
Go with the Flow—Early Assessment of Measurable Residual Disease in Children with Acute Lymphoblastic Leukemia Treated According to ALL IC-BFM2009

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Diagnosis and Assessment of MRD
2.3. Stratification—Allocation to Treatment Groups
2.4. Treatment
2.5. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. Outcomes
3.2.1. Outcome by Patient Characteristics
3.2.2. Outcome by Risk Group
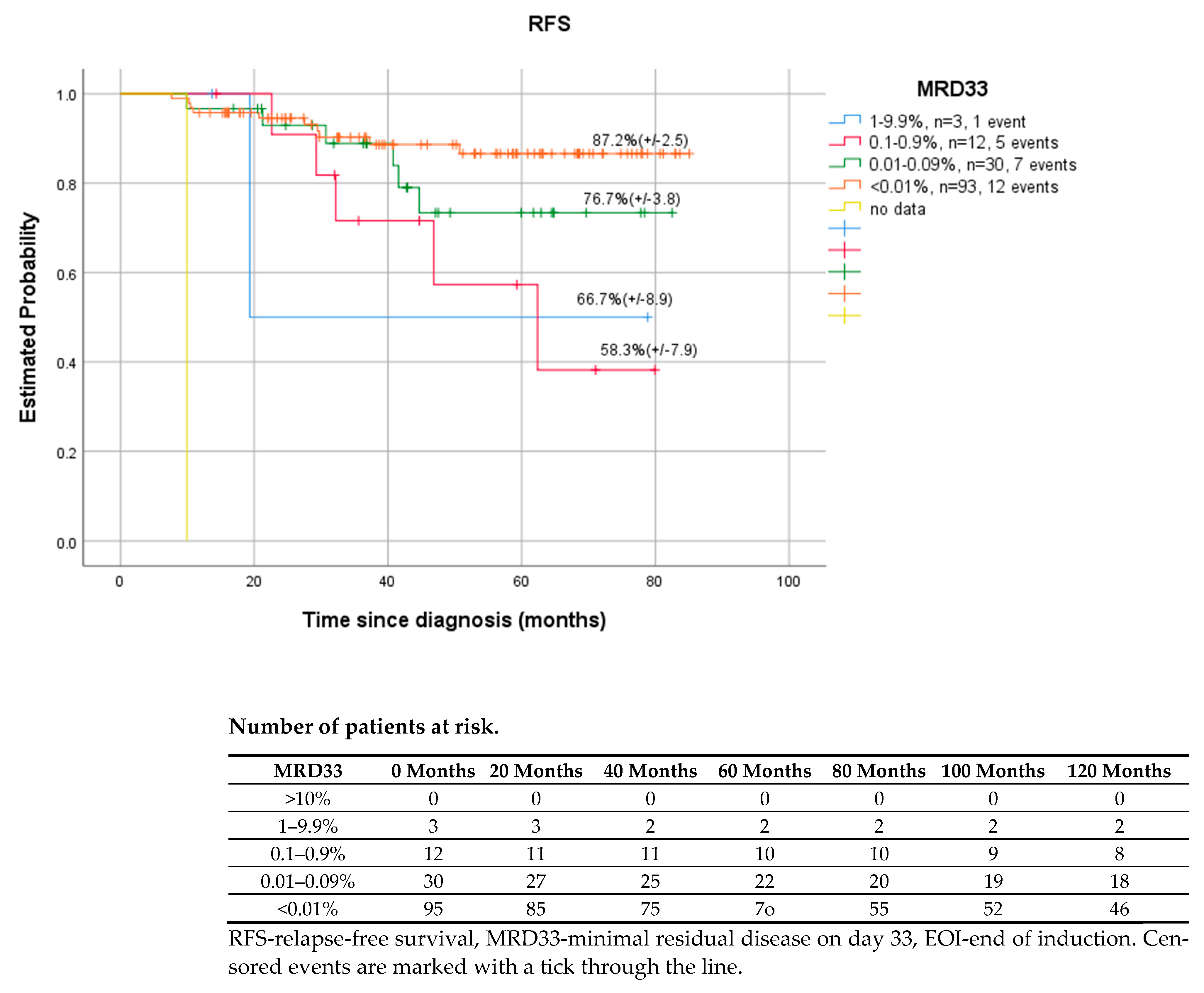
3.2.3. Outcome by MRD Status
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fuda, F.; Chen, W. Minimal/measurable residual disease detection in acute leukemias by multiparameter flow cytometry. Curr. Hematol. Malig. Rep. 2018, 13, 455–466. [Google Scholar] [CrossRef] [PubMed]
- Wood, B.; Wu, D.; Crossley, B.; Dai, Y.; Williamson, D.; Gawad, C.; Borowitz, M.J.; Devidas, M.; Maloney, K.W.; Larsen, E.; et al. Measurable residual disease detection by high-throughput sequencing improves risk stratification for pediatric B-ALL. Blood 2018, 12, 1350–1359. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, D.; Enshaei, A.; Bartram, J.; Hancock, J.; Harrison, C.J.; Hough, R.; Samarasinghe, S.; Schwab, C.; Vora, A.; Wade, R.; et al. Genotype-Specific Minimal Residual Disease Interpretation Improves Stratification in Pediatric Acute Lymphoblastic Leukemia. J. Clin. Oncol. 2018, 1, 34–43. [Google Scholar] [CrossRef]
- van Dongen, J.J.; Seriu, T.; Panzer-Grümayer, E.R.; Biondi, A.; Pongers-Willemse, M.J.; Corral, L.; Stolz, F.; Schrappe, M.; Masera, G.; Kamps, W.A.; et al. Prognostic value of minimal residual disease in acute lymphoblastic leukaemia in childhood. Lancet 1998, 9142, 1731–1738. [Google Scholar] [CrossRef]
- Heikamp, E.B.; Pui, C.H. Next-Generation evaluation and treatment of pediatric acute lymphoblastic leuekmia. J. Pediatr. 2018, 203, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Kruse, A.; Abdel-Azim, N.; Kim, H.N.; Ruan, Y.; Phan, V.; Ogana, H.; Wang, W.; Lee, R.; Gang, E.J.; Khazal, S.; et al. Minimal Residual Disease Detection in Acute Lymphoblastic Leukemia. Int. J. Mol. Sci. 2020, 3, 1054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Short, N.J.; Jabbour, E.; Albitar, M.; de Lima, M.; Gore, L.; Jorgensen, J.; Logan, A.C.; Park, J.; Ravandi, F.; Shah, B.; et al. Recommendations for the assessment and management of measurable residual disease in adults with acute lymphoblastic leukemia: A consensus of North American experts. Am. J. Hematol. 2019, 2, 257–265. [Google Scholar] [CrossRef]
- Ratei, R.; Basso, G.; Dworzak, M.; Gaipa, G.; Veltroni, M.; Rhein, P.; Biondi, A.; Schrappe, M.; Ludwig, W.D.; Karawajew, L.; et al. Monitoring treatment response of childhood precursor B-cell acute lymphoblastic leukemia in the AIEOP-BFM-ALL 2000 protocol with multiparameter flow cytometry: Predictive impact of early blast reduction on the remission status after induction. Leukemia 2009, 3, 528–534. [Google Scholar] [CrossRef] [Green Version]
