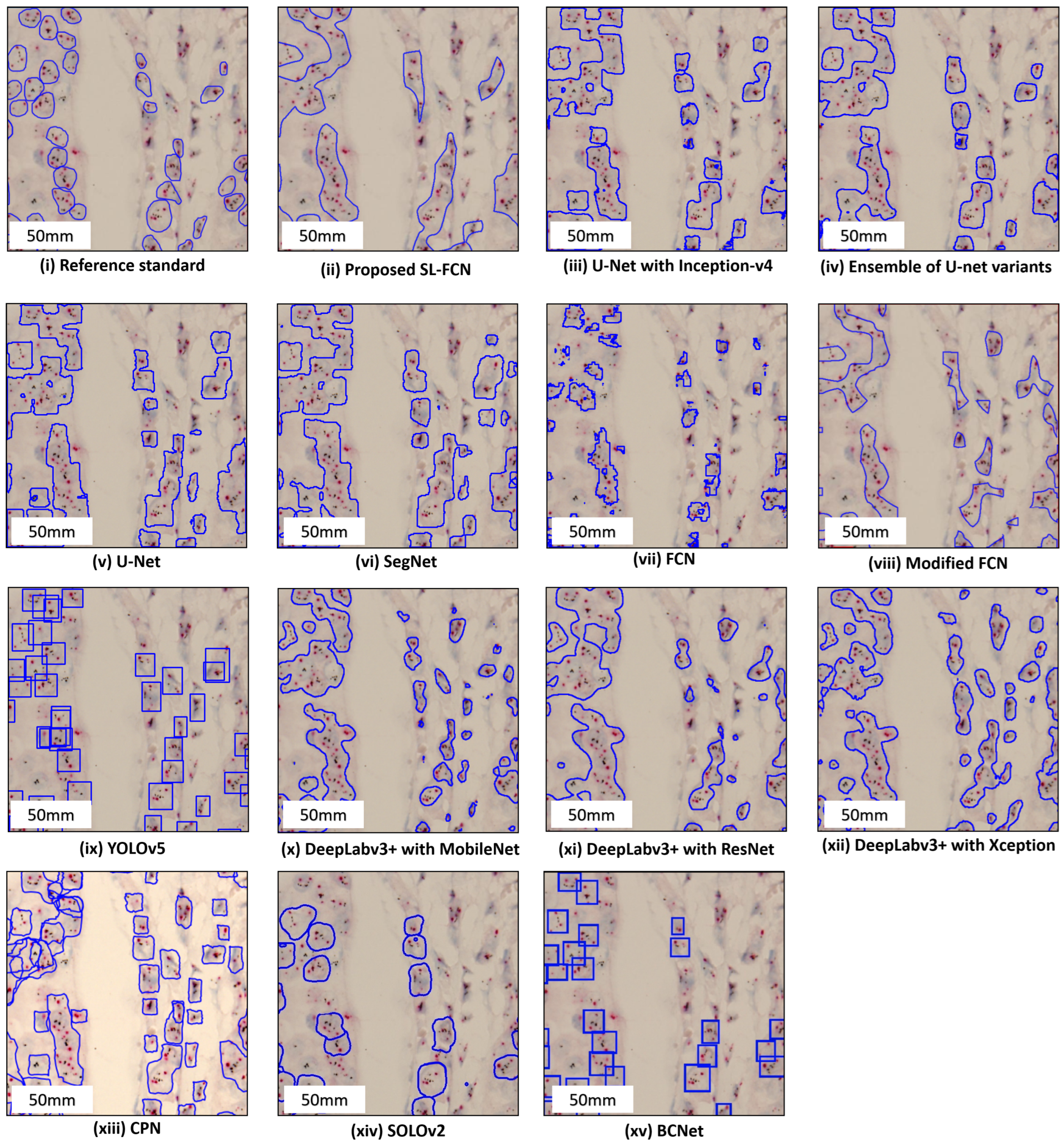
| (c) FISH Dataset | ||||||
| Method | Accuracy | Precision | Recall | F1-Score | Jaccard Index | Rank F1-Score |
| Proposed soft label FCN | 93.54 ± 5.24% | 91.75 ± 8.27% | 83.52 ± 13.15% | 86.98 ± 9.85% | 78.22 ± 14.73% | 1 |
| Modified FCN [6,7,8,9,10,11] | 93.37 ± 4.46% | 91.09 ± 7.87% | 82.13 ± 10.99% | 86.41 ± 8.38% | 76.97 ± 12.50% | 2 |
| DeepLabv3+ [40] with MobileNet [41] | 85.17 ± 5.18% | 75.53 ± 6.14% | 64.94 ± 9.99% | 69.36 ± 7.27% | 53.55 ± 8.08% | 8 |
| DeepLabv3+ [40] with ResNet [33] | 85.06 ± 5.23% | 69.78 ± 7.03% | 76.44 ± 9.28% | 72.52 ± 6.62% | 57.29 ± 7.65% | 6 |
| DeepLabv3+ [40] with Xception [42] | 76.83 ± 11.67% | 66.35 ± 19.82% | 45.27 ± 24.82% | 47.55 ± 20.44% | 33.73 ± 15.58% | 10 |
| CPN [37] | 77.67 ± 8.38% | 57.45 ± 8.46% | 76.95 ± 8.03% | 65.35 ± 6.72% | 48.46 ± 7.37% | 9 |
| SOLOv2 [38] | 88.11 ± 4.48% | 79.55 ± 8.01% | 75.86 ± 6.6% | 77.38 ± 5.82% | 62.94 ± 7.45% | 5 |
| BCNet [39] | 85.98 ± 5.58% | 83.27 ± 8.11% | 62.36 ± 12.08% | 70.55 ± 9.77% | 54.80 ± 10.79% | 7 |
| Modified mini-U-Net [61] | 83.89% | 73.83% | 3 | |||
| mini-U-Net [62] | 81.92% | 68.34% | 4 | |||
| LSD Multiple Comparisons | |||||||
|---|---|---|---|---|---|---|---|
| Measurement | (I) Method | (J) Method | Mean Difference (I-J) | Std. Error | Sig. | 95% C.I. | |
| Lower Bound | Upper Bound | ||||||
| Accuracy | Proposed method | U-Net [2] +InceptionV4 [32] | *** 9.03 | 1.59 | <0.001 | 5.90 | 12.15 |
| Ensemble of U-net variants | *** 7.06 | 1.59 | <0.001 | 3.93 | 10.18 | ||
| U-Net [2] | *** 7.40 | 1.59 | <0.001 | 4.27 | 10.52 | ||
| SegNet [34] | *** 5.88 | 1.59 | <0.001 | 2.75 | 9.00 | ||
| FCN [36] | *** 5.85 | 1.59 | <0.001 | 2.72 | 8.97 | ||
| Modified FCN [6,7,8,9,10,11] | * −3.49 | 1.59 | 0.029 | −6.61 | −0.36 | ||
| YOLOv5 [35] | *** 14.58 | 1.59 | <0.001 | 11.45 | 17.70 | ||
| Deeplabv3+ [40] with MobileNet [41] | ** 5.01 | 1.59 | 0.002 | 1.89 | 8.14 | ||
| Deeplabv3+ [40] with ResNet [33] | ** 5.32 | 1.59 | 0.001 | 2.20 | 8.45 | ||
| Deeplabv3+ [40] with Xception [42] | ** 4.24 | 1.59 | 0.008 | 1.12 | 7.37 | ||
| CPN [37] | *** 11.83 | 1.59 | <0.001 | 8.71 | 14.96 | ||
| SOLOv2 [38] | * 3.40 | 1.59 | 0.033 | 0.28 | 6.53 | ||
| BCNet [39] | * 4.06 | 1.59 | 0.011 | 0.94 | 7.19 | ||
| Precision | Proposed method | U-Net [2] +InceptionV4 [32] | *** 16.71 | 3.37 | <0.001 | 10.10 | 23.32 |
| Ensemble of U-net variants | ** 11.00 | 3.37 | 0.001 | 4.37 | 17.61 | ||