- Yametti, G.P.C.; Ostrow, T.H.; Jasinski, S.; Raets, E.A.; Carrol, W.L.; Evensen, N.A. Minimal residual disease in acute lymphoblastic leukemia: Current practice and future directions. Cancers 2021, 13, 1847. [Google Scholar] [CrossRef]
- Coustan-Smith, E.; Behm, F.G.; Sanchez, J.; Boyett, J.M.; Hancock, M.L.; Raimondi, S.C.; Rubnitz, J.E.; Rivera, G.K.; Sandlund, J.T.; Pui, C.H.; et al. Immunological detection of minimal residual disease in children with acute lymphoblastic leukaemia. Lancet 1998, 351, 550–554. [Google Scholar] [CrossRef]
- Coustan-Smith, E.; Ribeiro, R.C.; Stow, P.; Zhou, Y.; Pui, C.H.; Rivera, G.K.; Pedrosa, F.; Campana, D. A simplified flow cytometric assay identifies children with acute lymphoblastic leukemia who have a superior clinical outcome. Blood 2006, 1, 97–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borowitz, M.J.; Devidas, M.; Hunger, S.P.; Bowman, W.P.; Carroll, A.J.; Carroll, W.L.; Linda, S.; Martin, P.L.; Pullen, D.J.; Viswanatha, D.; et al. Clinical significance of minimal residual disease in childhood acute lymphoblastic leukemia and its relationship to other prognostic factors: A Children’s Oncology Group study. Blood 2008, 12, 5477–5485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basso, G.; Veltroni, M.; Valsecchi, M.G.; Dworzak, M.N.; Ratei, R.; Silvestri, D.; Benetello, A.; Buldini, B.; Maglia, O.; Masera, G.; et al. Risk of relapse of childhood acute lymphoblastic leukemia is predicted by flow cytometric measurement of residual disease on day 15 bone marrow. J. Clin. Oncol. 2009, 31, 5168–5174. [Google Scholar] [CrossRef]
- Pieters, R.; de Groot-Kruseman, H.; Van der Velden, V.; Fiocco, M.; van den Berg, H.; de Bont, E.; Egeler, R.M.; Hoogerbrugge, P.; Kaspers, G.; Van der Schoot, E.; et al. Successful Therapy Reduction and Intensification for Childhood Acute Lymphoblastic Leukemia Based on Minimal Residual Disease Monitoring: Study ALL10 From the Dutch Childhood Oncology Group. J. Clin. Oncol. 2016, 22, 2591–2601. [Google Scholar] [CrossRef] [Green Version]
- Vora, A.; Goulden, N.; Wade, R.; Mitchell, C.; Hancock, J.; Hough, R.; Rowntree, C.; Richards, S. Treatment reduction for children and young adults with low-risk acute lymphoblastic leukaemia defined by minimal residual disease (UKALL 2003): A randomised controlled trial. Lancet Oncol. 2013, 3, 199–209. [Google Scholar] [CrossRef] [Green Version]
- Schrappe, M.; Bleckmann, K.; Zimmermann, M.; Biondi, A.; Möricke, A.; Locatelli, F.; Cario, G.; Rizzari, C.; Attarbaschi, A.; Valsecchi, M.G.; et al. Reduced-Intensity Delayed Intensification in Standard-Risk Pediatric Acute Lymphoblastic Leukemia Defined by Undetectable Minimal Residual Disease: Results of an International Randomized Trial (AIEOP-BFM ALL 2000). J. Clin. Oncol. 2018, 36, 244–253. [Google Scholar] [CrossRef] [Green Version]
- Conter, V.; Bartram, C.R.; Valsecchi, M.G.; Schrauder, A.; Panzer-Grümayer, R.; Möricke, A.; Aricò, M.; Zimmermann, M.; Mann, G.; De Rossi, G.; et al. Molecular response to treatment redefines all prognostic factors in children and adolescents with B-cell precursor acute lymphoblastic leukemia: Results in 3184 patients of the AIEOP-BFM ALL 2000 study. Blood 2010, 16, 3206–3214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmiegelow, K.; Forestier, E.; Hellebostad, M.; Heyman, M.; Kristinsson, J.; Söderhäll, S.; Taskinen, M.; Nordic Society of Paediatric Haematology and Oncology. Long-term results of NOPHO ALL-92 and ALL-2000 studies of childhood acute lymphoblastic leukemia. Leukemia 2010, 2, 345–354. [Google Scholar] [CrossRef] [Green Version]
- Vora, A.; Goulden, N.; Mitchell, C.; Hancock, J.; Hough, R.; Rowntree, C.; Moorman, A.V.; Wade, R. Augmented post-remission therapy for a minimal residual disease-defined high-risk subgroup of children and young people with clinical standard-risk and intermediate-risk acute lymphoblastic leukaemia (UKALL 2003): A randomised controlled trial. Lancet Oncol. 2014, 8, 809–818. [Google Scholar] [CrossRef]
- Pui, C.H.; Pei, D.; Raimondi, S.C.; Coustan-Smith, E.; Jeha, S.; Cheng, C.; Bowman, W.P.; Sandlund, J.T.; Ribeiro, R.C.; Rubnitz, J.E.; et al. Clinical impact of minimal residual disease in children with different subtypes of acute lymphoblastic leukemia treated with Response-Adapted therapy. Leukemia 2017, 2, 333–339. [Google Scholar] [CrossRef]
- Campana, D.; Pui, C.H. Minimal residual disease–guided therapy in childhood acute lymphoblastic leukemia. Blood 2017, 129, 1913–1918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connor, D.; Moorman, A.V.; Wade, R.; Hancock, J.; Tan, R.M.; Bartram, J.; Moppett, J.; Schwab, C.; Patrick, K.; Harrison, C.J.; et al. Use of Minimal Residual Disease Assessment to Redefine Induction Failure in Pediatric Acute Lymphoblastic Leukemia. J. Clin. Oncol. 2017, 35, 660–667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeoh, A.E.; Ariffin, H.; Chai, E.L.; Kwok, C.S.; Chan, Y.H.; Ponnudurai, K.; Campana, D.; Tan, P.L.; Chan, M.Y.; Kham, S.K.; et al. Minimal residual disease-guided treatment deintensification for children with acute lymphoblastic leukemia: Results from the Malaysia-Singapore acute lymphoblastic leukemia 2003 study. J. Clin. Oncol. 2012, 30, 2384–2392. [Google Scholar] [CrossRef] [PubMed]
- Stanulla, M.; Cavé, H.; Moorman, A.V. IKZF1 deletions in pediatric acute lymphoblastic leukemia: Still a poor prognostic marker? Blood 2020, 135, 252–260. [Google Scholar] [CrossRef] [Green Version]