| U-Net [2] | *** 13.71 | 3.37 | <0.001 | 7.10 | 20.32 | ||
| SegNet [34] | *** 18.13 | 3.37 | <0.001 | 11.52 | 24.75 | ||
| FCN [36] | *** 22.72 | 3.37 | <0.001 | 16.11 | 29.34 | ||
| Modified FCN [6,7,8,9,10,11] | −5.94 | 3.37 | 0.078 | −12.55 | 0.68 | ||
| YOLOv5 [35] | *** 30.81 | 3.37 | <0.001 | 24.19 | 37.42 | ||
| Deeplabv3+ [40] with MobileNet [41] | *** 20.63 | 3.37 | <0.001 | 14.02 | 27.24 | ||
| Deeplabv3+ [40] with ResNet [33] | *** 24.41 | 3.37 | <0.001 | 14.81 | 28.03 | ||
| Deeplabv3+ [40] with Xception [42] | *** 15.45 | 3.37 | <0.001 | 8.84 | 22.07 | ||
| CPN [37] | *** 11.26 | 3.37 | 0.001 | 4.64 | 17.87 | ||
| SOLOv2 [38] | 0.37 | 3.37 | 0.912 | −6.24 | 6.98 | ||
| BCNet [39] | 0.98 | 3.37 | 0.770 | −5.63 | 7.59 | ||
| Recall | Proposed method | U-Net [2] +InceptionV4 [32] | *** 40.52 | 2.70 | <0.001 | 35.23 | 45.81 |
| Ensemble of U-net variants | *** 38.31 | 2.70 | <0.001 | 33.02 | 43.60 | ||
| U-Net [2] | *** 87.44 | 2.70 | <0.001 | 82.14 | 92.73 | ||
| SegNet [34] | *** 53.81 | 2.70 | <0.001 | 48.52 | 59.10 | ||
| FCN [36] | *** 40.89 | 2.70 | <0.001 | 35.60 | 46.18 | ||
| Modified FCN [6,7,8,9,10,11] | *** 19.59 | 2.70 | <0.001 | 14.30 | 24.88 | ||
| YOLOv5 [35] | 0.81 | 2.70 | 0.764 | -4.48 | 6.10 | ||
| Deeplabv3+ [40] with MobileNet [41] | *** 24.46 | 2.70 | <0.001 | 19.15 | 29.75 | ||
| Deeplabv3+ [40] with ResNet [33] | *** 28.71 | 2.70 | <0.001 | 23.42 | 34.00 | ||
| Deeplabv3+ [40] with Xception [42] | *** 30.47 | 2.70 | <0.001 | 25.18 | 35.76 | ||
| CPN [37] | *** 34.07 | 2.70 | <0.001 | 28.78 | 39.36 | ||
| SOLOv2 [38] | *** 20.96 | 2.70 | <0.001 | 15.66 | 26.25 | ||
| BCNet [39] | *** 28.86 | 2.70 | <0.001 | 23.57 | 34.15 | ||
| F1-score | Proposed method | U-Net [2] +InceptionV4 [32] | *** 30.79 | 2.38 | <0.001 | 26.11 | 35.47 |
| Ensemble of U-net variants | *** 27.27 | 2.38 | <0.001 | 22.59 | 31.95 | ||
| U-Net [2] | *** 74.91 | 2.38 | <0.001 | 70.23 | 79.59 | ||
| SegNet [34] | *** 41.47 | 2.38 | <0.001 | 36.79 | 46.15 | ||
| FCN [36] | *** 32.92 | 2.38 | <0.001 | 28.24 | 37.60 | ||
| Modified FCN [6,7,8,9,10,11] | * 5.88 | 2.38 | 0.014 | 1.20 | 10.57 | ||
| YOLOv5 [35] | *** 23.45 | 2.38 | <0.001 | 18.77 | 28.13 | ||
| Deeplabv3+ [40] with MobileNet [41] | *** 22.47 | 2.38 | <0.001 | 17.78 | 27.15 | ||
| Deeplabv3+ [40] with ResNet [33] | *** 25.22 | 2.38 | <0.001 | 20.54 | 29.90 | ||
| Deeplabv3+ [40] with Xception [42] | *** 22.74 | 2.38 | <0.001 | 18.06 | 27.42 | ||