- Stary, J.; Zimmermann, M.; Campbell, M.; Castillo, L.; Dibar, E.; Donska, S.; Gonzalez, A.; Izraeli, S.; Janic, D.; Jazbec, J.; et al. Intensive chemotherapy for childhood acute lymphoblastic leukemia: Results of the randomized intercontinental trial ALL IC-BFM 2002. J. Clin. Oncol. 2014, 32, 174–184. [Google Scholar] [CrossRef] [Green Version]
- Gaipa, G.; Basso, G.; Biondi, A.; Campana, D. Detection of minimal residual disease in pediatric acute lymphoblastic leukemia. Cytom. Part B Clin. Cytom. 2013, 84, 359–369. [Google Scholar] [CrossRef]
- Pedrosa, F.; Coustan-Smith, E.; Zhou, Y.; Cheng, C.; Pedrosa, A.; Lins, M.M.; Pedrosa, M.; Lucena-Silva, N.; Ramos, A.M.L.; Vinhas, E.; et al. Reduced-dose intensity therapy for pediatric lymphoblastic leukemia: Long-term results of the Recife RELLA05 pilot study. Blood 2020, 135, 1458–1466. [Google Scholar] [CrossRef]
- Whitlock, J.A. Go with the flow: Simplified MRD in LMIC ALL. Blood 2020, 135, 1414–1415. [Google Scholar] [CrossRef]
- Schumich, A.; Maurer-Granofszky, M.; Attarbaschi, A.; Pötschger, U.; Buldini, B.; Gaipa, G.; Karawajew, L.; Printz, D.; Ratei, R.; Conter, V.; et al. Flow-cytometric minimal residual disease monitoring in blood predicts relapse risk in pediatric B-cell precursor acute lymphoblastic leukemia in trial AIEOP-BFM-ALL 2000. Pediatr. Blood Cancer 2019, 66, e27590. [Google Scholar] [CrossRef]
- Bassan, R.; Spinelli, O.; Oldani, E.; Intermesoli, T.; Tosi, M.; Peruta, B.; Rossi, G.; Borlenghi, E.; Pogliani, E.M.; Terruzzi, E.; et al. Improved risk classification for risk-specific therapy based on the molecular study of minimal residual disease (MRD) in adult acute lymphoblastic leukemia (ALL). Blood 2009, 13, 4153–4162. [Google Scholar] [CrossRef]
- Pawinska-Wasikowska, K.; Balwierz, W. Cells antigens’ expression modulation during induction treatment of childhood acute lymphoblastic leukemia. Przegl. Lek. 2010, 67, 361–365. [Google Scholar] [PubMed]
- Dworzak, M.N.; Gaipa, G.; Schumich, A.; Maglia, O.; Ratei, R.; Veltroni, M.; Husak, Z.; Basso, G.; Karawajew, L.; Gadner, H.; et al. Modulation of antigen expression in B-cell precursor acute lymphoblastic leukemia during induction therapy is partly transient: Evidence for a drug-induced regulatory phenomenon. Results of the AIEOP-BFM-ALL-FLOW-MRD-Study Group. Cytom. B Clin. Cytom. 2010, 78, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Burnusuzov, H.A.; Spasova, M.I.; Murdjeva, M.A.; Stoyanova, A.A.; Mumdziev, I.N.; Kaleva, V.I.; Belcheva, M.I.; Bosheva, M.N. Immunophenotypic Modulation of the Blast Cells in Childhood Acute Lymphoblastic Leukemia Minimal Residual Disease Detection. Folia Med. 2016, 58, 8–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, D.A.; Zhou, S.; Higley, H.; Mukundan, L.; Fu, S.; Reaman, G.H.; Wood, B.L.; Kelloff, G.J.; Jessup, J.M.; Radich, J.P. Association of Minimal Residual Disease With Clinical Outcome in Pediatric and Adult Acute Lymphoblastic Leukemia: A Meta-analysis. JAMA Oncol. 2017, 3, e170580. [Google Scholar] [CrossRef] [Green Version]
- Xue, Y.J.; Wang, Y.; Jia, Y.P.; Zuo, Y.X.; Wu, J.; Lu, A.D.; Zhang, L.P. The role of minimal residual disease in specific subtypes of pediatric acute lymphoblastic leukemia. Int. J. Hematol. 2021, 113, 47–555. [Google Scholar] [CrossRef]
- Jeha, S.; Choi, J.; Roberts, K.G.; Pei, D.; Coustan-Smith, E.; Inaba, H.; Rubnitz, J.E.; Ribeiro, R.C.; Gruber, T.A.; Raimondi, S.C.; et al. Clinical significance of novel subtypes of acute lymphoblastic leukemia in the context of minimal residual disease-directed therapy. Blood Cancer Discov. 2021, 2, 326–337. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Panel A. For BCP-ALL, six-color tubes: |
 |
| Panel B. For BCP-ALL, ten-color tubes: |
 |
| Panel C. For T-ALL, six-color tubes: |
 |
| Risk Group | Criteria |
|---|---|
| Standard risk group (SRG) 1 |
|
| Intermediate risk group (IRG) High risk group (HRG) 2 | All patients who are not stratified for SR or HR are intermediate-risk patients.
|
| Features | Protocol ALL IC-BFM2009 n = 140 |
|---|---|
| Age in years | |
| Median (range) | 5.1 (1.1–17.4) |
| Sex [n (%)] | |
| Boy | 87 (62%) |
| Girls | 53 (38%) |
| Down syndrome [n (%)] | 5 (3.5%) |
| WBC count (×109/L) | |
| Median (range) | 10.2 (1.0–776) |
| Immunophenotype [n (%)] | |
| BCP-ALL | 130 (93%) |
| T-ALL | 10 (7%) |
| CNS [n (%)] | |
| CNS 1 | 130 (93%) |
| CNS 2 | 5 (3.5%) |
| CNS 3 | 5 (3.5%) |
| Risk group [n (%)] | |
| Standard risk (SR) | 13 (9%) |
| Intermediate risk (IR) | 98 (70%) |
| High risk (HR) | 29 (21%) |
| Genotype [n (%)] | |
| Negative * | 19 (14%) |
| ETV6-RUNX1 | 34 (24%) |
| KMT2A | 4 (3%) |
| TCF3-PBX1 | 2 (1%) |
| PAX5-ETV6 | 1 (<1%) |
| Hyperdiploidy (>50 chromosomes) | 30 (21%) |
| Hypodiploidy (<44 chromosomes) | 1 (<1%) |
| Normal karyotype | 33 (23.5%) |
| No data | 16 (11.5%) |
| Prednisone response [n (%)] | |
| PGR | 121 (86%) |
| PPR | 19 (14%) |
| Complete remission [n (%)] | 140 (100%) |
| Death [n (%)] | 11 (8%) |
| Relapse [n (%)] | 25 (18%) |
| BM relapse | 20 |
| CNS relapse | 3 |
| Relapse of testes | 1 |
| BM + CNS relapse | 1 |
| Secondary malignancies | 2 |
| Features | OS 5-Year % (SE) | p | RFS 5-Year % (SE) | p | EFS 5-Year % (SE) | p |
|---|---|---|---|---|---|---|
| Sex | ||||||
| Boy | 94.4 (2.1) | 0.42 | 81.8 (3.4) | 0.32 | 89.9 (3.5) | 0.32 |
| Girls | 98.1 (1.8) | 87.1 (3.5) | 82.8 (3.3) | |||
| Immunophenotype | ||||||
| BCP-ALL | 96.6 (1.5) | 0.39 | 85.6 (2.4) | 0.003 | 88.0 (2.4) | 0.005 |
| T-ALL | 70.0 (4.7) | 49.2 (9.8) | 50.7 (9.6) | |||
| CNS | ||||||