| CPN [37] | *** 22.30 | 2.38 | <0.001 | 17.62 | 26.98 | ||
| SOLOv2 [38] | *** 9.34 | 2.38 | <0.001 | 4.66 | 14.02 | ||
| BCNet [39] | *** 14.24 | 2.38 | <0.001 | 9.56 | 18.92 | ||
| Jaccard Index | Proposed method | U-Net [2] +InceptionV4 [32] | *** 37.30 | 2.44 | <0.001 | 32.51 | 42.08 |
| Ensemble of U-net variants | *** 33.96 | 2.44 | <0.001 | 29.18 | 38.74 | ||
| U-Net [2] | *** 68.71 | 2.44 | <0.001 | 63.93 | 73.50 | ||
| SegNet [34] | *** 45.62 | 2.44 | <0.001 | 40.84 | 50.40 | ||
| FCN [36] | *** 38.32 | 2.44 | <0.001 | 33.54 | 43.10 | ||
| Modified FCN [6,7,8,9,10,11] | *** 10.00 | 2.44 | <0.001 | 5.22 | 14.78 | ||
| YOLOv5 [35] | *** 29.17 | 2.44 | <0.001 | 24.39 | 33.96 | ||
| Deeplabv3+ [40] with MobileNet [41] | *** 29.96 | 2.44 | <0.001 | 25.18 | 34.75 | ||
| Deeplabv3+ [40] with ResNet [33] | *** 32.74 | 2.44 | <0.001 | 27.96 | 37.52 | ||
| Deeplabv3+ [40] with Xception [42] | *** 30.35 | 2.44 | <0.001 | 25.57 | 35.13 | ||
| CPN [37] | *** 29.19 | 2.44 | <0.001 | 24.41 | 33.97 | ||
| SOLOv2 [38] | *** 14.84 | 2.44 | <0.001 | 10.06 | 19.62 | ||
| BCNet [39] | *** 20.49 | 2.44 | <0.001 | 15.70 | 25.27 | ||
| LSD Multiple Comparisons | |||||||
|---|---|---|---|---|---|---|---|
| Measurement | (I) Method | (J) Method | Mean Difference (I-J) | Std. Error | Sig. | 95% C.I. | |
| Lower Bound | Upper Bound | ||||||
| Accuracy | Proposed method | U-Net [2] +InceptionV4 [32] | *** 9.72 | 1.72 | <0.001 | 6.33 | 13.10 |
| Ensemble of U-net variants | *** 9.82 | 1.72 | <0.001 | 6.43 | 13.21 | ||
| U-Net [2] | *** 7.75 | 1.72 | <0.001 | 4.36 | 11.13 | ||
| SegNet [34] | *** 8.47 | 1.72 | <0.001 | 5.29 | 11.64 | ||
| FCN [36] | *** 10.89 | 1.72 | <0.001 | 7.50 | 14.27 | ||
| Modified FCN [6,7,8,9,10,11] | ** 5.59 | 1.72 | 0.001 | 2.21 | 8.98 | ||
| YOLOv5 [35] | *** 9.97 | 1.72 | <0.001 | 6.59 | 13.36 | ||
| Deeplabv3+ [40] with MobileNet [41] | *** 17.31 | 1.72 | <0.001 | 14.92 | 20.69 | ||
| Deeplabv3+ [40] with ResNet [33] | *** 13.75 | 1.72 | <0.001 | 10.36 | 17.14 | ||
| Deeplabv3+ [40] with Xception [42] | *** 15.92 | 1.72 | <0.001 | 12.53 | 19.30 | ||
| CPN [37] | *** 11.03 | 1.72 | <0.001 | 7.64 | 14.41 | ||
| SOLOv2 [38] | *** 9.86 | 1.72 | <0.001 | 6.48 | 13.25 | ||
| BCNet [39] | *** 10.92 | 1.72 | <0.001 | 7.53 | 14.30 | ||
| Precision | Proposed method | U-Net [2] +InceptionV4 [32] | *** 13.28 | 3.21 | <0.001 | 6.96 | 19.60 |
| Ensemble of U-net variants | *** 12.39 | 3.21 | <0.001 | 6.07 | 18.71 | ||