| CNS 1 + 2 | 96.6 (1.5) | 84.9 (2.5) | 87.3 (2.5) | |||
| CNS 3 | 79.2 (12.9) | 0.1 | 63.7 (16.1) | 0.16 | 65.5 (15.7) | 0.17 |
| Risk group | ||||||
| Standard risk (SR) | 100 | 100 (2.5) | 100 (2.5) | |||
| Intermediate risk (IR) | 92.9 | 0.5 | 79.6 (3.5) | 0.22 | 79.6 (3.5) | 0.21 |
| High risk (HR) | 96.6 | 79.3 (7.4) | 79.3 (7.4) | |||
| Prednisone response | ||||||
| PGR | 96.2 (1.6) | 0.95 | 84.2 (2.7) | 0.7 | 86.7 (2.7) | 0.7 |
| PPR | 91.2 (3.3) | 77.1 (6.8) | 79.1 (6.9) | |||
| Age | ||||||
| <15 yr | 95.9 (1.5) | 0.41 | 84.1 (2.6) | 0.69 | 85.5 (2.5) | 0.69 |
| ≥15 yr | 91.6 (8.7) | 81.3 (10.4) | 84.2 (10.5) | |||
| WBC at diagnosis | ||||||
| <50,000/μL | 97.5 (1.4) | 0.04 | 87.0 (2.4) | 0.001 | 89.4 (2.4) | 0.002 |
| ≥50,000/μL | 86.9 (6.0) | 64.0 (8.9) | 65.7 (8.9) |
| MRD | Day 15 | Day 33 (EOI) | Day 78 (EOC) |
|---|---|---|---|
| ≥10% (10−1) | 31 (22%) | 0 | 0 |
| 1–10% (10−2–10−1) | 44 (31.5%) | 3 (2%) | 0 |
| 0.1–1% (10−3–10−2) | 39 (28%) | 12 (8.5%) | 0 |
| 0.01–0.1% (10−4–10−3) | 16 (11.5%) | 30 (21.5%) | 2 (1.5%) |
| ≤0.01% (<10−4) | 10 (7%) | 95 (68%) | 136 (98.5%) |
| Day 15 (TP1) | Day 33 (TP2) | Day 78 (TP3) | ||||
|---|---|---|---|---|---|---|
| MRD ≥0.1% | MRD < 0.1% | MRD ≥0.1% | MRD <0.1% | MRD ≥0.1% | MRD < 0.1% | |
| 5yOS | 93.1 | 100 | 86.7 | 95.2 | 33.3 | 95.2 |
| p = 0.08 | p = 0.027 | p = 0.001 | ||||
| 5yRFS | 80.5 | 96.2 | 44.2 | 87.2 | 33.3 | 86.3 |
| p = 0.027 | p = 0.008 | p = 0.001 | ||||
| 5yEFS | 80.9 | 96.2 | 44.2 | 87.2 | 33.3 | 86.3 |
| p = 0.097 | p = 0.009 | p = 0.001 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pawinska-Wasikowska, K.; Bukowska-Strakova, K.; Surman, M.; Rygielska, M.; Sadowska, B.; Ksiazek, T.; Klekawka, T.; Wieczorek, A.; Skoczen, S.; Balwierz, W. Go with the Flow—Early Assessment of Measurable Residual Disease in Children with Acute Lymphoblastic Leukemia Treated According to ALL IC-BFM2009. Cancers 2022, 14, 5359. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14215359
Pawinska-Wasikowska K, Bukowska-Strakova K, Surman M, Rygielska M, Sadowska B, Ksiazek T, Klekawka T, Wieczorek A, Skoczen S, Balwierz W. Go with the Flow—Early Assessment of Measurable Residual Disease in Children with Acute Lymphoblastic Leukemia Treated According to ALL IC-BFM2009. Cancers. 2022; 14(21):5359. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14215359
Chicago/Turabian StylePawinska-Wasikowska, Katarzyna, Karolina Bukowska-Strakova, Marta Surman, Monika Rygielska, Beata Sadowska, Teofila Ksiazek, Tomasz Klekawka, Aleksandra Wieczorek, Szymon Skoczen, and Walentyna Balwierz. 2022. "Go with the Flow—Early Assessment of Measurable Residual Disease in Children with Acute Lymphoblastic Leukemia Treated According to ALL IC-BFM2009" Cancers 14, no. 21: 5359. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14215359