| U-Net [2] | *** 16.38 | 3.21 | <0.001 | 10.06 | 22.70 | ||
| SegNet [34] | *** 21.07 | 3.21 | <0.001 | 14.76 | 27.39 | ||
| FCN [36] | *** 14.22 | 3.21 | <0.001 | 7.91 | 20.54 | ||
| Modified FCN [6,7,8,9,10,11] | 4.66 | 3.21 | 0.148 | −1.66 | 10.97 | ||
| YOLOv5 [35] | *** 27.00 | 3.21 | <0.001 | 20.68 | 33.32 | ||
| Deeplabv3+ [40] with MobileNet [41] | *** 31.72 | 3.21 | <0.001 | 25.41 | 38.04 | ||
| Deeplabv3+ [40] with ResNet [33] | *** 27.78 | 3.21 | <0.001 | 21.46 | 34.10 | ||
| Deeplabv3+ [40] with Xception [42] | *** 30.78 | 3.21 | <0.001 | 24.46 | 37.10 | ||
| CPN [37] | *** 19.39 | 3.21 | <0.001 | 13.07 | 25.71 | ||
| SOLOv2 [38] | * 7.67 | 3.21 | 0.018 | 1.35 | 13.98 | ||
| BCNet [39] | *** 13.17 | 3.21 | <0.001 | 6.85 | 19.48 | ||
| Recall | Proposed method | U-Net [2] +InceptionV4 [32] | *** 21.28 | 3.45 | <0.001 | 14.48 | 28.07 |
| Ensemble of U-net variants | *** 22.50 | 3.45 | <0.001 | 15.71 | 29.30 | ||
| U-Net [2] | *** 14.69 | 3.45 | <0.001 | 7.89 | 21.48 | ||
| SegNet [34] | 4.78 | 3.45 | 0.167 | −2.02 | 11.57 | ||
| FCN [36] | *** 38.07 | 3.45 | <0.001 | 31.28 | 44.87 | ||
| Modified FCN [6,7,8,9,10,11] | *** 24.36 | 3.45 | <0.001 | 17.57 | 31.16 | ||
| YOLOv5 [35] | * 8.72 | 3.45 | 0.012 | 1.93 | 15.52 | ||
| Deeplabv3+ [40] with MobileNet [41] | *** 14.28 | 3.45 | <0.001 | 7.48 | 21.08 | ||
| Deeplabv3+ [40] with ResNet [33] | ** 10.50 | 3.45 | 0.003 | 3.71 | 17.30 | ||
| Deeplabv3+ [40] with Xception [42] | *** 20.17 | 3.45 | <0.001 | 13.37 | 26.97 | ||
| CPN [37] | *** 16.56 | 3.45 | <0.001 | 9.76 | 23.35 | ||
| SOLOv2 [38] | *** 31.34 | 3.45 | <0.001 | 24.54 | 38.13 | ||
| BCNet [39] | *** 26.72 | 3.45 | <0.001 | 19.93 | 33.52 | ||
| F1-score | Proposed method | U-Net [2] +InceptionV4 [32] | *** 17.81 | 2.63 | <0.001 | 12.63 | 22.99 |
| Ensemble of U-net variants | *** 18.25 | 2.63 | <0.001 | 13.07 | 23.44 | ||
| U-Net [2] | *** 16.01 | 2.63 | <0.001 | 10.83 | 21.20 | ||
| SegNet [34] | *** 14.40 | 2.63 | <0.001 | 9.22 | 19.59 | ||
| FCN [36] | *** 30.92 | 2.63 | <.001 | 25.73 | 36.10 | ||
| Modified FCN [6,7,8,9,10,11] | *** 16.84 | 2.63 | <0.001 | 11.66 | 22.03 | ||
| YOLOv5 [35] | *** 18.75 | 2.63 | <0.001 | 13.57 | 23.94 | ||
| Deeplabv3+ [40] with MobileNet [41] | *** 25.37 | 2.63 | <0.001 | 20.18 | 30.55 | ||
| Deeplabv3+ [40] with ResNet [33] | *** 20.98 | 2.63 | <0.001 | 15.79 | 26.16 | ||
| Deeplabv3+ [40] with Xception [42] | *** 27.25 | 2.63 | <0.001 | 22.07 | 32.44 | ||
| CPN [37] | *** 18.81 | 2.63 | <0.001 | 13.63 | 23.99 | ||
| SOLOv2 [38] | *** 18.81 | 2.63 | <0.001 | 17.74 | 28.10 | ||
| BCNet [39] | *** 24.64 | 2.63 | <0.001 | 16.46 | 26.83 | ||
| Jaccard Index | Proposed method | U-Net [2] +InceptionV4 [32] | *** 23.70 | 3.06 | <0.001 | 17.68 | 29.72 |
| Ensemble of U-net variants | *** 22.98 | 3.06 | <0.001 | 19.96 | 29.00 | ||
| U-Net [2] | *** 21.70 | 3.06 | <0.001 | 15.68 | 27.72 | ||
| SegNet [34] | *** 19.68 | 3.06 | <0.001 | 13.66 | 25.69 | ||
| FCN [36] | *** 36.92 | 3.06 | <0.001 | 30.90 | 42.94 | ||
| Modified FCN [6,7,8,9,10,11] | *** 21.99 | 3.06 | <0.001 | 15.97 | 28.01 | ||
| YOLOv5 [35] | *** 25.06 | 3.06 | <0.001 | 19.04 | 31.08 | ||
| Deeplabv3+ [40] with MobileNet [41] | *** 30.67 | 3.06 | <0.001 | 24.65 | 36.69 | ||
| Deeplabv3+ [40] with ResNet [33] | *** 26.12 | 3.06 | <0.001 | 20.10 | 32.14 | ||
| Deeplabv3+ [40] with Xception [42] | *** 34.01 | 3.06 | <0.001 | 27.99 | 40.03 | ||
| CPN [37] | *** 24.35 | 3.06 | <0.001 | 18.33 | 30.36 | ||
| SOLOv2 [38] | *** 29.33 | 3.06 | <0.001 | 23.36 | 35.36 | ||
| BCNet [39] | *** 26.17 | 3.06 | <0.001 | 20.15 | 32.19 | ||
| LSD Multiple Comparisons | |||||||
|---|---|---|---|---|---|---|---|
| Measurement | (I) Method | (J) Method | Mean Difference (I-J) | Std. Error | Sig. | 95% C.I. | |
| Lower Bound | Upper Bound | ||||||
| Accuracy | Proposed method | Modified FCN [6,7,8,9,10,11] | 0.16 | 1.17 | 0.888 | −2.13 | 2.46 |
| Deeplabv3+ [40] with MobileNet [41] | *** 8.38 | 1.17 | <0.001 | 6.08 | 10.67 | ||
| Deeplabv3+ [40] with ResNet [33] | *** 8.48 | 1.17 | <0.001 | 6.19 | 10.77 | ||
| Deeplabv3+ [40] with Xception [42] | *** 16.71 | 1.17 | <0.001 | 14.42 | 19.00 | ||
| CPN [37] | *** 15.88 | 1.17 | <0.001 | 13.58 | 18.17 | ||
| SOLOv2 [38] | *** 5.44 | 1.17 | <0.001 | 3.14 | 7.73 | ||
| BCNet [39] | *** 7.56 | 1.17 | <0.001 | 5.27 | 9.85 | ||
| Precision | Proposed method | Modified FCN [6,7,8,9,10,11] | −0.15 | 1.76 | 0.932 | −3.60 | 3.30 |
| Deeplabv3+ [40] with MobileNet [41] | *** 16.22 | 1.76 | <0.001 | 12.77 | 19.68 | ||
| Deeplabv3+ [40] with ResNet [33] | *** 21.97 | 1.76 | <0.001 | 18.51 | 25.42 | ||
| Deeplabv3+ [40] with Xception [42] | *** 25.41 | 1.76 | <0.001 | 21.95 | 28.86 | ||
| CPN [37] | *** 34.21 | 1.76 | <0.001 | 30.75 | 37.66 | ||
| SOLOv2 [38] | *** 12.21 | 1.76 | <0.001 | 8.75 | 15.66 | ||
| BCNet [39] | *** 8.48 | 1.76 | <0.001 | 5.03 | 11.93 | ||
| Recall | Proposed method | Modified FCN [6,7,8,9,10,11] | 1.39 | 2.26 | 0.538 | −3.05 | 5.83 |
| Deeplabv3+ [40] with MobileNet [41] | *** 18.59 | 2.26 | <0.001 | 14.14 | 23.03 | ||
| Deeplabv3+ [40] with ResNet [33] | ** 7.09 | 2.26 | 0.002 | 2.64 | 11.53 | ||
| Deeplabv3+ [40] with Xception [42] | *** 38.25 | 2.26 | <0.001 | 33.81 | 42.69 | ||
| CPN [37] | ** 6.57 | 2.26 | 0.004 | 2.13 | 11.01 | ||
| SOLOv2 [38] | ** 7.66 | 2.26 | 0.002 | 3.22 | 12.10 | ||
| BCNet [39] | *** 21.16 | 2.26 | <0.001 | 16.72 | 25.60 | ||
| F1-score | Proposed method | Modified FCN [6,7,8,9,10,11] | 0.57 | 1.80 | 0.752 | −2.97 | 4.11 |
| Deeplabv3+ [40] with MobileNet [41] | *** 17.61 | 1.80 | <0.001 | 14.08 | 21.15 | ||
| Deeplabv3+ [40] with ResNet [33] | *** 14.46 | 1.80 | <0.001 | 10.92 | 18.00 | ||
| Deeplabv3+ [40] with Xception [42] | *** 39.43 | 1.80 | <0.001 | 35.89 | 42.97 | ||
| CPN [37] | *** 21.63 | 1.80 | <0.001 | 18.09 | 25.17 | ||
| SOLOv2 [38] | *** 9.60 | 1.80 | <0.001 | 6.06 | 13.17 | ||
| BCNet [39] | *** 16.43 | 1.80 | <0.001 | 12.89 | 19.97 | ||
| Jaccard Index | Proposed method | Modified FCN [6,7,8,9,10,11] | 1.25 | 1.91 | 0.515 | −2.51 | 5.00 |
| Deeplabv3+ [40] with MobileNet [41] | *** 24.67 | 1.91 | <0.001 | 20.91 | 28.43 | ||
| Deeplabv3+ [40] with ResNet [33] | *** 20.93 | 1.91 | <0.001 | 17.17 | 24.69 | ||
| Deeplabv3+ [40] with Xception [42] | *** 44.49 | 1.91 | <0.001 | 40.73 | 48.25 | ||
| CPN [37] | *** 29.75 | 1.91 | <0.001 | 25.99 | 33.51 | ||
| SOLOv2 [38] | *** 15.27 | 1.91 | <0.001 | 11.52 | 19.03 | ||
| BCNet [39] | *** 23.41 | 1.91 | <0.001 | 19.65 | 27.17 | ||
| (a) | |||||||
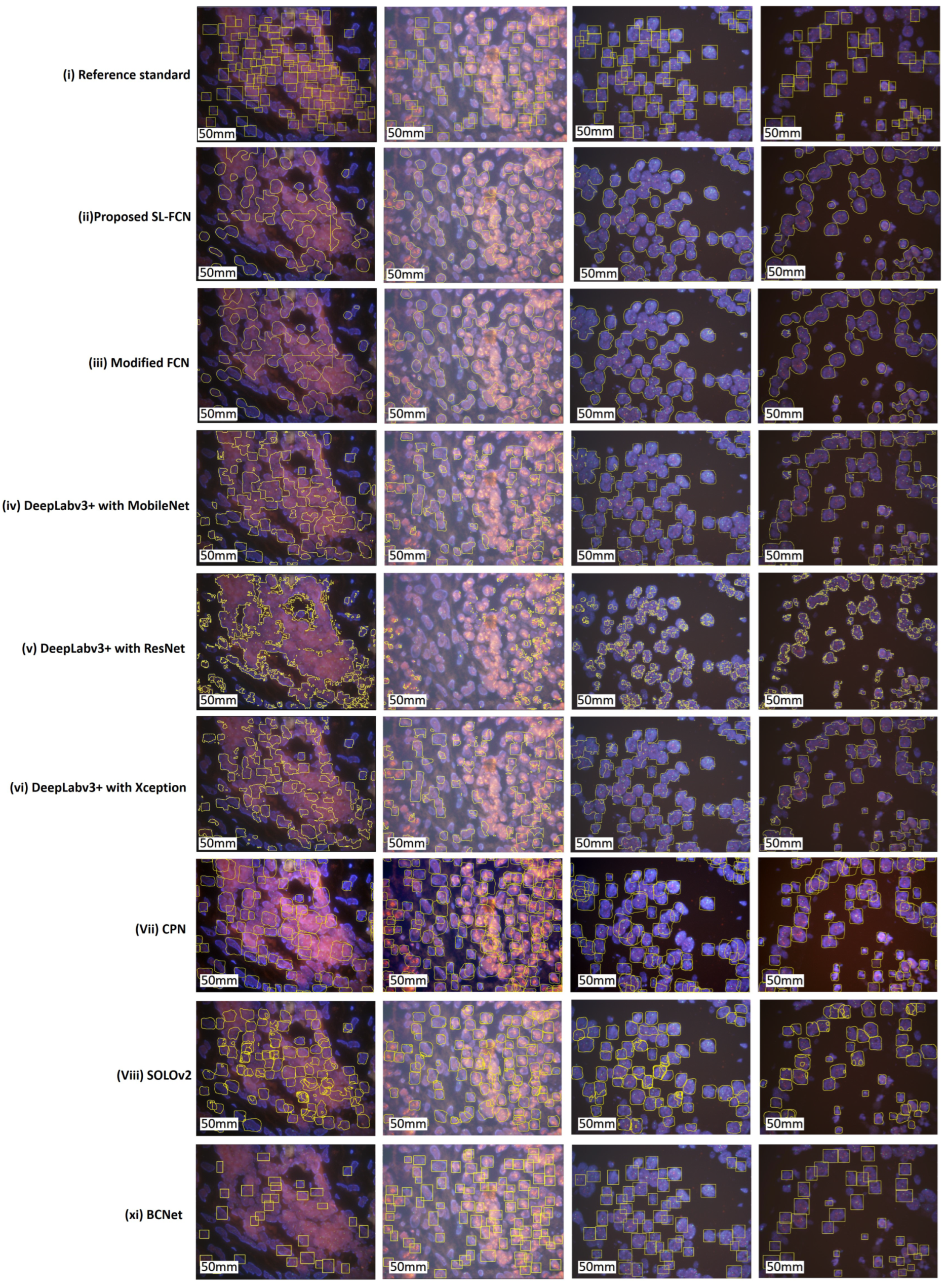
| Thyroid Dataset | |||||||
| Method | Accuracy | Precision | Recall | F1-Score | Jaccard Index | Rank F1-Score | |
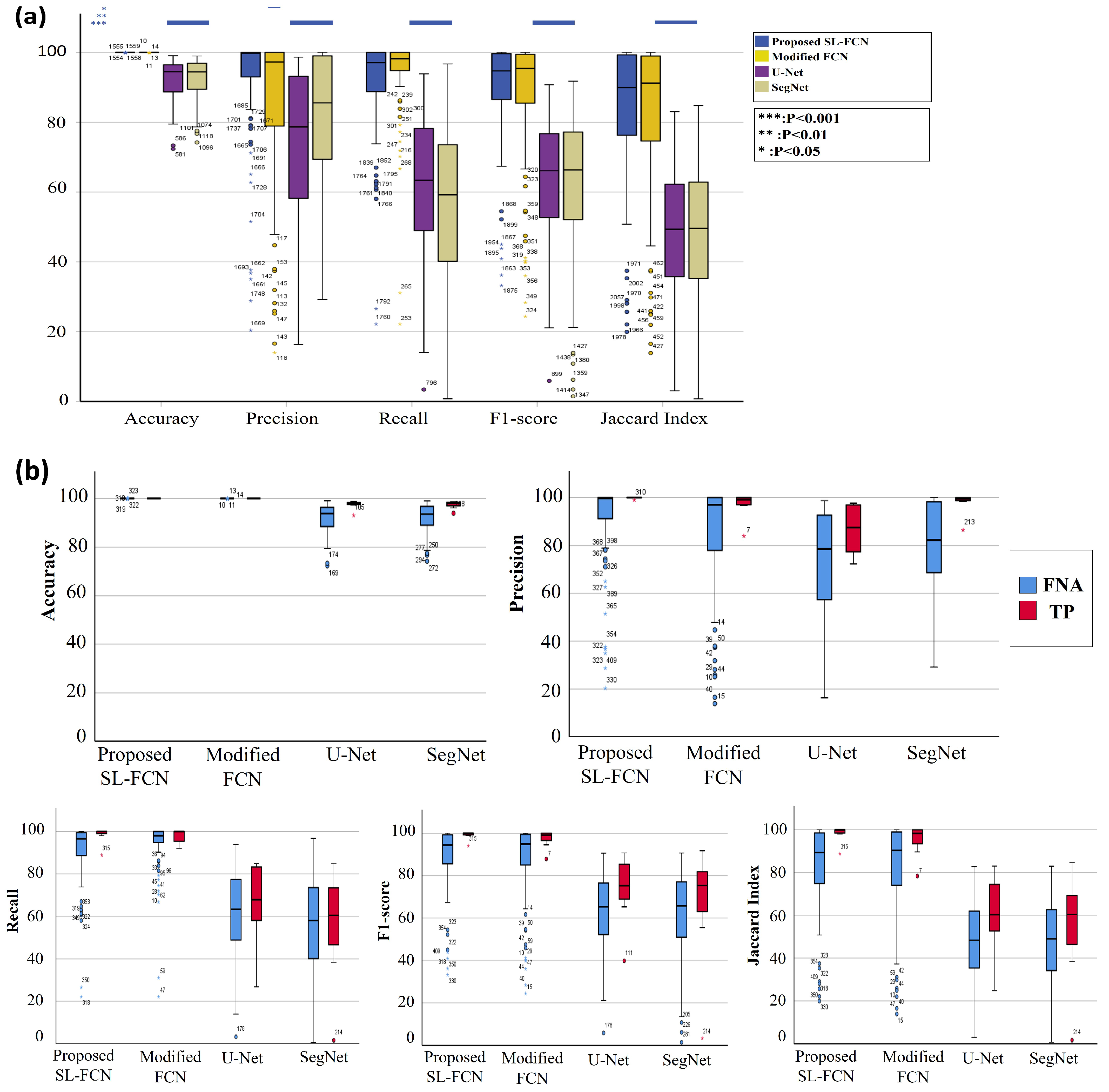
| Proposed soft label FCN | ALL | 99.99 ± 0.01% | 92.02 ± 16.60% | 90.90 ± 14.25% | 89.82 ± 14.92% | 84.16 ± 19.91% | 1 |
| TP | 100% | 99.86 ± 0.35% | 98.35 ± 3.91% | 99.06 ± 2.05% | 98.22 ± 3.87% | ||
| FNA | 99.99 ± 0.01% | 91.36 ± 17.13% | 80.28 ± 16.63% | 89.04 ± 15.28% | 82.98 ± 20.27% | ||
| Modified FCN [6,7,8,9,10,11] | ALL | 99.99 ± 0.01% | 85.91 ± 21.93% | 94.39 ± 11.7% | 87.6 ± 18.05% | 81.6 ± 23.21% | 2 |
| TP | 100% | 97.03 ± 5.42% | 97.85 ± 3.49% | 97.41 ± 4.25% | 95.12 ± 7.62% | ||
| FNA | 99.99 ± 0.01% | 84.97 ± 22.54% | 94.10 ± 12.14% | 86.78 ± 18.53% | 80.45 ± 23.73% | ||
| SegNet | ALL | 92.37 ± 5.99% | 81.38 ± 19.11% | 55.82 ± 23.45% | 61.82 ± 20.79% | 47.68 ± 20.04% | 4 |
| TP | 97.40 ± 1.59% | 97.84 ± 4.6% | 56 ± 26.08% | 66.95 ± 27.73% | 54.86 ± 25.28% | ||
| FNA | 91.95 ± 6.04% | 80 ± 19.23% | 55.81 ± 23.37% | 61.39 ± 20.23% | 47.08 ± 19.58% | ||
| U-Net | ALL | 92.14 ± 5.91% | 74.03 ± 20.99% | 61.03 ± 21.17% | 63.68 ± 18.34% | 49.21 ± 18.92% | 3 |
| TP | 97.42 ± 1.77% | 86.72 ± 10.1% | 66.26 ± 19.55% | 73.68 ± 15.99% | 60.34 ± 18.25% | ||
| FNA | 91.7 ± 5.93% | 72.96 ± 21.34% | 60.59 ± 21.33% | 62.84 ± 18.35% | 48.27 ± 18.77% | ||
| (b) | |||||||
| LSD Multiple Comparisons | |||||||
| Measurement | (I) Method | (J) Method | Mean Difference (I-J) | Std. Error | Sig. | 95%C.I. | |
| Lower Bound | Upper Bound | ||||||
| Accuracy | Proposed method | Modified FCN [6,7,8,9,10,11] | <0.01 | 0.59 | 0.990 | −1.15 | 1.15 |
| SegNet [34] | *** 7.62 | 0.59 | <0.001 | 6.49 | 8.77 | ||
| U-Net [2] | *** 7.88 | 0.59 | <0.001 | 6.69 | 9.00 | ||
| Precision | Proposed method | Modified FCN [6,7,8,9,10,11] | * 6.12 | 2.75 | 0.03 | 0.70 | 11.53 |
| SegNet [34] | *** 10.64 | 2.75 | <0.001 | 5.23 | 16.05 | ||
| U-Net [2] | *** 17.99 | 2.75 | <0.001 | 12.58 | 23.41 | ||
| Recall | Proposed method | Modified FCN [6,7,8,9,10,11] | −3.49 | 2.55 | 0.17 | −8.50 | 1.52 |
| SegNet [34] | *** 35.08 | 2.55 | <0.001 | 30.07 | 40.09 | ||
| U-Net [2] | *** 29.88 | 2.55 | <0.001 | 24.86 | 34.89 | ||
| F1-score | Proposed method | Modified FCN [6,7,8,9,10,11] | 2.21 | 2.53 | 0.38 | −2.76 | 7.19 |
| SegNet [34] | *** 27.99 | 2.53 | <0.001 | 23.03 | 32.97 | ||
| U-Net [2] | *** 26.14 | 2.53 | <0.001 | 21.17 | 31.11 | ||
| Jaccard Index | Proposed method | Modified FCN [6,7,8,9,10,11] | 2.56 | 2.87 | 0.37 | −3.08 | 8.20 |
| SegNet [34] | *** 36.48 | 2.87 | <0.001 | 30.84 | 42.12 | ||
| U-Net [2] | *** 34.95 | 2.87 | <0.001 | 29.31 | 40.59 | ||
| (a) Quantitative results when changing the soft label regions. | |||||
| Proposed Method | Accuracy | Precision | Recall | F1-Score | Jaccard Index |
| with ( = 0.01, = 2, = 6) | 87.77 ± 14.97% | 77.19 ± 23.41% | 91.20 ± 7.72% | 81.67 ± 17.76% | 72.40 ± 23.05% |
| with ( = 0.01, = 1, = 3) | 87.27 ± 13.94% | 76.58 ± 22.48% | 86.59 ± 10.36% | 79.69 ± 17.34% | 69.32 ± 21.90% |
| with ( = 0.01, = 4, = 12) | 86.66 ± 10.32% | 79.84 ± 20.09% | 74.80 ± 14.29% | 75.62 ± 15.85% | 63.17 ± 19.36% |
| (b) Quantitative results when changing the initialization methods. | |||||
| Proposed Method | Accuracy | Precision | Recall | F1-Score | Jaccard Index |
| without initialization | 87.77 ± 14.97% | 77.19 ± 23.41% | 91.20 ± 7.72% | 81.67 ± 17.76% | 72.40 ± 23.05% |
| with Kaiming initialization | 89.69 ± 9.93% | 80.37 ± 19.39% | 84.08 ± 13.37% | 81.16 ± 15.85% | 71.02 ± 20.99% |
| with Xavier initialization | 89.36 ± 11.08% | 80.63 ± 20.51% | 84.35 ± 12.70% | 81.24 ± 16.64% | 71.36 ± 21.59% |
| (c) Quantitative results by modifying the weight parameters of : (). | |||||
| Proposed Method | Accuracy | Precision | Recall | F1-Score | Jaccard Index |
| with () | 87.77 ± 14.97% | 77.19 ± 23.41% | 91.20 ± 7.72% | 81.67 ± 17.76% | 72.40 ± 23.05% |
| with (, , ) | 88.66 ± 10.11% | 78.83 ± 20.67% | 81.11 ± 14.14% | 78.64 ± 16.54% | 67.68 ± 21.64% |
| with (, , ) | 87.18 ± 12.82% | 78.66 ± 21.13% | 84.14 ± 11.71% | 79.62 ± 16.19% | 68.89 ± 20.90% |
| (d) Quantitative results for the ablation study when using Kaiming initialization and different optimizer. | |||||
| Proposed Method | Accuracy | Precision | Recall | F1-Score | Jaccard Index |
| with SGD with momentum | 89.69 ± 9.93% | 80.36 ± 19.39% | 84.08 ± 13.37% | 81.16 ± 15.85% | 71.02 ± 20.99% |
| with Adam | 63.18 ± 13.30% | 34.18 ± 19.90% | 21.03 ± 10.18% | 22.69 ± 8.59% | 13.07 ± 5.68% |
| with Adaptive Gradient | 72.63 ± 11.89% | 77.59 ± 23.94% | 1.15 ± 1.14% | 2.24 ± 2.16% | 1.14 ± 1.12% |
| with AdaDelta | 58.87 ± 10.45% | 35.39 ± 18.09% | 48.87 ± 19.80% | 35.02 ± 11.77% | 21.88 ± 9.44% |
| with NAG | 87.45 ± 10.54% | 79.08 ± 20.31% | 79.88 ± 13.46% | 77.91 ± 15.81% | 66.30 ± 19.70% |
| with RMSprop | 75.05 ± 10.99% | 81.10 ± 13.88% | 14.18 ± 7.15% | 23.16 ± 9.14% | 13.41 ± 6.22% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.-W.; Lin, K.-Y.; Lin, Y.-J.; Khalil, M.-A.; Chu, K.-L.; Chao, T.-K. A Soft Label Deep Learning to Assist Breast Cancer Target Therapy and Thyroid Cancer Diagnosis. Cancers 2022, 14, 5312. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14215312
Wang C-W, Lin K-Y, Lin Y-J, Khalil M-A, Chu K-L, Chao T-K. A Soft Label Deep Learning to Assist Breast Cancer Target Therapy and Thyroid Cancer Diagnosis. Cancers. 2022; 14(21):5312. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14215312
Chicago/Turabian StyleWang, Ching-Wei, Kuan-Yu Lin, Yi-Jia Lin, Muhammad-Adil Khalil, Kai-Lin Chu, and Tai-Kuang Chao. 2022. "A Soft Label Deep Learning to Assist Breast Cancer Target Therapy and Thyroid Cancer Diagnosis" Cancers 14, no. 21: 5312. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14215312